39
4 Description of Selected Tropical Diseases
4Description of Selected
Tropical Diseases
Contents
Page
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Malaria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Aspects of Natural History . . . . . . . . . . . . 59Malaria Control . . . . . . . . . . . . . . . . . . . . . . 61Recent Progress . . . . . . . . . . . . . . . . . . . . 64Research Needs . . . . . . . . . . . . . . . . . . . . . . 65
Schistosomiasis. . . . . . . . . . . . . . . . . . . . . . . . . 65Aspects of Natural History . . . . . . . . . . . . 65Interventions. . . . . . . . . . . . . . . . . . . . . . . 67Recent Progress . . . . . . . . . . . . . . . . . . . . . . 67
Trypanosomiasis . . . . . . . . . . . . . . . . . . . . . . 67African Sleeping Sickness . . . . . . . . . . . . . 69Chagas’ Disease . . . . . . . . . . . . . . . . . . . . . . 71
Leishmaniasis . . . . . . . . . . . . . . . . . . . . . . . . . 74Aspects of Natural History . . . . . . . . . . . . 74Interventions. . . . . . . . . . . . . . . . . . . . . . 78Recent Progress . . . . . . . . . . . . . . . . . . . . . . 78
Filariasis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78Aspects of Natural History . . . . . . . . . . . . 78Obstacles to Research . . . . . . . . . . . . . . . . . 80
Leprosy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80Aspects of Natural History . . . . . . . . . . . . 80Interventions. . . . . . . . . . . . . . . . . . . . . . . . . 83Recent Progress . . . . . . . . . . . . . . . . . . . . . . 83
Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 84Aspects of Natural History . . . . . . . . . . . . 84Interventions. . . . . . . . . . . . . . . . . . . . . . . . . 84Recent Progress . . . . . . . . . . . . . . . . . . . . . . 85
Diarrhea] and Enteric Diseases . . . . . . . . . . . 85Aspects of Natural History . . . . . . . . . . 85Viruses. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86Bacteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86Protozoa and Other Agents.. . . . . . . . . . 88
Acute Respiratory Infections. . . . . . . . . . . . . 88Aspects of Natural History . . . . . . . . . . . . 88Viruses. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89Bacteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89Other ARI Agents. . . . . . . . . . . . . . . . . . . . 90Interventions. . . . . . . . . . . . . . . . . . . . . . . . . 90Biotechnology and ARIs . . . . . . . . . . . . . . 91
Arboviral and Related Viral Infections . . . . 91Aspects of Natural History . . . . . . . . . . . . 91Research Needs . . . . . . . . . . . . . . . . . . . . . . 94
TABLETable No, Page4-1. Location in This Report of lnformation
About Selected Tropical Diseases . . . . . 60
Figure4-1.
4-2.
4-3.
4-4.
4-5.
4-6.
4-7.
4-8.
4-9.
4-1o
4-11.
4-12.
4-13.
4-14.4-15.
4-16.
4-17.
LIST OF FIGURESNo. Page
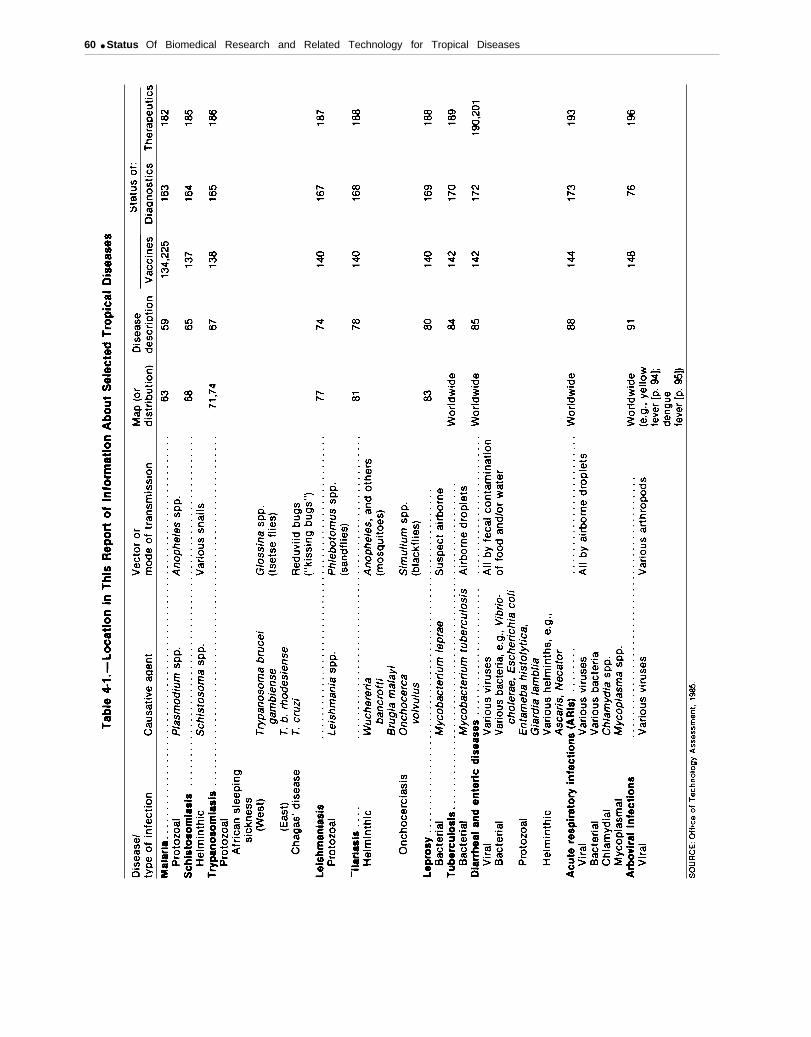
Generalized Life Cycle of Plasmodium,the Cause of Malaria . . . . . . . . . . . . . .Geographic Distribution of Malariaasof 1982 . . . . . . . . . . . . . . . . . . . . . . . , .Geographic Distribution ofChloroquine-Resistant Malaria asof 1983 . . . . . . . . . . . . . . . . . . . . . . . . . .Generalized Life Cycle of Schistosorna,the Cause of Schistosomiasis. . . . . . . .Geographic Distribution ofSchistosomiasis: Schistosomahaematobium, S. mansoni and S.japonicum . . . . . . . . . . . . . . . . . . . . . . . .Generalized Life Cycle of Trypanosomabruceigambiense and T.b. rhodesiense,the Causes of African Sleeping SicknessGeographic Distribution of AfricanSleeping Sickness . . . . . . . . . . . . . . . . . .Life Cycle of Trypanosoma cruzi theCause of Chagas’ Disease . . . . . . . . . . .Geographic Distribution ofChagas’ Disease . . . . . . . . . . . . . . . . . . .Generalized Life Cycle of leishmania,the Cause of Leishmaniasis . . . . . . . . .Geographic Distribution ofLeishmaniasis Caused by Four Speciesof Leishmania . . . . . . . . . . . . . . . . . . . . .Generalized Life Cycle of TwoImportant Filarial Worms: Wuchereriabancrofti and Brugia malayi . . . . . . . .Geographic Distribution of MajorFilarial Diseases: Infection WithOnchocerca volvulus, Brugia malayi,and Wuchereria bancrofti . . . . . . . . . .Geographic Distribution of Leprosy..Generalized Transmission Cycle ofan Arbovirus . . . , . . . , . . . . . . . . . . . .Geographic Distribution ofYellow Fever. . . . . . . . . . . . . . . . . . . . . .Geographic Distribution ofDengue Fever . . . . . . . . . . . . . . . . . . . . .
62
63
64
66
68
70
71
73
74
76
77
79
8183
92
93
94

4.Description of Selected Tropical Disease
INTRODUCTIONThis chapter describes the major tropical dis-
eases that are discussed in this report. The dis-eases considered are a rather diverse group.
Representing the diseases traditionally consid-ered “tropical” in this report are malaria, schis-tosomiasis, trypanosomiasis, leishmaniasis, filar-iasis, and leprosy. These are the six diseasessingled out for attention by the Special Programfor Research and Training in Tropical Diseases(TDR), which is sponsored jointly by the U.N.Development Program, the World Bank, and theWorld Health Organization (WHO). The six TDRdiseases together affect between 700 million and800 million people worldwide. Malaria, schisto-somiasis, and filariasis each affects more than 200million people.
Other diseases discussed in this report—tuber-culosis, diarrheal diseases, acute respiratory in-fections (ARIs), and arboviral infections—occurin nontropical countries as well as tropical ones.The toll these diseases take in developing coun-tries is much greater than the toll they take in thedeveloped world because of developing countries’higher incidence rates and poorer diagnostic andtherapeutic methods.
Tuberculosis was once a public health problemworldwide. It now persists mainly in developingcountries, where it infects large numbers ofpeople.
Diarrheal diseases and ARIs are the leadingcauses of death among infants and children in de-veloping countries. In countries where the infant
mortality rate is more than 100 per 1,000 livebirths, at least one-third of infant deaths are fromdiarrheal diseases.
Arboviral infections have a worldwide distri-bution, but are concentrated in the tropics. Withno specific treatments available and a vaccineagainst only two (yellow fever and Japanese en-cephalitis), arboviral infections are a potentialthreat to the U.S. population.
These are far from the only health problems intropical developing countries. In addition to be-ing affected by the often debilitating infectious dis-eases discussed here, people in the developingworld are increasingly affected by the chronic dis-eases that cause so much sickness and death inthe developed world: heart disease, cancer, stroke,and diabetes, for instance. Ironically, thesechronic diseases increase in incidence as life ex-pectancy increases and as the probability of dy-ing from infectious diseases decreases.
This chapter provides basic information abouteach of the diseases considered in the later chap-ters of this report. Chapter 5 discusses strategiesfor controlling tropical diseases, and chapters 6through 9 examine the status of disease controlmeasures: vector control technologies, immuni-zation technologies, diagnostic technologies, andtherapeutic technologies. Table 4-1 summarizessome basic information about each disease andguides the reader to the relevant sections, for eachdisease, in the remainder of the report.
MALARIAAspects of Natural History is no question that malaria is the most impor-
tant of all infectious diseases.In 1940, the Nobel Laureate Sir Macfarlane
Burnet wrote (37):His statement still holds true. Malaria is one ofthe most studied of all tropical diseases. The dis-
If we take as our standard of importance the ease is caused by various species of the protozoangreatest harm to the greatest number, then there genus Plasmodium . Malaria parasites have a com-
59
60 ● Status Of Biomedical Research and Related Technology for Tropical Diseases

