252 Ilth FORUM IN MICROBIOLOGY badlli are coated by a multiple lamellar structure: freeze fracture analysis of infected mouse liver. In- feet. lrtlmun., 59~ 3895-3902. Shiratsuchi, H., Johnson, J.L. & Ellner, J.J, (1991), Bi- directional effects of cytoklnes on the growth of Myeobaeterium avium within human monoc~tes. J. immunoL, 146, 3165-3170. Sot, A., Simgue, S., Sixou, S., L.-Ghazal, F., Tocanne, J.-t. & Lan6:lle, O. (1990},Mycobacteria glycelipids as potential pathogenicity effectors: alteration of model and natural membranes. Biochemistry, 29, 8498-8502, Tassell, S.K., Pourshafie; M., Wright, E.L., Richmond, M.G. & Barrow, W.W. (1992), Modified lymphocyte response to mitogens induced by lipopeptide fragment derived from Mycobacter~um avium serovar-specific glycnpvptidolipids. Infect. Zmmun., 60, 706-711. Tereletsky, M.J. & Barrow, W,W. (19831, Postphagocytic detection of glycopeptidolipids associated with the su- perficial L~ layer of Mycobacterium intracelluiare. Infect. Immun., 41, 1312-1321. Tomioka. H , Sako, H. & Yamada, Y. 11990), Characteris- tics of immunosuppressive macrophages induced in spleen cells of Mycobacterium avium complex infec- tions in mice. J. Gen. Microbiol., 136, 963-973. Tsang, A.Y., Denner, J.C., Brennnn, P.J. & MeClatchy, J.K. (19921, Clinical and epidemiologic importance of typing of Mycobacterium avium complex isolates. J. Clio. Microbiol., 30, 479-484. Tsang, A.Y., Drupa, 1., Goldberg, M., Clatchy, J.K.M. & Brennma,P.J. (1983), Use of serology and thin-layer chromatography for the assembly of an authentlcat- ¢d collection of serovars within the Mycobacterium aviu~Mycobaeterium intraeeflulare-Mycob~cterium ~¢rofulaeeum complex..rntemat..L System. Bac- teriol., 33, 285.292. Tsuyuguchi, I., Kawasumi, H., Takashima, T., Tsuyu- guchi, T. & Kishimoto, S. (1990), Mycobacterium avium.M~obacterium intracellulare complex-induced suppression of T-cell proliferation in vitro by regula- tion of monocyte accessory cell activity. Infect. lm- mun., 58, 1369-1378. Woodbury, J.L. & Barrow, W.W. (1989), gadiolabelling of M.Vcobacteriumavium oligosaceharide determinant and use in maerophage studies. J. Gen. Mi~robiol., 135, i875-188,1. Wright, E.L. & Barrow, W.W. (1991), Identification o~" lipoproteins common to rough variants of the Mycobactcrium avium complex, abstr. U-47, p. 150. Abstr. 91st Gem Meet., American Society for Microbiology, Washington, DC. Wright, E.L & Barrow, W.W. (1992), Lipopeptides of potential importance in Myeobaeterium avium GPL biosynthesis, abstr. U-47, p. 173. Abstr. 92st Gem Meet., American Society for Microbiology, Washing- ton~ De. Wright, E.L., Pourshafie, M. & Barrow, W.W. (1992), Mycobacterium avium rough to smooth colony con- version resulting from growth in Twecn 80 without presence of type-specific glyeopeptidolipid antigens. FEMS Microbiol. Lett., 98, 209-216. Yeager, H., Ir. & Raleigh, J.W. (19731, Pulmonary dis- ease due to Mycobacterium inlraceflulare.Amer. Rev. Respir. Dis., 108, 547-552. DISCUSSION J.O. Falkinham, III: Drc:; resistance in Mycobaeterium avium an be due to genetic factors: namely mutation. For exam- ple, clarithromycin-, rifampin- and streptomycir: resistant isolates recovered during or after drug ther- apy and whose appearance correlates with relapse are mutants of the original drug-sensitive isolate, That has been shown by sequencing the mutations and by DNA fingerprinting (e.g., RAPD patterns). Drug- resistant mutants are quite likely because of the hill, numbers of M. avium which are found in AIDS pa- tients. Comments on Tt~oen Differences in serotype distribution of M. avium recovered from chickens, AIDS and non-AIDS hu- man patients would suggest that either the sources of M. avium infecting those groups of patients are different (e.g., water for AIDS patients and aerosols for non-AIDS pa.qents) or that the target populations differ in susceptibility Io different serotypes. Comments on Crawford The higher rate of recovery ofM. avium using the Bactee indicates that there exist viable but uneultiv- able M. avium when using other methods (e.g., agar media). We have seen acid-fast organisms in water samples, yet ,have been able to isolate viable, colony- forming individuals. There exist at least two hypotheses for the role of environmental strains in the emergence of drug- resistance and relapse in M. avium disease in AIDS patients. {1) Patients are initially infected with two M. avium isolates; one drug-sensitive, the ether drug- resistant; the ratio is not necessarily important, ex-
Transcript
252 I l t h F O R U M I N M I C R O B I O L O G Y
badlli are coated by a multiple lamellar structure: freeze fracture analysis of infected mouse liver. In- feet. lrtlmun., 59~ 3895-3902.
