Diabetes Mellitus and Diabetes Mellitus and Disorders of Glucose Disorders of Glucose Homeostasis Homeostasis Rosen’s Chapter 124 Rosen’s Chapter 124 December 21, 2006 December 21, 2006 Presented by: Dr. D’Isa-Smith Presented by: Dr. D’Isa-Smith Prepared by: Michael Savino, DO Prepared by: Michael Savino, DO (PGY-2) (PGY-2)
Transcript
Diabetes Mellitus and Diabetes Mellitus and Disorders of Glucose Disorders of Glucose
Presented by: Dr. D’Isa-SmithPresented by: Dr. D’Isa-Smith
Prepared by: Michael Savino, DO (PGY-2)Prepared by: Michael Savino, DO (PGY-2)
Normal PhysiologyNormal Physiology• Normal glucose range: 60-150 mg/dLNormal glucose range: 60-150 mg/dL• Normal plasma glucose levels are critical Normal plasma glucose levels are critical
to survival, because glucose is main fuel to survival, because glucose is main fuel for CNSfor CNS
• CNS does not synthesize glucose and only CNS does not synthesize glucose and only stores a few minutes supply of glucose.stores a few minutes supply of glucose.
• Brief hypoglycemia can cause profound Brief hypoglycemia can cause profound brain dysfunctionbrain dysfunction
• Prolonged severe hypoglycemia can Prolonged severe hypoglycemia can cause cellular deathcause cellular death
GlucoseGlucose
• Derived from 3 sources:Derived from 3 sources:• 1. intestinal absorption1. intestinal absorption• 2. glycogenolysis – glycogen breakdown2. glycogenolysis – glycogen breakdown• 3. gluconeogenesis – glucose formed from 3. gluconeogenesis – glucose formed from
precursors such as lactate, pyruvate, amino precursors such as lactate, pyruvate, amino acids, glycerolacids, glycerol
• After glucose ingestion, plasma levels After glucose ingestion, plasma levels rise and endogenous production is rise and endogenous production is suppressed.suppressed.
InsulinInsulin
cells of the pancreas detect elevated cells of the pancreas detect elevated glucose levels triggering release of insulin glucose levels triggering release of insulin into the hepatic portal circulationinto the hepatic portal circulation
• Major anabolic hormone in diabetic disorderMajor anabolic hormone in diabetic disorder• Stimulates glucose uptake, storage, and use Stimulates glucose uptake, storage, and use
by other insulin-sensitive tissues (fat, by other insulin-sensitive tissues (fat, muscle)muscle)
• Half-life of insulin is about 3-10 minutesHalf-life of insulin is about 3-10 minutes• Metabolized through the liver and kidneyMetabolized through the liver and kidney
Liver and KidneyLiver and Kidney
• Liver and kidney contain Liver and kidney contain glucose-6-glucose-6-phosphatasephosphatase – enzyme necessary for – enzyme necessary for the release of glucose into the the release of glucose into the circulationcirculation
• The liver is the sole source of The liver is the sole source of endogenous glucose production in endogenous glucose production in normal conditionsnormal conditions
• The kidney undergoes The kidney undergoes gluconeogenesis under prolonged gluconeogenesis under prolonged starvationstarvation
• Hepatocytes do not require insulin Hepatocytes do not require insulin for glucose transport across cell for glucose transport across cell membranemembrane
• But, insulin augments hepatocyte But, insulin augments hepatocyte glucose uptake and storage for glucose uptake and storage for energyenergy
• Insulin inhibits hepatic Insulin inhibits hepatic gluconeogenesis and glycogenolysisgluconeogenesis and glycogenolysis
Muscle cellsMuscle cells
• Can store and use glucose via glycolysisCan store and use glucose via glycolysis• In muscle: glucose In muscle: glucose pyruvate pyruvate• Pyruvate Pyruvate lactate or alanine lactate or alanine
transported to liver transported to liver precursor for precursor for gluconeogenesisgluconeogenesis
Fasting conditions:Fasting conditions:
glucose uptake – use fatty acids as glucose uptake – use fatty acids as energy, mobilize amino acids to liver for energy, mobilize amino acids to liver for energy.energy.