Ch. 4—Description of Selected Tropical Diseases Ž 61
plex life cycle, alternating between vertebratehosts and mosquito vectors of the genus Anopheles.
Four species of Plasmodium cause malaria inhumans: Plasmodium falciparum, P. vivax, P.ovale, and P. malariae. Other species of Plasmo-dium infect a wide variety of other vertebrates.
The four species that infect humans have some-what different clinical effects. P. falciparum cancause severe anemia, kidney failure, and braindamage and is often fatal, especially in children.P. vivax and P. ovale infections are seldom fa-tal, but relapses of the symptoms (chills, high fe-ver, nausea, headache, etc. ) can occur periodicallyfor up to 3 years. P. malariae infections can per-sist in the blood for years without causing anysymptoms.
Life Cycle
All species of Plasmodium progress through asimilar life cycle, though each species differs insome of the details. All human malaria infectionbegins with the bite of an infected female Anophelesmosquito (see fig. 4-l). As the mosquito ingestsa blood meal to nourish her eggs, she incidentallyinjects saliva containing plasmodial sporozoites(which have been clustered in the mosquito’s sal-ivary glands) into the human bloodstream.
Within about an hour, the threadlike sporo-zoites leave the bloodstream and move to the hu-man liver. Over the next week or two, depend-ing on the species of Plasmodium, each sporozoitethat has invaded a liver cell becomes a schizont,a developmental stage that contains thousands ofmerozoites, the next stage in the life cycle of theparasite. When the schizont matures, it rupturesout of the infected liver cell and dischargesmerozoites into the human host’s bloodstream.In P. vivax and P. ovale malaria, some sporo-zoites, instead of developing into shizonts, becomehypnozoites, forms that can remain dormant inthe liver for months or years before they start toproliferate.
Merozoites invade red blood cells (erythrocytes)and there undergo a second round of asexual re-production, similar to that in the liver. In 2 or3 days, the merozoites develop into trophozoites,then into a second dividing schizont form. When
the schizonts mature, they rupture and releaseanother round of merozoites, perpetuating the cy-cle of infection. It is at the time of this rupturethat clinical symptoms of malaria appear. The cy-cle repeats every 2 or 3 days, depending on thespecies of Plasmodium.
Some merozoites, instead of developing intoschizonts, differentiate into sexual forms, gameto-cytes. Mature gametocytes remain in the host’sred blood cells, and can be ingested by femaleAnopheles when they bite. Gametocytes developfurther into male and female gametes, whichundergo sexual reproduction in the mosquito’sgut. Eventually a new generation of sporozoitesdevelops in the mosquito and migrates to themosquito’s salivary glands, ready to infect anotherhuman.
Incidence and Prevalence
Malaria is one of the most widespread and de-structive of diseases, having doubled in worldprevalence in the last decade (430). Worldwide,an estimated 250 million to 300 million cases ofmalaria occur each year. In tropical Africa alone,an estimated 160 million to 200 million people areinfected every year, and 1 million people die,mostly infants and small children (193).
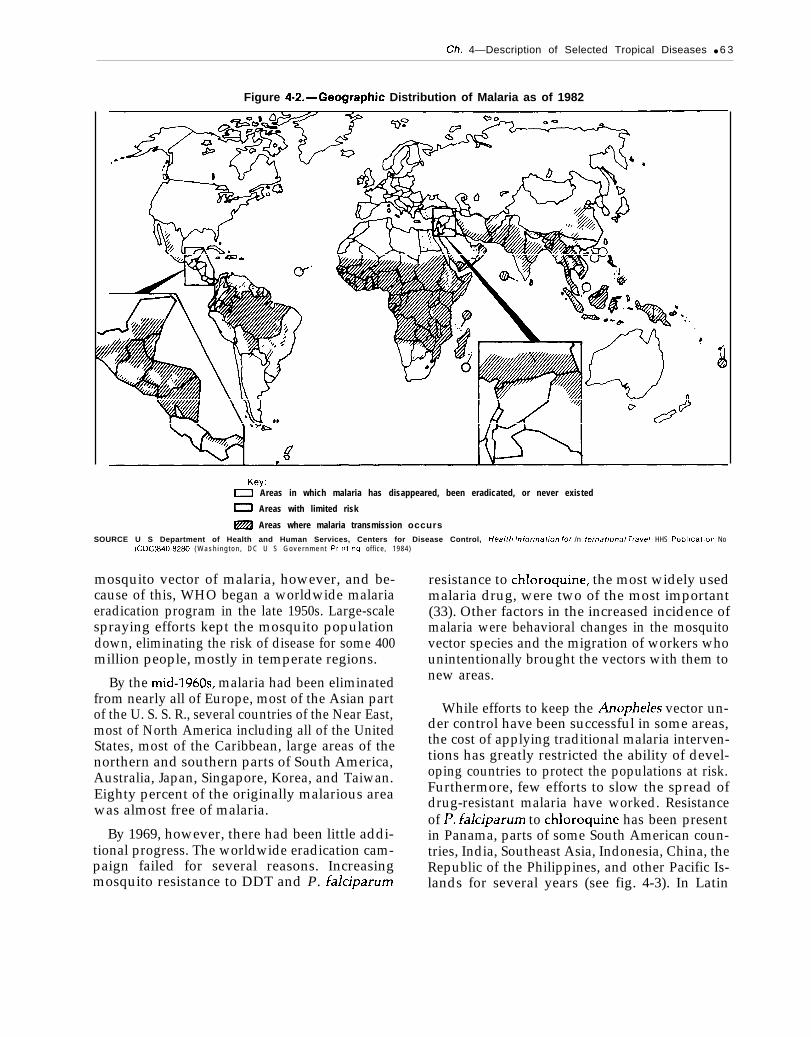
About 1.5 billion people live in areas of theworld where the risk of malaria ranges from mod-erate to high (see fig. 4-2). The countries of high-est malaria incidence are Haiti, Guatemala, Hon-duras, El Salvador, Colombia, Bolivia, Brazil,India, Sri Lanka, Pakistan, and many parts ofAfrica and Asia. In Europe, the Caribbean, NorthAmerica, and parts of South America, and Aus-tralia, the gains against malaria brought about bythe WHO eradication program (see discussion be-low) have been maintained. However, developednations such as England and the United Stateshave experienced an increase in the number of im-ported malaria cases.
Malaria Control
Before World War II, approximately two-thirdsof the worlds population was at risk for malaria.DDT (dichloro-diphenyl-trichloro-ethane) was ini-tially highly successful at controlling the Anopheles
62 ● Status of Biomedical Research and Related Technology for Tropical Diseases
0
o
c
Ch. 4—Description of Selected Tropical Diseases ● 6 3
Figure 4“2.–Geographic Distribution of Malaria as of 1982
Key:O Areas in which malaria has disappeared, been eradicated, or never existed
o Areas with limited risk
~ Areas where malaria transmission occursSOURCE U S Department of Health and Human Services, Centers for Disease Control, Hea/th /nforrnat/orr for /n fernaf/ona/ Trave/. HHS Publlcatlon No
(CDC)840-8280 ( W a s h i n g t o n , D C U S G o v e r n m e n t Prlntlng off ice, 1984)
mosquito vector of malaria, however, and be-cause of this, WHO began a worldwide malariaeradication program in the late 1950s. Large-scalespraying efforts kept the mosquito populationdown, eliminating the risk of disease for some 400million people, mostly in temperate regions.
By the mid-1960s, malaria had been eliminatedfrom nearly all of Europe, most of the Asian partof the U. S. S. R., several countries of the Near East,most of North America including all of the UnitedStates, most of the Caribbean, large areas of thenorthern and southern parts of South America,Australia, Japan, Singapore, Korea, and Taiwan.Eighty percent of the originally malarious areawas almost free of malaria.
By 1969, however, there had been little addi-tional progress. The worldwide eradication cam-paign failed for several reasons. Increasingmosquito resistance to DDT and P. falciparum
resistance to chloroquine, the most widely usedmalaria drug, were two of the most important(33). Other factors in the increased incidence ofmalaria were behavioral changes in the mosquitovector species and the migration of workers whounintentionally brought the vectors with them tonew areas.
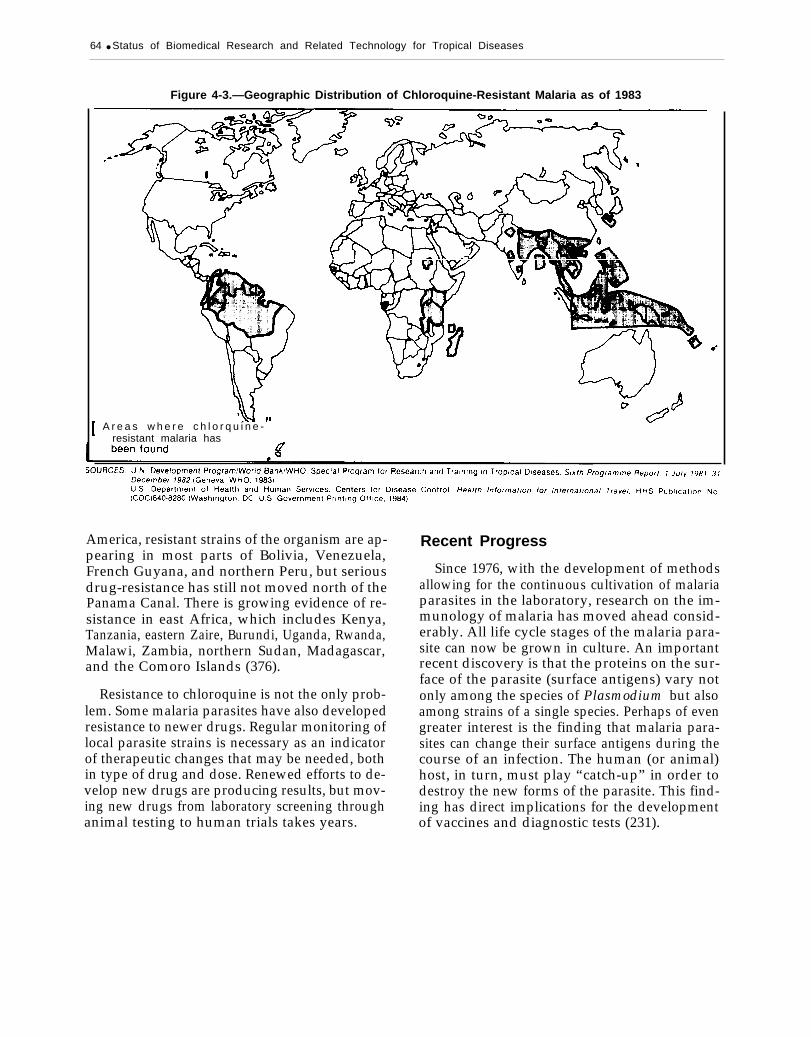
While efforts to keep the Anopheles vector un-der control have been successful in some areas,the cost of applying traditional malaria interven-tions has greatly restricted the ability of devel-oping countries to protect the populations at risk.Furthermore, few efforts to slow the spread ofdrug-resistant malaria have worked. Resistanceof P. falciparum to chloroquine has been presentin Panama, parts of some South American coun-tries, India, Southeast Asia, Indonesia, China, theRepublic of the Philippines, and other Pacific Is-lands for several years (see fig. 4-3). In Latin
64 ● Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-3.—Geographic Distribution of Chloroquine-Resistant Malaria as of 1983
A r e a s w h e r e c h l o r q u i n e -resistant malaria has
America, resistant strains of the organism are ap-pearing in most parts of Bolivia, Venezuela,French Guyana, and northern Peru, but seriousdrug-resistance has still not moved north of thePanama Canal. There is growing evidence of re-sistance in east Africa, which includes Kenya,Tanzania, eastern Zaire, Burundi, Uganda, Rwanda,Malawi, Zambia, northern Sudan, Madagascar,and the Comoro Islands (376).
Resistance to chloroquine is not the only prob-lem. Some malaria parasites have also developedresistance to newer drugs. Regular monitoring oflocal parasite strains is necessary as an indicatorof therapeutic changes that may be needed, bothin type of drug and dose. Renewed efforts to de-velop new drugs are producing results, but mov-ing new drugs from laboratory screening throughanimal testing to human trials takes years.
Recent Progress
Since 1976, with the development of methodsallowing for the continuous cultivation of malariaparasites in the laboratory, research on the im-munology of malaria has moved ahead consid-erably. All life cycle stages of the malaria para-site can now be grown in culture. An importantrecent discovery is that the proteins on the sur-face of the parasite (surface antigens) vary notonly among the species of Plasmodium but alsoamong strains of a single species. Perhaps of evengreater interest is the finding that malaria para-sites can change their surface antigens during thecourse of an infection. The human (or animal)host, in turn, must play “catch-up” in order todestroy the new forms of the parasite. This find-ing has direct implications for the developmentof vaccines and diagnostic tests (231).

Ch. 4—Description of Selected Tropical Diseases . 65
Basic malaria research has advanced consider-ably. Metabolic studies have identified parasite-specific enzyme pathways that can be exploitedto kill the malaria parasite without harming thehuman host. Membrane research has revealedhow the parasite finds, attaches to, and invadesthe human host’s red blood cells, yielding impor-tant clues for drug therapy and vaccine research.Recent clinical studies have suggested better waysof preventing and treating cerebral malaria, anoften fatal complication of severe malaria in-fection.
A vaccine against the sporozoite stage of ma-laria may be available for testing by 1986. Vac-cines against the merozoite and the gamete stagesare behind this in development. If animal testingin humans confirms the feasibility of immuniza-tion against the malaria parasite, extensive humanand field trials will be required before the vac-cine can be widely used. Furthermore, given thedifficulties that have plagued other disease immu-nization campaigns there is some debate about the
SCHISTOSOMIASISAspects of Natural History
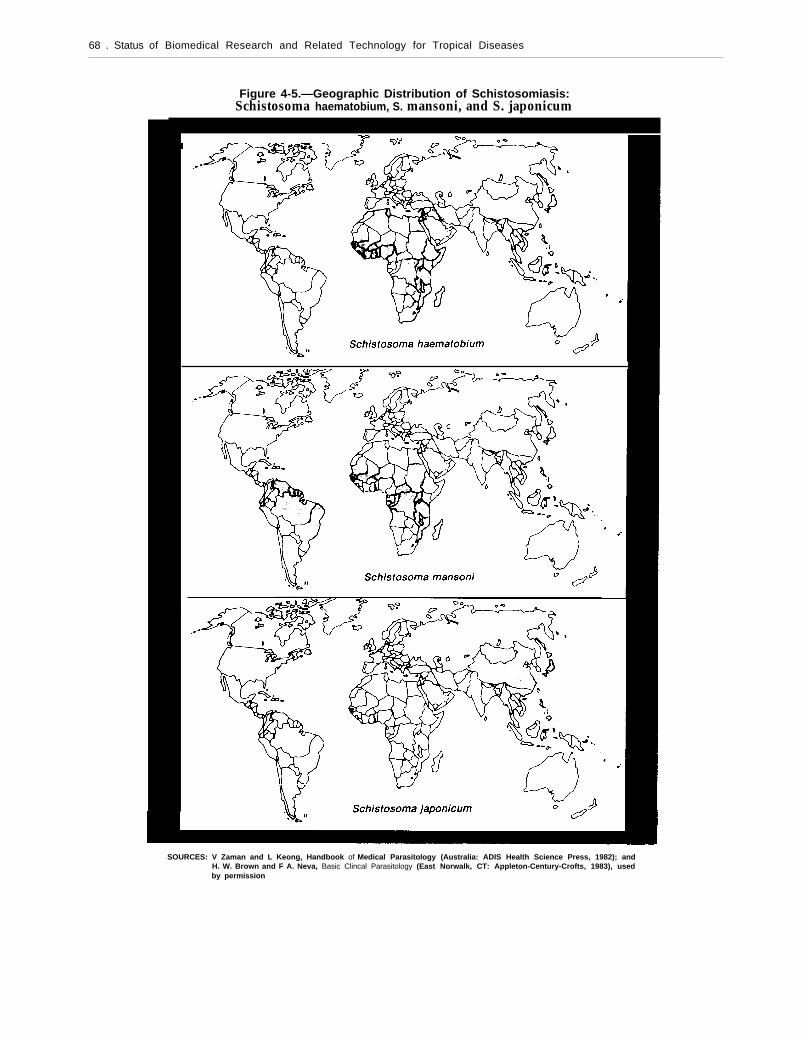
Schistosomiasis is a debilitating disease causedby trematode worms of the genus Schistosorna.There are three major species affecting humans,Schistosoma mansoni, S. haematobium, and S.japonicum, all of which originated in the OldWorld but now occur worldwide. S. mansonioriginated in Africa, but now has become estab-lished in the Americas. A fourth species, S.mekongi, was discovered in the late 1960s and isendemic in areas of Southeast Asia.
Life Cycle
The adult parasitic worms that cause schisto-somiasis live in pairs in the human host’s blood-stream, sometimes for many years. Eggs (from afew hundred to several thousand per day) areproduced by the female schistosome and are de-posited in the host’s blood vessels. The eggs es-cape into the host’,s bowel (S. mansoni, S. japoni-cum) or bladder (S. haematobium), and then areexcreted in feces or urine. If the eggs become
usefulness of a malaria vaccine (see Case StudyB: The Development of a Malaria Vaccine for amore comp
Research
ete discussion).
Needs
Field- and community-based studies are neededto assess the impact of antimalarial interventions.The emergence of insecticide-resistant mosquitovectors of malaria has seriously handicapped cur-rent malaria control efforts, making studies of theecological impact of future interventions criticallyimportant. The effect of antimalarial activities onthe actual immunity levels of populations needsclarification. Studies in the past have clearly doc-umented the immediate impact of antimalarialprojects on morbidity and mortality, but not thelong-term consequences when projects cease orfail. Other studies are needed to evaluate the im-portance of sociological and human behavioralfactors and the usefulness of health education,community self-help, and volunteer collaborators.
trapped in the human host’s bladder or liver, how-ever, granulomas (masses of small blood vesselsand connective tissue) form around them, and theeggs eventually die and calcify, producing inflam-mation and scars. The damage done by schisto-somiasis is primarily due to the human body’s re-action to accumulated eggs and their associatedgranulomas.
The schistosome eggs that are excreted by thehost into freshwater lakes or streams hatch intociliated larval worms (miracidia). Miracidia thenenter an intermediate snail host, in which theyproliferate. Immature worms (cercariae) are re-leased from the snail and can rapidly penetratethe unbroken skin of persons who enter infectedwater (see fig. 4-4). The tailless immature worms(now called shistosomules) enter the human cir-culatory system and proceed to the liver, wherethey mature. As they mature, they coat their sur-faces with proteins acquired from their humanhosts, which enable them to fool the hosts’ im-mune system into tolerating their presence (130).After emerging from the liver, mature worms

66 . Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-4.—Generalized Life Cycle of Schistosoma, the Cause of Schistosomiasis
Excretedin feces
l \4
Excreted
1. Microscopic cercariae are released from snail intermediate host.2. Cercariae penetrate skin of human host.3. Tailless cercariae, now called schistosomules, migrate to the human host’s small blood vessels, are carried to lungs, then
through the heart into the liver to mature; paired (male and female) mature schistosomes lodge in the human host’s veins(S. mansoni shown).
4. Female schistosomes continually produce eggs (up to thousands each day), which penetrate the human host’s intestine(S. mansoni and S. japonicum) or the urinary bladder (S. haernatobium), from which they are excreted in feces or urine,respectively.
5. Eggs hatch in fresh water into ciliated miracidia.6. Miracidia penetrate intermediate snail host, lose cilia, and become sporocysts. Sporocysts reproduce asexually in the snail,
proliferating greatly, eventually giving rise to cercariae.SOURCES Adapted from T C Cheng. Symbiosis (New York Pegasus, 1970), and E R Noble and G A Noble Parasitology. 3d ed (philadelphia Lea & Febiger. 1973)