Shiratsuchi, H., Johnson, J.L. & Ellner, J.J, (1991), Bi- directional effects of cytoklnes on the growth of Myeobaeterium avium within human monoc~tes. J. immunoL, 146, 3165-3170.
Sot, A., Simgue, S., Sixou, S., L.-Ghazal, F., Tocanne, J.-t . & Lan6:lle, O. (1990}, Mycobacteria glycelipids as potential pathogenicity effectors: alteration of model and natural membranes. Biochemistry, 29, 8498-8502,
Tassell, S.K., Pourshafie; M., Wright, E.L., Richmond, M.G. & Barrow, W.W. (1992), Modified lymphocyte response to mitogens induced by lipopeptide fragment derived from Mycobacter~um avium serovar-specific glycnpvptidolipids. Infect. Zmmun., 60, 706-711.
Tereletsky, M.J. & Barrow, W,W. (19831, Postphagocytic detection of glycopeptidolipids associated with the su- perficial L~ layer of Mycobacterium intracelluiare. Infect. Immun., 41, 1312-1321.
Tomioka. H , Sako, H. & Yamada, Y. 11990), Characteris- tics of immunosuppressive macrophages induced in spleen cells of Mycobacterium avium complex infec- tions in mice. J. Gen. Microbiol., 136, 963-973.
Tsang, A.Y., Denner, J.C., Brennnn, P.J. & MeClatchy, J.K. (19921, Clinical and epidemiologic importance of typing of Mycobacterium avium complex isolates. J. Clio. Microbiol., 30, 479-484.
Tsang, A.Y., Drupa, 1., Goldberg, M., Clatchy, J.K.M. & Brennma, P.J. (1983), Use of serology and thin-layer chromatography for the assembly of an authentlcat-
¢d collection of serovars within the Mycobacterium aviu~Mycobaeterium intraeeflulare-Mycob~cterium ~¢rofulaeeum complex..rntemat..L System. Bac- teriol., 33, 285.292.
Tsuyuguchi, I., Kawasumi, H., Takashima, T., Tsuyu- guchi, T. & Kishimoto, S. (1990), Mycobacterium avium.M~obacterium intracellulare complex-induced suppression of T-cell proliferation in vitro by regula- tion of monocyte accessory cell activity. Infect. lm- mun., 58, 1369-1378.
Woodbury, J.L. & Barrow, W.W. (1989), gadiolabelling of M.Vcobacterium avium oligosaceharide determinant and use in maerophage studies. J. Gen. Mi~robiol., 135, i875-188,1.
Wright, E.L. & Barrow, W.W. (1991), Identification o~" lipoproteins common to rough variants of the Mycobactcrium avium complex, abstr. U-47, p. 150. Abstr. 91st Gem Meet., American Society for Microbiology, Washington, DC.
Wright, E.L & Barrow, W.W. (1992), Lipopeptides of potential importance in Myeobaeterium avium GPL biosynthesis, abstr. U-47, p. 173. Abstr. 92st Gem Meet., American Society for Microbiology, Washing- ton~ De.
Wright, E.L., Pourshafie, M. & Barrow, W.W. (1992), Mycobacterium avium rough to smooth colony con- version resulting from growth in Twecn 80 without presence of type-specific glyeopeptidolipid antigens. FEMS Microbiol. Lett., 98, 209-216.
Yeager, H., Ir. & Raleigh, J.W. (19731, Pulmonary dis- ease due to Mycobacterium inlraceflulare. Amer. Rev. Respir. Dis., 108, 547-552.
DISCUSSION
J.O. Falkinham, III:
Drc:; resistance in Mycobaeterium avium a n be due to genetic factors: namely mutation. For exam- ple, clarithromycin-, rifampin- and streptomycir: resistant isolates recovered during or after drug ther- apy and whose appearance correlates with relapse are mutants of the original drug-sensitive isolate, That has been shown by sequencing the mutations and by DNA fingerprinting (e.g., RAPD patterns). Drug- resistant mutants are quite likely because of the hill , numbers of M. avium which are found in AIDS pa- tients.
Comments on Tt~oen
Differences in serotype distribution of M. avium recovered from chickens, AIDS and non-AIDS hu- man patients would suggest that either the sources of M. avium infecting those groups of patients are
different (e.g., water for AIDS patients and aerosols for non-AIDS pa.qents) or that the target populations differ in susceptibility Io different serotypes.
Comments on Crawford
The higher rate of recovery ofM. avium using the Bactee indicates that there exist viable but uneultiv- able M. avium when using other methods (e.g., agar media). We have seen acid-fast organisms in water samples, yet ,have been able to isolate viable, colony- forming individuals.
