Dietary intakes of calcium and vitamin D and risk of colorectal cancer in women Jennifer Lin, PhD Division of Preventive Medicine Brigham and Women’s Hospital Harvard Medical School, USA [email protected]
Transcript
Dietary intakes of calcium and vitamin D and risk of colorectal
cancer in women
Jennifer Lin, PhDDivision of Preventive MedicineBrigham and Women’s HospitalHarvard Medical School, USA
Calcium and vitamin D and colorectal cancer incidence
• Calcium may reduce risk of colorectal cancer by binding to carcinogenic bile acids and ionized fatty acids.
• Vitamin D has the potential to regulate cell proliferation and is important in calcium absorption in the gut.
• The RDA recommends calcium intake of 1000-1200 mg/day and vitamin D of 5-15 μg/day (200-400 IU/day) for healthy adults.
Calcium and colorectal cancer incidence—(1)
• Extensive efforts have been made in epidemiologic studies to evaluate calcium intake and colorectal cancer risk. However, findings have been inconclusive.
• A meta-analysis of 10 cohort studies observed a 14% risk reduction in the highest quintile of total calcium intake relative to the lowest quintile (Cho et al,2004), while the other metal-analysis study reported no association (Bergsma-Kadijk et al 1996).
Calcium and colorectal cancer incidence—(2)
• Clinical trials of calcium supplementation for the prevention of recurrence of colorectal adenomas: (1) one observed a 30% risk reduction after 1 year of follow-up among participants taking 1200 mg/day of calcium (Baron et al, 1999);
(2) another trial found that 2000 mg/day of calcium after 3 years of follow-up was associated with a modest risk reduction (Bonithon-Kopp et al, 2000).
Vitamin D and colorectal cancer incidence
• Observational findings on the association between vitamin D intake and colorectal cancer risk have also been inconclusive.
• Only three studies have reported a dose-response trend of lower colorectal cancer risk with higher vitamin D intake (La Vecchia et al 1992; Garland et al 1995; McCullough et al 2003).
Possible explanations of discrepant findings on calcium and vitamin D intake
• Methodological limitations: calcium and vitamin D supplements were not available in some studies, which may have attenuated the associations.
• Other dietary factors: Intakes of fat, phosphorus, fiber may have reduced calcium absorption in the gut.
In this study (Lin et al, 2005, Am J Epi) …
• We prospectively evaluated baseline intakes of calcium and vitamin D using both dietary sources and supplements from a large female cohort in the Women’s Health Study.
• We also evaluated whether the effect of calcium on colorectal cancer risk was modified by intakes of total fat, phosphorus, total fiber and vitamin D.
Statistical Analysis
• Relative risks (RR) and 95% confidence intervals (CI) were estimated from Cox proportional hazards regression. Tests for trend were performed by fitting the median value of each category as a continuous variable in the models. All p values were two sided.
• The models were controlled for age and randomized trial assignment, and additionally for body mass index, physical activity, family history of colorectal cancer in a first degree relative, history of colon or rectal polyps, smoking status, multivitamin use, postmenopausal hormone therapy, saturated fat intake, red meat intake, and total energy intake.
The Women’s Health Study• A completed randomized trial evaluating low-
dose aspirin and vitamin E for the prevention of cardiovascular disease and cancer among 39,876 women aged 45 years.
• At baseline, participants provided information on lifestyle exposures, dietary intake, and medical history characteristics.
• During an average follow-up of 9 years, 212 women had a confirmed diagnosis of colorectal cancer (85 cases had primary tumor occurred in the proximal colon, 73 in the distal colon, and 40 cases in the rectum) .
