Developing Competency to Build Capacity in a Pediatric Intensive Care Unit Lynn Coolen, Becky Palmer, Amanda Bush, Leslie Braun, Sarb Randhawa, Rosella Jefferson, Dori Van Stolk, Melanie McVittie, Tracie Northway, and Karen LeComte
Transcript
Developing Competency to Build Capacity in a Pediatric
Intensive Care UnitLynn Coolen, Becky Palmer, Amanda Bush,
Leslie Braun, Sarb Randhawa, Rosella Jefferson, Dori Van Stolk, Melanie McVittie,
Tracie Northway, and Karen LeComte
British Columbia Children’s Hospital
The province’s tertiary care centre for children and youth142 bed inpatient facility
Deliver the following programs:Critical CareCardiac SciencesNeurosciencesOncology/Hematology/Bone Marrow TransplantPediatric General and Sub-specialty MedicineSurgery and Surgical Suite ServiceChild Development and Rehabilitation Program
Academic heath centre affiliated with University of British Columbia
Critical Care Program
22 bed combined Intensive Care Unit and Transitional Care Unit
Deliver services to all programs1200 admissions per year50% of patients cardiacProvide critical care services for infants →18 years
average age of patient = 3.5 years
Intraprofessional team 118 RNs 40 RT’s10 Allied Health5 Intensivists
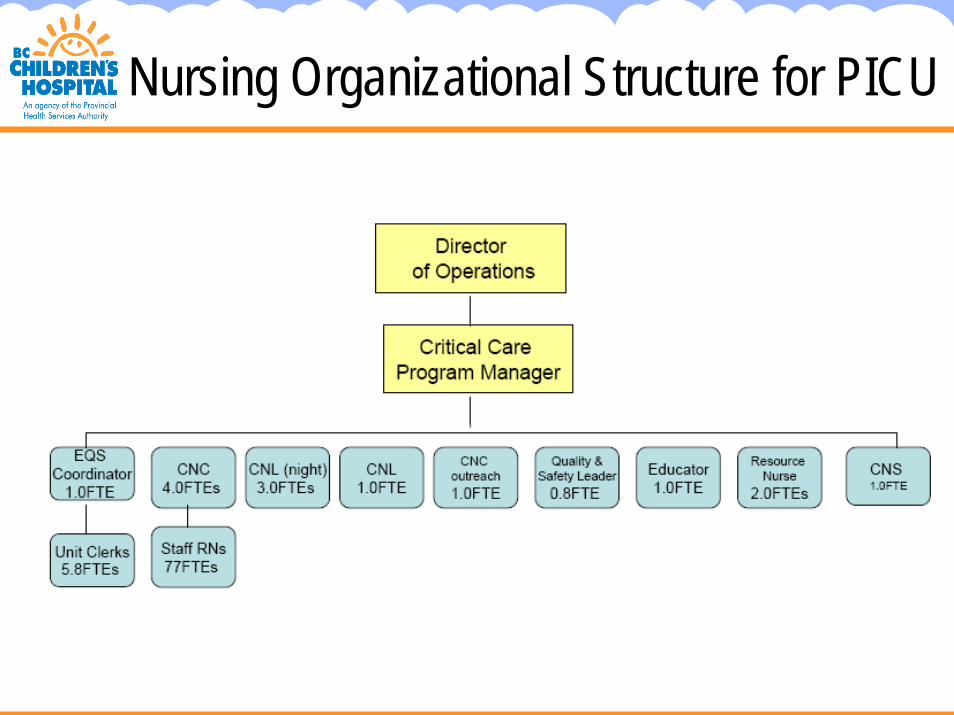
Nursing Organizational Structure for PICU
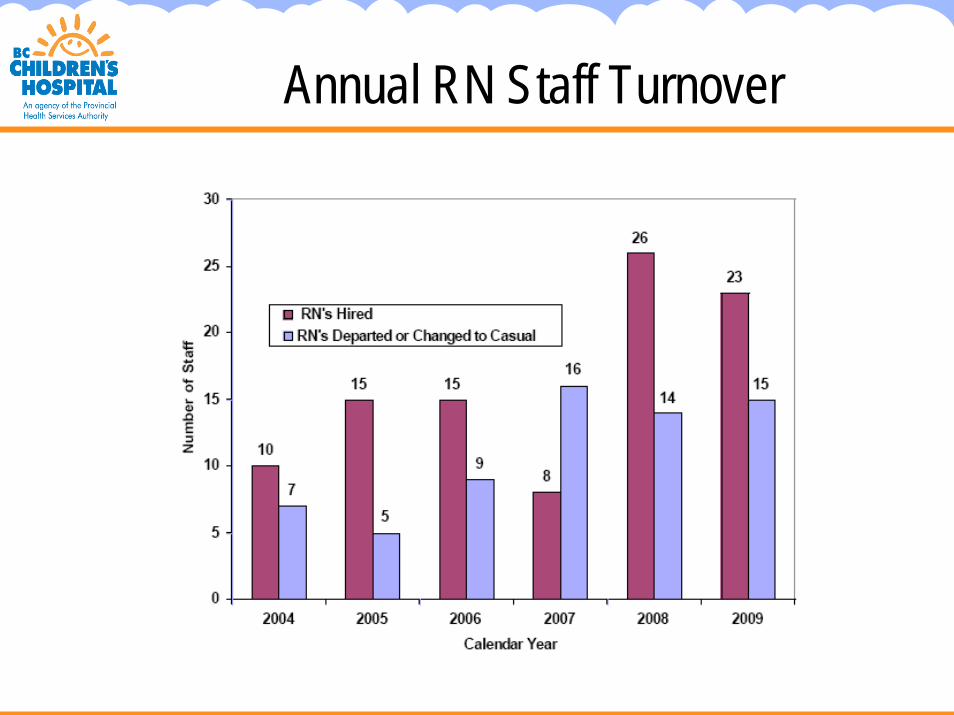
Annual RN Staff Turnover
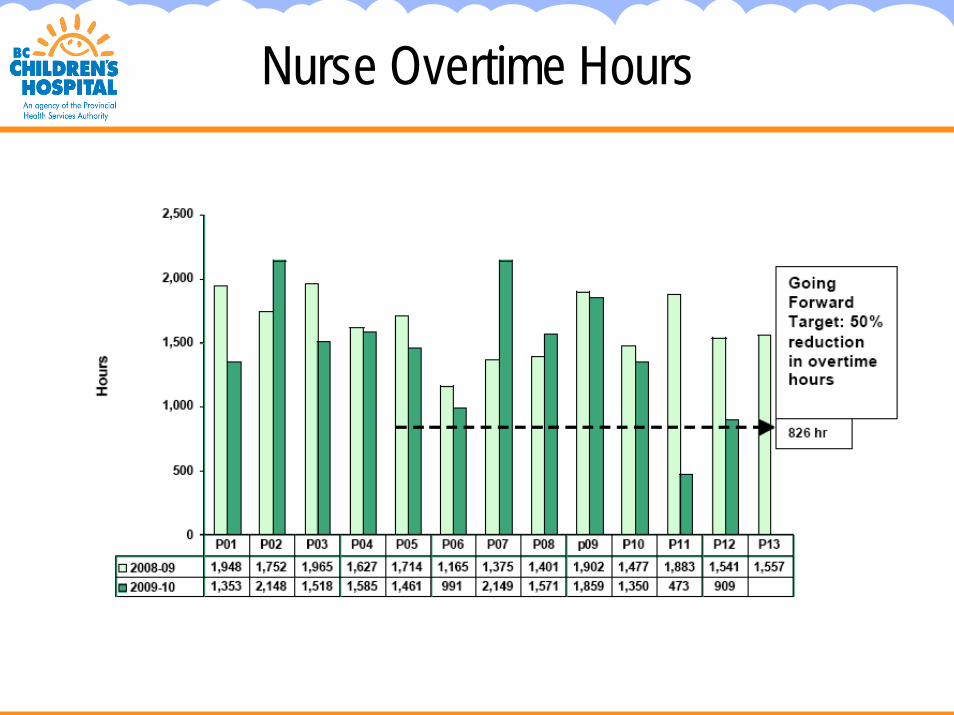
Nurse Overtime Hours
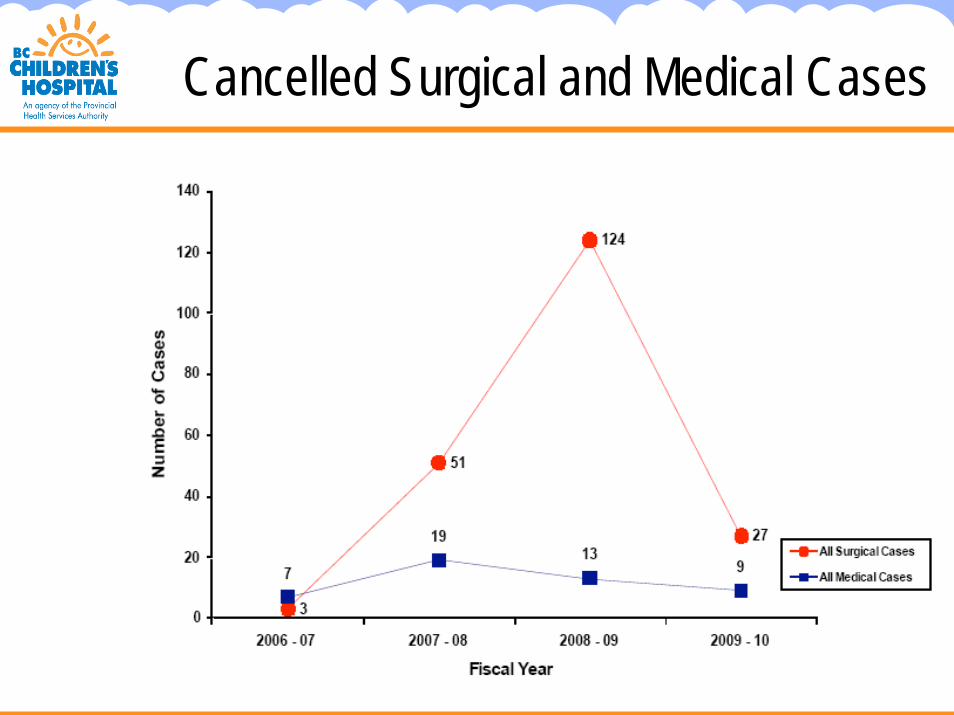
Cancelled Surgical and Medical Cases
Nursing Resource Team (NRT)
following restructuring in early 2000’s → team of nurses formed to provide support in inpatient areas
structure integrated well on medical/surgical unitsincreased need to utilize NRT support in Critical Care
areas (ER, PICU) development of ‘internship’ to support NRT working in