• The major catabolic agent that increases blood The major catabolic agent that increases blood glucoseglucose
• cells of pancreas cells of pancreas • Released in response to hypoglycemia, stress, Released in response to hypoglycemia, stress,
trauma, infection, starvation.trauma, infection, starvation.• Decreases glycoloysis, increases gluconeogenesisDecreases glycoloysis, increases gluconeogenesis• Increases ketone production in liverIncreases ketone production in liver
• Epinephrine – Epinephrine – hepatic glucose production hepatic glucose production and limits glucose use through a and b and limits glucose use through a and b adrenergic mechanisms adrenergic mechanisms • acts directly: glycogenolysis, gluconeogenesisacts directly: glycogenolysis, gluconeogenesis
• Norepinephrine – similar to epinephrineNorepinephrine – similar to epinephrine• Growth hormone and cortisol – initially Growth hormone and cortisol – initially
glucose, but long-term glucose, but long-term glucose glucose
Types of DiabetesTypes of Diabetes
• Type 1 Diabetes Mellitus Type 1 Diabetes Mellitus • Type 2 Diabetes Mellitus Type 2 Diabetes Mellitus • Gestational DiabetesGestational Diabetes• Impaired Glucose ToleranceImpaired Glucose Tolerance
Type 1 DMType 1 DM
• Failure to produce insulin. Failure to produce insulin. Tendency to ketosis Tendency to ketosis
• Parenteral insulin required to Parenteral insulin required to sustain lifesustain life
• Autoimmune destruction of Beta Autoimmune destruction of Beta cells of pancreascells of pancreas
• Strong association with HLA Strong association with HLA
Type 1 DMType 1 DM
• Typical patient is lean, younger than 40, Typical patient is lean, younger than 40, prone to ketosis. prone to ketosis.
• Plasma insulin levels are low or absent.Plasma insulin levels are low or absent.• Glucagon levels are high, but Glucagon levels are high, but
suppressible with insulinsuppressible with insulin• Symptoms of polydipsia, polyuria, Symptoms of polydipsia, polyuria,
polyphagia, and wt. loss develop rapidlypolyphagia, and wt. loss develop rapidly• Complications incl: DKA, retinopathy, Complications incl: DKA, retinopathy,
• Typical patient is middle aged or older, Typical patient is middle aged or older, overweight, normal to high insulin overweight, normal to high insulin levels. levels.
• Impaired insulin function related to poor Impaired insulin function related to poor insulin production, failure of insulin to insulin production, failure of insulin to reach the site of action, or failure of end reach the site of action, or failure of end organ response to insulinorgan response to insulin
• Symptoms begin more gradually than in Symptoms begin more gradually than in Type 1Type 1
Type 2 DM - SubgroupsType 2 DM - Subgroups
• Most are obese, but 20% are notMost are obese, but 20% are not• Nonobese Type 2 patients present Nonobese Type 2 patients present
more like Type 1more like Type 1• Young persons with mature-onset Young persons with mature-onset
diabetesdiabetes
Type 2 DMType 2 DM
• Symptoms come on graduallySymptoms come on gradually• Diagnosis usually made by elevated Diagnosis usually made by elevated
blood glucose on routine lab workblood glucose on routine lab work• Blood glucose levels controlled by Blood glucose levels controlled by
diet, oral hypoglycemics, or insulin.diet, oral hypoglycemics, or insulin.• Decompensation usually leads to Decompensation usually leads to
hyperosmolar nonketotic comahyperosmolar nonketotic coma rather than ketosis.rather than ketosis.
Gestational DiabetesGestational Diabetes
• Characterized by abnormal oral Characterized by abnormal oral glucose tolerance test (OGTT). glucose tolerance test (OGTT).
• During pregnancyDuring pregnancy• Reverts to normal in postpartum Reverts to normal in postpartum
period or remains abnormalperiod or remains abnormal• Clinical pathogenesis similar to Type 2Clinical pathogenesis similar to Type 2• Clinical presentation usually Clinical presentation usually
nonketotic hyperglycemianonketotic hyperglycemia during during pregnancypregnancy
Impaired Fasting GlucoseImpaired Fasting Glucose• Plasma glucose levels between normal Plasma glucose levels between normal
and diabetic and who are at increased and diabetic and who are at increased risk for development of diabetesrisk for development of diabetes
• Pathogenesis related to insulin Pathogenesis related to insulin resistanceresistance
• Presentations: nonketotic Presentations: nonketotic hyperglycemia, insulin resistance, hyperglycemia, insulin resistance, hyperinsulinism, often obesityhyperinsulinism, often obesity
• Less complications than diabetesLess complications than diabetes
Diagnostic StrategiesDiagnostic StrategiesDiagnosis made by:Diagnosis made by:• Random plasma glucose > 200 mg/dLRandom plasma glucose > 200 mg/dL• or Fasting glucose > 140 mg/dLor Fasting glucose > 140 mg/dL• or 2 hr postload OGTT or 2 hr postload OGTT
• HbA1c – high glucose binds to Hb HbA1c – high glucose binds to Hb chain. chain. Half-life of RBC’s allows index of [glucose] Half-life of RBC’s allows index of [glucose] for prior 6-8 weeks (normal 4-6%)for prior 6-8 weeks (normal 4-6%)
• Glucose dipstick tests use glucose oxidaseGlucose dipstick tests use glucose oxidase• Ketone dipstick tests use nitroprusside rxn.Ketone dipstick tests use nitroprusside rxn.