There exist at least two hypotheses for the role of environmental strains in the emergence of drug- resistance and relapse in M. avium disease in AIDS patients.
{1) Patients are initially infected with two M. avium isolates; one drug-sensitive, the ether drug- resistant; the ratio is not necessarily important, ex-
L A B O R A T O R Y A N D CLINICAL A S P E C T S OF M, AVIUM EPIDEMIC 253
eept with reference to selection of an isolate for an- tibiotic susceptibility testing. Drug therapy selects for the drug-resistant, which then predominate~.
(2) Patients could be initially infected with one drug-sensitive isolate. During therapy, the patient is infected with a second drug-resistant isolate, whicia then predominates.
In both instances, a treatment relaps~ would coin- cide with isolation of a drug-resistant population. Further, the drug-resistant isolates might not be relat- ed to the drug-sensitive predecessor. Only in the case of mutation would the isolates demonstrate related- ness (e.g., RFLP, LRF or RAPD patterns).
Comments on Mang~tra and Reichman
Proof of the route of M. avium infection in AIDS patieuts will be dependent upon development of tech- niques to detect and enumerate M. avium in contami- nated specimens (Le., sputum and faeces). Thus, we ought to put some effort into developing be~ter methods for recovery or detection.
Comments on Suzuki and Inamine
Not only quantitative but qualitative differences i~n wall composition could have direct impact on an- timierobial susceptibility patterns.
Comm~ "ts on Gangadharam and Reddy
Studies of the role of M. avium plasmid-encoded genes in virulence require either construction (e.g., by transformation) or isolation (e.g., by curing) of isogenic plasmid-free and plasmid-carrying strains. There is a clear need to develop methods fo~ trans- mission or curing of M. avium plasmids.
There are a number of factors which are expect- ed to influence M. avium virulence, including medium composition, growth temperature and stage of growth. Differences in results between laborato- ries could involve those factors.
Comments on Shiratsuchi
Plasmid content has not been proven to influence AI. avium virulence. Unfortunately, after publication of work describing differences in virulence and eata- lase activity of a supposed isogenic plasmid-carrying and plasmid-free pair, it was shown that the plasmid- carrying strain was a representative of M. avium, while the supposed plasmid-free derivative was a representative of Mycobacterium intraeellulare.
J.T. Crawford:
The results described by Dr. Heifets for suscepti- bility to clarithromycin illustrate the fundamental difference in susceptibitity testing between M. tuber- culosis and M, aviurn. Critical drag concentrations can be used in testing M. tuberculosis because the iso- lates are relatively homogeneous in their susceptibil- ity. Isolates resistant to the various drugs at the critical concentrations represent mutants that have been selected upon treatment, either in the current patient or in a previous one. M. avium is apparently acquired from environmental sources, and thus the initial isolates from patients have never been exposed to the drugs (although trmtsmission from one im- munocompromised patient to another is theoretically possible). The wide variations in MIC values for drugs tested against M. avium strains reflect differ- ent levds of intrinsic resistance due a number of fac- tors, such as permcabil.~ty, rather than specific mutations that confer resistance onto an otherwise susceptible strain. This makes it difficult to divide the susceptible and resistant isolates and use MIC data directly to predict cIinical outcome. In the case of elarithromycin, all wild strains o f M. avium are susceptible to a low concentration. Mutants that are selected in response to therapy are resistant to much higher levels. Thus, it is possible to select a critical concentration (such as 32 ~tg/ml as Dr. Heifers sug- gests), divide the isolates imp susceptible and resis- tant, and predict the clinical outcome of use of the drug. As Dr. Heifets points out, this may reflect the fact that eIarithromycin is highly active and thus is capable of rapidly killing the initial susceptible popu- lation and selecting resistant mutants.
L. i-ie~fets :
How do you interpret the drug susceptibility te~t with M A C ?
1 agree with L.S. Young, L.E.M. Bermudez and C.B- Inderlied that the best way to find an answer to this question is by correlation between the test results and the patients' response to therapy. There were no such data until recently, but recently we have presented clear evidence on such correlation in regard to ctarithromycin (AAC, 1993; also see our review in this Forum). Almost all patients whose isolates were susceptible to 2.0 ~-g/ml or Iess have respond- ed favourahly to therapy, while at the time when their isolates showed the emergence of resistance to 128.0 ~.g/ml, they did not respond to therapy any- more &ld developed a relapse in bacteraemia. This corrdation took place when the isolates were tested 7,t pH 7.4 in broth. This pH is still good for cultiva- tion of M. aviurn, and the test is easy to perform.
254 l lth FORUM IN MICRO,$1OLOGY
Of course, it ha.s to he standardized, but we don ' t see that such a test is "technically problematic".