Ch. 4—Description of Selected Tropical Diseases . 67
mate for life within small veins around either thebowel or bladder area, thus completing the par-asite’s life cycle.
Incidence
A worldwide survey in 1972 (including 71 coun-tries) estimated that 500 million people were ex-posed to infection by schistosomiasis and 125 mil-lion were infected (169). The various forms of thisdisease occur in parts of Africa, the Caribbean,South America, and the Orient (see fig. 4-5). InLatin America, recorded schistosomiasis incidenceis highest in Surinam, where 385 of every 100,000inhabitants were infected in 1980 (265). S. man-soni is also established in suitable snail hosts inmore than half of Brazil, where 10 million peo-ple are believed infected, and in parts of Vene-zuela, where 10,000 more people are thought tohave the disease. Foci in the Caribbean occur inthe Dominican Republic, Guadaloupe, Mar-tinique, and St. Martin. A few cases have beendetected in Montserrat.
Interventions
Over the last 10 years, the incidence and prev-alence of schistosomiasis have dropped consider-ably in several countries. In Japan, the prevalencedropped from 25 percent in 1950 to less than 1percent in 1973 (169). This formidable decreasewas brought about by the concrete lining of irri-gation ditches, snail control, land reclamation,environmental sanitation, chemotherapy, andhealth education. Similar decreases reported forsome parts of Egypt, Iran, Puerto Rico, Tunisia,and Venezuela were brought about by more or
TRYPANOSOMIASISTrypanosomiasis is a general term for two sep-
arate diseases caused by protozoan parasites ofthe genus Trypanosoma. Trypanosoma brucei in-fections cause African sleeping sickness (alsocalled African trypanosomiasis), and T. cruzi in-fections cause Chagas’ disease (also called Amer-ican trypanosomiasis). The two diseases have
less the same combination of control methods andimproved socioeconomic conditions (169). On theminus side, schistosomiasis has spread to newareas as a result of water impoundment and irri-gation projects which create and expand suitableenvironmental conditions for snail hosts and in-crease human-snail contact. Areas where largehydroelectric dams are being built, especially inSouth America, may require special surveillanceand assessment.
Chemotherapy against schistosomiasis with thenewest generation of chemotherapeutic agents iseffective and relatively safe. However, total andcomplete control in endemic areas is difficult toachieve, since it requires attention to other meas-ures, particularly water supply and sanitation,and treatment of snail breeding sites (mollusci-ciding).
Recent Progress
A fairly large corps of American researchersstudies schistosomiasis, and about a dozen lab-oratories use the techniques of biotechnology. Thelife cycle of the schistosomiasis parasite is read-ily adaptable to the laboratory, and small rodentsare easily infected. The immunology of schisto-somiasis has been studied extensively (39). Mostworkers are attempting to identify and isolate rele-vant protective antigens, and many are activelyengaged in gene cloning experiments. A live ir-radiated larval vaccine has been used in cattle inthe Sudan with encouraging results (338), but itsuse in humans is not feasible, because the larvaeare alive (though unable to continue their lifecycle) when injected.
completely different transmission cycles, differ-ent vectors, and cause a different pathology. Cha-gas’ disease begins as a blood infection but ulti-mately attacks various body organs, principally
the heart, African sleeping sickness also begins as
a blood infection but progresses to central nerv-ous system disease and death,
68 . Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-5.—Geographic Distribution of Schistosomiasis:Schistosoma haematobium, S. mansoni, and S. japonicum
SOURCES: V Zaman and L Keong, Handbook of Medical Parasitology (Australia: ADIS Health Science Press, 1982); andH. W. Brown and F A. Neva, Basic Clincal Parasitology (East Norwalk, CT: Appleton-Century-Crofts, 1983), usedby permission

Ch. 4—Description of Selected Tropical Diseases ● 6 9
African Sleeping Sickness(African Trypanosomiasis)
Aspects of Natural History
T. brucei, the agent of African sleeping sick-ness in humans and nagana in livestock, is en-demic to large areas of the African continent butdoes not occur naturally outside of Africa. In theUnited States, there have been six published re-ports of imported cases of African sleeping sick-ness since 1967. All the infected travelers had beenon vacation in game parks in eastern or southernAfrica, where they were exposed to the tsetse flyvector. The tsetse fly vector of African sleepingsickness is not found in the United States, so thereis little danger that the disease will become estab-lished in this country (368).
Life Cycle.—There are actually two kinds ofAfrican sleeping sickness, each caused by a differ-ent variety of T. brucei and occurring in its ownenvironmental niche. Both forms of the diseasehave an early stage involving the blood and lym-phatic system and a late stage involving the brain.
In west Africa, sleeping sickness is caused bythe parasite T. brucei gambiense, which is trans-mitted by tsetse flies (Glossina palpalis) that feedonly on humans. The disease is transmitted nearstreams where tsetse flies breed. T. b. gambienseinfection usually results in a chronic condition thatslowly leads to death.
In east Africa, sleeping sickness is actually azoonosis (a disease of animals that can be trans-mitted to humans) caused by T. b. rhodesienseand transmitted by a different species of tsetse fly(G. morsitans). Humans acquire the disease whenthey venture into areas, such as hunting groundsand grazing lands, where animals are infected.The disease is fatal to humans within weeks ormonths and very destructive to livestock. Largeexpanses of land have become totally unusablebecause of the disease risk to humans enteringthem.
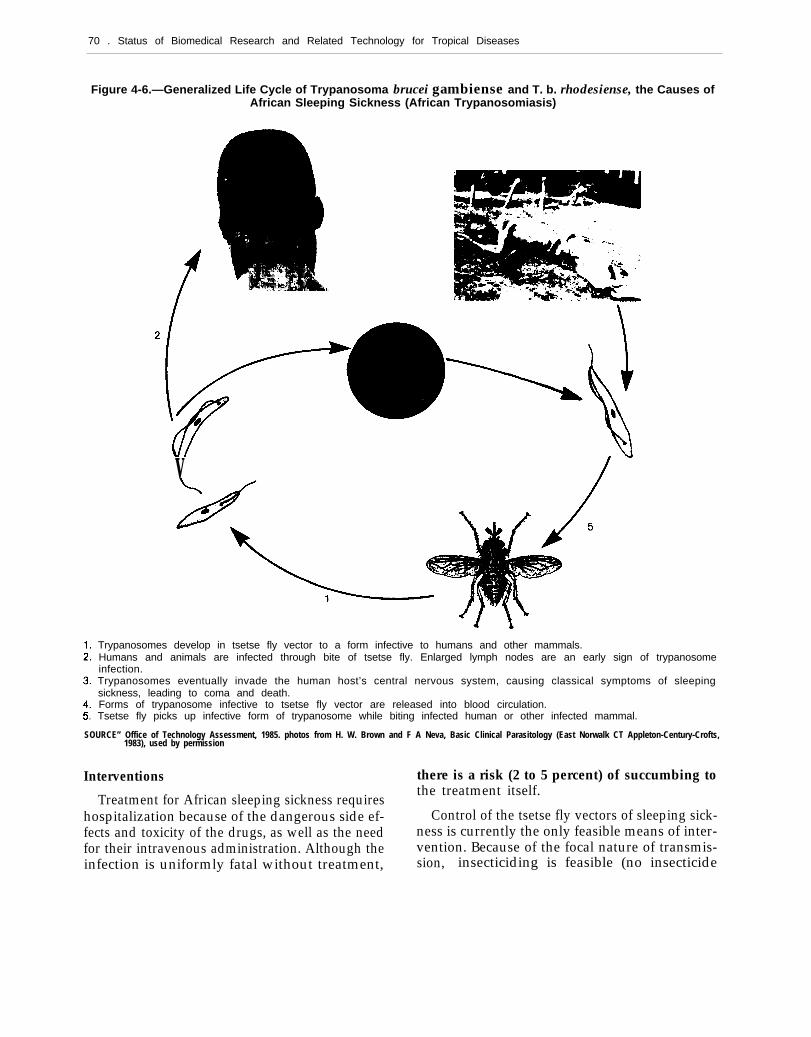
Either form of African sleeping sickness beginswhen an infected tsetse fly feeds on a human oranimal host, depositing trypanosomes in thewound (see fig. 4-6). The trypanosomes invade
the host’s blood, lymph, and tissue fluids. In cy-clical waves, the trypanosomes wane, then re-appear, as the body’s immune system and theparasites interact. These parasites can undergo fre-quent changes in a specific surface protein, knownas variant surface glycoprotein (VSG) or variantsurface antigen. Located on the blood form of thetrypanosome, VSGS stimulate the production bythe host of a particular responsive and protectiveantibody.
Within any individual human or animal host,the VSGS of the trypanosome population shiftover time through a repertoire of changes num-bering potentially over 100, each having no ex-posed determinants in common with other pastor future populations. Two distinct mechanismsappear to be responsible for the VSG changes,which are called antigenic switching. Each mech-anism generates cohorts of parasites to which themammalian host has not yet made antibody.Since antibodies raised against one variant aregenerally not effective against other variants, thetrypanosome is able to evade the host’s immuneresponse.
Until the host can mount another antibody re-sponse, symptoms of fever, headache, and jointpain occur. As the infection progresses, lesionsdevelop in the brain, heart, and small blood ves-sels. Ultimately, nervous system involvementdevelops, first with signs of insomnia and excita-bility, then coma and death. Symptoms and out-come are similar in both the acute and chronicforms, but the duration differs.
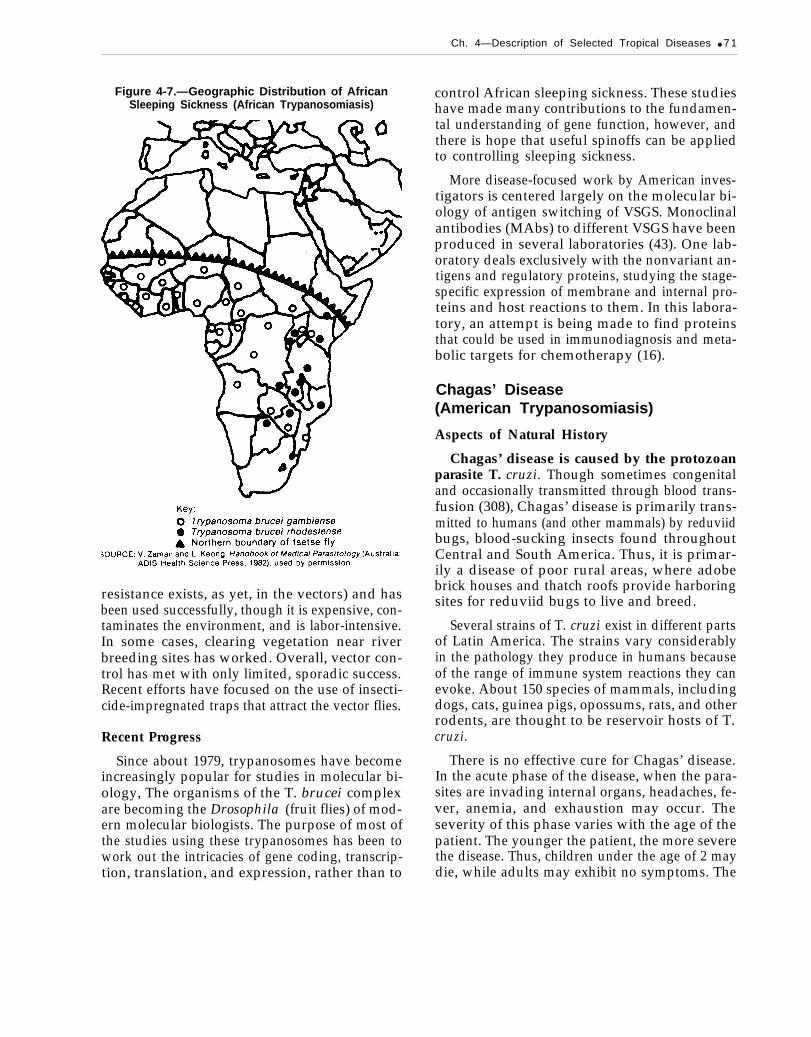
Incidence.—Recent estimates put 45 millionpeople at risk of sleeping sickness infection inAfrica. Until 1979, about 10,000 new cases wererecorded annually, but since then, serious out-breaks have resulted in more than 20,000 newcases recorded per year (353). Because of the dif-ficulties of diagnosing chronic cases and the usualoccurrence of the disease in rural areas, thesefigures are probably underestimates. Althoughwidespread across Africa (see fig. 4-7), sleepingsicknesss occurs in well-defined endemic foci be-cause the tsetse fly vectors breed in rivers andstreams. Unfortunately, those same water sourcesare essential to humans and grazing animals.
70 . Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-6.—Generalized Life Cycle of Trypanosoma brucei gambiense and T. b. rhodesiense, the Causes ofAfrican Sleeping Sickness (African Trypanosomiasis)
v
Trypanosomes develop in tsetse fly vector to a form infective to humans and other mammals.Humans and animals are infected through bite of tsetse fly. Enlarged lymph nodes are an early sign of trypanosomeinfection.Trypanosomes eventually invade the human host’s central nervous system, causing classical symptoms of sleepingsickness, leading to coma and death.Forms of trypanosome infective to tsetse fly vector are released into blood circulation.Tsetse fly picks up infective form of trypanosome while biting infected human or other infected mammal.
SOURCE” Office of Technology Assessment, 1985. photos from H. W. Brown and F A Neva, Basic Clinical Parasitology (East Norwalk CT Appleton-Century-Crofts,1983), used by permission
Interventions there is a risk (2 to 5 percent) of succumbing to
Treatment for African sleeping sickness requiresthe treatment itself.
hospitalization because of the dangerous side ef- Control of the tsetse fly vectors of sleeping sick-fects and toxicity of the drugs, as well as the need ness is currently the only feasible means of inter-for their intravenous administration. Although the vention. Because of the focal nature of transmis-infection is uniformly fatal without treatment, sion, insecticiding is feasible (no insecticide
Ch. 4—Description of Selected Tropical Diseases ● 7 1
Figure 4-7.—Geographic Distribution of AfricanSleeping Sickness (African Trypanosomiasis)
resistance exists, as yet, in the vectors) and hasbeen used successfully, though it is expensive, con-taminates the environment, and is labor-intensive.In some cases, clearing vegetation near riverbreeding sites has worked. Overall, vector con-trol has met with only limited, sporadic success.Recent efforts have focused on the use of insecti-cide-impregnated traps that attract the vector flies.
Recent Progress
Since about 1979, trypanosomes have becomeincreasingly popular for studies in molecular bi-ology, The organisms of the T. brucei complexare becoming the Drosophila (fruit flies) of mod-ern molecular biologists. The purpose of most ofthe studies using these trypanosomes has been towork out the intricacies of gene coding, transcrip-tion, translation, and expression, rather than to
control African sleeping sickness. These studieshave made many contributions to the fundamen-tal understanding of gene function, however, andthere is hope that useful spinoffs can be appliedto controlling sleeping sickness.
More disease-focused work by American inves-tigators is centered largely on the molecular bi-ology of antigen switching of VSGS. Monoclinalantibodies (MAbs) to different VSGS have beenproduced in several laboratories (43). One lab-oratory deals exclusively with the nonvariant an-tigens and regulatory proteins, studying the stage-specific expression of membrane and internal pro-teins and host reactions to them. In this labora-tory, an attempt is being made to find proteinsthat could be used in immunodiagnosis and meta-bolic targets for chemotherapy (16).
Chagas’ Disease(American Trypanosomiasis)
Aspects of Natural History
Chagas’ disease is caused by the protozoanparasite T. cruzi. Though sometimes congenitaland occasionally transmitted through blood trans-fusion (308), Chagas’ disease is primarily trans-mitted to humans (and other mammals) by reduviidbugs, blood-sucking insects found throughoutCentral and South America. Thus, it is primar-ily a disease of poor rural areas, where adobebrick houses and thatch roofs provide harboringsites for reduviid bugs to live and breed.
Several strains of T. cruzi exist in different partsof Latin America. The strains vary considerablyin the pathology they produce in humans becauseof the range of immune system reactions they canevoke. About 150 species of mammals, includingdogs, cats, guinea pigs, opossums, rats, and otherrodents, are thought to be reservoir hosts of T.cruzi.
There is no effective cure for Chagas’ disease.In the acute phase of the disease, when the para-sites are invading internal organs, headaches, fe-ver, anemia, and exhaustion may occur. Theseverity of this phase varies with the age of thepatient. The younger the patient, the more severethe disease. Thus, children under the age of 2 maydie, while adults may exhibit no symptoms. The

