DIARE Def : increased water volume in stools Mechanism : increased secretion & decreased absorption Major mechanism in pathogenesis of diarrhea Effect on Net Transport of Water Mechanism Examples Increased secretion Enterotoxin Cholera toxin, E.coli, LT & ST Intraluminal metabolites Dihydroxy bile acids, fatty acids Hormone & neurotransmitter VIP, CCK, acetylcholine Other endogenous agents prostaglandins Laxatives Diocryl sodium sulfosuccinate (coloxyl) Senna compounds Decreased absorption Loss of area of absorbing surface Intestinal resection Mucosal damage Celiac disease Gastroenteritis (particularly viral) Osmotic diarrhea Sugar intolerance Lactulose Chloridorrhea Rapid intestinal transit Gastroenteritis Hormones (CCK, motilin) I.Increased Secretion Most commonly caused by bacterial endotoxin These agents can increase intracellular concentration of cAMP/cGMP/calcium lead to changes in ion channels/transport ENTEROTOXIN Enterotoxin Affecting cAMP Cholera toxin (CT) & E.coli heat-labile toxin (LT) Consist of : B subunit to bind to cell surface A subunit to activete adenylate cyclase Steps : 1. CT (B subunit) bind to GM1 membrane receptor 2. A subunit divide into A1 & A2 fragments 3. Penetration A subunit (water soluble) enter cells & reaches basolateral membrane to activete adenylate cyclase 4. A1 irreversibly inhibit GTPase (GTP: bindsto regulatory unit in adenylate cyclase) so, the unit remain activated
Transcript
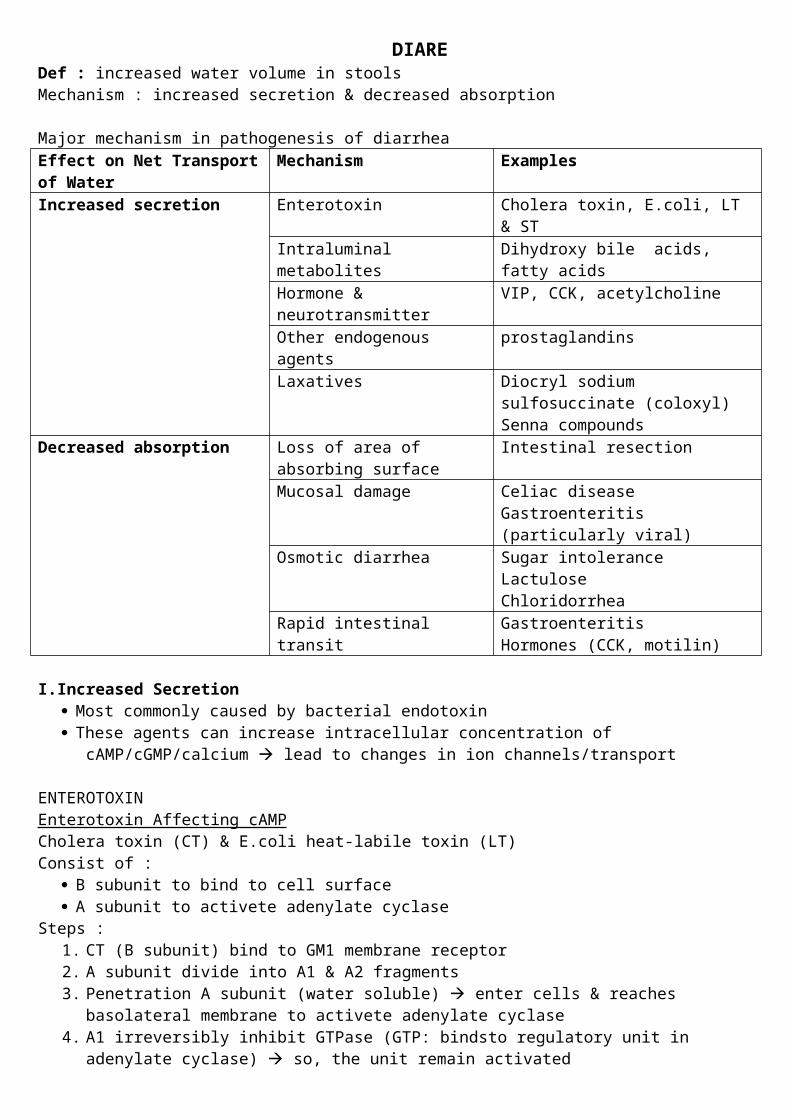
DIAREDef : increased water volume in stoolsMechanism : increased secretion & decreased absorption
Major mechanism in pathogenesis of diarrheaEffect on Net Transport of Water
I.Increased Secretion Most commonly caused by bacterial endotoxin These agents can increase intracellular concentration of cAMP/cGMP/calcium lead to changes in ion
B subunit to bind to cell surface A subunit to activete adenylate cyclase
Steps :1.CT (B subunit) bind to GM1 membrane receptor2.A subunit divide into A1 & A2 fragments3.Penetration A subunit (water soluble) enter cells & reaches basolateral membrane to activete adenylate
cyclase4.A1 irreversibly inhibit GTPase (GTP: bindsto regulatory unit in adenylate cyclase) so, the unit remain
activated5.Adenylate cyclase also have catalytic unit which response to regulatory unit6.Adenylate cyclase yielding cAMP activate protein kinase phosphorilation membrane protein
modify ion channel & transport :o Cl- permeability ↑o NaCl uptake ↓o HCO3
- secretion ↑CT also ↑ intestinal peristalsisEffects of LT is similar, but less fluid secretion than CT
Enterotoxin Affecting cGMP- E.coli heat-stable toxin (ST) & other enterobacteria (eg.Yersenia) can incresae intracellular cGMP- The response is immediate & reversible- ST has2 type : methanol-soluble STA(ST I) & methanol insoluble STB (ST II)
- Mechanism 2 modelso First model :
@ brush border, ST bind to receptor ↓
resulting in phopholipase-activated arachidonic acid cascade ↓
produce metabolites for stimulating guanylate cyclaseo Second model :
STA bind to guanylate cyclase ↓
produce conformational changes ↓
activate catalytic unit, cGMP↑↓
Phosphorylation of membrane protein↓
Changes in transport of electrolytes & water
Enterotoxin Affecting Ca-calmodulin- Intercellular Ca2+ regulation Na+ & Cl- transport in small & large intestine
- C.difficile enterotoxin is an enterotoxin for which Ca2+ has been emplicated as the direct 2nd messenger- E.histolytica secretes peptides (eg.substance P) that can stimulate secretion through a calmodulin-
dependent mechanism- Ca2+ & calmodulin system : ultimate mediator of intestinal secretion