• Generally more accurate than Generally more accurate than urine dipurine dip
• Hematocrits <30% or >55% cause Hematocrits <30% or >55% cause unduly high or low readings, unduly high or low readings, respectivelyrespectively
HypoglycemiaHypoglycemia
• Common problem in Type 1 diabeticsCommon problem in Type 1 diabetics• 9 – 120 episodes per 100 patient-years9 – 120 episodes per 100 patient-years• Severe hypoglycemia associated with Severe hypoglycemia associated with
blood sugar below 40-50 mg/dL and blood sugar below 40-50 mg/dL and impaired cognitive functionimpaired cognitive function
• Hypoglycemia unawarenessHypoglycemia unawareness – a – a dangerous complication of Type 1. Pts dangerous complication of Type 1. Pts become unarousable without warningbecome unarousable without warning
• Somogyi phenomenonSomogyi phenomenon
Hypoglycemia - Hypoglycemia - symptomssymptoms
• Blood glucose level below 40-50 mg/dLBlood glucose level below 40-50 mg/dL• Rate at which glucose decreases, age, Rate at which glucose decreases, age,
gender, overall health, and previous gender, overall health, and previous hypoglycemic reactions all contribute to hypoglycemic reactions all contribute to symptom severitysymptom severity
• S/Sx caused by excessive epinephrine S/Sx caused by excessive epinephrine secretion and CNS dysfunction: secretion and CNS dysfunction: • SweatingSweating• Nervousness, tremorNervousness, tremor• TachycardiaTachycardia• Bizarre behavior, confusionBizarre behavior, confusion• SeizuresSeizures• ComaComa
• Check serum glucose; if strong suspicion treat Check serum glucose; if strong suspicion treat before results availablebefore results available
• 2. Correct serum glucose2. Correct serum glucose• If awake, cooperative: PO intakeIf awake, cooperative: PO intake• If unable to take PO: 25-75 g glucose as D50W If unable to take PO: 25-75 g glucose as D50W
(1-3 amps) IV(1-3 amps) IV• Children: 0.5-1 g/kg glucose as D25W IVChildren: 0.5-1 g/kg glucose as D25W IV• Neonates: 0.5-1 g/kg glucose as D10W IVNeonates: 0.5-1 g/kg glucose as D10W IV
• If unable to get IV access: 1-2 mg glucagon IM If unable to get IV access: 1-2 mg glucagon IM or SC; may repeat q20 minor SC; may repeat q20 min
• Glucagon – onset of action 10-20 min, peaks at 30-60 Glucagon – onset of action 10-20 min, peaks at 30-60 minmin
• Ineffective in alcohol-induced hypoglycemia b/c lack of Ineffective in alcohol-induced hypoglycemia b/c lack of glycogenglycogen
• ABC’sABC’s• Aspiration, seizure precautionsAspiration, seizure precautions• If ETOH suspected, give thiamineIf ETOH suspected, give thiamine• D50W should not be used in infants or D50W should not be used in infants or
young children because venous young children because venous sclerosis causes rebound hypoglycemiasclerosis causes rebound hypoglycemia
• Oral hypoglycemics (chlorpropamide) – Oral hypoglycemics (chlorpropamide) – can cause prolonged hypoglycemia. can cause prolonged hypoglycemia. Should be admitted for observationShould be admitted for observation• May require constant infusion of D10WMay require constant infusion of D10W
Hypoglycemia Hypoglycemia
• Non-diabetic patientsNon-diabetic patients• Most common cause of Most common cause of postprandial postprandial
hypoglycemiahypoglycemia is alimentary is alimentary hyperinsulinism (s/p gastrectomy, hyperinsulinism (s/p gastrectomy, gastrojejunostomy, vagotomy, gastrojejunostomy, vagotomy, pyloroplasty)pyloroplasty)
• Fasting hypoglycemiaFasting hypoglycemia – inadequate – inadequate glucose production (hormone glucose production (hormone deficiencies, enzyme and substrate deficiencies, enzyme and substrate defects, severe liver disease)defects, severe liver disease)
• Syndrome in which insulin deficiency Syndrome in which insulin deficiency and glucagon excess produce:and glucagon excess produce:• HyperglycemiaHyperglycemia• DehydrationDehydration• AcidosisAcidosis• Electrolyte imbalanceElectrolyte imbalance
• DKA is typically characterized by:DKA is typically characterized by:• Hyperglycemia over 300 mg/dL, Hyperglycemia over 300 mg/dL, • Low bicarbonate (<15 mEq/L), and Low bicarbonate (<15 mEq/L), and • Acidosis (pH <7.30) with ketonemia and Acidosis (pH <7.30) with ketonemia and
ketonuria ketonuria
Etiology of DKAEtiology of DKA
• Almost always in Type 1 DiabeticsAlmost always in Type 1 Diabetics• Non-compliance with insulinNon-compliance with insulin• Stress: (Physical or emotional) Stress: (Physical or emotional)
• May have altered mental statusMay have altered mental status• Kussmaul respirationsKussmaul respirations• Odor of acetone (sweet) on breathOdor of acetone (sweet) on breath• Signs of dehydration Signs of dehydration
• Markedly elevated glucose levels spill Markedly elevated glucose levels spill over into the urine, drawing water, over into the urine, drawing water, sodium, potassium, magnesium, sodium, potassium, magnesium, calcium, phosphorus into the urine. calcium, phosphorus into the urine.