Results– (1)
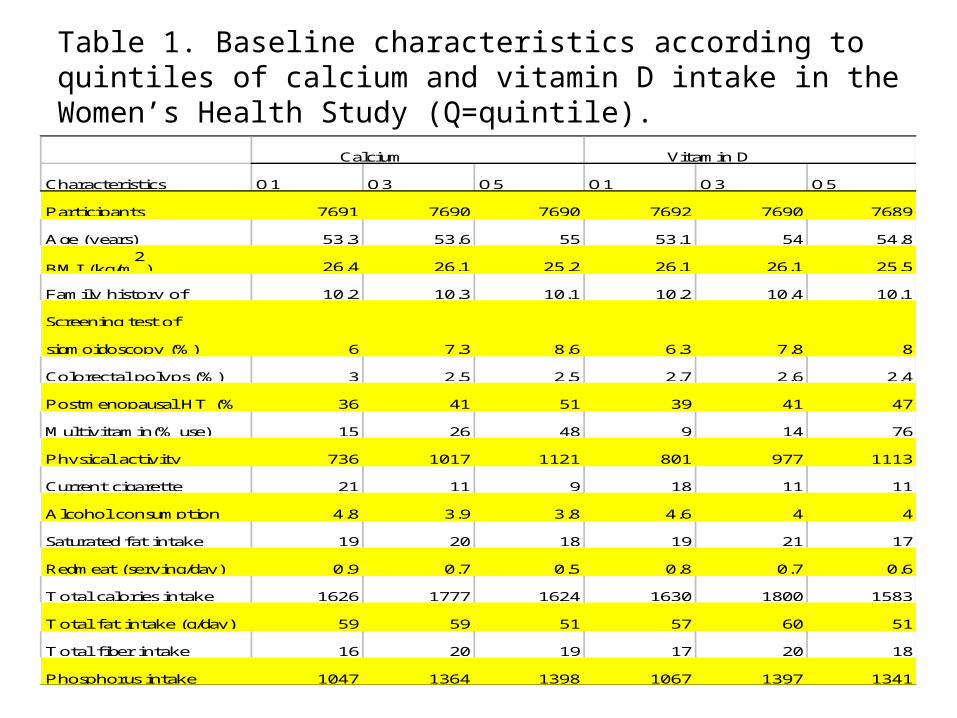
• Table 1 presents the baseline distributions of risk factors for colorectal cancer according to intakes of total calcium and vitamin D. Women who consumed greater amounts of calcium and vitamin D tended to be older and health conscious.
• Intake of total calcium intake was not associated with risk of colorectal cancer (Table 2).
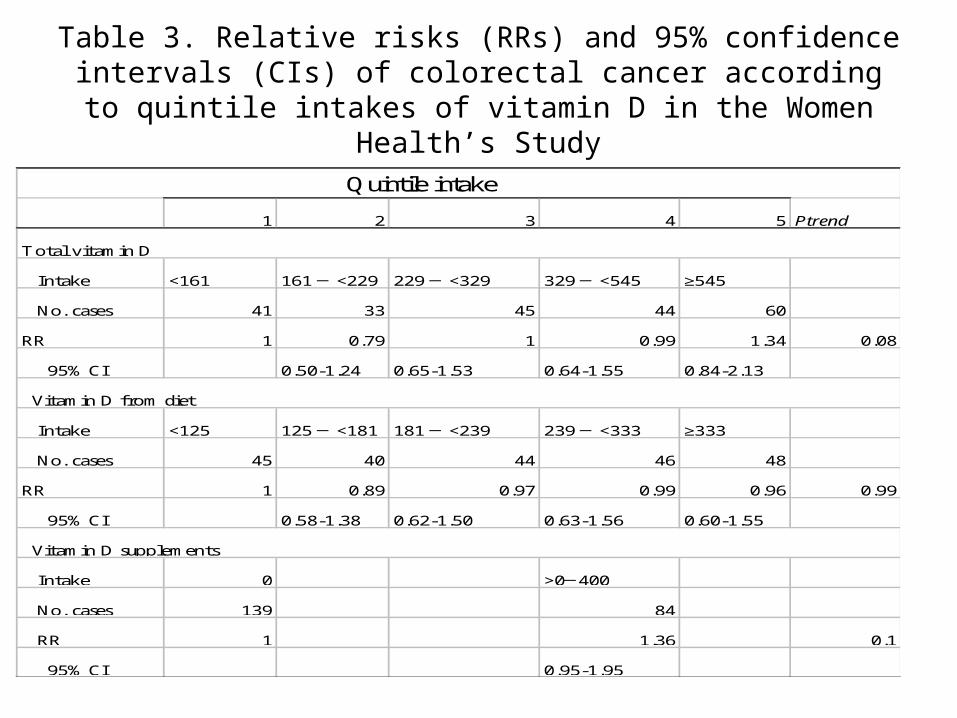
• Intake of total vitamin D intake was also not shown to be related to risk of colorectal cancer (Table 3).
Results – (2)• Major food sources of calcium and vitamin D were
also not associated with colorectal cancer risk (Tables 4a and 4b).
