51
Department of Critical Care Medicine Kovai Medical Center and
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| Upload: | rebecca-sherman |
| View: | 218 times |
| Download: | 0 times |

Department of Critical Care MedicineKovai Medical Center and Hospital

MONITORING OF MECHANICALLY VENTILATED PATIENT
DR.T.GOPINATHAN MD., IDCCM.,EDIC
Consultant Intensivist Kovai Medical Center and Hospital
GOALS OF MECHANICAL VENTILATION
Decrease the WOB and improve patient
comfort
Maintain adequate gas exchange to keep
body in relative homeostasis

Monitoring : monere - meaning ‘to warn’
Goals of continuous monitoring :
Baseline measurement – initial plan,
reference for future
follow real time specific physiological values
that changes rapidly – alerts for adverse
events
Assessment of therapeutic intervention
OBJECTIVE
Monitoring gas exchange
• Oxygenation
• Ventilation
Monitoring lung and chest wall
mechanics
• Pressure
• Volume
• Flow
• Compliance
• Resistance
RESPIRATORY

Clinical signs and symptoms -
Nonspecific, late
ABG
PULSE OXYMETRY
CAPNOGRAPHY
The clinical significance of
hypoxia/hypercapnia depends on
Chronicity of Compensatory mechanisms
and tolerance of vital organs
GAS EXCHANGE
Pulsatile signal generated by
arterial blood
Difference in the absorption
spectra of oxyHb and Hb.
Determines O2 saturation by
absorption spectrophotometry
PULSE OXYMETRY

Advantages:
• Inexpensive
• Accuracy - Spo2 below 80%
• Direct measurement
• Continuous
• Non-invasive
• Pleth variability index
PULSE OXYMETRY
Shape of oxygen dissociation
curve
Dyshemoglobinemia
Dyes
Nail polish
Ambient light
LIMITATIONS OF PULSE OXYMETRY
False alarms
Motion artifact
Skin pigmentation
Low perfusion state
Advantages:
• Direct measurement of PaO2 and PaCO2
• Also gives values for acid-base status and
electrolytes
Disadvantages:
• Not specific or sensitive
• Calculates saturation
• Requires invasive procedure
• Intermittent sampling - miss events
ABG

Factors influencing values:
PaO2 varies
• Age
• Altitude
• Sampling techniques: air bubble, heparin
PaCO2 remains relatively constant
ABG
Efficacy of oxygen exchange
• Alveolar gas equation
PAO2 = PIO2 – (PaCO2/R)
• AaDO2 = PAO2 – PaO2
• Oxygenation index : PaO2/(FiO2 X Paw)
• PaO2/FiO2
OXYGENATION
• PaCO2 is directly measured in blood.
• PaCO2 is a measure of ventilation - CO2
elimination
• Increased PaCO2
PaCO2 = VCO2/ ( Vt –Vd ) RR
VENTILATION
.

• Between ETT and expiratory limb of vent
tubing
• Expired CO2 against time
• Healthy subjects, V/Q ≈ 1, EtCO2
≈PaCO2
• Information about RR and rhythm
• ETT placement (obstr, discon, kinking)
• Determine dead space, CO and PE
• Best PEEP, PaCO2 – PET CO2 difference
CAPNOGRAPHY