Another universally accepted option for valida.. tion of a laboratory test is the correlation with the pharmaeokinetie parameters (not just with Cm~, !). In this regard, S.L. Young and colleagues have mis- interpreted our suggestion for interpretation of MIC. We have not based our interpretation of results with M. avium only "on the comparative activity of agents against M. tuberculosis". Our suggestion was to first identify those isolates that are resistant even to Crux when tested in vitro. Unlike resistant isolates, iden- tification of those that can be called "susceptible" ~s much more complicated, and comparison with M. tuberculosis was only an additional criterion to separate those M. avium isolates that were most sus- ceptible.
What is the probability o f developing drug resistance to elarithromycin in A1DS patients with MAC ?
In our recent report (Antimicrob. Agents Chemother., 1993, 37, 2364-2370), we presented clear evidence that 100 % of the patients undergoing monotherapy had an emergence of clarithromycin- resistance, and associated with it, relapses of bacter- aemia, if they lived long enough to reach these events. The assumption is made in Dr. Dautzenberg's review that the clarithromycin resistance was developed in 33 to 50 % of patients. This is already high enough for seeking combined therapy, as is clearly stated in Dr. Dautzenberg's review, but we would like to stress that this observed frequency of the emerging drug resistance (33 to 50 a/0) is a result of the fact that a substantial proportion of patients died during the ob- servation, from various AIDS-related conditions, and did not reach the phase of drug resistance associat- ed with its relapses of baeteraemia.
Bacteriological response in AIDS patients with MAC dissemineted infection to monotherapy with clarithromycin
There is a statement in the review by B.T. Man- gura and L.B. Reichman that "monotherapy can he associated with the development of resistance or (un- derlined by us - - L.H.) an increase in MIC" . In our study (Atuimierob. Agents Chemother., 1993, 37, 2364-2370), we have shown tha t prolonged anonotherapy with clarithromycin inevitably leads to a relapse of bacteraemia, which was always associat- ed with a dramatic increase in MIC, from
2.0 Izg/ml before treatment to <~ 236.0 ~.g/ml at the time of relapse. I believe tt~at our report should have been taken into account, ~dcng with a not yet published study by Reisner.
How rapid is the rapid method?
Some of the procedures for identification of mycubacteria described in the review by J.T. Craw- ford are rapid techniques indeed, since teehnicafly the test can be done rapidly within a few days and even a few hours. The question is, however, whether a rapid technique is a rapid method, taking into ac- count turnarour~d time between the arrival of a raw specimen to the laboratory and the lab report on identification. This distinction is much more than just a semantic problem: there were many publications in which the authors of some new rapid techniques did not make such a distinction, implying that these new methods represented an answer to the problem of obtaining rapid results. No such critique can be found in Dr. Crawford's review.
HPLS. All published reports an the specificity and sensitivity of this method were based on analy- sis of cultures grown on solid media, which required three or even six weeks of cultivation to obtain a sufficient amount of the biomass. Obviously, this rapid technique is not a rapid method. Now there are unpublished reports that this test can be done with cultures grown in Bactec or Septi-Check liquid me- dia, implying that the results of identification can be reported sooner *.han within three weeks. Where are the facts that would support this suggestion? How long do these cultures have to be cultivated? How reliable will the HPLC method be with these broth cultures? Since these questions do not have clear an- swers, the HPLC rapid technique should not be clas- sified today as a rapid method.
DNA probe assay. The Accu-Prohe test is indeed a rapid technique, but unfortunately, the manufac- turer (Gen-Probe, Inc.) has developed this technique for cultures grown on solid media only, which re- quires at least tlu'ee weeks to report the results. Many laboratories are using the Bactec cultures for this test, but this technique has never been standardized by the manufacturer of the Accu-Probe, and therefore this test has not actually been developed into a rapid method !
Drug susceptibility testing. Not so long ago, the CDC issued a statement that drug susceptibility test- ing of MAC is not worthwhile. A few years before that, the CDC stated that testing all M. tuberculosis pretrcatment isolates was net necessary. Recently, the CDC officially changed the policy regarding M. tuberculosis: now the testing of these organisms is mandatory. Is Dr. Crawford's review evidence of a reversal in the CDC policy regarding drug suscepti- bility tesÂing of MAC as well ? If tiffs is not the case, then it is not dear why a rap.~d method (hiciferase test) will be more suitable than any other method. While rapid detection of drug resistance of M. tuber- culosis is essential, ~t~e timing of ~his test for patients with MAC is not at all critical. The currently stan-
L A B O R A T O R Y A N D CLINICAL A S P E C T S OF M. AVIUM EPIDEMIC 255
dardized Bactec method for MIC determination pro- vides results within 8 days, plus 7 days for primary isolation - - a totaI of 15 days, which is more than sufficient for this infection. What is the need for de- veloping luciferase test for MAC ?
B. Dautzenberg:
Disseminated M. avium infection is an increas- ing disease. In this Forum, experts expose sometimes different opinions about the same topic. While the Forum provides numerous new information, it raises more questions than it answers:
H o w does M. avium enter the organism ?