72 ● Status of Biomedical Research and Related Technology for Tropical Diseases
Photo credit: H. W. Brown and F. A. Neva, “Basic Clinical Parasitology, “Appleton-Century-Crofts, 1983. Reprinted by permission,
Megacolon, one effect of Chagas’ disease.
acute stage of Chagas’ disease may resolve com-pletely in a few weeks or months or instead maypass into a subacute or chronic stage.
Long-term sequelae of Chagas’ disease includegrotesque enlargement of the digestive tract(megaesophagus and megacolon), circulatoryproblems, and central nervous system damagesand most seriously, damage to the heart muscle,sometimes leading to death from heart failure.
Life Cycle. -T. cruzi infection in humans re-sults when an infected reduviid bug bites a per-son, usually around the eye while the person issleeping, and deposits feces containing 7’. cruziparasites into the bite wound (see fig. 4-8). T. cruzihas two life stages in the mammalian host, onethat circulates in blood and another that prolifer-ates intracellularly within the tissues. Forms of theparasites infective to reduviid bugs are releasedinto the mammalian host’s circulation, ready tobe picked up by reduviid bugs in the course ofanother insect bite.
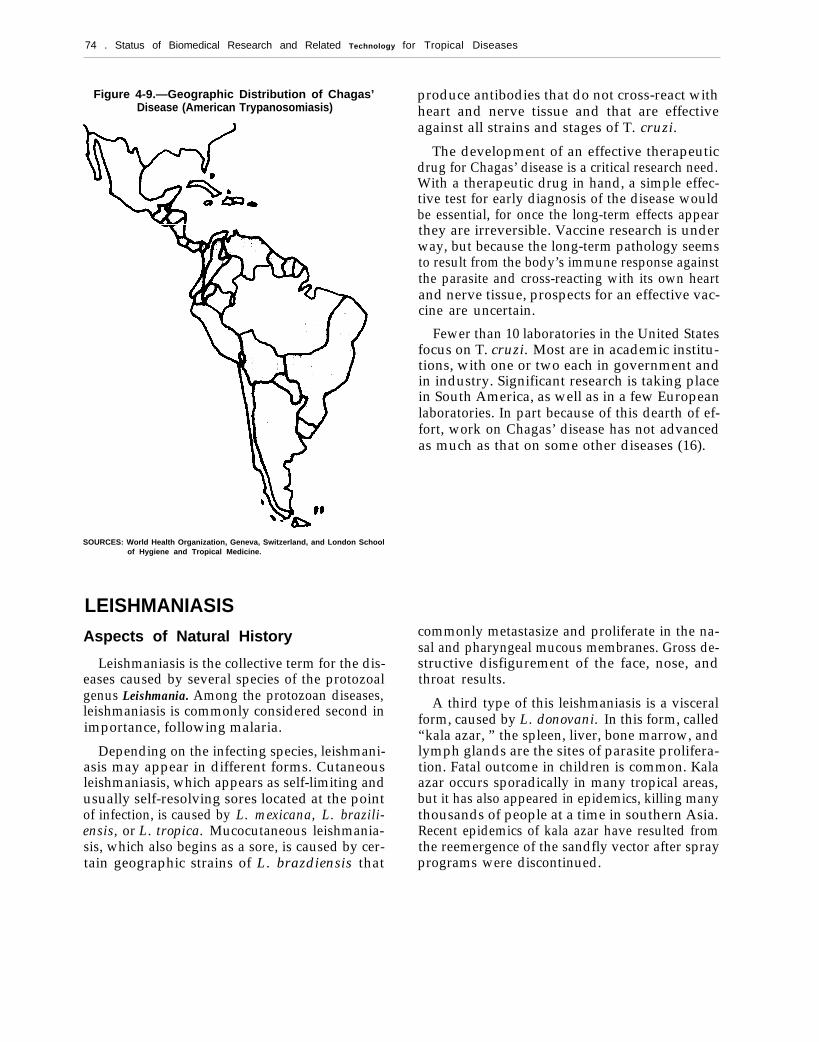
Incidence.—Chagas’ disease occurs in almostevery country of Latin America: Brazil, Peru,Venezuela, Chile, Bolivia, Paraguay, Uruguay,Argentina, Colombia, Mexico, Costa Rica, andPanama (see fig. 4-9) (265). Although the vectorsand reservoir hosts are also present across theSouthern United States, only three indigenouscases of Chagas’ disease have been reported. Twowere infants reported to have contracted the dis-ease in Texas in 1955, and the third was a womanfrom the Sacramento Valley area in California in1982. None of the three had previously had con-tact with pets carrying the disease or had recentblood transfusions or had been outside the coun-try (309).
It has been estimated that about 12 million ofthe 50 million exposed people living in endemicareas are infected with T. cruzi (229). Since notifi-cation of authorities regarding the presence ofChagas’ disease is not compulsory, there are noreliable morbidity data. Studies in Brazil haveshown Chagas’ disease to be a significant causeof mortality in people under 45 years of age (287)and a heavy burden to society because of the needfor hospitalization and disability assistance (268).
Interventions
Control measures for Chagas’ disease concen-trate on insecticide spraying of houses and up-grading of housing construction. In one area ofVenezuela, the use of insecticides was believed toaccount for a significant decline in the percent-age of the population infected with T. cruzi dur-ing the 1970s (29). Vector bionomics remains animportant research topic for defining transmissionareas, vector behavioral characteristics, and im-proved control measures.
Recent Progress
In an attempt to understand why the humanhost’s immune system is not effective in control-ling Chagas’ disease, some investigators have ex-amined the proteins produced by T. cruzi. Thereis no evidence for VSGS in T. cruzi (322), althougha large number of local genetic strains do exist.Some other mechanism must be responsible forT. cruzi’s ability to evade the human immunesystem.
Ch. 4—Description of Selected Tropical
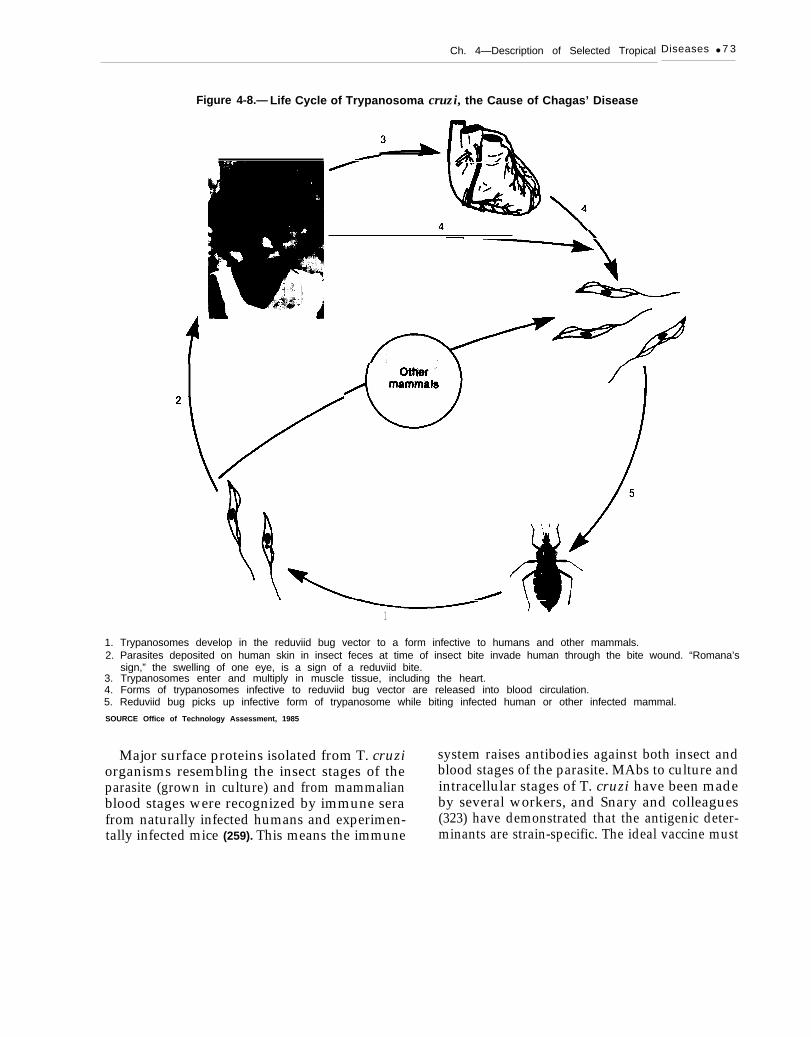
Figure 4-8.— Life Cycle of Trypanosoma cruzi, the Cause of Chagas’ Disease
\
Diseases ● 7 3
1
1. Trypanosomes develop in the reduviid bug vector to a form infective to humans and other mammals.2. Parasites deposited on human skin in insect feces at time of insect bite invade human through the bite wound. “Romana’s
sign,” the swelling of one eye, is a sign of a reduviid bite.3. Trypanosomes enter and multiply in muscle tissue, including the heart.4. Forms of trypanosomes infective to reduviid bug vector are released into blood circulation.5. Reduviid bug picks up infective form of trypanosome while biting infected human or other infected mammal.
SOURCE Office of Technology Assessment, 1985
Major surface proteins isolated from T. cruzi system raises antibodies against both insect andorganisms resembling the insect stages of the blood stages of the parasite. MAbs to culture andparasite (grown in culture) and from mammalian intracellular stages of T. cruzi have been madeblood stages were recognized by immune sera by several workers, and Snary and colleaguesfrom naturally infected humans and experimen- (323) have demonstrated that the antigenic deter-tally infected mice (259). This means the immune minants are strain-specific. The ideal vaccine must
74 . Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-9.—Geographic Distribution of Chagas’Disease (American Trypanosomiasis)
SOURCES: World Health Organization, Geneva, Switzerland, and London Schoolof Hygiene and Tropical Medicine.
LEISHMANIASISAspects of Natural History
Leishmaniasis is the collective term for the dis-eases caused by several species of the protozoalgenus Leishmania. Among the protozoan diseases,leishmaniasis is commonly considered second inimportance, following malaria.
Depending on the infecting species, leishmani-asis may appear in different forms. Cutaneousleishmaniasis, which appears as self-limiting andusually self-resolving sores located at the pointof infection, is caused by L. mexicana, L. brazili-ensis, or L. tropica. Mucocutaneous leishmania-sis, which also begins as a sore, is caused by cer-tain geographic strains of L. brazdiensis that
produce antibodies that do not cross-react withheart and nerve tissue and that are effectiveagainst all strains and stages of T. cruzi.
The development of an effective therapeuticdrug for Chagas’ disease is a critical research need.With a therapeutic drug in hand, a simple effec-tive test for early diagnosis of the disease wouldbe essential, for once the long-term effects appearthey are irreversible. Vaccine research is underway, but because the long-term pathology seemsto result from the body’s immune response againstthe parasite and cross-reacting with its own heartand nerve tissue, prospects for an effective vac-cine are uncertain.
Fewer than 10 laboratories in the United Statesfocus on T. cruzi. Most are in academic institu-tions, with one or two each in government andin industry. Significant research is taking placein South America, as well as in a few Europeanlaboratories. In part because of this dearth of ef-fort, work on Chagas’ disease has not advancedas much as that on some other diseases (16).
commonly metastasize and proliferate in the na-sal and pharyngeal mucous membranes. Gross de-structive disfigurement of the face, nose, andthroat results.
A third type of this leishmaniasis is a visceralform, caused by L. donovani. In this form, called“kala azar, ” the spleen, liver, bone marrow, andlymph glands are the sites of parasite prolifera-tion. Fatal outcome in children is common. Kalaazar occurs sporadically in many tropical areas,but it has also appeared in epidemics, killing manythousands of people at a time in southern Asia.Recent epidemics of kala azar have resulted fromthe reemergence of the sandfly vector after sprayprograms were discontinued.
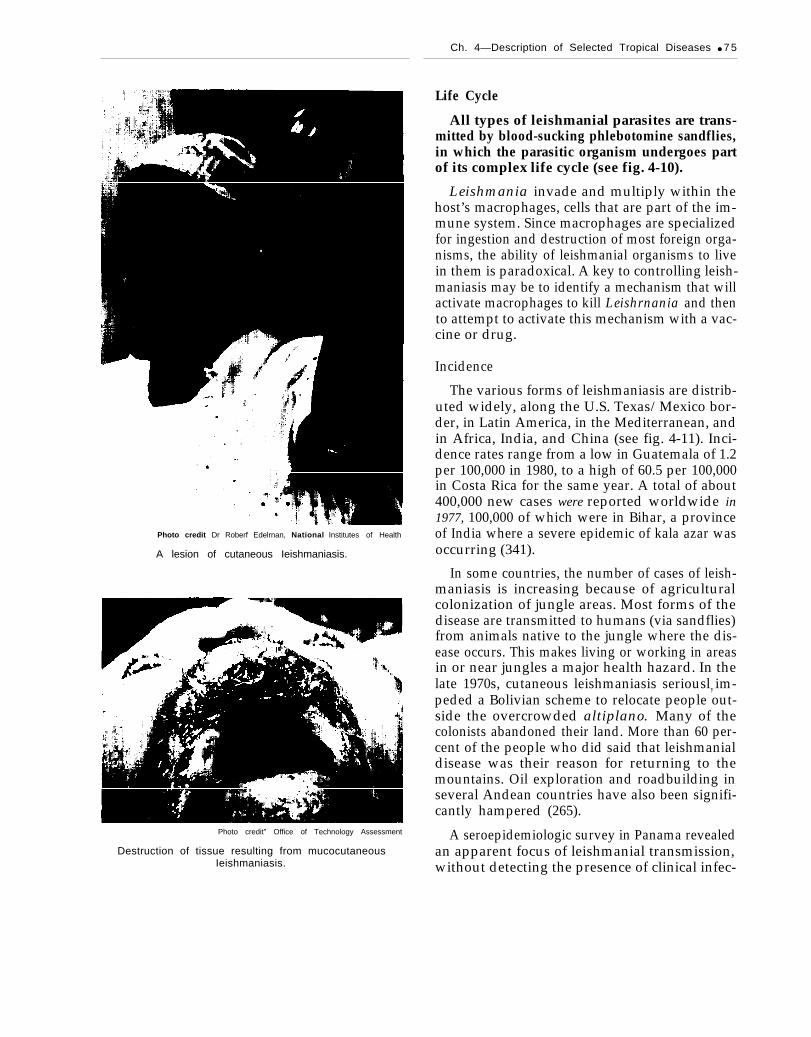
Photo credit Dr Roberf Edelrnan, National Institutes of Health
A lesion of cutaneous Ieishmaniasis.
Photo credit” Office of Technology Assessment
Destruction of tissue resulting from mucocutaneousIeishmaniasis.
Ch. 4—Description of Selected Tropical Diseases ● 7 5
Life Cycle
All types of leishmanial parasites are trans-mitted by blood-sucking phlebotomine sandflies,in which the parasitic organism undergoes partof its complex life cycle (see fig. 4-10).
Leishmania invade and multiply within thehost’s macrophages, cells that are part of the im-mune system. Since macrophages are specializedfor ingestion and destruction of most foreign orga-nisms, the ability of leishmanial organisms to livein them is paradoxical. A key to controlling leish-maniasis may be to identify a mechanism that willactivate macrophages to kill Leishrnania and thento attempt to activate this mechanism with a vac-cine or drug.
Incidence
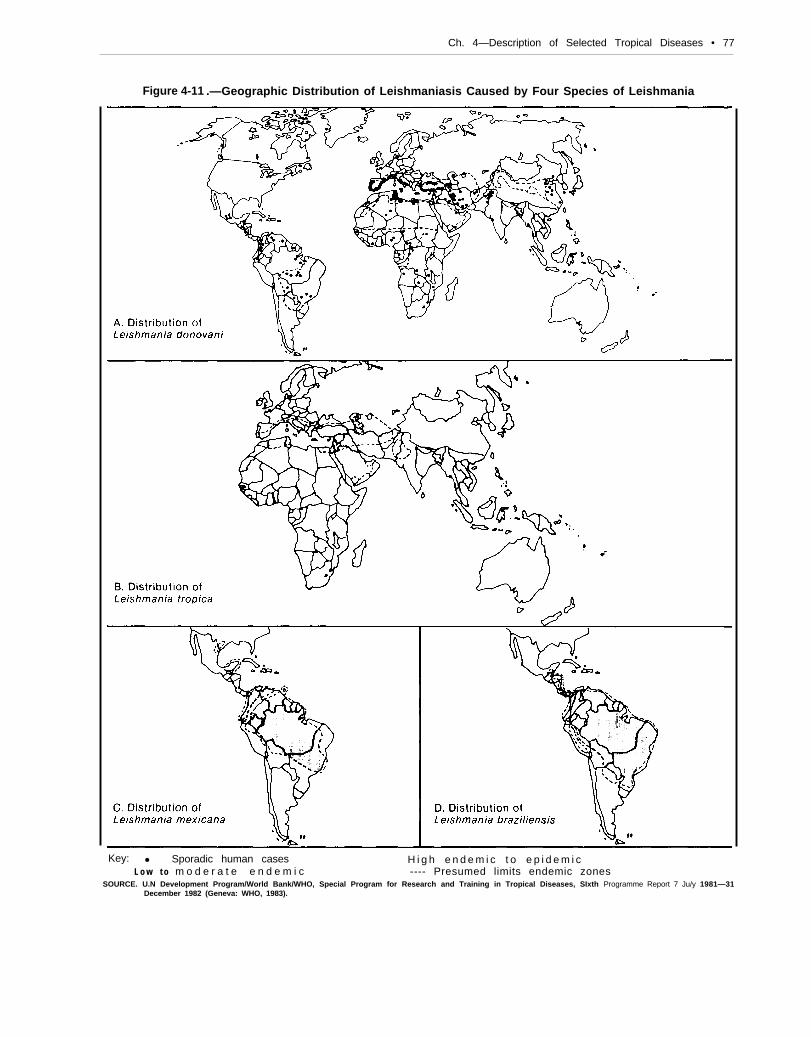
The various forms of leishmaniasis are distrib-uted widely, along the U.S. Texas/Mexico bor-der, in Latin America, in the Mediterranean, andin Africa, India, and China (see fig. 4-11). Inci-dence rates range from a low in Guatemala of 1.2per 100,000 in 1980, to a high of 60.5 per 100,000in Costa Rica for the same year. A total of about400,000 new cases were reported worldwide in1977, 100,000 of which were in Bihar, a provinceof India where a severe epidemic of kala azar wasoccurring (341).
In some countries, the number of cases of leish-maniasis is increasing because of agriculturalcolonization of jungle areas. Most forms of thedisease are transmitted to humans (via sandflies)from animals native to the jungle where the dis-ease occurs. This makes living or working in areasin or near jungles a major health hazard. In thelate 1970s, cutaneous leishmaniasis seriously im-peded a Bolivian scheme to relocate people out-side the overcrowded altiplano. Many of thecolonists abandoned their land. More than 60 per-cent of the people who did said that leishmanialdisease was their reason for returning to themountains. Oil exploration and roadbuilding inseveral Andean countries have also been signifi-cantly hampered (265).
A seroepidemiologic survey in Panama revealedan apparent focus of leishmanial transmission,without detecting the presence of clinical infec-