CAPNOGRAPHY

ABNORMAL EtCO2 WAVEFORMS
ASTHMA/ COPD
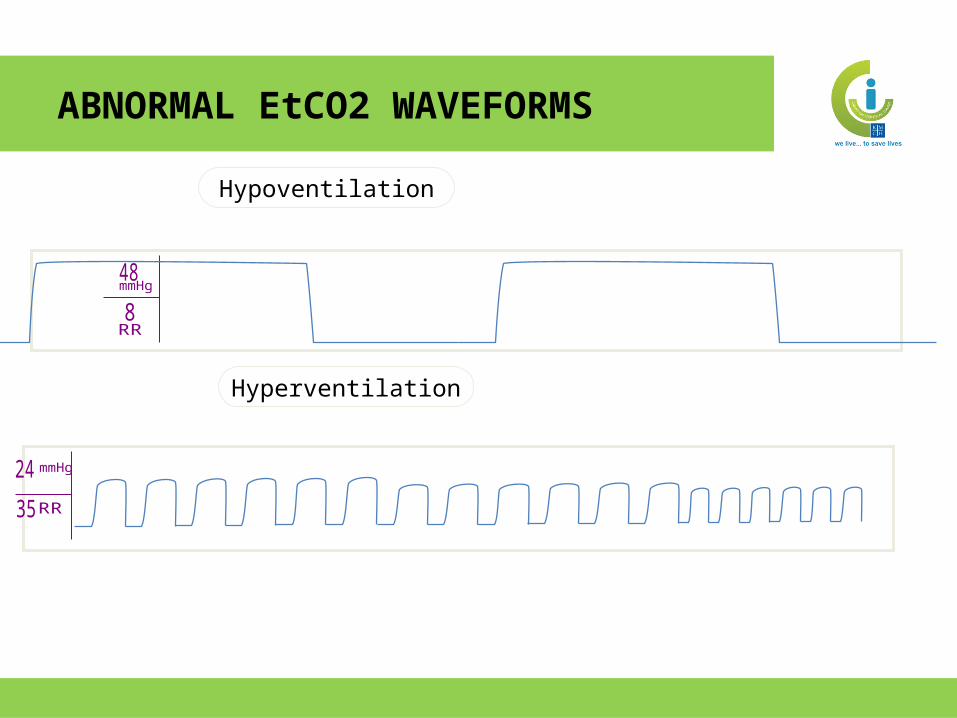
Hypoventilation
ABNORMAL EtCO2 WAVEFORMS
Hyperventilation

• Describe how to use graphics to more
appropriately adjust the patient ventilator
interface.
• Identify adverse complications of mechanical
ventilation.
OBJECTIVES OF VENTILATOR GRAPHICS
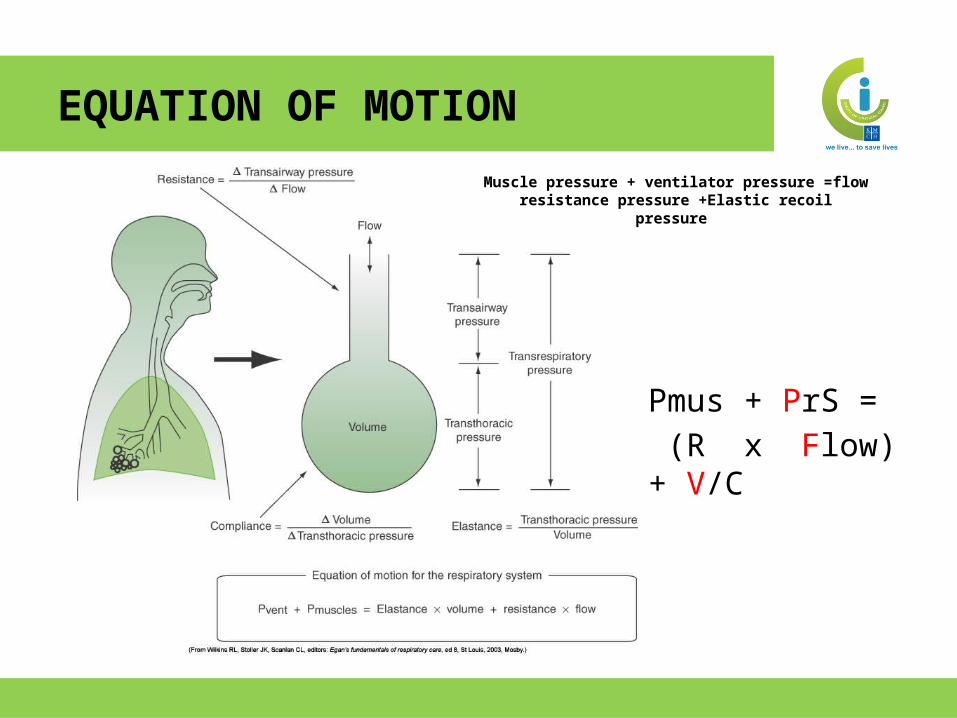
Pmus + PrS = (R x Flow) + V/C
Muscle pressure + ventilator pressure =flow resistance pressure +Elastic recoil
pressure
EQUATION OF MOTION