The portal of e~_try was mainly digestive for Man- gura but not determined for Faikinham. Ganga- dharam proposed the rectal route as a hypothetical important portal of entry. The knowlcdg ~ , of exact portal of entry (or of resurgence of colonization oc- curring during infancy) may influence the design of prophylactic trials to prevent colonization or inva- sion of the human organism by M. avium.
H o w does M. avium survive in the human bady ?
The ability of M. avium to stay for a long time in the cells remains mysterious, but new data arise from this Forum. In the host cell, M. avium produces a surface coat. The protection of bacilli from the envelope and cell coat is not simply passive protec- tion. M. avium, particularly if it was isolated from smooth dome colonies, was able to decrease secre- tion of mediators, such as I L 1, IL6 and TNF-e.lpha, used by the call to kill intraeellular microorganism. The fusion in the host cell of phagosomes contain- ing M. avium and lysosomes is inhibited by M. avium by an unknown mechanism. All the data concerning these mechanisms come from the lal~oratory. There is no clinical issue expected using specific immune therapy in the near future for the treatment of pa- tients infected by M. avium in AIDS patients.
There is no existing consensus on the optimal bac- teriologic method. The Baclec system is now used world-wide, but we need quantification after posi- tive culture on Baetee.
The sensitivity of PCR in routine practice was dis- cussed in this Forum. The promising re.,~ults from the experimeatal laboratory were not reproducible at this time at a routine level. Preparation of e!inica~ sam- pies for PCR, PCR procedure and interpretation of results have to bc improved.
We don' t know h~w t~ predict the bacteriologi- cal and clinical efficacy of a drug in human disease
from in vitro testing. A question raised in the Fo- rum is: does a standard procedure exist to determine in vitro susceptihility of M. avium ?
L. Heifers responds yes, and proposes interlabora- ~ory standard measures. Young says, "no, we do not have standard methods". The procedures recom- mended by Heifers would be acceptable after offi- cial international validation. The interpretation of in vitro r~ults needs bacteriological and clinical com- parison. Azithromycin, which has clear clinical bac- tericidal efficacy, is non-effective in vitro at the reported Cma x in humans.
We don't know how to treat disseminated M. avium disease. The 114. avium resistance to antituber- culous drugs is due to the inability of drugs to pene- trate into this microorganism. Antituberculous drugs could bt active inside the cells, but because ofeharuc- teristics of the cell membrane and envelope, drugs remain outside of this microorgemsm.
As no drugs except new macrolides (and vtham- butol) are active, the selection of resistant mutants occurs at a high rate with macrolide therapy. New drugs have to be evaluated. The assessment of new drugs is harder than 3 years ago. Since we now have active drugs, a monotherapy regimen is not ethical. New drugs have to be assessed in combination with elarRhromycin or azithromycin.
The multidrug trials published are often not properly designed. Often r.o conclusion could be drawn on the individual activity of drugs. At present, we don't know if rifabutin, quinolones, clofazimine or amikacin are useful in treating M. avium disease of AIDS patients.
We need b~ic and applied research on dissemi- nated M. crvium disease, which has become the most common opportunistic infection in AIDS patients.
C.B. IndedkM:
Dr. Falkinham's discussion ~f the epidemiolngy o f 2"14. avia'n complex (MAC) infections raises an in- triguing and perplexing aspect of tiffs problem, spe- cifically that the geographical distribution of MAC disease does not appear to reflect the natural biolo- gy of the microorganisms. For example, the incidence of MAC disease in large eiti*.s in the Northeastern USA is two-fold greater than the incidence in the Southeastern USA where the apparent incidex, ce of exposure to MAC is significantly higher. The increas- ing evidence that MAC is present in municipal water supplies, including and perhaps most notably hospi- tal water supplies, may provide a pa=tial answer to this paradox, tf the primary portal of MAC infec- tion is the gastrointestinal tract, and many believe this is true, it may be the presence of MAC in pota- ble water that is more important than the presence
256 l ill , F O R U M I N M I C R O B I O L O O Y
of MAC in natural waters. At the same time there may be a more subtle mechanism of exposure. Although MAC di.¢e.~e in HIV-infeeted persons ap- pears to be primarily due to M. evium versus M. in- tracellulare, as Dr. Falkinham points out, a significant number of patients with disseminated MAC disease are infected with polyclonal stains. S~.nce polyclomd disseminated infections are unusual and one would not expect that all MAC strains pos- sess attachment and penetration virulence factors, that polyclnnal infections occur suggests to me that, at least in certain patients, there may be a co-factor that facilitates the attachment and invasion of MAC; e.g. intestinal pathogens and perhaps in particular CMV.