• This combined with vomiting contribute This combined with vomiting contribute to dehydration experienced in DKAto dehydration experienced in DKA
• Exocrine pancreas dysfunction produces Exocrine pancreas dysfunction produces malabsorption, further limiting body’s malabsorption, further limiting body’s intake of fluid and electrolytes. intake of fluid and electrolytes.
• 95% of DKA patients:95% of DKA patients:• Na = normal or lowNa = normal or low• K = very low (5-7 mEq/L)K = very low (5-7 mEq/L)• Mg = very lowMg = very low• Phos = very low (3 mEq/L)Phos = very low (3 mEq/L)
• Because of dehydration and Because of dehydration and acidosis, however, these lab values acidosis, however, these lab values are reported as high!are reported as high!
Ketosis/AcidosisKetosis/Acidosis
• Adipose tissue fails to clear the circulation Adipose tissue fails to clear the circulation of lipids. Insulin deficiency results in of lipids. Insulin deficiency results in activation of hormone-sensitive lipase activation of hormone-sensitive lipase increasing free fatty acid [FFA] levels. increasing free fatty acid [FFA] levels. Overload of FFA’s on the liver oxidizes Overload of FFA’s on the liver oxidizes them to acetoacetate and Beta-them to acetoacetate and Beta-hydroxybuterate.hydroxybuterate.
• Result is oxidation of FFA’s to ketones Result is oxidation of FFA’s to ketones instead of reesterification to triglyceridesinstead of reesterification to triglycerides
• The body while increasing ketone The body while increasing ketone production, utilizes less ketones in production, utilizes less ketones in peripheral tissues leading to peripheral tissues leading to ketoacidosis.ketoacidosis.
KetoacidosisKetoacidosis
• Glucagon levels are 4-5x higher in Glucagon levels are 4-5x higher in DKA and is the most influential DKA and is the most influential ketogenic hormone.ketogenic hormone.
• Glucagon inhibits malonyl Glucagon inhibits malonyl coenzyme A and inhibits glycolysiscoenzyme A and inhibits glycolysis
• The counterregulatory hormones: The counterregulatory hormones: Epinephrine, norepinephrine, cortisol, Epinephrine, norepinephrine, cortisol, growth hormone, dopamine, and thyroxin growth hormone, dopamine, and thyroxin enhance ketogenesis indirectly by enhance ketogenesis indirectly by stimulating lipolysis.stimulating lipolysis.
• Propranolol and metyrapone can block Propranolol and metyrapone can block the effect of counterregulatory hormones. the effect of counterregulatory hormones. They have been used to prevent They have been used to prevent recurrent episodes in known DKA recurrent episodes in known DKA patients. patients.
Acidosis in clinical Acidosis in clinical presentationpresentation
• Acidotic patient attempts to increase Acidotic patient attempts to increase lung ventilation and rid the body of lung ventilation and rid the body of excess acid with Kussmaul’s respiration. excess acid with Kussmaul’s respiration. Bicarbonate is used up in the process. Bicarbonate is used up in the process.
• Current evidence suggests that acidosis Current evidence suggests that acidosis compounds the effects of ketosis and compounds the effects of ketosis and hyperosmolality to depress mental hyperosmolality to depress mental status directly.status directly.