LOOPS
• Pressure vs
Volume
• Flow vs volume
SCALARS
• Pressure vs.
Time
• Flow vs. Time
• Volume vs. Time
SCALARS & LOOPS

Mode of ventilation
Independent variables
Dependent variables
Waveforms that will be useful
Waveforms that normally remain unchanged
Volume Control/ Assist-Control
Tidal volume,
RR, Flow rate, PEEP, I/E ratio
PawPressure-time:Changes in Pip, Pplat
Flow-time (expiratory): Changes in compliancePressure-volume loop: Overdistension, optimal PEEP
Volume-timeFlow time (inspiratory)Flow-volume loop
Pressure Control
Paw, Inspiratory time (RR), PEEP and I/E ratio
Vt, flowVolume-time and flow-time: Changes in Vt and compliancePressure-volume loop: Overdistension, optimal PEEP
Pressure-time
Pressure support/CPAP
PS and PEEP Vt,and RR, flow, I/E Ratio
Volume- timeFlow- time(for Vt and VE)
MODE OF VENTILATION -> USEFUL WAVEFORMS

PRESSURE TIME

1 2 3 4 5 6
20
Sec
Paw
cmH2O
Pressure VentilationVolume Ventilation
PRESSURE TIME
time
pres
sure
time
flow
time
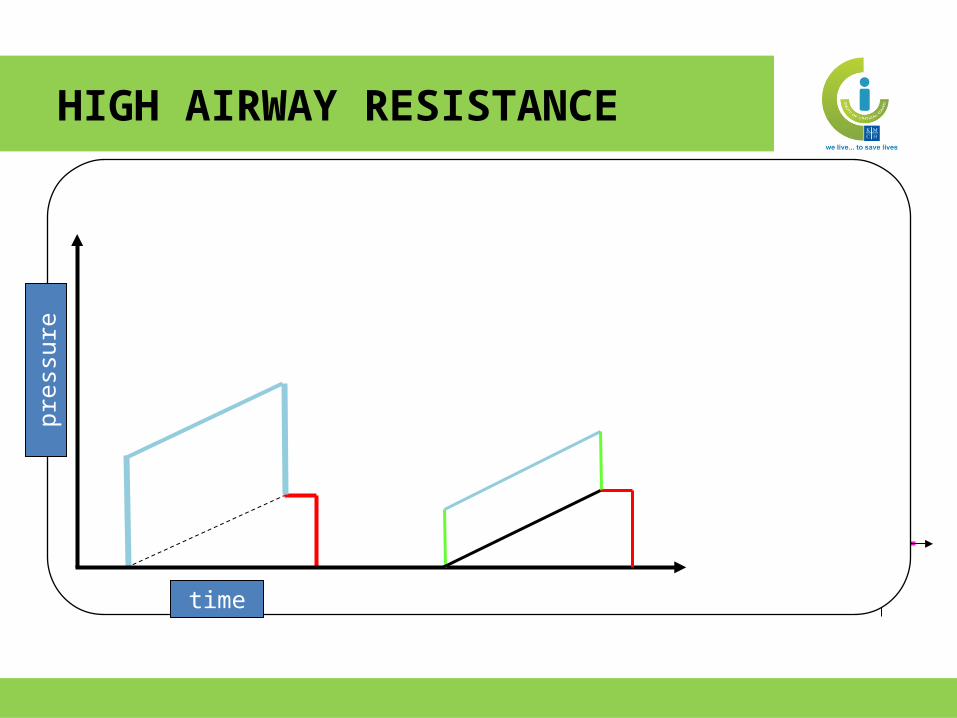
pres
sure
HIGH AIRWAY RESISTANCE

time
pres
sure
Paw(peak) = Flow x Resistance + Volume x 1/compliance + PEEP
HIGH FLOW RATE