Dr. Heifers must be lauded for the efforts he and his colleagues have made to verify the culture methods used to diagnose disseminated MAC disease and for their efforts to develop a rational basis for MAC susceptibility testing. However, I disagree with the proposal to base interpretive criteria for in vitro susceptibility testing on serum levels of drugs and the susceptibility of wild-type strains of M. tuberculo- s/s. Furthermore, I believe that the testing of mac- rotides (i.e,, clarithromycin and azithromycin) at a slightly alkaline pH ('/.2 to 7.4) is both unnecessary and inappropriate. More importantly, as we empha- sized in our own contribution to this Forum, the in- terpRtive criteria for in vitro susceptibility tests must ultimately relate to clinical efficacy and, perhaps with the exception of clarithromycin and azithromycin, there is scant information available to establish such correlates. Dr. Dautzenberg has made an important effort in this direction in his thoughtful review of various clinical trials of single agents and combina- tions. Yet, we still lack sufficient information to de- velop truly useful interpretive criteria. For example, Dr. Heifers' proposal to use a breakpoint of 4 ~g/ml for amikacin seems to me to be preposterous. Again, the primary basis for establishing interpretive criteria for MAC susceptibility testing should be the iden- tification of MIC that correlate with clinical effica- cy. The use of serum concentrations and comparative activity with other slm.cies of mycob~tcteda as criteria lacks a sound scientific or clinical basis and could be dangerously ndsleading.
l~egarding the pH effect on macrolide activity, 1 see no value in manipulating the in vitro system to make the maeroF.des appear more potent than may be the case in viva. The recent studies of Sturgill- Koszycki et al. (Science, 263, 6"18-681, 1994) show that, even if MAC prevem macrophage acidification, the intraccllular pH of MAC-infected macroI~hagcs drops to pH 6.0 to (i.5, while inhibition of the acidifi- cation mechanism prevents the more substantial drop to pH 5.0 to 5.5. Furthermore, there is little infor- mation about how efficiently MAC blocks acidifi- cation, i.e., are 100 % of infected macrophages
effected ? While the macrolides may be more potent at pH 7.2-%4, these compounds retain significant ac- tivity at the slightly acidic pH that is routinely used in MAC susceptibility testing. Thus, the imposition of pH as another variable in susceptibility testing seems unnecessary.
My own view, at this point in time, is that in vitro suseeptlbilhy testing o" MAC is inappropriate and largely a waste of time and money except to confirm macrolide resistance. In fact, I am not sure that con- firming macxolide resistance is much help in manag- ing patients, since it isn't clear to me that macrolide treatment should be withdrawn in the face of resistance, since we know very little about the effect of multiple drug regimens on such resistant strains. In addition, it isn't clear how effective multiple drug regimens are on the prevention of macrolide resistance. This question becomes even more vexing in light of the observations about the incidence of polyclonal MAC infections and the possibility of mixed susceptible and resistant strains.
Dr. Suzuki and Inamine's discussion of the genetic aspects of drug resistance in M. avium provid- ed valuable insights into the molecular nature :and mechanisms of drug resistance. Clearly we need a bet- ter understanding of ethambutol resistance given the important role of this agent both as a therapeutic agent and as a potentiating agent for other drugs, in addition, there is a clear need to determine whether the addition of ethambutol '.o a treatment regimen that includes a macrolide also prevents or decreases the incidence of macrolide resistance. This will be more apparent when there is a clear understanding of the mechanism of action of ethambutol a~d the correlating mechanism of resistance.
i disagree with some of the comments about rifampicin and MAC. While the in vitro activity of rifampicin against MAC is variable, I believe ~here is little evidence to support the use of this drug in the treatment of MAC disease. In a more specific response to Dr. Suzuki and Inamine's discussion, I believe thin the available evidence indicates that the vast majority of rifampicin resistance in MAC is in- herent resistance, probably due to impermeability, and that mutations in the rpoB gene are largely ir- relevant to rifampicin resistance, at least in the clinical context of MAC disease. This situation may rapidly change with the recent identification of rifamycin derivatives, the benzoxazinorifamycins, with potent in vitro activity against MAC. With these drugs, I would expect that rpoB mutations will be the primary cause of resistance; however, the clinical significance of benzoxazinorifamycin resistance wilt, of course, be dependent on the ther- apeutic utility of these compounds which has been demonstra'.ed in animal models, but not as yet in humans.
L A B O R A T O R Y A N D C L I N I C A L A S P E C T S OF M. AVIUM EPIDEMIC 257
P.R..I. Gansadharam:
Chemotherapy of Mycobacterium avium complex (MAC) disease has been dealt with in at least three chapters in this Forum by Mangura and Reichman, by Dantzenberg and by Young, Bermudez and In- defiled. While there is no argument with the broad recommendations made by the various authors, I would like to bdng out a few points which are either overlooked or are not adequately discussed.