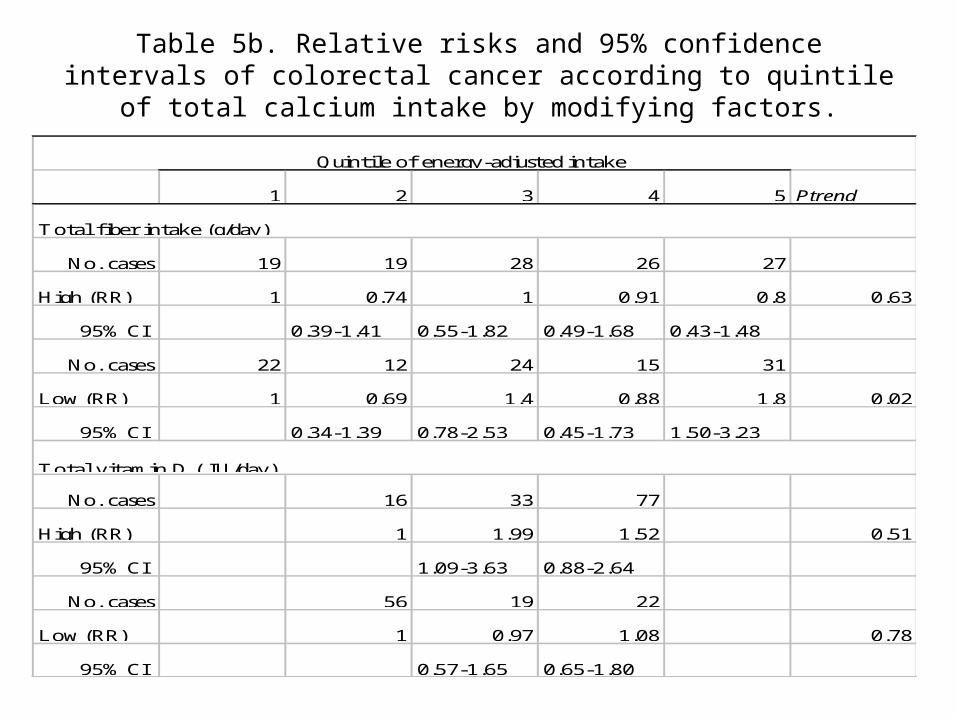
• Test for the interaction of calcium intake with intakes of total fat, phosphorus, vitamin D, and total fiber in relation to colorectal cancer was not statistically significant (p values for interaction >0.2). No significant associations could be observed in the stratified analyses according to these four nutrients (Tables 5a and 5b).
• The overall results were also not changed according to tumor location (colon, rectum) (Data not shown).
Table 1. Baseline characteristics according to quintiles of calcium and vitamin D intake in the Women’s Health Study (Q=quintile).
Characteristics Q1 Q3 Q5 Q1 Q3 Q5
Participants 7691 7690 7690 7692 7690 7689
Age (years) 53.3 53.6 55 53.1 54 54.8
BMI (kg/m2
) 26.4 26.1 25.2 26.1 26.1 25.5
Family history of 10.2 10.3 10.1 10.2 10.4 10.1
Screening test of
sigmoidoscopy (%) 6 7.3 8.6 6.3 7.8 8
Colorectal polyps (%) 3 2.5 2.5 2.7 2.6 2.4
Postmenopausal HT (% 36 41 51 39 41 47
Multivitamin(% use) 15 26 48 9 14 76
Physical activity 736 1017 1121 801 977 1113
Current cigarette 21 11 9 18 11 11
Alcohol consumption 4.8 3.9 3.8 4.6 4 4
Saturated fat intake 19 20 18 19 21 17
Redmeat (serving/day) 0.9 0.7 0.5 0.8 0.7 0.6
Total calories intake 1626 1777 1624 1630 1800 1583
Total fat intake (g/day) 59 59 51 57 60 51
Total fiber intake 16 20 19 17 20 18
Phosphorus intake 1047 1364 1398 1067 1397 1341
Calcium Vitamin D
Table 2. Relative risks (RRs) and 95% confidence intervals (CIs) of colorectal cancer according to quintile intakes of calcium in
Table 3. Relative risks (RRs) and 95% confidence intervals (CIs) of colorectal cancer according to quintile intakes of vitamin D in
the Women Health’s Study
1 2 3 4 5 Ptrend
Intake <161 161 ─ <229 229 ─ <329 329 ─ <545 ≥545
No. cases 41 33 45 44 60
RR 1 0.79 1 0.99 1.34 0.08
95% CI 0.50-1.24 0.65-1.53 0.64-1.55 0.84-2.13
Intake <125 125 ─ <181 181 ─ <239 239 ─ <333 ≥333
No. cases 45 40 44 46 48
RR 1 0.89 0.97 0.99 0.96 0.99
95% CI 0.58-1.38 0.62-1.50 0.63-1.56 0.60-1.55
Intake 0 >0─400
No. cases 139 84
RR 1 1.36 0.1
95% CI 0.95-1.95
Vitamin D from diet
Vitamin D supplements
Quintile intake
Total vitamin D
Table 4a. Relative risks and 95% confidence intervals (CIs) of colorectal cancer according to quintile intakes of specific dietary sources of calcium and vitamin D in the Women Health’s Study.