30
Time (s)
-10
1 2
awPcmH2O
Adequate flow
Flow set too low3
INADEQUATE FLOW - VCV

time
pres
sure
DECREASED COMPLIANCE

1 2 3 4 5 6
SEC
120
120EXH
INSP
Expiration
V
.LPM
Inspiration
PIFR
PEFR
Ti
Te
Vt
FLOW - TIME
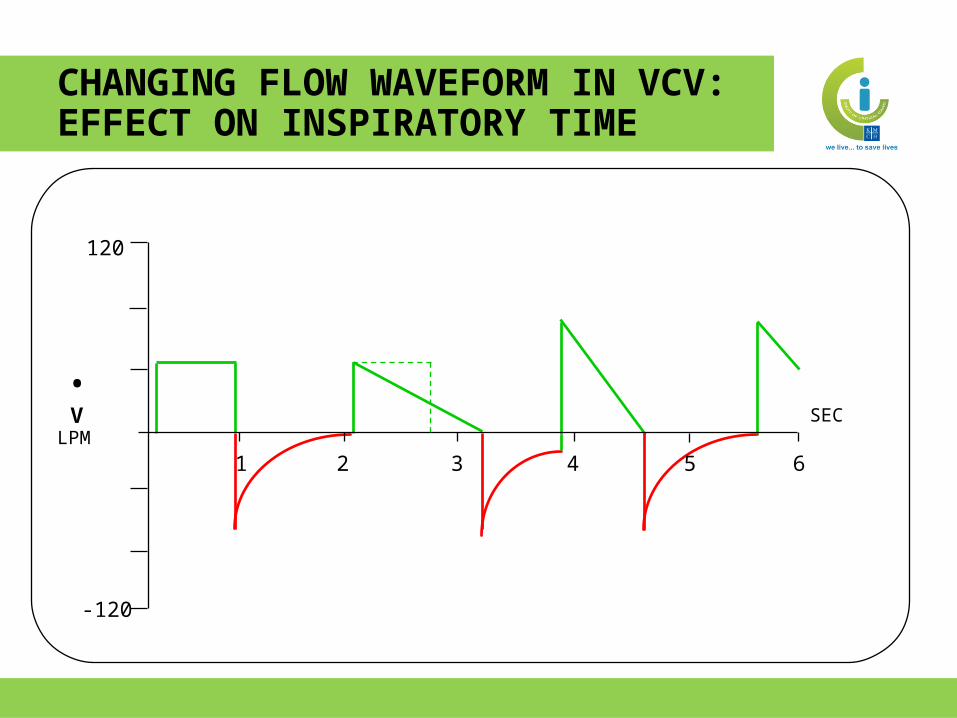
1 2 3 4 5 6
SEC
120
-120
V
.LPM
CHANGING FLOW WAVEFORM IN VCV: EFFECT ON INSPIRATORY TIME