PICU to care for the high acuity patients
Assignment Algorithm
Support to assign reassigned staff to PICU
problematic when nurse competency did not meet patient care requirements
Vitality Survey
Measurement of overall health and vitality of organizationOriginated from Institute for Health Improvement (2
questions adapted)Administered in March 2009Response rate = 50Average score = 3.38 / 5, where
1 = Strongly Disagree5 = Strongly Agree
to be re-administered in October
Vitality Survey Scores1 I have easy access to the supplies and equipment I need to do my work on this unit. 3.262 Care team members on this unit feel free to make important decisions about patient care. 3.363 The work environment on this unit promotes patient safety. 3.414 The support services to this unit respond in a timely way. 3.605 I can discuss challenging issues with care team members on this unit. 3.276 There is good cooperation among different hospital departments. 3.317 My ideas really seem to count on this unit. 3.048 I feel a sense of accomplishment and pride after I have completed my work on this unit. 3.359 Nurses, physicians, and other staff on this unit work as a high-functioning team. 3.4310 I speak up if I have a patient safety concern. 4.4011 Care team members on this unit feel free to question the decisions or actions of those with more authority. 2.9612 Important patient care information is exchanged during shift changes. 4.1013 The work environment on this unit is well organized. 3.1414 If I have an idea about how to make things better on this unit, the manager and other staff are willing to try it 3.3015 Care professionals communicate complete patient information during handoffs. 3.5116 Staff members on this unit treat one another with respect. 3.4017 Essential patient care equipment is in good working condition on this unit. 3.3318 There are enough experienced registered nurses to care for the patients on this unit. 2.88