Cytotoxic Enterotoxins- Several bacteria produce exotoxins which cause fluid accumulation in the intestine, therefore enterotoxins- It also capable of causing tissue damage in cell systems (in vivo), therefore cytotoxins- Mechanism : uncertain
Mechanism of Action of Bacterial EnterotoxinsIncrease in cAMP Increase in cGMP Ca2+-
calmodulinCytotic Enterotoxins
Vibrio choleraeE.coli LTSalmonella spp.Aeromonas spp.C.jejuniShigella dysenteriae I
INTRALUMINAL METABOLITES- Dihydroxy bile acids and Hydroxy & nonhydroxy fatty acids secretagogues, potential to cause
diarrhea- Effects: related to ileal disease (short segments: bile acids & long segments: fatty acids) increase
intracellular cAMP, & their secretory effects may be mediated by calcium-ionophore-like activity- They also increase mucosal permeability & mucosal damage (increase prostaglandin increase
secretion), intestinal motility changes- In the patient w/inflammatory disease : bacterial overgrowth in small bowel bacterial metabolites
affect net fluid absorption & osmolality
HORMONES & NEUROTRANSMITTER
- Vasoactive intestinal peptide (VIP) & its peptide; peptide histidine methionin; peptide histidine valine are potent secretory agents
OTHER ENDOGENOUS AGENTS- Histamine : capable causing intestinal secretion- Bradykinin : increases cAMP- Kinins : potential mediators of intestine secretion- Prostaglandin (PG), derivatives fatty acids, produce intestinal secretion of cAMP in small & large
intestine & affect intestine motility
LAXATIVES- Mech : many are similar to bile salts & fatty acids, include :
o Inhibition of Na/K ATPase activityo Elevation of cAMPo Mucosal injury, PG release
- Jg ada yg meiliki Ca2+-ionophore effects
II.Decreased Absorption
DECREASED SURFACE AREA & MUCOSAL DAMAGE- Surface area for absorption yg decrease berkaitan dengan mucosal damage- Pada gastroenteritis (esp.viral) productionin villous area is seen- Decreased of several enzymes, eg. NaKAtpase may also limit absorption
Unabsorbed carbohydrate and bacterial metabolism of CH in colon↓
increase osmolality of intestinal contents↓
Diarrhea- Mannitol also reduce absorption- Defective in exchange between Cl- & HCO3- also leads to increase in osmolality
RAPID INTESTINAL TRANSITContraction of longitudinal fibers & Loss of haustral contractions
↓Rapid intestinal transit
↓Slowing absorption
↓Diarrhea
- Shigella dysentriae, CCK, ricinoleic acid can produce this type- Loperamide (opiate derivatives) is an antidiarrheal drugs that act by slowing intestinal transit
INFECTIVE DIARRHEA
Epidemiology- Pattern depend on host & environmental factors (hygiene, food & waste supplies, age, etc)- Developing countries : commonest agents were ETEC, Rotavirus, & shigella- Day-care centers for young children reservoirs of respiratory & enteric pathogens
Etiology- Hospital study :
o Rotavirus (47%)o ETEC (22%)
o C.difficile (16%)o Entero-adherent E.coli (15%)o Etc shigella and salmonella
Viral Diarrhea- Major cause of diarrheal disease, particularly in children < 2 years old- Main cause : rotavirus- Others : Norwalk virus, enteric adenovirus, calicivirus, & astrovirus
Rotaviruses- Typically an endemic infection of infants & young children; older patient are not commonly affected- Also in young animals : calves, piglets
Microbiology- Family Reoviridae- D = 70nm, when complete, have an inner & outer capsid, although single-shelled particle are commonly
seen- There is a genome consisting of 11 segments of dsRNA- Outer capsid :
hemaglutinin VP4 (as a virulence factor) f(x) : proteolysis in the intestinal lumen before infection can be established