First, amikacin which has been evaluated exten- sively by in vitro, macrophage, animal models and in clinical settings, has not been given adequate recog- nition, perhaps because it has not been tested ade- quately in clinical trials. Secondly, clofazimine has also been considered to be unimportant, even though many retrospective and prospective studies did show its importance, particularly in preventing bacterae- mia (Davidson et at., 1979). Thirdly, streptomycin has not been considered to the extent it deserves. In spite of our extensive investigations showing high ac- tivity of this drug, which were prompted by a sug- gestion by Dr. Wol~nsky, in in vitro, animal and macrophage models (Gangadharam et al., 1991 ; Duzgunes et aL, 1991; Ashtekar et al,, 1991), not much clinical application has been made, In all the studies, streptomycin showed activity comparable to amikacin, but it has many advantages over amika- t in in that it is less expensive and perhaps slightly less toxic and we know a lot more about this drug than amikacin because it is still used in chemotherapy of tuberculosis in short-course and intermittent chemotherapy regimens. As such, one can argue that streptomycin should be assessed as an important drug for the treatment of MAC disease. Fourthly, we would like to bring out the point about isoniazid. It is true that isoniazid does not have that high activity against MAC comparable to its activity against ,Mr, tuberculosis. Nevertheless, it is included ratber em- pirically in many of the drug regimens, including those recommended earlier by Lester and o)hers (1969) from the National Jewish Center. However, Heifers and Iseman (1990, 1991) have not on!y stressed the obvious point that isoniazid is not ac- tive against MAC in vitro, and therefore might not have no useful role in the treatment of MAC disease, but even argued against its use. Studies done in vitro and in ~ i m a i models by Reddy el al. (1994) have in- deed shown that isoniazid does have some slight syn- ergistic activity with clofazimine or streptomy.dn against MAC disease. This drug, which is the main- stay in the treatment of tuberculosis, and which has been shown to he the least toxic and most powerful against M. tuberculosis, can still be used until we have more powerful drugs. Certainly, it does not do any harm. Unlike rifampin, it does not have r.ny ca- pacity to induce tile metabolisin of other drugs. Fifth- ly, an important suggestion can be aired as a prelude or substitute for clinical trims. A simple new method,
originally published by Jindani et at. (1980) in Nairo- hi, and more recently stressed by Mitchison and col- leagues (Sirgel et d . , 1993) in London, involves the use of a simple qnantitative assessmem of sputum counts as a good substitute for clinical trials. Unfor- tunately, this simple methodology has not been at- tempted by anyone for establishing the ctinical effectiveness of any new drag against MAC. It is time that sltch an approach be explored for MAC disease with and without AIDS complications.
Finally, the importance of drug susceptibility pat- terne ~-, choosing the drug re$imen has been stressea by mi=ny workers. On the other hand, therapeutic drug monitoring using the achievable serum levels, especially in patients with HIV and AIDS complica- tions, even though this practice was introduced by the National Jewish group, has not been followed by anyone. One should discuss whether such a useful approach should be encouraged to be pursued by others.
Ashtekar. D.R., Duzgurcs. N. & Gangadharam, P.R.J: (1991), Activity of free and liposome encapsulated streptomycin against Mycobacterium evium complex (MAC) inside peritoneal macrophages. J. Antimicrob. Chemother., 28, 615-617.
Davidson, P.T., Goble, M., Fernandez, E. & Gangad- haram, P.R.J. (1979), CIofazimine {B663) for the treatment ofM. intracetlulore infection in man. Am. Rev. Respir. Dis., 119, 39'$ (abstract}.
Duzgunes, N., A~htekar, D.R., Hasher, D.L., Ghori, N., Debbs. RJ. , FTeund, D.S. & Gangadharam, P.R..J. (1991), Treatment of My,-obacterium intracellulare complex infection in beige mice with free and Iipo- some encapsulated strep.omycin. Role of liposome type and duration of treatment. J. lnfect, l~is., 164, 143-151.
Gangadharam, P.R.J., Ashtekar, D.R., Ghori, N., Gold- stein, J.A., Delos, R.5, & Duzgune~, N. 0991), Chemotherapeutic potential of free and liposom¢ en- capsulated streptomycin against experimemal Mycobacterium aviupr comp!ex infections in beige mice. J. Antimicrob. Chemother,, 2~, 425-435.
Heifers, L.B. & lseman, M.D. (1990}, Choice of an- dmicrobial agents for M. avium disease based on quandtative tests for drug susceptibility, N. Engl. J. Med., ]23, 419-420.
Heifers, L.B. & Iseman, M.D. (1991), Individualized ther- ap'¢ versus standard regimens in the treatment of Mycobacterium art;an infections. Am. Rev. Respir. D/s., 144, 1-2.
Jindani, A., Abet, V.R., Edwards, E.A. & Mitchison, D.A. (1980), The early bactericidal activity of drugs in pa- tients with pulmonary tuberculosis. Am. Rev. Respfr. Dis., t2~, 939-49.
Lester, W., Moulding, T., Fraser, R.I., McClatchy, J.K. & Fisher, D.A. (r969), Quintuple drug regimens m the treatment c,f Battey-type infections. Tran~ 28th Pulm. Dis. Res. ConL VA Armed Forces pp. 289-294.