1 2 3 4 5 6
SEC
120
-120
V
.LPM
EXPIRATORY FLOW RATE AND CHANGES IN EXPIRATORY RESISTANCE
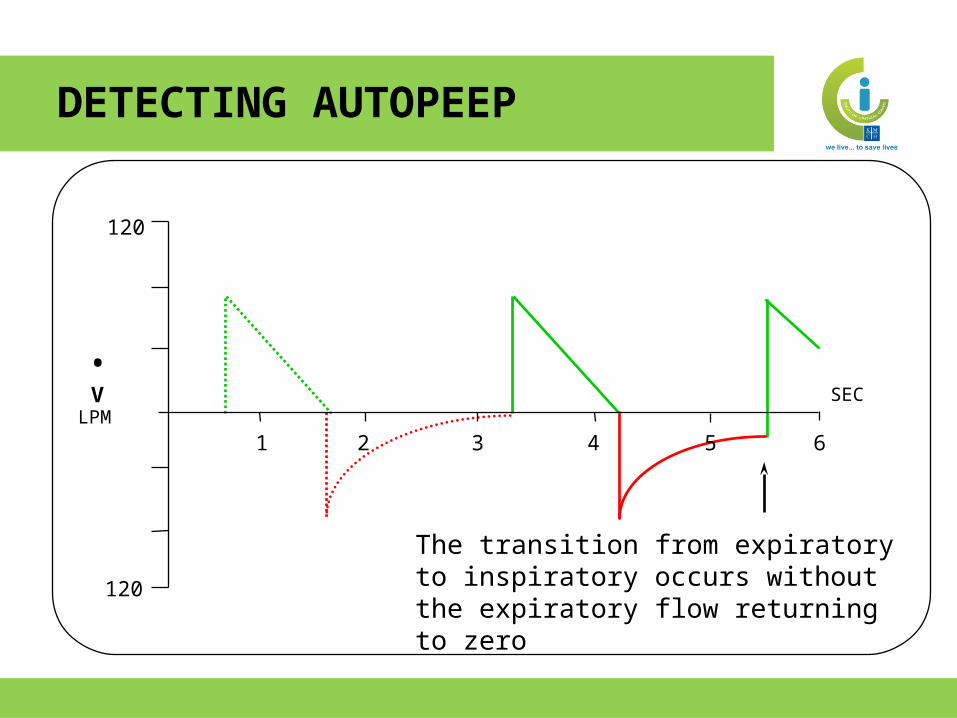
The transition from expiratory to inspiratory occurs without the expiratory flow returning to zero
1 2 3 4 5 6
SEC
120
120
V
.LPM
DETECTING AUTOPEEP

Expiration
SEC
800 ml
2 3 4 5 61
VT
Inspiration
Vt
Ti Te
VOLUME Vs TIME CURVE

1 2 3 4 5 6
SEC
1.2
-0.4
VT
Liters
A
A = exhalation that does not return to zero
Leak Volume
LEAKS

Expiration
SEC
800 ml
2 3 4 5 61
VT
Inspiration
Ti Te
End Expiratory Hold
PEEP i
PEEP e
MEASUREMENT OF AUTOPEEP
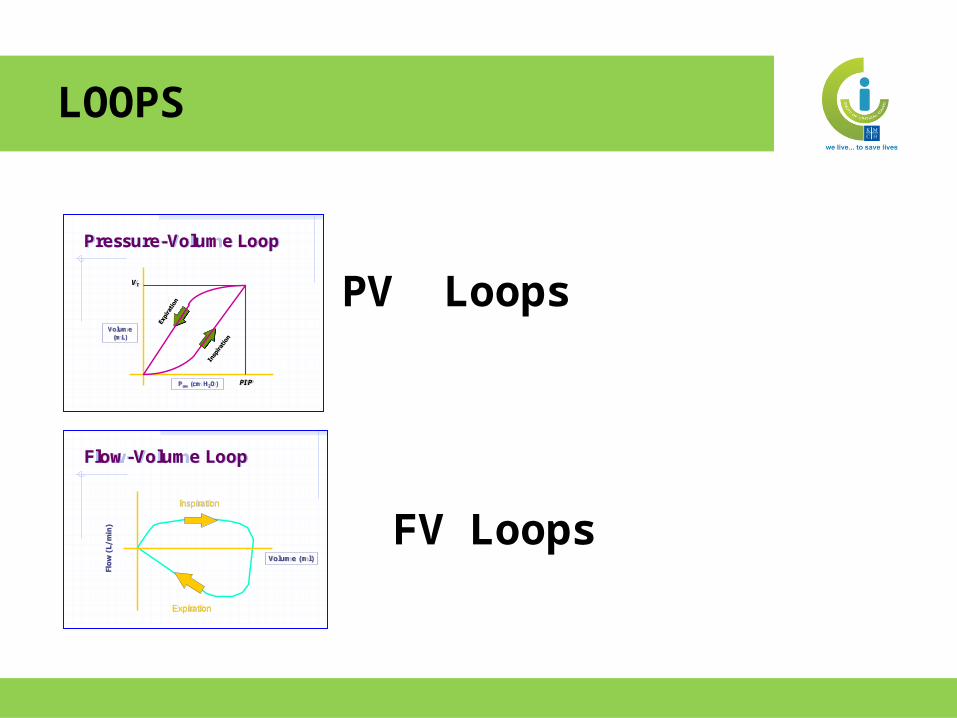
PV Loops
FV Loops
Flow-Volume Loop
Volume (ml)
Inspiration
Expiration
Pressure-Volume Loop
Volume (mL)
PIP
VT
Paw (cm H2O)
LOOPS