76 ● Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4.10.—GeneraIized Life Cycle of Leishmania, the Cause of Leishmaniasis
J
1. Parasites develop to “promastigote”2. Parasites are transmitted to humans
stage infective to humans and other mammals in sandfly vector.and other mammals through bite of sandfly.
3. Parasites transform to “amastigote” stage in mammalian host, multiplying within certain cells of the host’s immunesystem.
4. Some amastigotes infect new cells in the mammalian host.5. Some amastigotes are picked up by sandflies during bite of infected mammalian host.
SOURCE: Off Ice of Technology Assessment, 1985. Photo from H. W. Brown and F. A. Neva, Basic Clinical Parasitology (East Norwalk, CT: Appleton-Century-Crofts,1983), used by permission.
Ch. 4—Description of Selected Tropical Diseases • 77
Figure 4-11 .—Geographic Distribution of Leishmaniasis Caused by Four Species of Leishmania
Key: ● Sporadic human cases H i g h e n d e m i c t o e p i d e m i cL o w t o m o d e r a t e e n d e m i c ---- Presumed limits endemic zones
SOURCE. U.N Development Program/World Bank/WHO, Special Program for Research and Training in Tropical Diseases, SIxth Programme Report 7 Ju/y 1981—31December 1982 (Geneva: WHO, 1983).

78 . Status of Biomedica/lResearch and Related Technology for Tropical Diseases
tion. Completely subclinical leishmaniasis waspreviously unknown and may be an importantclue to vaccine development.
Interventions
For disease caused by most species of Lekh-mania, no effective prevention is known. How-ever, immunity to Old World cutaneous leishma-niasis (also called Oriental sore) arising from L.tropica infection can be induced by inoculationof a susceptible person with organisms from anactive lesion, a procedure apparently known fromancient times in endemic regions.
Specific treatment for leishmaniasis is now lim-ited to antimony compounds. These compoundsare not always effective and often have adversetoxic side effects. Another disadvantage of thesecompounds is that they require daily injectionsfor 10 to 20 days, making them impractical forpatients living in remote and inaccessible areas.Hospitalization for such a period is not only ex-pensive but also a major inconvenience to patientswho cannot afford to leave work or their farmsfor an extended period. For these reasons, im-proved treatment of the tens of thousands of ex-isting cases is a priority research goal. The PanAmerican Health Organization/WHO is attempt-ing to foster development of new therapeuticdrugs. One, allopurinol, in combination withother drugs, is a promising new treatment (393).
FILARIASISAspects of Natural History
Filariasis is a collective term for several distinctparasitic infections of tissue-dwelling, threadlikenematodes, which are transmitted by mosquitoesand other insects. There are at least eight differ-ent types of human filarial infections, among theminfection by the infamous guinea worm, whichbefore modern chemotherapy evolved was re-moved by gradually winding the protrudingworm around a stick. Probably the most impor-.tant of the filarial parasites, in terms of world-wide prevalence and severity of disease, are Wu-
Recent Progress
Fewer than 10 laboratories in the United Statesstudy leishmanial organisms. The difficulty in dis-tinguishing between Leishmania species (necessaryto properly predict clinical outcomes and selecttreatment) has been a persistent problem. The so-lution, however, may be aided by biotechnology.In recent years, MAbs have been prepared againsta variety of antigenic determinants in Leishmaniaspp. (16) and used to probe morphologic and tax-onomic differences. Rapid identification of Leish-mania spp. may soon be possible with a recentlypublished technique of DNA hybridization (40s).
A variation of the enzyme-linked immuno-sorbent assay (ELISA), called the “DOT-ELISA”method (267), is also a major advance, allowingfor rapid easy field diagnosis. These and othermethods would permit early treatment of the de-structive mucocutaneous form of the disease andwould also facilitate precise epidemiologic fieldstudies.
The possibility of developing a vaccine againstthe promastigote form of the leishmaniasis para-site (the stage transferred through the bite of thesandfly) remains. Such a vaccine would havelimited usefulness because it would be ineffectiveagainst the amastigote form of the parasite (thestage which lives within the microphage). Thetransformation from promastigote to amastigoteoccurs rapidly within the host, before a vaccine-initiated antibody response could be effective.
chereria bancrofti and Brugia malayi, which causelymphatic forms of filariasis; and Onchocercavolvulus, the agent of onchocerciasis (riverblindness).
Life Cycles and Interventions
The life cycles of W. bancrofti and B. malayiare fairly similar (see fig. 4-12). These organismsare transmitted to humans by several species ofmosquitoes, including common household pestspecies. The adult filarial worms live in the hu-man host’s lymphatic system and cause pathol-

Ch. 4—Description of Selected Tropical Diseases ● 7 9
Figure 4-12.-Generalized Life Cycle of Two Important Filarial Worms:Wuchereria bancrofti and Brugk malayi
v&40 x 0.11 mm
3 83x 0.24 m m
1. Infective larvae develop, but do not multiply, in mosquito vector.2. Larvae deposited on skin of human or other mammalian host (B. malayi only) through mosquito proboscis at time of bite.3. Larvae penetrate skin, migrate to host’s lymphatic system, and mature.4. Masses of adult worms can block lymph vessels, causing accumulation of lymph fluid and growth of lymph tissue, in a
manifestation called elephantiasis.5. Adult worms release immature microfilariae into blood circulation, usually in a circadian rhythm.6. Mosquitoes ingest microfilariae during bite of infected human or other mammal.SOURCE: Office of Technology Assessment, 1985. Photo from F. W. Brown and F. A. Neva, Basic Clinical Parasitology (East Norwalk, CT: Appleton-Century-Crofts,
1983), used by permission.

80 . Status of Biomedical Research and Related Technology for Tropical Diseases
ogy that differs with the host’s immune response.Inflammation and gross obstruction results invarying degrees of swelling of the lymph glands,which may result grotesque enlargement (elephan-tiasis) of the legs, breasts, or scrotum. Adultworms release immature forms (microfilariae) thatcirculate in the human blood and then infect feed-ing mosquitoes to complete the transmission cy-cle. Drugs are available to kill the microfilariae,but the means to kill mature worms are poor.
0. volvulus parasites are transmitted to humansby blackflies of the genus Simulium. These black-flies require running water to complete their lifecycles, limiting their habitat mainly to areasaround rivers (hence the name river blindness foronchocerciasis). The adult parasitic worms livein the tissues of the human body and often formlarge nodules where an intertwined clump ofworms localizes. Microfilariae released by theadult worms migrate through the human host’sbody in subcutaneous tissues where they can bepicked up by feeding blackflies. When microfilar-iae reach the human eye, blindness can result. Theprevention of blindness is imperfectly achievedby chemotherapy and surgical removal of thenodules. Few preventive measures are available,and larvicides used to control the blackfly vec-tor of onchocerciasis are subject to resistance andhave only transient effects.
Incidence and Prevalence
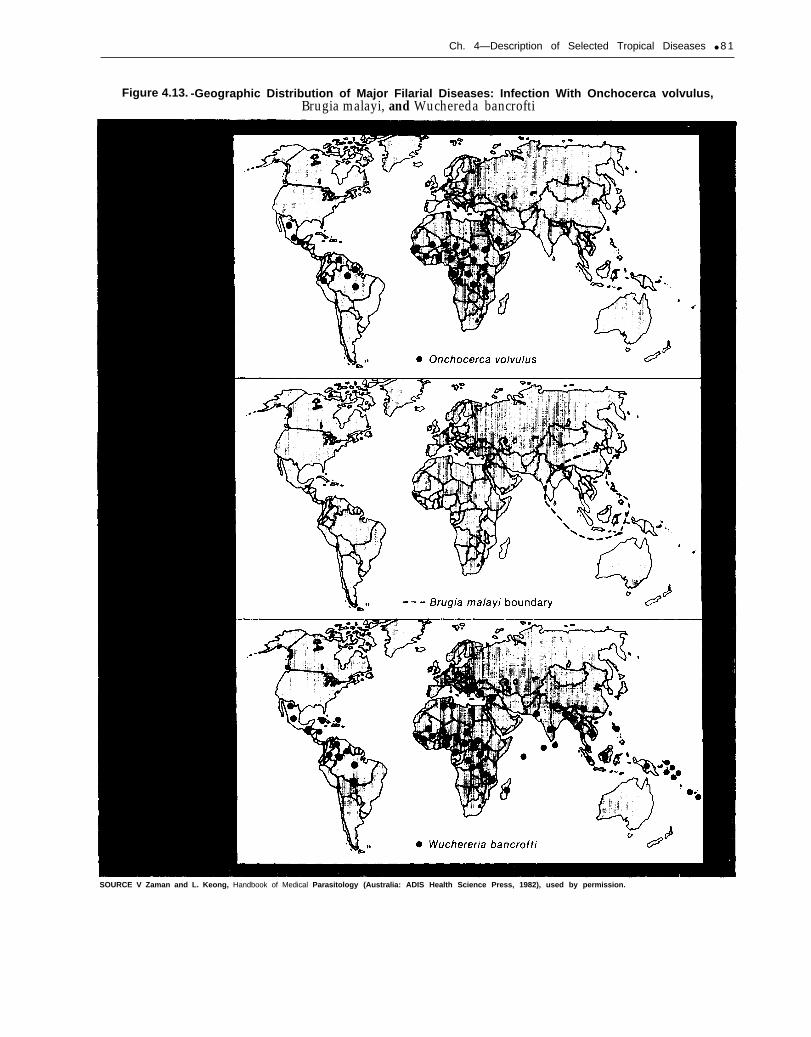
Filariasis due to W. bancrofti has a wide butfocal urban distribution throughout the Pacific re-
LEPROSY (HANSEN’S DISEASE)Aspects of Natural History
Leprosy is a chronic bacterial infection that con-tinues to be an important public health problemin many countries. The disease is caused byMycobacterium leprae, a bacterium similar to theone that causes tuberculosis. Leprosy is mainlya disease of the skin and peripheral nerves, butit is characterized by a wide array of clinicalpresentations.
gion, Asia, Africa, and Latin America (see fig. 4-13) (406). Lymphatic filariasis caused by B. malayiis primarily found in rural foci in Sri Lanka, Thai-land, Malaysia, Vietnam, China, South Korea, Bor-neo, and Indonesia. Onchocerciasis is found incentral and western Africa, North Yemen, SaudiArabia, Mexico, Venezuela, Colombia, Brazil,Ecuador, and Central America.
It is estimated that bancroftian filariasis andonchocerciasis are more prevalent today than theywere more than 100 years ago (256). More than300 million people are exposed to mosquito-trans-mitted lymphatic filariasis, and more than 30 mil-lion are infected. The main endemic areas in In-dia remain, and there is little control of the diseasein Africa, where in Savannah areas it is estimatedthat more than 15 percent of the adults are in-fected.
Obstacles to Research
Considering the great number of people affectedor at risk, their widespread geographical distri-bution, and the severity of their pathology, thefilarial diseases are relatively neglected by Amer-ican researchers. A major obstacle to research onfilariasis is the difficulty in maintaining filarialorganisms for laboratory study. Their compli-cated life cycles and the unavailability of suitableanimal models make these parasites among themost frustrating to work with.
Much of the pathology of leprosy is associatedwith a defective cell-mediated immune responsein certain individuals. Depending on the host’s im-munologic response, leprosy ranges from benigntuberculoid leprosy, with localized skin lesionsand nerve involvement (sometimes severe periph-eral neuropathy) and the presence of few M.leprae bacteria, to lepromatous leprosy, withspreading lesions that become nodular and dis-
Ch. 4—Description of Selected Tropical Diseases ● 8 1
Figure 4.13. -Geographic Distribution of Major Filarial Diseases: Infection With Onchocerca volvulus,Brugia malayi, and Wuchereda bancrofti
SOURCE V Zaman and L. Keong, Handbook of Medical Parasitology (Australia: ADIS Health Science Press, 1982), used by permission.