major constituent : VP7, glycoprotein responsible for serotype- inner capsid : VP6, protein which determine group antigenicity- Classified into 5 group (A-E) based on antigenic epitopes on the internal structural protein VP6- group : A, B, C infects human- A most frequent human pathogens; associated mainly w/gastroenteritis in infants & young children- B associated w/epidemic diarrhea in adults in China- C related to sporadic diarrhea in children
Epidemiology- In developed countries, rotavirus probably accounts for up to 8.5 hospital admission per 1000 children- Seasonal pattern : mainly in winter, in tropical climates cases are distributed thru out the year- In tropical countries, hospital admission : 10-25%- Occur mainly betwenn the age of 3-15 mo (uncommon after 3 yrs)
- Transmission : fecal-oral route; symptoms usually appear within 3 days after inoculation- Shed profusely during diarrheal illness & for up to 8 days afterward - Although it has been suggested that droplet spread via respiratory tract may also occur, respiratory
symptoms & the presence of rotavirus in respiratory tract are inconsistent- Rotavirus can survive for prolonged period in water, other source is fomites & air, as well hands & food
standard disinfectants & agents for hand-washing do not control rotaviruses adequatelyPathogenesis
- Predilection : mature villous cells which become replaced w/immature enterocytes from the crypts - crypt cells lack disaccharidases & other enzymes, and also show differences from villous cells with
regard to transport of fluid & electrolytes- Coupled sodium transport is decreased & the profile of enzymes present is more similar to normal crypt
than normal villous cells- Typical appearance of small intestine : mucosa shows patchy changes with shortening of villi and virus
particles can be seen in the RE enterocytes ; disaccharidase deficiency accompanies these mucosal abnormalities
- Diarrhea probably results from a combination of : Decrease in surface area related to mucosal damage Decrease of disaccharidase level impaired glucose absorption Abnormalities of trnasport processes such as coupled sodium transport
- All of these symptoms is because of damaged cell on villi are replaced by nonabsorbing immature crypt cells
- May take 3-8 weeks for normal function to be restored
Infect cells in the villi of the small intestine(gastric & colonic mucosa are spared)
↓Multiply in the cytoplas of enterocytes & damage their transport mechanism
↓Rotavirus-encoded protein, NSP4, is a viral enterotoxin and induces secretion by trigerring a signal trnasduction
pathway ↓
Damage cells↓
Sloughed into lumen of intestine & release large quantities of virus in stool(up to 1010 particles per gram of feces)
↓Viral excretion ususally last for 2-12 days in healthy patients (prolonged in poor nutrition)
Clinical Features- Cannot be distinguished on clinical ground from other typers- Incubation period : 1-3 days- S & S
sudden onset of diarrhea & vomiting usually associated with fever abdominal pain dehydration : more commonly associated with rotaviruses than other type several authors URT preceeding or in association with rotavirus infection
- diarrhea is most severe on second or third day of the illness & usually last for 4 or 5 days- mild diarrhea may persist up to 10 days- chronic diarrhea may follow the acute infection & is often related to secondary disaccharidase deficiency- complications : intestinal hemorrhage, intussusception, Reye’s syndrome, encephalitis- neonatal period is usually mild or aymptomatic, but severe illness with dehydration and blood in