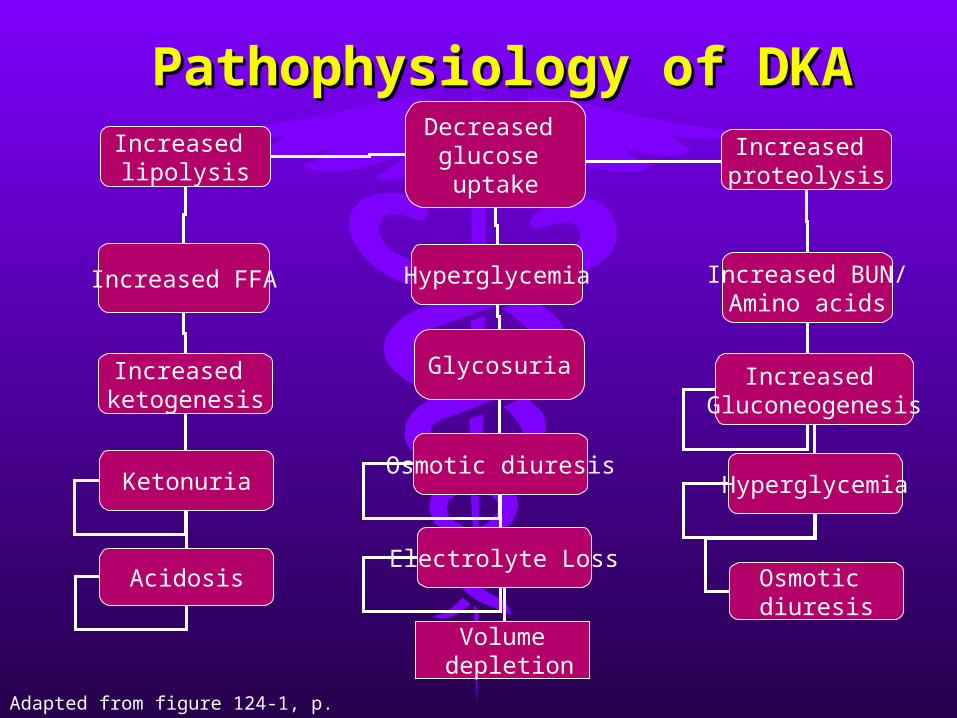
Pathophysiology of DKAPathophysiology of DKADecreased
glucose uptake
Increased lipolysis
Hyperglycemia
Increased proteolysis
Glycosuria
Increased FFA Increased BUN/Amino acids
Increased ketogenesis
Osmotic diuresis
Increased
Gluconeogenesis
Ketonuria
Electrolyte Loss
Volume depletion
Hyperglycemia
Osmotic diuresis
Acidosis
Adapted from figure 124-1, p. 1963
Laboratory TestsLaboratory Tests
• Allow confirmation of diagnosisAllow confirmation of diagnosis• serum and urine glucose serum and urine glucose (usually (usually
greater than 350, but up to 18% of greater than 350, but up to 18% of patients may have euglycemic DKA)patients may have euglycemic DKA)
ElectrolytesElectrolytes ABG/venous pH ABG/venous pH (w/ K+ if available)(w/ K+ if available)
• Obtain EKG immediatelyObtain EKG immediately
Metabolic acidosisMetabolic acidosis
• Metabolic acidosis with elevated Metabolic acidosis with elevated anion gap is secondary to elevated anion gap is secondary to elevated plasma levels of plasma levels of acetoacetateacetoacetate and and -hydroxybutyrate-hydroxybutyrate. Also . Also contributed by lactate, FFA’s, contributed by lactate, FFA’s, phosphates, volume depletionphosphates, volume depletion
and lactate levelsand lactate levels• U/A – rule out infection/renal dzU/A – rule out infection/renal dz
SodiumSodium• Serum sodium value often misleading!Serum sodium value often misleading!• Sodium is often low in presence of dehydration Sodium is often low in presence of dehydration
• Marked hyperglycemia – water flows from cells Marked hyperglycemia – water flows from cells into vessels to decrease osmolar gradient, causing into vessels to decrease osmolar gradient, causing dilutional hyponatremiadilutional hyponatremia
• Correction: Na + (Gluc – 100) * 1.6 / 100Correction: Na + (Gluc – 100) * 1.6 / 100• For every increase of 100 mg/dL glucose, For every increase of 100 mg/dL glucose,
the serum sodium decreases by 1.6 the serum sodium decreases by 1.6
HypertriglyceridemiaHypertriglyceridemia
• Common in DKACommon in DKA• Impaired lipoprotein lipase activity Impaired lipoprotein lipase activity
and hepatic overproduction of and hepatic overproduction of VLDLVLDL
AcidosisAcidosis
• Acidosis and hyperosmolarity by Acidosis and hyperosmolarity by high glucose levels shift potassium, high glucose levels shift potassium, magnesium, and phosphorous from magnesium, and phosphorous from intracellular to extracellular space. intracellular to extracellular space.