82 • Status of Biomedical Research and Related Technology for Tropical Diseases
figuring, resulting in destruction of the nose, in-volvement of the vocal cords and eyes, and oftensevere nerve damage, with a heavy infection ofM. leprae.
Questions about why leprosy has such variedeffects on its victims have not been fully answered.Researchers are not even sure how the disease istransmitted. The latent period, the time betweeninfection and the actual appearance of symptoms,often lasts for many years. The individual is ca-pable of unknowingly infecting others during thistime. Leprosy is more likely to be spread bychronic exposure to dried skin lesion matter andnasal secretions from the lepromatous and moresevere borderline patients. The general consen-sus seems to be that M. leprae bacteria enter thehuman body through the respiratory system, al-though some researchers suspect entry may alsobe through the skin (406).
Immunologic diagnostic techniques have shownthat people with tuberculoid leprosy have a strongand effective cell-mediated immune response (vialymphocytes) that controls the infection, whereaslepromatous leprosy patients do not. There issome evidence to suggest a genetic basis for thisdifference. The nerve damage in patients withlepromatous leprosy seems to result from an ab-sence of cellular immune response. Characteriza-tion of this defect in Iepromatous leprosy patientsis being investigated with MAbs that can iden-tify lymphocyte subsets and also by analysis ofthe patients’ genetic type.
Incidence and Prevalence
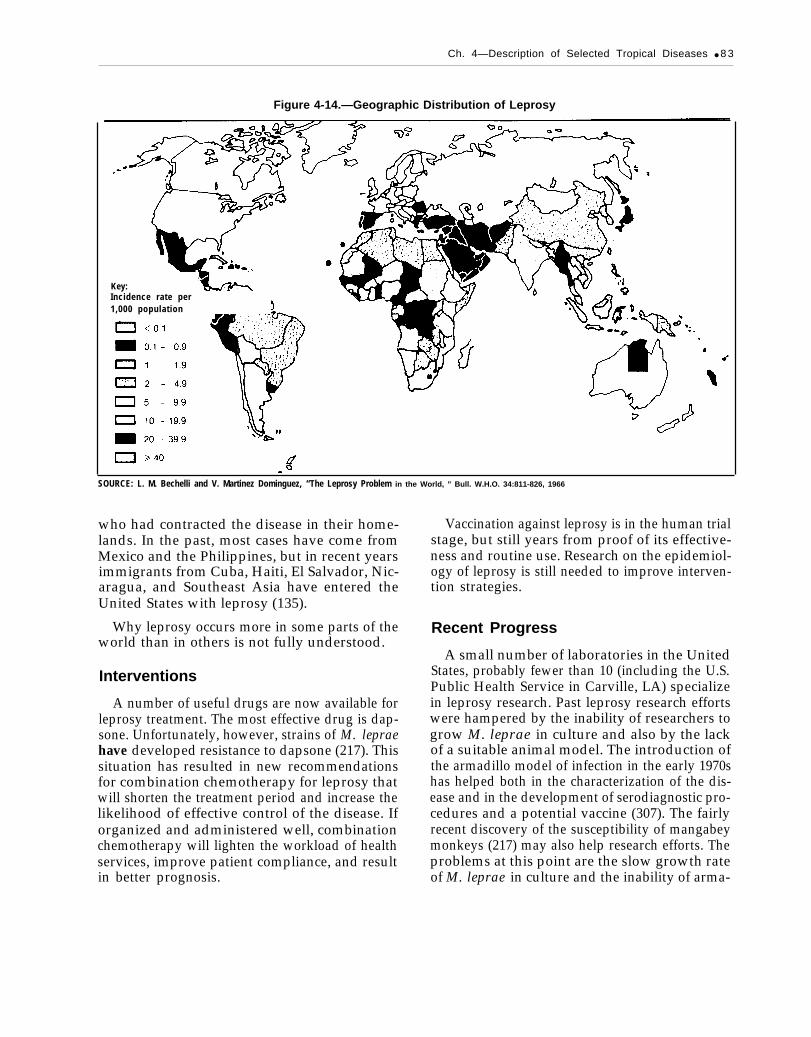
Worldwide there are an estimated 15 millionleprosy cases (307). The prevalence of leprosy hasbeen reduced in many places, but the overall in-cidence (i.e., the number of new cases per year)has not changed with advances in science (see fig.4-14). In some very small, isolated communitiesin parts of Africa and Australia, the prevalenceof leprosy may be as high as 1 out of every 50inhabitants. The disease is also common in south-ern Asia, especially India (210). In China, an esti-mated 500,000 cases of leprosy occurred in theearly 1950s, but fewer than 200,000 cases werereported in 1984 (307). As of 1984, there were 2.5million cases in Southeast Asia alone (135).
In the Americas, there are about 400,000 casesof leprosy, 80 percent of the new cases occurringin Argentina, Colombia, and the Amazon areaof Brazil (265). The recorded incidence of leprosyin the Americas has almost doubled in the last 10years, but the increase is thought to reflect im-provements in case finding and notification of au-thorities, rather than to be a true change. Overhalf the clinical cases are of the more severelepromatous form. However, as many as four-fifths of those infected with M. leprae never getsick, though they may transmit the disease tothose with more susceptible immune systems(210).
About 20 cases of leprosy acquired in theUnited States are diagnosed each year, occurringin Texas, Louisiana, California, Florida, and Ha-waii. Of the 250 new cases of leprosy diagnosedin the United States in 1982, 233 were immigrants
Ch. 4—Description of Selected Tropical Diseases ● 8 3
Figure 4-14.—Geographic Distribution of Leprosy
Key:Incidence rate per1,000 population
SOURCE: L. M. Bechelli and V. Martinez Dominguez, “The Leprosy Problem in the World, ” Bull. W.H.O. 34:811-826, 1966
who had contracted the disease in their home-lands. In the past, most cases have come fromMexico and the Philippines, but in recent yearsimmigrants from Cuba, Haiti, El Salvador, Nic-aragua, and Southeast Asia have entered theUnited States with leprosy (135).
Why leprosy occurs more in some parts of theworld than in others is not fully understood.
Interventions
A number of useful drugs are now available forleprosy treatment. The most effective drug is dap-sone. Unfortunately, however, strains of M. lepraehave developed resistance to dapsone (217). Thissituation has resulted in new recommendationsfor combination chemotherapy for leprosy thatwill shorten the treatment period and increase thelikelihood of effective control of the disease. Iforganized and administered well, combinationchemotherapy will lighten the workload of healthservices, improve patient compliance, and resultin better prognosis.
Vaccination against leprosy is in the human trialstage, but still years from proof of its effective-ness and routine use. Research on the epidemiol-ogy of leprosy is still needed to improve interven-tion strategies.
Recent Progress
A small number of laboratories in the UnitedStates, probably fewer than 10 (including the U.S.Public Health Service in Carville, LA) specializein leprosy research. Past leprosy research effortswere hampered by the inability of researchers togrow M. leprae in culture and also by the lackof a suitable animal model. The introduction ofthe armadillo model of infection in the early 1970shas helped both in the characterization of the dis-ease and in the development of serodiagnostic pro-cedures and a potential vaccine (307). The fairlyrecent discovery of the susceptibility of mangabeymonkeys (217) may also help research efforts. Theproblems at this point are the slow growth rateof M. leprae in culture and the inability of arma-

84 ● Status of Biomedical Research and Related Technology for Tropical Diseases
dillos to breed in captivity, necessitating their con-tinual trapping from the wild.
Despite the paucity of workers, the tools of bio-technology are being applied to M. Ieprae. At least
TUBERCULOSISAspects of Natural History
Tuberculosis is caused by the bacterium Myco-bacterium tuberculosis, transmitted mainly by air-borne droplets from person to person. There isno insect vector or animal reservoir. Tuberculosisremains a major threat to health in many partsof the world, causing several million deaths an-nually. Though basically a chronic respiratory dis-ease, tuberculosis can spread into the cardiovas-cular, endocrine, and genital systems, and intothe lymph nodes, bone, brain, kidneys, and otherorgans (406).
Incidence
A 1982 worldwide estimate put the number oftuberculosis cases at 11 million (265), with some3.5 million new cases occurring each year (92).Tuberculosis is still a serious problem in mostcountries of the world. About 500,000 deaths areattributed to the disease each year.
Even in countries such as Canada and the UnitedStates, with highly developed coverage for diag-nosis and treatment of tuberculosis available, asignificant number of cases of tuberculosis are en-countered each year. Often the disease is presentamong immigrants arriving from tuberculosis-prevalent tropical areas. From 1962 to 1975, priorto the current wave of immigrants to the UnitedStates from Indochina, the tuberculosis case rateamong children under 14 in the United States de-creased from 10.4 to 3.7 per 100,000, represent-ing a 9-percent decline per year. But this down-ward trend has not continued, and the rate in 1984was about the same as that of 1975 (281). In 1980,some 30,000 new cases of pulmonary tuberculosiswere reported in the United States (70).
three investigators are preparing MAbs as part ofstudies on the immunochemistry or antigenicstructure of the bacterium (16).
Interventions
In the past, control of tuberculosis was basedon the identification, isolation, and treatment ofpatients with active disease, since these patientsare the source of continued transmission andspread. More recently, with the advent of effec-tive chemotherapy and reduction of active cases,developed countries with lower prevalence oftuberculosis have emphasized identification ofnewly infected persons via the tuberculin skin testand treatment of these individuals, in addition toidentification and treatment of persons with activedisease. Developing countries continue to empha-size identifying and treating patients with activedisease, who account for most of the transmis-sion. Tuberculosis is generally diagnosed by spu-tum microscopy or culture.
Treatment of tuberculosis patients consists ofdaily administration of one or more drugs in com-bination for 6 to 12 months. The drugs most com-monly used include isoniazid (INH), streptomy-cin, Para-aminosaliqlic acid (PAS), pyrazi.namide,and rifampicin. If the course of treatment is fol-lowed properly, cure rates can be as high as 100percent (406). Because of the practical problemsof long-term treatment, however, a 100-percentcure rate is seldom realized.
Unfortunately, some strains of M. tuberculosishave developed resistance to INH, the most ef-fective drug available. Cases of INH-resistanttuberculosis are commonly reported in tropicalareas from Asia to Latin America. Patients in-fected with resistant strains must take severalchemotherapeutic drugs, and for a longer timeperiod, before the infection is arrested.

Ch. 4—Description of Selected Tropical Diseases ● 8 5
A factor strongly contributing to the resistanceproblem is the high cost of rifampicin. This drug,when used with INH, is highly effective in con-trolling tuberculosis, but it costs about 400 timesas much as INH (see ch. 9). Developing countriesthat cannot afford to use rifampicin in their treat-ment regimes often opt for other less expensivedrugs. The short-term savings, are lost, however,because patients often do not complete long-termregimens. Partial treatment that does not elimi-nate the infection encourages the proliferation ofdrug-resistant organisms, as the most susceptibleare kiIIed off even with an incomplete course oftherapy.
Despite the availability of a vaccine for tuber-culosis, Bacillus Calmette-Guerin (BCG), there isconsiderable controversy as to its effectiveness.BCG vaccine is derived from a live, attenuatedbovine tubercle bacillus, isolated from a singlestrain by the Pasteur Institute 50 years ago. BCG
vaccination of uninfected persons can producehigh resistance to tubercle bacilli, but the protec-tion against tuberculosis has varied greatly in fieldtrials. Since the vaccine was made years agoagainst only one isolated strain, it may not be ca-pable of immunizing individuals against all cur-rently active strains of M. tuberculosis. Never-theless, some trials have shown very effectiveprotection, and BCG vaccine is still recommendedin high-risk areas.
Recent Progress
The tuberculin skin test is not an adequatepredicter of infection or active tuberculosis, par-ticularly for research purposes. The use of anti-gen probes and ELISA methods may be helpfulin more accurately characterizing the state of aninfection (16).
DIARRHEAL AND ENTERIC DISEASESAspects of Natural History
Diarrheal diseases, all of which are transmittedby fecal contamination of food and water, consti-tute a clinical syndrome of varied etiology. Suchdiseases are caused by a variety of viruses (pri-marily rotaviruses), bacteria (Shigella, Sahno-nella, Cryptosporidium, Escherichia coli, Cam-pylobacter, and Yersinia), protozoa (Entamoebaand Giardia), and worms (Ascaris, Ancylostoma,and Necator), interacting in a complex fashionwithin the susceptible host. Diarrheal diseases aredistributed worldwide.
Diarrhea is primarily a disease of infants andchildren. The great danger in diarrheal disease isthe dehydration and subsequent shock caused bytremendous losses of fluids and electrolytes (salts).Severe dehydration is the most frequent cause ofdiarrheal deaths. Although treatment directed atthe disease-causing organisms may or may not beeffective, there now exists effective treatment formost cases of dehydration caused by diarrhea.Oral dehydration therapy (ORT) for diarrheal dis-eases is considered one of the most significant ther-
apeutic advance in the past several decades (seeCase Study A: Oral Dehydration Therapy forDiarrheal Diseases).
In 1980, WHO conservatively estimated thatamong children under the age of 5, 750 millionto 1 billion diarrheal episodes occur yearly inAfrica, Asia (excluding the People’s Republic ofChina), and Latin America (324). Data from sev-eral developing countries indicate that childrenunder 5 years of age in these countries typicallyexperience four to eight diarrheal episodes annu-ally (23,215,216). In contrast, infants in the UnitedStates and other developed countries experienceone or two diarrheaI episodes yearly. In somecountries, up to 45 percent of all hospital visitsduring the months of highest diarrhea prevalenceare due to childhood diarrhea, and case fatalityrates as high as 40 percent have been recorded (249).
A comparison of death rates between childrenunder 1 year of age in Latin America and NorthAmerica is startling. For the United States andCanada, the mortality rate due to diarrheal dis-ease among infants in 1979 was 21.9 deaths per

86 Ž Status of Biomedical Research and Related Technology for Tropical Diseases
100,000 infants; for Latin America, it was 914.6per 100,000. The Latin American figure is 40 timeshigher, which means almost 1 in 100 infants bornthere dies of diarrheal dehydration. Wherever theinfant mortality rate exceeds 100 per 1,000 births,at least one-third of the deaths can be attributedto diarrhea (216,257).
Viruses
The complex of diarrheal diseases caused byviruses-rotaviruses, Norwalk-like agents, adeno-viruses, astroviruses, enteroviruses, corona-viruses, calciviruses, and others, perhaps not yetidentified—present extreme difficulties in diagno-sis (15). Viral agents cause a significant amountof diarrheal illnesses in the tropics, but very littleis known about any of them except rotaviruses.
Rotaviruses, the most frequently isolated groupof viruses, have a worldwide distribution. Theywere first detected in humans in 1973. Rota-viruses, which are believed to cause one-third ofall diarrheal disease in the world, may cause upto 40 percent of diarrheal disease in children indeveloped countries. Serologic studies have shownthat by the age of 2, nearly all children have beeninfected with rotaviruses.
Photo credit: S. S. Raphael, “Lynch’s Medical Laboratory Technology, ”W. B. Saunders Co., 1983. Reprinted by permission.
Electron micrograph of a rotavirus, a major cause ofdiarrheal disease in children.
In Australia, Canada, the United Kingdom, andthe United States, a large percentage (40 to 60 per-cent) of all children hospitalized with diarrhea areinfected with rotaviruses; the percentage in coun-tries like Guatemala and El Salvador is smaller(20 to 40 percent) (371,420). However, since theincidence of all diarrhea] disease is much higherin developing countries than in developed coun-tries, the toll due to rotaviral infection in thesedeveloping countries is actually much greater thanthe percentages indicate.
Growing recognition of the importance of rota-viruses emphasizes the need for further epidemio-logic, clinical, and basic research. Rotavirus bi-ology currently is studied at the National Institutesof Health, where each of the rotavirus genes hasbeen cloned into bacteria and identified (117). Im-munologically based diagnostic testing can be usedfor field studies of prevalence and incidence. Sincea rotavirus vaccine exists for animals, a major ob-jective now is to develop one for humans.
Bacteria
Numerous bacteria are known to cause diar-rheal illness, and the list continues to grow as lab-oratory identification methods improve. In manyareas of developing countries, the facilities neededto identify the agents responsible for diarrhea arenot available. The question of causality is com-plicated by the wide variety of bacteria which liveharmlessly in the intestine. This large “intestinalflora” confounds efforts to isolate and identify theimportant pathogens, among them enterotoxigenic(toxin-producing) E. coli, Shigella spp. (whichcause dysentery), Salmonella spp. (which causefood poisoning and typhoid fever), Vibriocholerae (which causes cholera), and Campylo-bacter.
At present, there is a great deal of concernabout the apparent rise in antibiotic-resistant bac-teria. Two separate factors may be responsible forthe increase. One factor is the widespread mis-use of antibiotics both in the United States andabroad, due to ineffective dosing of individuals,indiscriminate prescribing of drugs (regardless ofthe etiologic agent), and the availability of anti-biotic drugs over-the-counter in many develop-ing countries. As a result of this misuse, many