stools, necrotizing eneterocolitis, bowel perforations, & death have been reportedDiagnosis
- electron microscopy to demonstrate rotavirus in stools but is unsuitable for routine use (sensitivity 80%)
- ELISA and latex agglutination methods widely available- Rotaclone (monoclonal antibody-based system) high rates false positive- Electrophoretic detection of rotavirus RNA, gene probes, PCR detect rotavirus & its serotypes
Treatment- Supportive to correct the loss of water & electrolytes that may lead to dehydration- Cconsist of : replacement of fluid & restoration of electrolyte balance either IV or orally - Example : Oral rehydration therapy- Control meausres for transmission : waste-water treatment & sanitation- Vaccine withdrawn because of reports of intussusception (side effects)
Norwalk Virus- First identified as the cause of an outbreak of diarrhea & vomiting among primary school-children in
Norwalk-Ohio, in 1968- Smaller than rotavirus & has benn more difficult to visualize nut may be identified by immune electron
microscopy- d = 27-35 nm- Associated with epidemic diarrhea, especially in older children & adults- Made up of ssRNA & single structural protein which resembles of calcivirus
Epidemiology- May cause illness in any age group except infants and young children, at any time of the year- Outbreak associated with contaminated water and food such as salads or shellfish - Transmission :
Fecal-oral route Air-borne spread may be possible (although respiratory symptoms do not occur
- Antibody to norwalk virus become detectable at about the time of adolescence in industrialized countries, but appear earlier in developed countries
Pathogenesis- Less well understood- Histology abnormality :
proximal small bowel with pathces of broad, blunt villi and some infiltration with mononuclear cells shortening microvilli associated with impaired absorption of fat, xylose, and lactose gastric emptying is delayed nausea and vomiting activity of brush border enzyme is decreased
Clinical features- symptoms develop about 48 hour after exposure to virus- incubation period : 10 hours- vomiting, diarrhea, mild fever, headache, abdominal pain, myalgia last for 12-24 hrs- severe dehydration is unusual
Diagnosis- no specific diagnostic methods- ELISA & radioimmunoassay have been used in research lab (ELISA is more sensitive)
Norwalk-like Viruses- Characteristic is similar with norwalk virus- Symptoms similar with norwalk virus- There is some immunologic cross-reactivity between these viruses and with norwalk-like virus
Enteric Adenovirus- Serotypes 40 & 41 associated with gastroenteritis- Do not produce URT symptoms- Genom : ds-DNA- Most common cause, after rotavirus, which cause gastroenteritis in children- Most common : at infants under 12 mo, unusual after 2 yrs age- Transmission : person to person- No seasonal peak
Cinical features- Incubation period : 8-10 days- After incubation period :
watery diarrhea lasting up 2 weeks (sometimes longer) accompanying by 1 or 2 days of vomiting at the onset mild fever is usual for 2-3 days ART symptoms is rare Less likely cause severe dehydration
Diagnosis- Electron microscopy profuse adenovirus particle- Gene probes, immunoassay, examination of nucleic acid pattern
Caliciviruses- Related to norwalk virus- Occur mainly in adults- Associated with contaminated shellfish, water, and nosocomial infections- Incubation period : 1-3 days; usually affect infants & young children- Features : similar to mild rotavirus gastroenteritis- Diagnosis : immunoassays