• Dehydration produces Dehydration produces hemoconcentration, which hemoconcentration, which contributes to normal-high initial contributes to normal-high initial serum potassium, mag, and phosserum potassium, mag, and phos
Calculate Correction for Calculate Correction for potassiumpotassium
• Correction for the effects of Correction for the effects of acidosis on serum potassium:acidosis on serum potassium:• Subtract 0.6 mEq/L from lab K+ for Subtract 0.6 mEq/L from lab K+ for
every 0.1 decrease in pH on ABG’severy 0.1 decrease in pH on ABG’s• Ex: if K+ is reported as 5 mEq/L and Ex: if K+ is reported as 5 mEq/L and
the pH is 6.94, the corrected K+ = 2 the pH is 6.94, the corrected K+ = 2 mEq/LmEq/L
Management of DKAManagement of DKA
• Consider intubation in vomiting Consider intubation in vomiting decompensated patient for airway protectiondecompensated patient for airway protection
• Once intubated, hyperventilation should be Once intubated, hyperventilation should be maintained to prevent worsening acidosismaintained to prevent worsening acidosis
• Hypovolemic shock: requires aggressive fluid Hypovolemic shock: requires aggressive fluid resuscitation with 0.9% NSS, rather than resuscitation with 0.9% NSS, rather than pressorspressors• Consider other causes of shock: MI, sepsisConsider other causes of shock: MI, sepsis
• 1. Rehydrate: 1-2 L NSS over 1-3 hours1. Rehydrate: 1-2 L NSS over 1-3 hours• Children: 20 mL/kg NSS over first hr, then follow w/ 0.45% Children: 20 mL/kg NSS over first hr, then follow w/ 0.45%
NSSNSS
• 2. Insulin – bolus 0.1 U/kg regular IV2. Insulin – bolus 0.1 U/kg regular IV• Maintenance: 0.1 U/kg/hr regular IVMaintenance: 0.1 U/kg/hr regular IV• Change to D5W/0.45%NS when glucose <300 mg/dLChange to D5W/0.45%NS when glucose <300 mg/dL
• 3. Correct electrolytes. 3. Correct electrolytes. • Na – 0.9% NSS and 0.45%Na – 0.9% NSS and 0.45%• K – add 20-40 mEq KCl to each liter. Ensure good renal K – add 20-40 mEq KCl to each liter. Ensure good renal
fxnfxn• Phos – usually not necessary to replenishPhos – usually not necessary to replenish• Mg – 1-2 g MgSO4Mg – 1-2 g MgSO4
• 4. Correct acidosis – add 44-88 4. Correct acidosis – add 44-88 mEq/L bicarb to 1mEq/L bicarb to 1stst liter of IV fluids liter of IV fluids if pH < 7.0. Correct to a pH of 7.1if pH < 7.0. Correct to a pH of 7.1
• Correct underlying precipitantCorrect underlying precipitant• Monitor VS, I & O’s, serum glucose, Monitor VS, I & O’s, serum glucose,
and electrolytesand electrolytes• Admit to ICUAdmit to ICU
InsulinInsulin
• Historically, high dosages of insulin Historically, high dosages of insulin were used, but resulted in were used, but resulted in hypoglycemia and hypokalemiahypoglycemia and hypokalemia
• Now, low-dose insulin therapy with Now, low-dose insulin therapy with aggressive fluid therapy is used, aggressive fluid therapy is used, more gradual decrease in blood more gradual decrease in blood glucose levels, while decreasing glucose levels, while decreasing risk of hypokalemiarisk of hypokalemia
InsulinInsulin
• May start with bolus of 10 units regular May start with bolus of 10 units regular insulininsulin
• Or infuse regular insulin at a rate of 0.1 Or infuse regular insulin at a rate of 0.1 U/kg/hr up to 5-10 U/hr, mixed with IV U/kg/hr up to 5-10 U/hr, mixed with IV fluids.fluids.
• In children, dosing is 0.1 U/kg. In children, dosing is 0.1 U/kg. Reduction of plasma glucose should be Reduction of plasma glucose should be more gradual because of greater risk of more gradual because of greater risk of developing cerebral edema.developing cerebral edema.
• Half-life of regular insulin is 3 – 10 Half-life of regular insulin is 3 – 10 minutes. minutes.
• Therefore, it should be infused, rather Therefore, it should be infused, rather than given as repeated boluses.than given as repeated boluses.