Ch. 4—Description of Selected Tropical Diseases ● 8 7
intestinal bacteria, both pathogenic and non-pathogenic, are being exposed to antibiotics. Mostintestinal bacteria are killed by antibiotics, butthose bacteria that have some sort of resistancemechanism, often genetically determined, surviveand are passed on.
The second factor is the ability of many intes-tinal bacteria to exchange genetic material amongdifferent strains, species, and even genera throughthe transfer of DNA. Bacteria that survive antibi-otic exposure may transfer the genes that code fortheir resistance to previously susceptible bacte-ria, and these bacteria in turn incorporate theminto their genetic material and pass them on toboth pathogenic and nonpathogenic bacteria.Thus, in the past, a cholera infection might havebeen successfully treated with a few highly effec-tive doses of tetracycline, but now larger dosesof two or more other antibiotics may be requiredto combat the disease. Strains of E. coli, Shigella,and Vibrio cholerae have all been shown to beantibiotic resistant.
Escherichia coli. —E. coli is second to rota-viruses as an important cause of diarrheal disease.For the American traveling abroad (or the foreignvisitor touring the United States), E. coli is fre-quently the source of the infamous travelers’diarrhea.
Ironically, although E. coli is one of the mostintensely studied of all organisms in the labora-tory, little is known about its disease-causing abil-ities. Most strains are harmless inhabitants of theintestine, and only certain strains cause disease:enterotoxigenic E. coli produces toxins that resultin excessive fluid production; enteroinvasive E.coli invades the cells of the intestinal wall; andenteropathogenic E. coli produces a toxin simi-lar to that of Shigella, which causes diarrhea ininfants. Investigators are currently studying thegenetic basis for disease-causing properties of dif-ferent E. coli strains.
Shigella. —In 1981, there were 19,859 cases ofdiarrhea due to Shigella reported in the UnitedStates (366). Infections by Shigella dysertteriae re-sult in bacillary dysentery, a serious and some-times fatal disease. Most Shigella infections, how-ever, are by species other than S. dysenteriae (e.g.,S. sonnei and S. flexneri), and the symptoms are
not as severe. Shigella is difficult to study becauseit colonizes only primates; thus, research on itspathology is very expensive. The genes coding forthe attachment factors (which allow the organismto adhere to the intestinal wall) have been clonedand inserted into E. coli.
Salmonella. —This genus is frequently dividedinto Salmonella typhi, the cause of typhoid fe-ver, and the nontyphi species. In general, the non-typhi species of Salmonella cause self-limitedgastrointestinal distress, although some speciesmay cause bacteremia bacteria in the blood. Thewide variety of symptoms associated with Sal-monella infection, ranging from mild flu-likestomach upsets to severe food poisoning to ty-phoid fever, make the collection of accurate in-cidence and prevalence statistics almost im-possible.
In 1981, there were 39,990 cases of salmonellosisfood poisoning reported in the United States (367).Salmonellosis is usually associated with the con-sumption of contaminated livestock or poultryproducts. In that year, there were approximatelyhalf of the 510 cases of typhoid fever reported inthe United States, about half of which were ac-quired during travel abroad. During the period1970-80 while the incidence of typhoid fever inLatin America increased, the number of cases re-mained stable in North America and the Carib-bean region (265).
Sahnonella spp. usually cause endemic diar-rhea, but they may cause epidemics. The need forimproved sanitation and new antibiotics wasbrought forcefully home during a nontyphoid epi-demic in Mexico in 1972-73, when it was discov-ered that the strain causing the epidemic was resis-tant to chloramphenicol, the drug of choice, andto other antibiotics (265).
Recently, researchers at the Walter Reed ArmyMedical Research and Development Commandcloned Shigella genes into an attenuated live ty-phoid vaccine developed by a group of research-ers in Switzerland. The result was a vaccine thatproduced immunity to both Shigella and Salmo-nella (126,423).
Vibrio cholerae. -Cholera occurs in both en-demic (in parts of China and India) and epidemicforms (in Asia and Africa). Because of improved

88 ● Status of Biomedica/ Research and Related Technology for Tropical Diseases
sanitation in many countries, cholera epidemicsare not as common as in the past, although onereached the U.S.S.R. as recently as 1970 (406).For unknown reasons, cholera epidemics havespared the Western Hemisphere.
The severe diarrhea characteristic of cholera iscaused by the action of a bacterial toxin on thegut wall. One of the factors that makes choleraso virulent is the number and variety of transmis-sible genetic elements, which vary from one strainto the next. Researchers have been collecting chol-era strains from endemic areas around the world,and recombinant DNA libraries, consisting of seg-ments of genes from wild-type organisms andlaboratory-grown strains, have been created. Bystudying and comparing the gene segments of tox-igenic and nontoxigenic strains, scientists hope topinpoint exactly which genes are responsible forcholera’s virulence (16).
Campylobacter. —Various species of Cam-pylobacter are commonly the cause of sporadicdiarrhea in developing and developed countries(45). Following rotavirus and enterotoxigenic E’.coli, Campylobacter is the third most commoncause of diarrhea in developing countries (297).Campylobacter also is a “frequent, cosmopolitanrisk to travelers” (278). Epidemics sometimes af-fecting thousands of people, have been caused byCampylobacter contaminating unpasteurizedmilk, chicken carcasses, and water (194).
Protozoa and Other Agents
There are several protozoal diarrheal patho-gens, among them Entamoeba spp., Giardia Jam-blia, and Cryptosporidium spp.
Giardiasis is now recognized as significant andubiquitous throughout the United States, but is
more prevalent in tropical countries. Outbreaks,such as occurred in Aspen, CO, and Rome, NY,have been well publicized (313). G. lamblia is awell-known hazard to camping and backpackingenthusiasts, who are becoming aware that wilder-ness water may not be as pristine as it looks. Manyother less publicized outbreaks have occurred in pre-school day care centers (400).
Cryptosporidium spp. are common diarrhea-causing agents in individuals whose immune sys-tems are compromised, and they have also beenfound in some otherwise healthy individuals.Cryptosporidium was first described in 1907, butits oocysts (spherical egglike cells) were not rec-ognized in animal feces until 1978. The impor-tance of Cryptosporidium spp. has been ap-preciated only recently. Investigators using asimple diagnostic procedure developed in the lastfew years have estimated that the organism ac-counts for 1 to 4 percent of all cases of diarrheain human beings (400).
Not much is known about chronic low-level en-teric infections by bacteria such as Yersinia (theagent of plague). Multiple infections by severaldifferent pathogens frequently occur, makingdiagnosis difficult. One study of people living ina poor rural area of Panama with substandardsanitation showed that 90 percent of the 202 peo-ple examined were infected by one or more para-sites, the majority of which were either Ascarislumbricoides (roundworm), E. histolytica, or G.lamblia (88). WHO estimates there are at least 650million people in the world with roundworm (as-cariasis), 450 million people with hookworm (an-cylostomiasis), 350 million people with amebiasis,and 350 million people with whipworm (trichu-riasis) infections (318).
ACUTE RESPIRATORY INFECTIONS (ARIs)Aspects of Natural History the elderly, sometimes exceeding the mortality
rate due to diarrheal diseases. The ultimate con-ARIs are among the most important causes of sequences of an ARI depend on the organism(s)
preventable deaths in the world. They are a ma-, responsible for the infection and the patient’s nu-jor cause of mortality among children under 5 and tritional status and age.

Ch. 4—Description of Selected Tropical Diseases . 89
All of the ARIs are aggravated by malnutritionand substandard living conditions, and the pres-ence of other infectious diseases. A principal epi-demiologic factor of ARI transmission is close,overcrowded conditions that promote inhalationof pathogens aerosolized by coughs, sneezes, andpersonal contact.
ARI agents include viral, bacterial, chlamydial,and mycoplasmal organisms, all transmitted tohumans by airborne droplets. For medical pur-poses, ARIs are usually characterized as upper orlower respiratory tract infections (URTIS orLRTIs); then as community- or hospital-acquired;and then grouped by etiologic agent. Many of thesame organisms cause infections in both the up-per and lower respiratory tracts, however.
Incidence and Prevalence
Data about the frequency of ARIs are not gen-erally available, making a discussion of incidenceand prevalence of this important group of diseasesdifficult. Surveys in India, Guatemala, the UnitedStates, and the United Kingdom suggest that theincidence of ARIs is similar throughout the de-veloping and developed countries, averaging fourto eight separate episodes per year (175). How-ever, mortality rates for ARIs in India are thoughtto be 30 to 75 times higher than those in the UnitedKingdom or the United States (175). What mightcause inconvenient days out of work or schoolin a developed country might well kill a personin a developing country.
Some 12 percent of all deaths of children liv-ing in Africa, Central America, and Asia are at-tributed to ARI (289), and most of these childrendie of either pneumonia, bronchiolitis, or acuteobstructive laryngitis (croup) (370). Among in-fants, mortality from ARI can range as high as1,500 per 100,000 in areas of Egypt, Paraguay,and Mexico—a figure 30 times higher than in theUnited States and Canada (57)—or even higherto the 4,000 to 4,400 per 100,000 observed in areasof Bolivia and Brazil (370). The incidence of pneu-monia, 70 to 100 cases per 1,000 per year, in chil-dren under 5 in developing countries, is doublethat of the United States. Among children whoare suffering from malnutrition, almost half willalso contract pneumonia during any given year(370).
WHO data, collected from 88 countries on fivecontinents, representing a quarter of the world’spopulation, reported over 660,000 deaths fromARIs in 1978 (35). Extrapolating this figure to theworld population suggests that there are morethan 2.2 million deaths from ARIs per year, a sig-nificant number of which could have been pre-vented. In addition to presenting a serious mor-tality risk for the very young and the very old,ARIs impose a tremendous social burden in termsof lost productivity and demands on the healthcare system by all age groups.
Viruses
Viruses cause most URTIS and some importantinfections of the lower respiratory tract. Most vi-ral infections of the upper respiratory tract—infec-tions with respiratory syncytial virus (RSV),adenoviruses, rhinoviruses, coronaviruses, and in-fluenza, parainfluenza, measles, and Epstein-Barrviruses, for example—are self-limiting, eliminatedby a healthy immune system. In weakened indi-viduals, particularly children, who may be mal-nourished and have other infections, however, evennormally benign URTIS can be life-threatening.
Measles is one of the few URTIS against whicha highly effective vaccine exists. The vaccine’s useis not universal, however, and measles remainsa major cause of death among children in thedeveloping world. Worldwide, 900,000 people,mainly children, died from measles in 1979 (392).The high death rate may be due to concurrent in-fections, or overcrowded living conditions, whichresult in heavy exposure of the susceptible indi-vidual to the virus whenever several members ofthe same household are infected (118).
In general, LRTIs cause more serious healthproblems than do URTIS, though they are causedby many of the same viruses. RSV, measles, andinfluenza are major causes of pneumonias, whichoften lead to death in developing countries.
Bacteria
Bacteria cause a host of infections in and aroundthe upper respiratory tract including the sinuses,throat, tonsils, epiglottis, larynx, and trachea.Four types of bacteria are particularly significant

90 ● Status of Biomedical Research and Related Technology for Tropical Diseases
causes of URTIS. Corynebacterium diphtheria,is the cause of diphtheria, an infection of the phar-ynx. A second, Bordetella pertussis, is the causeof pertussis (whooping cough). Effective vaccinesto prevent diphtheria and whooping cough areroutinely given to newborns in developed coun-tries and are included in WHO’s Expanded Pro-gram on Immunization. Immunization is muchmore effective than treatment for these twodiseases.
A third bacterium, Streptococcus pyogenes,commonly infects the pharynx, but is also theorganism responsible for rheumatic fever. Thefourth is Hemophilus influenzae, which causes earinfections and the more serious condition of men-ingitis in children.
Bacterial pneumonias (LRTIs) area major causeof morbidity and mortality in developing coun-tries, as they are in developed countries. Strep-tococcus pneumoniae is one of the most commoncauses of bacterial pneumonia affecting all ages.Other causes of bacterial pneumonia are S. py-ogenes, Staphylococcus aureus, H. influenza,Klebsiella pnemonia, E. coli, and Pseudomonaspseudomallei.
Most bacterial ARIs respond to treatment withantibiotics. Important exceptions are many hos-pital-acquired pneumonias, which are often causedby drug-resistant organisms, a problem in devel-oped as well as developing countries.
Other ARI Agents
Other less known ARI agents include Chla-mydia spp. (congenital) and Mycoplasma spp.,usually responsible for URTIS and atypical pneu-monia among adolescents and adults. Chlamydiaspp. appear similar to bacteria, but their size isclose to that of viruses. Mycoplasma spp., a groupof organisms which lack a rigid cell wall, are con-sidered by some to be primitive bacteria.
Interventions
For most viral ARIs, there is no treatment otherthan symptomatic and supportive relief, thoughbacterial infections can be effectively treated withantibiotics. Vaccinations for measles, whooping
cough, and diphtheria are effective and are pro-moted for vaccinating children under the Ex-panded Program on Immunization of WHO.However, use of the vaccines for these diseasesis frequently limited by the cost of vaccines, theability of the health infrastructure to maintain avaccination program, and the problems inherentin maintaining a “cold chain” for certain vaccines.(Cold chain is the name given to the means forcontinuous refrigeration of vaccines from produc-tion to vaccinee. )
Measles is an example of an ARI which could,like smallpox, be eradicated by vaccination. Priorto the development of the measles vaccine in 1962,481,530 cases were reported in the United States,46 resulting in deaths. In 1979, after several yearsof widespread use of the vaccine, there were only13,597 cases and only 1 death (366). In many de-veloping countries, however, vaccinations againstmeasles have been infrequent. Among childrenunder 1 year of age in 1982, only 8.3 percent inMexico, 15.9 percent in Bolivia, and 22.4 percentin Colombia (265) were immunized. Measles vac-cine must be administered after maternal antibod-ies lose their effectiveness, but prior to the child’sfirst exposure to a virus, in order for it to work—acritically short time span.
Vaccines against pneumococcal pneumonia(due to S. pneumonia) and influenzas are avail-able, but their usefulness in developing countries,is limited because pneumococcal vaccine is notvery effective in children under 2 years old andinfluenza vaccines must be renewed periodicallyaccording to the currently prevalent strain. Be-cause of the high cost of annually manufacturinga different strain of influenza vaccines, influenzavaccines are generally available only to high-riskgroups.
Improved living conditions and access to healthcare are critical factors in controlling ARI, butfield-based epidemiologic studies are also needed.ARI control is largely ignored in most develop-ing countries. This situation is a function of sev-eral factors: difficulty in identifying the etiologicagents of ARIs, lack of effective treatment formany ARIs, and failure to define ARIs as tropi-cal diseases, or to recognize ARIs as worthy offocused research.