Astroviruses- D = 27-32nm, resemble calciviruses- Consisting ss-RNA but posses 3 structural protein- Can also be distinguished by growth in cell culture & immunologic differences- Diagnosis : electron microscopy & ELISA- Incubation period 1-2 days- Clinical features : illlness resembling mild rotavirus infection, mainly in children up to ages 7 yrs
Other viruses- Coronavirus- Picobirnaviruses, pestivirus- Toroviruses
ACUTE GASTROENTERITIS IN CHILDRENDef : infection of GIT caused by bacterial, viral, or parasitic pathogenMost common manifestation : diarrhea & vomiting
Etiology- Infection acquired thru the feco-oral route or by contaminated food/water- Person-to-person contact : Shigella, E.coli, noroviruses, rotavirus, G.lamblia, E.hystolitica- Contamination of food/water supply : cholera- Most common viral agents in US ; rotavirus, noroviruses, enteric adenovirus, astrovirus- Most common pathogen in dev countries : Salmonella, Shigella, E.coli- Antibiotic-associated diarrhea & pseudomembranous colitis : Clostridium difficile
Pathogenesis1. Noninflammatory diarhhea :
enterotoxin production by some bacteria destruction of villous (surface) cells by viruses adherence by parasites adherence &/trnaslocation by bacteria
2. Inflammatory diarrhea : Bacteria that directly invade intestine/production cytotoxins w/consequent fluid, protein, & cells (RBC, WBC) that enter intestinal lumen
Risk factors- Major : environmental contamination & increased exposure to enteropathogen- Young age- Immune dificiency- Measles- Malnutrition (eg. Vit A deficiency, zinc deficiency)- Lack of exclusive/predominant breastfeeding
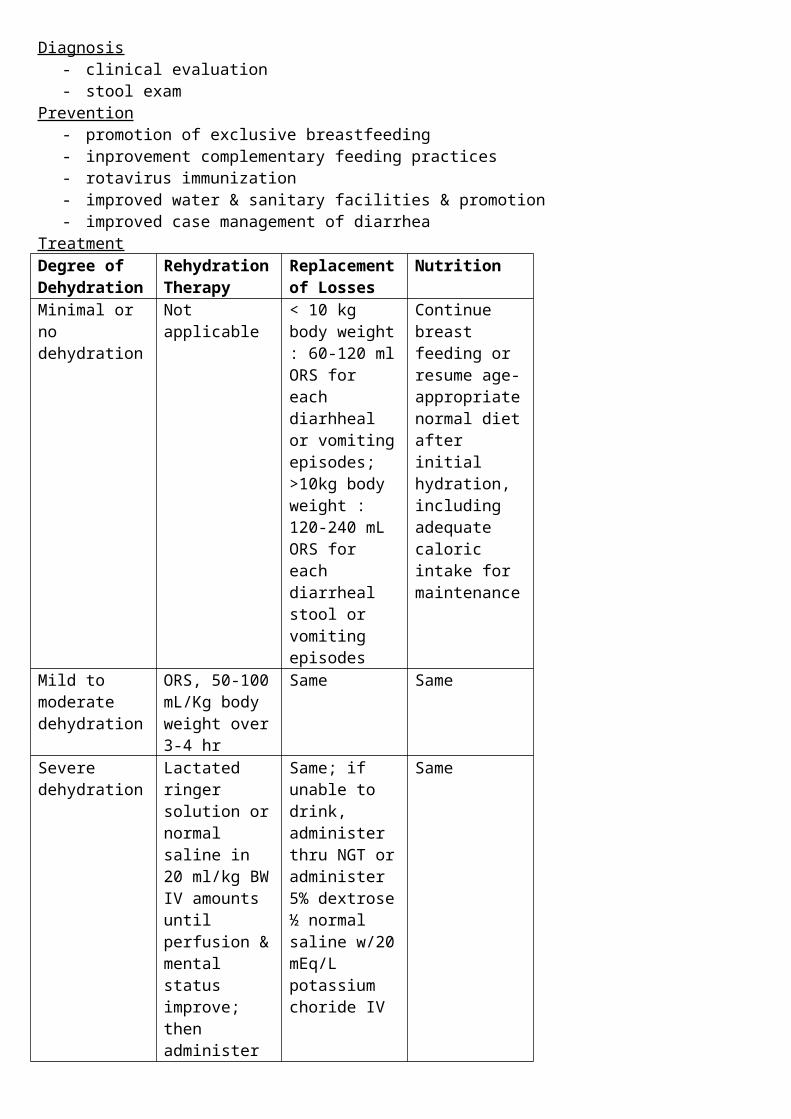
Prevention- promotion of exclusive breastfeeding- inprovement complementary feeding practices- rotavirus immunization- improved water & sanitary facilities & promotion- improved case management of diarrhea
TreatmentDegree of Dehydration
Rehydration Therapy
Replacement of Losses
Nutrition
Minimal or no dehydration
Not applicable < 10 kg body weight : 60-120 ml ORS for each
Continue breast feeding or resume age-
diarhheal or vomiting episodes; >10kg body weight : 120-240 mL ORS for each diarrheal stool or vomiting episodes
appropriate normal diet after initial hydration, including adequate caloric intake for maintenance
Mild to moderate dehydration
ORS, 50-100 mL/Kg body weight over 3-4 hr
Same Same
Severe dehydration
Lactated ringer solution or normal saline in 20 ml/kg BW IV amounts until perfusion & mental status improve; then administer 100ml/kg BW ORS over 4 hr or 5% dextrose ½ normal saline IV @ twice maintenance fluid rates
Same; if unable to drink, administer thru NGT or administer 5% dextrose ½ normal saline w/20 mEq/L potassium choride IV
Same
+ zinc supplementation+ antibiotic therapy
CHRONIC DIARRHEADef : total daily stool output, usually associated w/ increased stool water contentInfants or children >10 g/kg/24 hrAdult limit : 200 g/24 hr>2 weeks --> chronic
Patfis1. Osmotic diarrhea
- Caused by : Malabsorption of water soluble nutrients Excessive intake of carbonated fluid Excessive intake of nonabsorbable solutes
E.g. lactose intolerance due to lactase enzyme deficiency in which lactose is nor absorbed in small intestine & reaches d colon intact
↓Colonic bacteria ferment d nonabsorbed lactose to short chain organic acids
↓Generating an osmotic load
↓Causing water to be secreted into lumen
↓Osmotic diarrhea
2. Secretory diarrheaAgents2 : bind to enterocyte surface receptor
↓Toxin mediated injury to tight junction