19 I am part of an effective work team that continuously strives for excellence even when the conditions are less than optimal. 3.63
20 I have the supports and resources to do my best job. 3.3421 I have a high level of job satisfaction. 3.4022 I receive adequate feedback on my performance 2.98
1 = Strongly Disagree 5 = Strongly Agree
Staffing Model
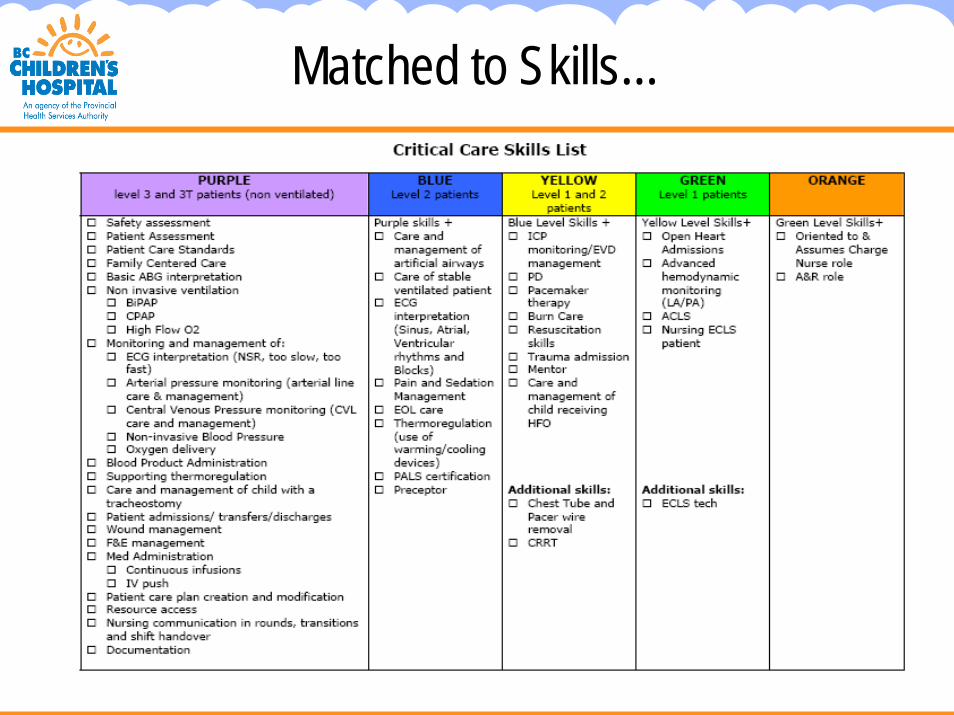
Matched to Skills…
Current Situationcontinual intake of new staff limited
attention to ongoing competency development
varied perceptions regarding progression in Critical Care beyond initial orientation
varied points of entry with differing experiences
Supervision and measurement of competencies on an ongoing basis challenging d/t scheduling, role clarity, & unit activity
development pathways and expectations are not clear (clinical, leadership, education)
Current Situation (con’t)Frustrated staff (= push system)Mismatch patient needs to nsg skills
Competency Validation process not formalized (resource intense)Educational and Clinical Support
shifted from 2.0 Educators to 1.0 Educator and 2.0 Clinical Resource Nurses
No incentives in place to advancePreceptors may be pulled away from
preceptees because of skill mixOT called for skill mix Staff take cues regarding
performance feedback based on selected advancement Limited admin support for education
methodologyBased on the Toyota Production System and ‘lean’ thinkingEmpowers staff to maximize value by eliminating waste and
variation from workflowWasteVariation
Cultural change/mindset shiftCore organizational strategyimPROVE vs. other QI Approaches
1. Removal of waste2. Systems thinking from the patient perspective3. Rapid cycle improvement4. Driven by staff