Inspiration
Expiration
v0 20 40 602040-60
Paw
cmH2O
Assisted breath
controlled breath
spontaneous breath
ASSISTED BREATH

PV LOOP-INCREASED RESISTANCE
PCV
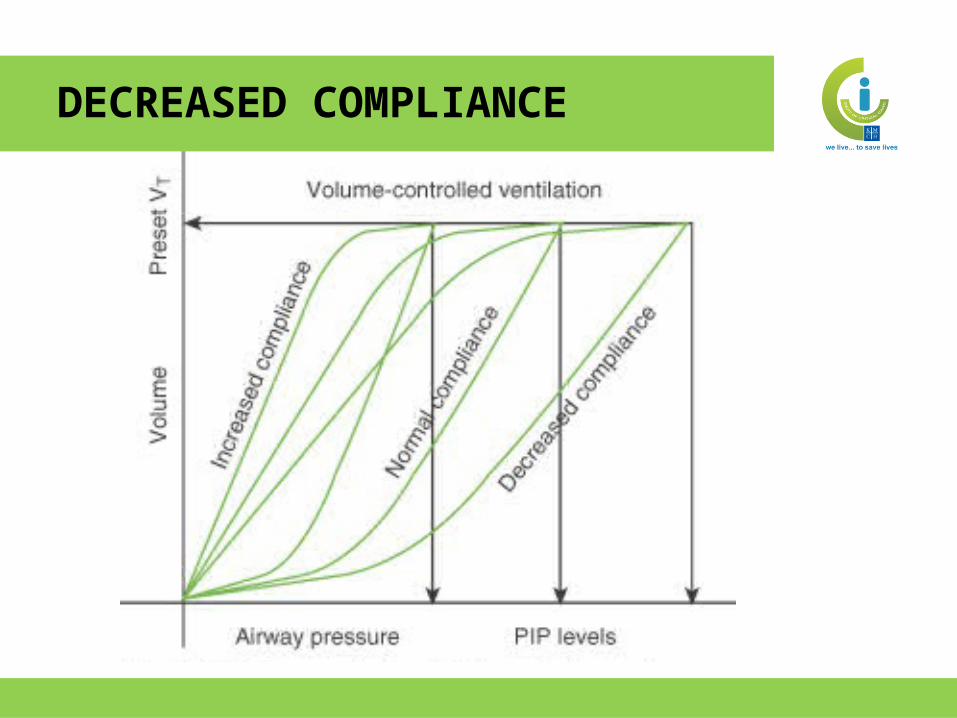
DECREASED COMPLIANCE
Essentials of Ventilator Graphics ©2000 RespiMedu
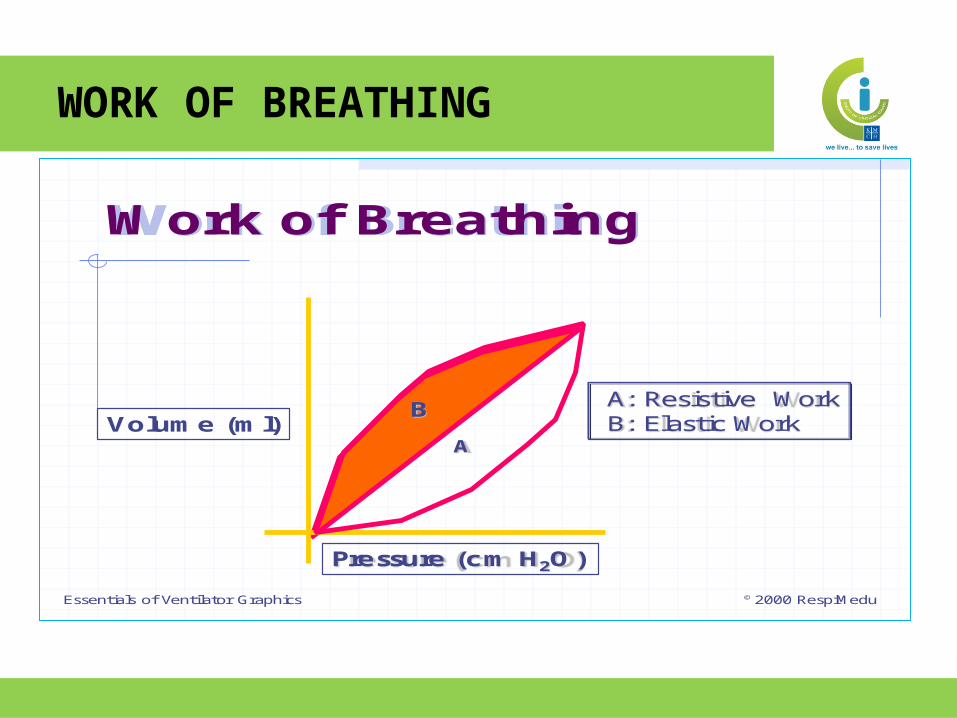
Work of Breathing
B
A
A: Resistive WorkB: Elastic Work
Pressure (cm H2O)
Volume (ml)
WORK OF BREATHING