↓Fragments of the toxin enter the cells
↓Activate adenylate cyclase on basolateral membrane via interaction w/stimulatory G protein
Non infective diarrhea DISORDER OF CARBOHYDRATE DIGESTION & ABSORPTION
caused by :- inadequancy hydrolysis of disaccaharides (disaccharidase deficiency)- failure of absorbtion of monosaccharides in the presence of normal hydrolysis
typesImpaired disaccharide digestion Impaired monosaccharide transport
Mucosal damage :- Lactase deficiency- Defiency of disaccaharidase
Monosaccharide malabsorption (all sugars)
Symptoms & Clinical Features- Sugar are normally absorbed quickly in the upper small intestine. If they are not, their presence in the
intestinal lumen provides an osmotic load, which, with distention of the gut wall by the extra content in the lumen , stimulates peristalsis passage of frequent fluid stools
- Unabsorbed sugars will in part be excreted unchanged in the feces & in part undergo bacterial degradation in the lower ileum & large gut to produce volatile fatty acids which are absorbed from the lumen, lactic acid, Co2, water, causing further fermentative diarrhea
- Main symptoms : watery, acid diarrhea- Fermentation further increases stool water content by reducing intraluminal pH below that optimal for
water resorbtion in large intestine- In young infants passage of content thru the small intestine & colon is normally more rapid than in
adults, the frequency of the stools can be very great & up to 1 L of fluid may be lost daily in this way- In infants if sugar intolerance is present the stools are watery, usually of pH 5.5 or less, iiritating to
the buttocks frequent, and passed noisily w/flatusDiagnosis
- Suggested from the watery character of stools- Detailed dietary history from births- Fluid & electrolyte losses from the diarrhea may be sufficient to cause dehydration, intestinal hurry may
cause steatorrhea- Weight may remain stationary or go down- The buttocks of the affected infant still in napkins become excoriated- Fermentation : cause gaseous distention & borborygami which sometimes leads to colicky abdominal
painInvestigation : stools may be tested for - Reducing substances :by clinitest or chromatography- Product of fermentation : pH & lactic acidOthers test :- Radiologic method- Sugar tolerance test- The breath hydrogen test- Excretion of sugar in the urine
PRIMARY DISORDER OF CH DIGESTION & ABSORPTION1. Specific disaccharidase deficiency2. Specific lactase deficiency
Two types :- Congenital alactasia rare, inborn error of development brush border β galactosidase- Late-onset hypolactasia deficient of lactase emerges of different ages after early childhood
SECONDARY DISORDER OF CH DIGESTION & ABSORPTION1. Dissacharidase Deficiency StatesOccurs in association w/may GI disorders & as some of these disorders occur frequently in infants & childrenPathology
- mucosal damage : even if only the epithelial cells & the brush border are involved- activities of disaccharidase are depressed- lactase is usually the last to return to normal (weeks-months) when recovery from the underlying GI
disorder takes placeClinical Features
- fluid diarrheaPostgastroenteritis syndrome
- commonest cause of secondary disaccharidase deficiency & disaccharide intolerance - viral gastroenteritis more commonly- Symptoms :
Fluid stool, contain felcks of feces passed forcefully w/flatus & cause excoriation of buttock Very young infants more at risk Delayed recovery occurs mostly in patients under 18 months of age, particularly in those belom 6
months Fecal fat & nitrogen losses are slightly increased in secondary lactase deficiency