1 3 4 5 Ptrend
Intake <0.9 1.4 ─ <2.1 2.1 ─ <3.1 ≥3.1
No. cases 41 34 47 43
RR 1 0.79 1.04 0.89 0.42
95% CI 0.49-1.27 0.65-1.64 0.54-1.47
Intake 0.27 ─ < 0.50 ─ 0.78 ─ < ≥1.14
No. cases 53 33 51 43
RR 1.33 0.9 1.35 1.11 0.82
95% CI 0.89-2.00 0.57-1.44 0.88-2.07 0.69-1.77
Intake 0.1 ─ <0.4 0.4 ─ 1 >1
No. cases 58 76 47
RR 1.15 1.1 1.12 0.79
95% CI 0.77-1.71 0.75-1.61 0.72-1.74
58
1.35
Quintile intake
2
Dairy products (serving/day)
0.9 ─ <1.4
0.90-2.02)
Fermented milk products (serving/day)
<0.27
43
Milk
(serving/day)
<0.1
42
1
1
Table 4b. Relative risks and 95% confidence intervals (CIs) of colorectal cancer according to quintile intakes of specific dietary sources of calcium and vitamin D in the Women Health’s Study.
1 3 4 5 Ptrend
Intake 0.1 ─ <0.3 0.3 ─ <0.5 0.5 ─ <0.7 ≥0.7
No. cases 60 46 26 49
RR 1.48 1.32 1.07 1.38 0.53
95% CI 0.99-2.22 0.85-2.03 0.64-1.80 0.87-2.19
Intake <0.1 0.1 ─ <0.2 0.2 ─ <0.5 ≥0.5
No. cases 53 48 32 43
RR 1.3 0.96 0.89 1.23 0.66
95% CI 0.88-1.93 0.64-1.44 0.56-1.41 0.79-1.92
42
Cheese (serving/day)
Quintile intake
2
47
1
1
Yogurt (serving/day)
0
<0.1
Table 5a. Relative risks and 95% confidence intervals of colorectal cancer according to quintile of total calcium intake by modifying factors.
1 2 3 4 5 Ptrend
No. cases 21 15 23 19 26
High (RR) 1 0.63 1.05 0.79 1.61 0.04
95% CI 0.32-1.24 0.57-1.93 0.41-1.50 0.87-2.98
No. cases 20 16 29 22 32
Low 1 0.84 1.29 1.05 1 0.96
95% CI 0.44-1.64 0.72-2.32 0.55-1.97 0.55-1.81
No. cases 13 14 30 32 36
High (RR) 1 0.51 0.88 0.72 0.85 0.67
95% CI 0.24-1.09 0.45-1.72 0.37-1.41 0.42-1.73
No. cases 28 17 22 9 22
Low (RR) 1 0.8 1.18 0.73 1.12 0.69
95% CI 0.44-1.48 0.66-2.10 0.34-1.58 0.61-2.05
Quintile of energy-adjusted intake
Total fat intake (g/day)
Phosphorus intake (mg/day)
Table 5b. Relative risks and 95% confidence intervals of colorectal cancer according to quintile of total calcium intake by modifying factors.
1 2 3 4 5 Ptrend
No. cases 19 19 28 26 27
High (RR) 1 0.74 1 0.91 0.8 0.63
95% CI 0.39-1.41 0.55-1.82 0.49-1.68 0.43-1.48
No. cases 22 12 24 15 31
Low (RR) 1 0.69 1.4 0.88 1.8 0.02
95% CI 0.34-1.39 0.78-2.53 0.45-1.73 1.50-3.23
No. cases 16 33 77
High (RR) 1 1.99 1.52 0.51
95% CI 1.09-3.63 0.88-2.64
No. cases 56 19 22
Low (RR) 1 0.97 1.08 0.78
95% CI 0.57-1.65 0.65-1.80
Total vitamin D ( IU/day)
Quintile of energy-adjusted intake
Total fiber intake (g/day)
Limitations of our study
• Residual confounding.• Insufficient power for subgroup analysis.• Inadequate measures of vitamin D intake:
the synthesis of vitamin D in the skin from the sun is an important source, however, we had no information on sun exposure.
• Intakes of calcium and vitamin were only measured once at baseline.
Conclusion
• Our findings do not support a protective role of calcium and vitamin D intake against colorectal cancer incidence.
• However, given the evidence from both animal and in vitro studies, the benefits of these two nutrients cannot be ruled out.
References
• Cho et al (2004). J Natl Cancer Inst, 96:1015-22.• Bergsma-Kadijk et al (1996). Epidem, 7:590-7.• La Vecchia et al (1997). Int J Cancer, 73:525-30.• Garland C et al (1985). Lancet, 1:307-9.• McCullough ML et al (2003). Cancer Causes Control, 14:1-12.• Bonithon-Kopp et al (2000). Lancet, 3561300-6.• Baron et al (1999). N Engl J Med, 340:101-7.• Lin et al (2005). Am J Epi, 161:755-64.