COPD

LEAK

B
A
0 20 40 60-20-40-60
0.2
0.4
0.6
LITERS
Paw
cmH2O
C
A = inspiratory pressure
B = upper inflection point
C = lower inflection point
VT
OVERDISTENSION
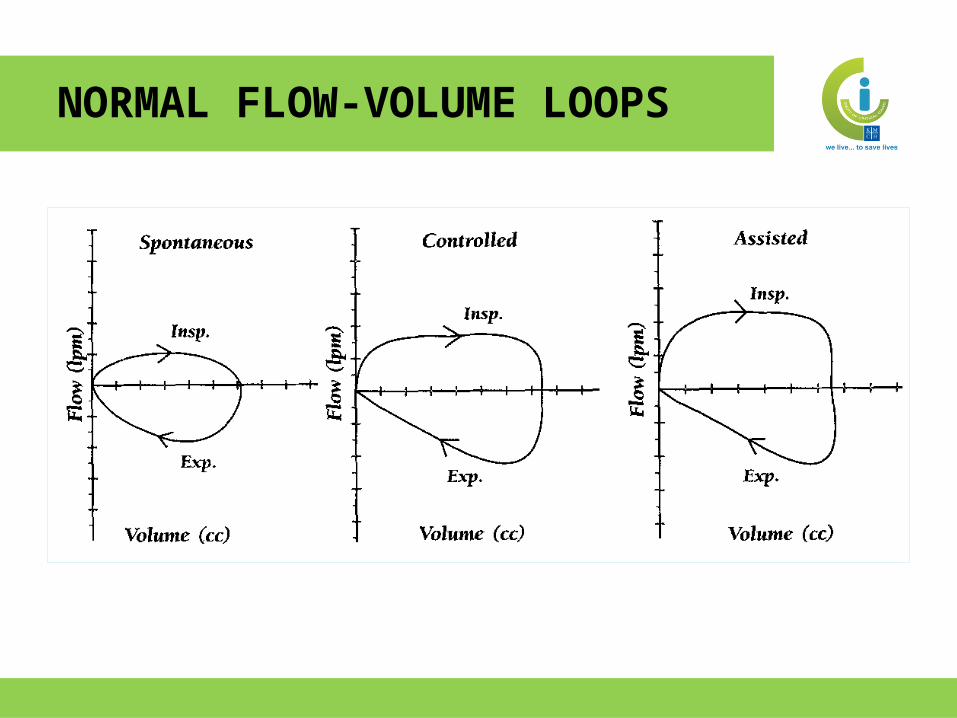
NORMAL FLOW-VOLUME LOOPS