Managements- Lactose-free milk, but some required dietary restriction of sucrose as well- Severity of diarrhea is proportional to the osmotic load, that is the amount of sugar ingested at any one
time- Dilution of the usual milk/frequent feeds at small volume may be helpfull
2. Secondary Monosaccharide Malabsorption
ANTIDIARRHEAL AGENTS
OPIOID AGONISTSOpioids have significant constipating effects . They increase colonic phasic segmenting activity through inhibition of presynaptic cholinergic nerves in the submucosal and myenteric plexuses and lead to increased colonic transit time and fecal water absorption. They also decrease mass colonic movements and the gastrocolic reflex. Although all opioids have antidiarrheal effects, central nervous system effects and potential for addiction limit the usefulness of most. Loperamide is a nonprescription opioid agonist that does not cross the blood-brain barrier and has no analgesic properties or potential for addiction. Tolerance to long-term use has not been reported. It is typically administered in doses of 2 mg taken one to four times daily. Diphenoxylate is another opioid agonist that has no analgesic properties in standard doses; however, higher doses have central nervous system effects and prolonged use can lead to opioid dependence. Commercial preparations commonly contain small amounts of atropine to discourage overdosage (2.5 mg diphenoxylate with 0.025 mg atropine). The anticholinergic properties of atropine may contribute to the antidiarrheal action.
COLLOIDAL BISMUTH COMPOUNDS
Chemistry & PharmacokineticsThe only bismuth compound available in the USA is bismuth subsalicylate, a nonprescription formulation containing bismuth and salicylate. In other countries, bismuth subcitrate and bismuth dinitrate are also available. Bismuth subsalicylate undergoes rapid dissociation within the stomach, allowing absorption of salicylate. Over 99% of the bismuth appears in the stool. Although minimal (< 1%) bismuth is absorbed, it is stored in many tissues and has slow renal excretion. Salicylate (like aspirin) is readily absorbed and excreted in the urine.PharmacodynamicsLike sucralfate, bismuth probably coats ulcers and erosions, creating a protective layer against acid and pepsin. It may also stimulate prostaglandin, mucus, and bicarbonate secretion. Bismuth subsalicylate reduces stool frequency and liquidity in acute infectious diarrhea, due to salicylate inhibition of intestinal prostaglandin and chloride secretion. Bismuth has direct antimicrobial effects and binds enterotoxins, accounting for its benefit in preventing and treating traveler's diarrhea. Bismuth compounds have direct antimicrobial activity against H pylori.Clinical Uses nonspecific treatment of dyspepsia and acute diarrhea prevention of traveler's diarrhea (30 mL or 2 tablets four times daily). Bismuth compounds have been used in multidrug regimens for the eradication of H pylori infection. In the
USA, a "triple therapy" regimen has been used, consisting of bismuth subsalicylate (2 tablets; 262 mg each), tetracycline (500 mg), and metronidazole (250 mg), each taken four times daily for 14 days
Adverse Effects : Bismuth causes blackening of the stool, which may be confused with gastrointestinal bleeding Liquid formulations may cause harmless darkening of the tongue prolonged usage of some bismuth compounds may rarely lead to bismuth toxicity, resulting in
encephalopathy (ataxia, headaches, confusion, seizures) High dosages of bismuth subsalicylate may lead to salicylate toxicity.