Rapid Process Improvement Workshop (RPIW)
A method of continuous improvement concentrated in a one week workshop
Utilizes the Lean tools and methodologiesIncludes observing the work on the “gemba”, testing
change ideas, proposing and implementing changes, auditing and sustaining the change.
Diverse team members~ people performing the work is key to success
Communication to team
Our Team
Aim of RPIW #12
create a competency based, learner centered professional development pathway for Critical Care RNs in PICU from the time of hire through the first two years
pathway to be:cleartransparentvisible
What preparation occurred for this RPIW?
25 interviews of frontline staff about the current way that nurses progress from one colour level to another (most dissatisfied)
Observations of the CRNs to understand ‘Just in time’ teaching and support
Consultation with other departments and other PICUs regarding their competency development
construction of a ‘straw man’ pathway as a beginning step to creating a roadmap during the RPIW
Why is advancement important?
nurses are clear on the expectation for development and can actively engage in their own learning
capacity is enhanced by ensuring appropriately trained staff are available to care for the various levels of patient care needs
retention is addressed and nurses have higher satisfaction levels with a clear pathway for professional progress
Why did we do this?
with a continual intake of new staff, limited attention has been paid to the ongoing competency development of Critical Care Nurses
since 2008, 46 new hires have come to PICU (almost half of the staff in 2 years is new to the organization)
dissatisfaction on how to progress to care for increasingly acute patients
OT and rework occurs to compensate for a mismatch of nurse skills and patient needs
What did we do?