Flow
Volume
Peak Expiratory Flow
Peak Inspiratory Flow
Tidal Volume
Inspiration
Expiration
FV LOOP – VOLUME CONTROL

ETT OR CICUIT LEAKS
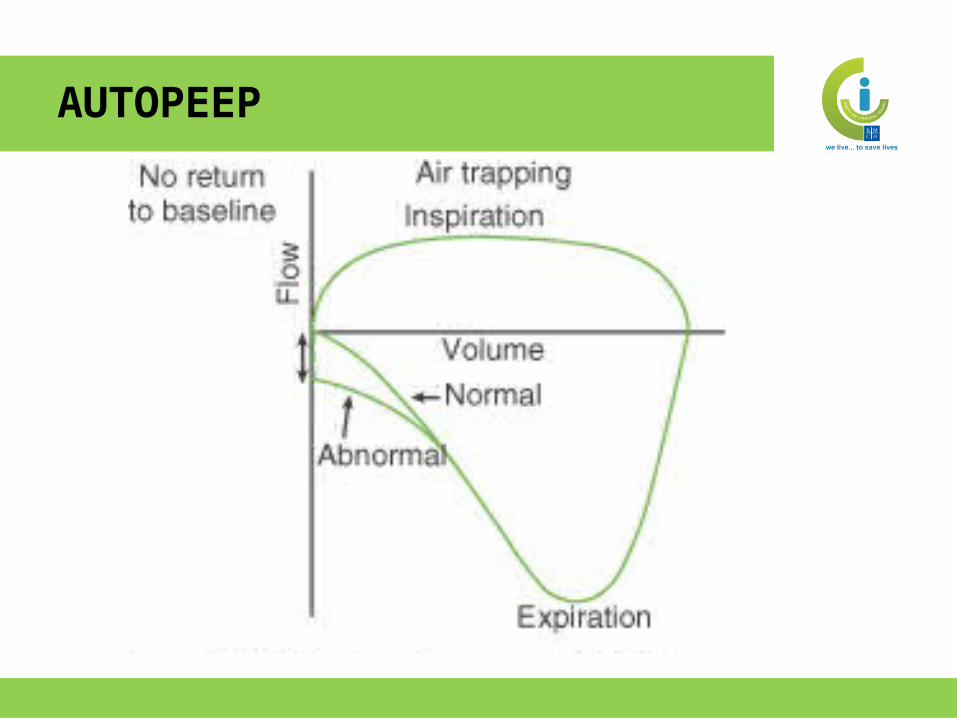
AUTOPEEP

2
1
1
2
3
3
VLPS
.VT
INSP
EXH
BEFORE AFTER
2
1
1
2
3
3
VLPS
.
BRONCHODILATOR RESPONSE
• Identify mode
• Detect auto-PEEP
• Determine patient-ventilator synchrony
• Assess and adjust trigger levels
• Measure the work of breathing
• Adjust tidal volume and minimize
overdistension
• Assess the effect of bronchodilator admn.
USES
• Detect equipment malfunctions
• Determine appropriate PEEP level
• Evaluate adequacy of inspiratory time in
pressure control ventilation
• Detect the presence and rate of continuous leaks
• Determine appropriate Rise Time
USES

No monitoring device, no matter how
simple or complex, invasive or non-
invasive, inaccurate or precise will
improve outcome unless coupled to a
treatment, which itself improves
outcome

Thank you

