KAOLIN & PECTINKaolin is a naturally occurring hydrated magnesium aluminum silicate (attapulgite), and pectin is an indigestible carbohydrate derived from apples. Both appear to act as absorbents of bacteria, toxins, and fluid, thereby decreasing stool liquidity and number. They may be useful in acute diarrhea but are seldom used on a chronic basis. A common commercial preparation is Kaopectate. The usual dose is 1.2–1.5 g after each loose bowel movement (maximum: 9 g/d). Kaolin-pectin formulations are not absorbed and have no significant adverse effects except constipation. They should not be taken within 2 hours of other medications (which they may bind).
BILE SALT–BINDING RESINSConjugated bile salts are normally absorbed in the terminal ileum. Disease of the terminal ileum (eg, Crohn's disease) or surgical resection leads to malabsorption of bile salts, which may cause colonic secretory diarrhea. The bile salt-binding resins cholestyramine or colestipol may decrease diarrhea caused by excess fecal bile acids (see Chapter 35). The usual dose is 4–5 g one to three times daily before meals. Adverse effects include bloating, flatulence, constipation, and fecal impaction. In patients with diminished circulating bile acid pools, further removal of bile acids may lead to an exacerbation of fat malabsorption. These agents bind a number of drugs and reduce their absorption; hence, they should not be given within 2 hours of other drugs.
OCTREOTIDESomatostatin is a 14 amino acid peptide that is released in the gastrointestinal tract and pancreas from paracrine cells, D-cells, and enteric nerves as well as from the hypothalamus (see Chapter 37). It is a key regulatory peptide that has many physiologic effects:
1. It inhibits the secretion of numerous hormones and transmitters, including gastrin, cholecystokinin, glucagon, growth hormone, insulin, secretin, pancreatic polypeptide, vasoactive intestinal peptide, and 5-HT.
2. It reduces intestinal fluid secretion and pancreatic secretion. 3. It slows gastrointestinal motility and inhibits gallbladder contraction. 4. It induces direct contraction of vascular smooth muscle, leading to a reduction of portal and splanchnic
blood flow.
5. It inhibits secretion of some anterior pituitary hormones.The clinical usefulness of somatostatin is limited by its short half-life in the circulation (3 minutes) when it is administered by intravenous injection. Octreotide is a synthetic octapeptide with actions similar to somatostatin. When administered intravenously, it has a serum half-life of 1.5 hours. It also may be administered by subcutaneous injection, resulting in a 6- to 12-hour duration of action. A longer-acting formulation is available for once-monthly depot intramuscular injection.Clinical Uses :
Inhibition of endocrine tumor effects Other causes of diarrhea Other uses because it inhibits pancreatic secretion, ocreotide may be of value in patients w/pancreatic
fistula. Sometimes used in GI bleedingAdverse Effects : Impaired pancreatic secretion may cause steatorrhea, which can lead to fat-soluble vitamin deficiency Alterations in gastrointestinal motility cause nausea, abdominal pain, flatulence, and diarrhea Due to inhibition of gallbladder contractility and alterations in fat absorption, long-term use can cause
formation of sludge or gallstones in over half of patients, which rarely results in the development of acute cholecystitis
Because octreotide alters the balance between insulin, glucagon, and growth hormone, hyperglycemia or, less frequently, hypoglycemia (usually mild) can occur
Prolonged treatment with octreotide may result in hypothyroidism. Octreotide also can cause bradycardia.