What change ideas were tested and what were the findings?
Four areas of work evolved during the RPIW week:1. Pathway development2. Evaluation and Validation3. Professional Portfolio4. Roles and Supports
1. Pathway Development
creation of the pathway started with the ‘skills checklist’ and the focus was to be able to describe how a nurse moves from one colour to the next
revisions occurred during the week to achieve this current pathway based on staff input (PDSA cycle)
Further revisions will occur as we start to use this pathway and incorporate further feedback from staff
CAPE tools utilized for ongoing competency development
Validation tools to be developed for competency validation
Roles will define who can validate and how (see roles)
Regular check-ins, validation, evaluation and feedback is being built into the system (see STOP signs on the pathway)
Skills Validation Tools (SVT)
Validate domains of competency
Knowledge
Skill
Clinical Decision Making
Patient & Family Considerations
3. Professional Portfolio
reintroduction of the Professional portfolio was agreed by staff as a way to track progress
portfolio allows staff to keep track of feedback, validation tools, CAPE tools, learning plans, etc.
Inserts will be available for role out
4. Roles and Supports
clearly defining leaders’ roles in staff development is an important support
further work is to be done so that each role is clearly articulated in terms of what a nurse can expect from each leader so that their learning is supported in a meaningful way
Chief of Nursing and Professional Practice will lead this continued work regarding role definition
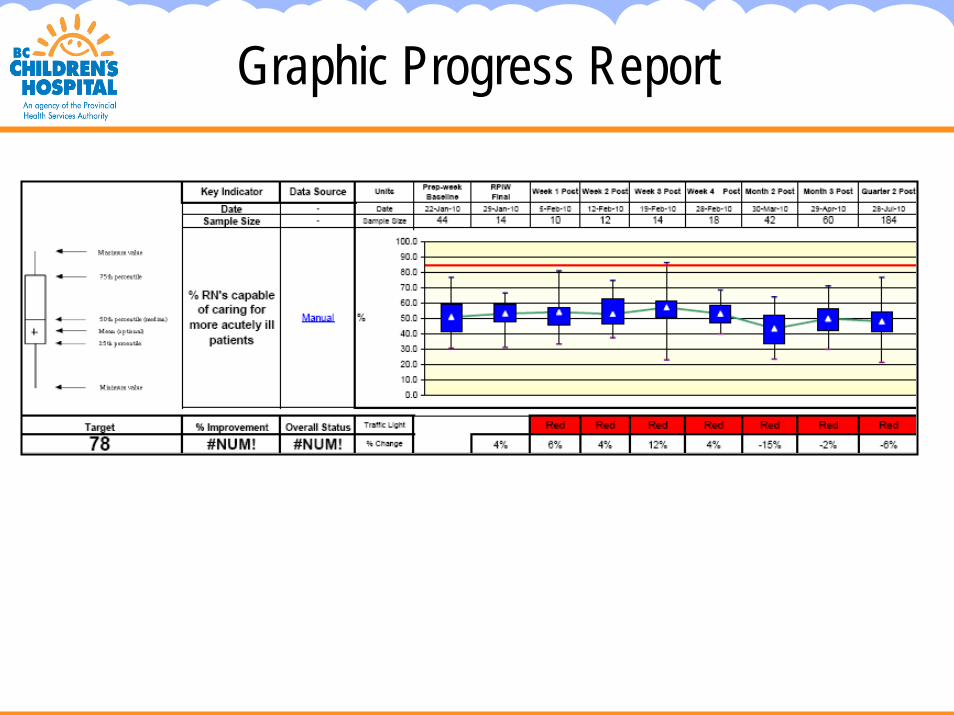
Progress Report
Graphic Progress Report
Rolling Out to Staff
professional development session in September
early testing and evaluation – very goodcleartransparentstaff aware expectations
Ongoing Evaluation
continued tracking of performance measures
rolled into performance improvement initiative
Vitality Scores – to be repeated every 6 months on an ongoing basis