• When blood glucose has dropped to When blood glucose has dropped to 250-300 mg/dL, then start 250-300 mg/dL, then start D5W/0.45% NS to prevent iatrogenic D5W/0.45% NS to prevent iatrogenic hypoglycemia and cerebral edemahypoglycemia and cerebral edema
ComaComa• Acute diabetic decompositionAcute diabetic decomposition• Results from severe dehydration that Results from severe dehydration that
results from sustained hyperglycemic results from sustained hyperglycemic diuresis, in which patient is unable to diuresis, in which patient is unable to drink enough fluids to sustain hydrationdrink enough fluids to sustain hydration
• Absence of ketoacidosis is unknown, but Absence of ketoacidosis is unknown, but FFA levels are lower than in DKA, thus FFA levels are lower than in DKA, thus less substrates to form ketones. Most less substrates to form ketones. Most likely because still producing tiny amount likely because still producing tiny amount of insulin required to block ketogenesisof insulin required to block ketogenesis
• More common in elderly with Type 2, but has More common in elderly with Type 2, but has been reported in children with Type 1been reported in children with Type 1
• May occur in pts who are not diabetic: after May occur in pts who are not diabetic: after burns, parenteral hyperalimentation, burns, parenteral hyperalimentation, peritoneal dialysis, or hemodialysisperitoneal dialysis, or hemodialysis
• Clinically: signs of dehydration and CNS Clinically: signs of dehydration and CNS findings predominatefindings predominate
• Most common associated diseases: CRI, gm – Most common associated diseases: CRI, gm – pneumonia/sepsis, GI bleedingpneumonia/sepsis, GI bleeding
• On average, the HHNC patient has 24% or 9L On average, the HHNC patient has 24% or 9L fluid fluid deficitfluid fluid deficit
Treatment of HHNCTreatment of HHNC• Identify HHNCIdentify HHNC• Rehydrate: 2-3 L NSS over first few hours. Rehydrate: 2-3 L NSS over first few hours.
Correct ½ fluid deficit in first 8 hours, Correct ½ fluid deficit in first 8 hours, remainder over remaining 24 hrsremainder over remaining 24 hrs
• Insulin – bolus 0.05-0.1 U/kg regular IVInsulin – bolus 0.05-0.1 U/kg regular IV• Maintenance: 0.05-0.1 U/kg/hr regular IVMaintenance: 0.05-0.1 U/kg/hr regular IV• Change to D5W/0.45%NS when glucose <300 mg/dLChange to D5W/0.45%NS when glucose <300 mg/dL
• . Correct electrolytes. . Correct electrolytes. • Na – 0.9% NSS and 0.45%Na – 0.9% NSS and 0.45%• K – add 20-40 mEq KCl to each liter. Ensure good K – add 20-40 mEq KCl to each liter. Ensure good
renal fxnrenal fxn• Phos – usually not necessary to replenishPhos – usually not necessary to replenish• Mg – 1-2 g MgSO4Mg – 1-2 g MgSO4
• 4. Correct acidosis – add 44-88 4. Correct acidosis – add 44-88 mEq/L bicarbonate to 1mEq/L bicarbonate to 1stst liter of IV liter of IV fluids if pH < 7.0. Correct to a pH fluids if pH < 7.0. Correct to a pH of 7.1of 7.1
• Correct underlying precipitantCorrect underlying precipitant• Monitor VS, I & O’s, serum glucose, Monitor VS, I & O’s, serum glucose,
and electrolytesand electrolytes• Admit to ICUAdmit to ICU
Late complications of Late complications of DMDM
• Develop 15-20 yrs after overt Develop 15-20 yrs after overt hyperglycemiahyperglycemia
• VascularVascular – atheroslerosis, – atheroslerosis, thromboembolic complications. Probably thromboembolic complications. Probably related to oxidated low-density lipoprotein related to oxidated low-density lipoprotein and increased platelet activity. CAD, and increased platelet activity. CAD, stroke, silent MI, claudication, non-healing stroke, silent MI, claudication, non-healing ulcers, and impotenceulcers, and impotence
• Diabetic nephropathyDiabetic nephropathy – renal disease is – renal disease is leading cause of death and disability in leading cause of death and disability in diabetic patients. diabetic patients. • Two pathological patterns: diffuse and nodularTwo pathological patterns: diffuse and nodular
• RetinopathyRetinopathy – diabetes leading cause of – diabetes leading cause of adult blindness in US. (11-18% of adult blindness in US. (11-18% of diabetics) diabetics) • Background (simple) retinopathyBackground (simple) retinopathy• Proliferative retinopathyProliferative retinopathy