Ch. 4—Description of Selected Tropical Diseases Ž 91
The prevention and treatment of ARIs couldbe simplified through studies precisely identify-ing the important etiologic agents in different geo-graphic areas and determining the risk factors thatmake ARI mortality so high. Practical manage-ment of ARI depends on differential diagnosis ofviral from other bacterial, chlamydial, and myco-plasmal agents for which specific treatments areeffective.
Biotechnology and ARIs
The tools of biotechnology are slowly being ap-plied to the many viruses that cause ARIs in hu-mans, but bacterial agents are being largelyignored.
ARBOVIRAL AND RELATED VIRALAspects of Natural History
Arboviral infections constitute a large group ofdiseases caused by viruses (currently about 80known in humans) defined by ecologic, epidemio-logic, and clinical, rather than taxonomic, char-acteristics. The term “arbovirus” is a contractionof “arthropod-borne virus. ” Strictly speaking,arboviruses replicate in and are transmitted byarthropods (predominantly mosquitoes, but alsoticks, sandflies, midges, and gnats) (a generalizedarbovirus life cycle is shown in fig. 4-15). How-ever, there are some arbovirus-like diseases whosevector is still unidentified (e.g., those caused bythe Arenaviridae family) and some whose earlyepidemiologic profile incorrectly suggested arthro-pod transmission (e.g., Argentinean and Bolivianhemorrhagic fevers). These exceptions are noted,but for lack of a better characterization system,they are discussed here.
Arboviruses are widely distributed throughoutall areas of the world and cause significant en-demic and epidemic disease. Most arboviral dis-eases are infections of animals accidentally trans-mitted to humans (zoonoses), although epidemicsof human-to-human transmission, via insect vec-tors, can occur.
The number of known arboviruses has grownrapidly as the etiologic agents of many fevers and
ARI viruses are being isolated, identified, andcharacterized. A few laboratories are working onthe molecular biology of influenza are studyingmechanisms of immunity (76) as well as the ef-fectiveness of immunization (271). All of the in-fluenza genes have been identified and sequenced.Recently, some of the influenza genes have beencloned into the vaccinia virus used to inoculateagainst smallpox. Hamsters were inoculated withthe vaccine and immunity was produced againstboth smallpox and influenza (319). There is hopethat all the genes from the various types of in-fluenza can eventually be cloned into the vacciniavirus to produce a single vaccine effective againstevery strain.
INFECTIONS
brain inflammations (encephalitis) have been iden-tified and their transmission cycles elucidated. Themajor groups of arboviruses are classified by theirbiochemical and physical properties into theTogaviridae, Bunyaviridae, and Arenaviridaefamilies.
The Togaviridae family is divided into twogroups. There are about two dozen “alphaviruses”(formerly known as Group A), including the agentsof Eastern, Western, and Venezuelan equine en-cephalitis frequently found in North and SouthAmerica, Chikungunya of Africa and the Far East,and Sindbis and Semliki Forest viruses of Africa;and three dozen or so “flaviviruses” (formerlyGroup B), including the agents of yellow fever,dengue fever, Japanese B encephalitis and SaintLouis encephalitis (found in the United States).About a third of the flaviviruses are tick-borneand cause various febrile and hemorrhagic ill-nesses.
The Bunyaviridae family includes several hun-dred distinct viruses, among them the agents ofCalifornia encephalitis, Oropouche fever of Bra-zil, Crimean hemorrhagic fever, and Rift Valleyfever of east Africa.
The Arenaviridae are not arboviruses, althoughthe possibility remains that arthropod vectors willsomeday be identified for the group. Included here
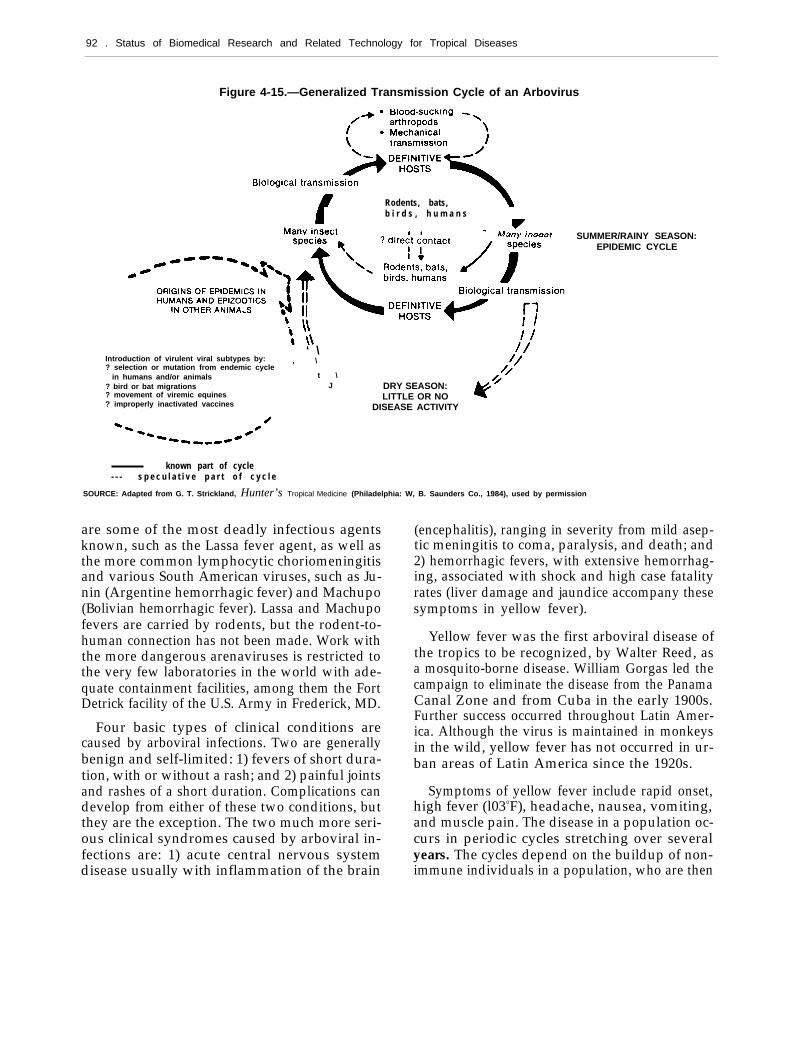
—
92 . Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-15.—Generalized Transmission Cycle of an Arbovirus
1
Rodents, bats,b i r d s , h u m a n s
.SUMMER/RAINY SEASON:
EPIDEMIC CYCLE
‘ \Introduction of virulent viral subtypes by: , \? selection or mutation from endemic cycle
in humans and/or animals t \? bird or bat migrations J? movement of viremic equines? improperly inactivated vaccines
DRY SEASON:LITTLE OR NO
DISEASE ACTIVITY
known part of cycle- - - s p e c u l a t i v e p a r t o f c y c l e
SOURCE: Adapted from G. T. Strickland, Hunter’s Tropical Medicine (Philadelphia: W, B. Saunders Co., 1984), used by permission
are some of the most deadly infectious agentsknown, such as the Lassa fever agent, as well asthe more common lymphocytic choriomeningitisand various South American viruses, such as Ju-nin (Argentine hemorrhagic fever) and Machupo(Bolivian hemorrhagic fever). Lassa and Machupofevers are carried by rodents, but the rodent-to-human connection has not been made. Work withthe more dangerous arenaviruses is restricted tothe very few laboratories in the world with ade-quate containment facilities, among them the FortDetrick facility of the U.S. Army in Frederick, MD.
Four basic types of clinical conditions arecaused by arboviral infections. Two are generallybenign and self-limited: 1) fevers of short dura-tion, with or without a rash; and 2) painful jointsand rashes of a short duration. Complications candevelop from either of these two conditions, butthey are the exception. The two much more seri-ous clinical syndromes caused by arboviral in-fections are: 1) acute central nervous systemdisease usually with inflammation of the brain
(encephalitis), ranging in severity from mild asep-tic meningitis to coma, paralysis, and death; and2) hemorrhagic fevers, with extensive hemorrhag-ing, associated with shock and high case fatalityrates (liver damage and jaundice accompany thesesymptoms in yellow fever).
Yellow fever was the first arboviral disease ofthe tropics to be recognized, by Walter Reed, asa mosquito-borne disease. William Gorgas led thecampaign to eliminate the disease from the PanamaCanal Zone and from Cuba in the early 1900s.Further success occurred throughout Latin Amer-ica. Although the virus is maintained in monkeysin the wild, yellow fever has not occurred in ur-ban areas of Latin America since the 1920s.
Symptoms of yellow fever include rapid onset,high fever (l03oF), headache, nausea, vomiting,and muscle pain. The disease in a population oc-curs in periodic cycles stretching over severalyears. The cycles depend on the buildup of non-immune individuals in a population, who are then

Ch. 4—Description of Selected Tropical Diseases ● 9 3
swept by an epidemic of the virus, leaving an im-mune population of survivors. Safe and effectivevaccination of human populations near endemicjungle areas is one control strategy and providesimmunity for at least 10 years. Surveillance ofmonkey populations and jungle mosquitoes bysampling for virus isolation is an important mon-itor, providing early warning of high levels of in-fection.
Yellow fever still remains a major threat in trop-ical America and Africa (see fig. 4-16), becausethe virus is maintained by transmission througha number of jungle mosquitoes, with monkeysand possibly certain marsupials serving as reser-voirs. Recent research has demonstrated that pas-sage of the virus from the female mosquito to theegg (transovarial transmission) occurs among thevectors of yellow fever. Thus, the mosquito mayfunction not only as a vector, but also as a reser-voir (100).
Cases of yellow fever in humans are associatedwith humans invading the jungle habitat. In re-cent years, however, an outbreak appeared in Co-
Photo credit: K.S. Warren and A.A.F. Mahmoud “Tropical and GeographicalMedicine, ” McGraw-Hill Book Co., 1984. Reprinted by permission.
Electron micrograph of the dengue virus, agentof dengue fever.
lombia where there were no apparent known vec-tors or reservoirs, and in Trinidad where no caseshad been detected for almost 20 years. The pos-sibility of unknown reservoirs is of concern, asAedes aegypti, the vector of yellow fever in theurban setting, remains abundant throughout the
Figure 4-16.—Geographic Distribution of Yellow Fever
SOURCE: U.S. Department of Health and Human Services, Centers for Disease Control, Health Informat/in for International Travel, HHS Publication No.(CDC)840-8280 (Washington, DC: U.S. Government Printing Office, 1984).
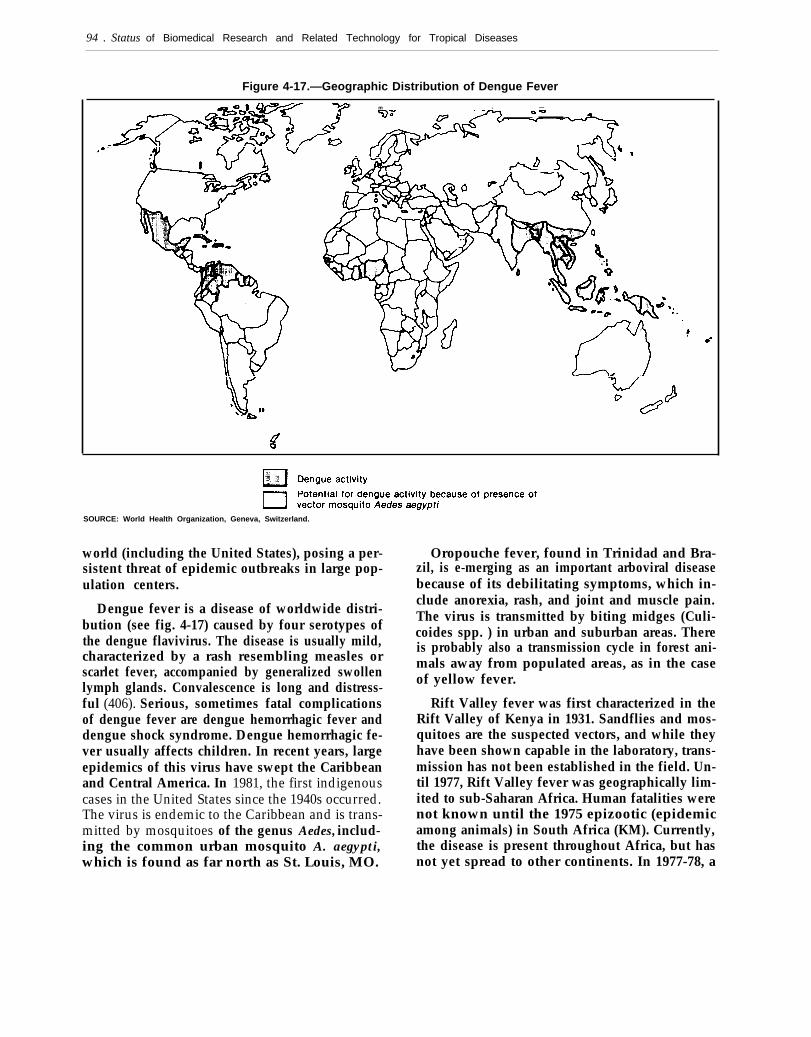
94 . Status of Biomedical Research and Related Technology for Tropical Diseases
Figure 4-17.—Geographic Distribution of Dengue Feverb m - —
SOURCE: World Health Organization, Geneva, Switzerland.
world (including the United States), posing a per-sistent threat of epidemic outbreaks in large pop-ulation centers.
Dengue fever is a disease of worldwide distri-bution (see fig. 4-17) caused by four serotypes ofthe dengue flavivirus. The disease is usually mild,characterized by a rash resembling measles orscarlet fever, accompanied by generalized swollenlymph glands. Convalescence is long and distress-ful (406). Serious, sometimes fatal complicationsof dengue fever are dengue hemorrhagic fever anddengue shock syndrome. Dengue hemorrhagic fe-ver usually affects children. In recent years, largeepidemics of this virus have swept the Caribbeanand Central America. In 1981, the first indigenouscases in the United States since the 1940s occurred.The virus is endemic to the Caribbean and is trans-mitted by mosquitoes of the genus Aedes, includ-ing the common urban mosquito A. aegypti,which is found as far north as St. Louis, MO.
Oropouche fever, found in Trinidad and Bra-zil, is e-merging as an important arboviral diseasebecause of its debilitating symptoms, which in-clude anorexia, rash, and joint and muscle pain.The virus is transmitted by biting midges (Culi-coides spp. ) in urban and suburban areas. Thereis probably also a transmission cycle in forest ani-mals away from populated areas, as in the caseof yellow fever.
Rift Valley fever was first characterized in theRift Valley of Kenya in 1931. Sandflies and mos-quitoes are the suspected vectors, and while theyhave been shown capable in the laboratory, trans-mission has not been established in the field. Un-til 1977, Rift Valley fever was geographically lim-ited to sub-Saharan Africa. Human fatalities werenot known until the 1975 epizootic (epidemicamong animals) in South Africa (KM). Currently,the disease is present throughout Africa, but hasnot yet spread to other continents. In 1977-78, a

Ch. 4—Description of Selected Tropical Diseases ● 9 5
widespread epizootic and epidemic of Rift Val-ley fever occurred in Egypt. Some 18,000 humancases were officially reported, and almost 600 peo-ple died of the disease (209). The disease in ani-mals has a serious economic effect, causing cat-tle to abort and high fatality rates among newbornlambs. In humans, infection usually results onlyin mild dengue-like febrile illness, although it canresult in severe ocular (inflammation of the ret-ina and blindness), encephalitic, or hemorrhagiccomplications.
Lassa fever is endemic to some regions of WestAfrica. Symptoms include prostration, severe sorethroat, tonsillitis, chest pain, and pneumonitis (in-flammation of the walls of the air sacs in the lung).There is evidence that mild or subclinical infec-tions occur, but among those hospitalized withLassa fever, fatality rates range from 20 to 40percent.
Research Needs
Laboratory techniques can identify arbovirusesand define antigenically similar groups, but there
is great geographic and climatic diversity in eachserologic grouping. This situation emphasizes thecomplexity and challenge of arbovirus researchand control.
There is no cure for arboviral diseases, onlysymptomatic and supportive relief. Early diagno-sis of the agents responsible for potential out-breaks and epidemics identified down to the finestlevel possible, has three important values: 1) todifferentiate ambiguous presenting symptoms; 2)to anticipate life-threatening complications, as inyellow fever and dengue fever; and 3) to targetthe vector, which then determines control strate-gies. Current control efforts rely on early iden-tification of epidemic outbreaks of arboviraI in-fections, allowing the institution of vector-controlmeasures such as insecticide fogging. In manytropical countries, however, disease surveillanceis not well developed.

