• Complaints range from acute blurring of Complaints range from acute blurring of vision to sudden unilateral /bilateral vision to sudden unilateral /bilateral blindness. Also may have “snowflake” blindness. Also may have “snowflake” cataract (vision improves with decreasing cataract (vision improves with decreasing blood glucose levels)blood glucose levels)
• NeuropathyNeuropathy – peripheral neuropathy in 15- – peripheral neuropathy in 15-60%. Poorly understood60%. Poorly understood
• Diabetic vascular dz effects on vasa Diabetic vascular dz effects on vasa nervorum, myoinositol, polyol pathway, and nervorum, myoinositol, polyol pathway, and protein glycosylation may have rolesprotein glycosylation may have roles
principle contributors to diabetic foot disease. principle contributors to diabetic foot disease. Loss of sensation Loss of sensation pressure necrosis pressure necrosis
• Must be Xrayed, no weight bearing, assessed Must be Xrayed, no weight bearing, assessed for infectionfor infection
• Mild vs Deep infections managed differentlyMild vs Deep infections managed differently• Mild: gram +, oral abiotics, no wt bearing, homeMild: gram +, oral abiotics, no wt bearing, home• Deep: full-thickness, cellulitis > 2cm, Deep: full-thickness, cellulitis > 2cm,
lymphangitis, bone involvement. Polymicrobial: lymphangitis, bone involvement. Polymicrobial: aerobic gm + cocci, gm – bacilli, and anaerobesaerobic gm + cocci, gm – bacilli, and anaerobes
• Require hospitalization, cultures, IV tx with amp-Require hospitalization, cultures, IV tx with amp-sulbactam, ticarcillin-sulbactam, cefoxitin, imipenem, or sulbactam, ticarcillin-sulbactam, cefoxitin, imipenem, or fluoroquinolone + clindamycin. Debridement, no wt. fluoroquinolone + clindamycin. Debridement, no wt. bearingbearing
InfectionsInfections
• Diabetics at increased risk of Diabetics at increased risk of extremity infections and extremity infections and pyelonephritispyelonephritis
• Tuberculosis, mucocutaneous Tuberculosis, mucocutaneous candidiasis, intertrigo, mucormycosis, candidiasis, intertrigo, mucormycosis, soft tissue infections, nonclostridial soft tissue infections, nonclostridial gas gangrene, osteomyelitis, and gas gangrene, osteomyelitis, and malignant otitis externa.malignant otitis externa.
Cutaneous Cutaneous manifestationsmanifestations
• Dermal hypersensitivity – pruritic, Dermal hypersensitivity – pruritic, red, induration at insulin injection red, induration at insulin injection sitessites
• Insulin lipoatrophyInsulin lipoatrophy• Insulin lipohypertrophyInsulin lipohypertrophy• Insulin pumps – sensitivity to Insulin pumps – sensitivity to
catheterscatheters
Oral Hypoglycemic Oral Hypoglycemic AgentsAgents
• Sulfonylureas (developed 1940’s) – mainstay of Sulfonylureas (developed 1940’s) – mainstay of treatment. Increase insulin secretion by binding treatment. Increase insulin secretion by binding to specific beta cell receptors. Risk of to specific beta cell receptors. Risk of hypoglycemiahypoglycemia
• Repaglinide – similar to sulfonylureas. More Repaglinide – similar to sulfonylureas. More rapid onset, but less risk of hypoglycemia. OK rapid onset, but less risk of hypoglycemia. OK with sulfa allergies.with sulfa allergies.
• Metformin – decreases hepatic glucose output. Metformin – decreases hepatic glucose output. Contraindicated in renal insufficiency and Contraindicated in renal insufficiency and metabolic acidosis. Withold for 48 hours of metabolic acidosis. Withold for 48 hours of iodinated contrast media b/c risk of acidosisiodinated contrast media b/c risk of acidosis
• Alpha glucosidase inhibitors delay intestinal Alpha glucosidase inhibitors delay intestinal absorption and prevent complex carb breakdown. absorption and prevent complex carb breakdown. GI side effects, monitor liver enzymes GI side effects, monitor liver enzymes
New med on the blockNew med on the block
• Byetta (Exetinide) – first in a class of Byetta (Exetinide) – first in a class of encretin mimetics. encretin mimetics.
• ““mimics” the enhancement of glucose-mimics” the enhancement of glucose-dependent insulin secretiondependent insulin secretion
• For Type 2 DMFor Type 2 DM• Used with metformin and/or sulfonylureaUsed with metformin and/or sulfonylurea• Pre-filled injection pen (SQ)Pre-filled injection pen (SQ)• Dose: 5 mcg BID for first 30 daysDose: 5 mcg BID for first 30 days