Reddy, M.V., Srmivasan, S. & Gangadharam, P.R..L (1994), In vitro and in vi':o synergistic effect of isonia-
258 l lth FORUM IN MICROBIOLOGY
zid with streptomycin and clofazimine against Mycobacterium avium complex (MAC). Tuber. Lung D/s., 75 tin press).
Sirgel, F.A., Botha, FA.H., Parkin, D.P., Van De Wal, B.W., Donald, P.R., Clark, P,K. & Mitchlson, D,A. (1993), The early bactericidal activity of fifabntin in patients with pulmonary tuberculosis measured by sputum viable counts: a ~ew method of drug assess- ment. J. Antimicrob. Chemother., 32, 86%875.
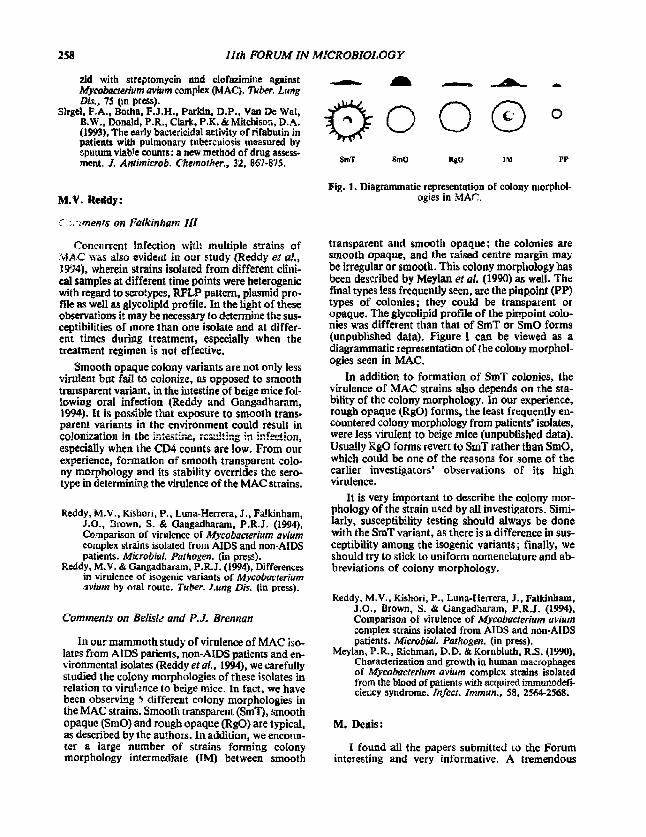
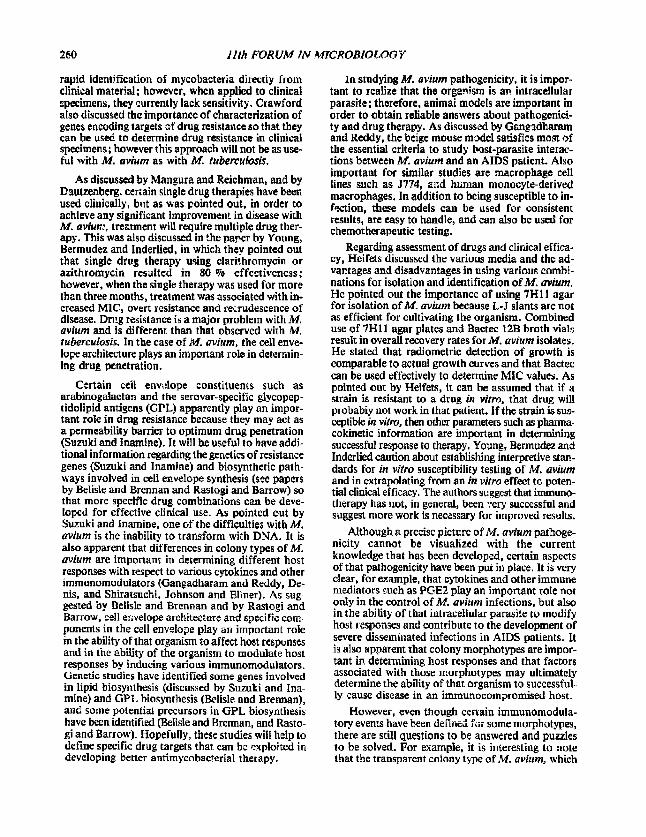
M.V. Reddy: Fig. 1. Diagrammatic representation of colony morphol-
ogies in MAC.
er ~I' ~ m e n ~ On E a l k i n h a m I I1
Concurrent infection with multiple s*.rains of MAC was also evident in our study (Rcddy eta! . , 1994), wherein strains isolated from different cihfi- col samples at different time points were heterogenic with regard to serotypes, RFLP pattern, plasmid pro- file as well as glycolipid profile. In the light of these observations it may be necessary to determine the sus- ceptibilities of more than one isolate and at differ- ent times during treatment, especially when the treatment regimen is not effective.
Smooth opaque colony variants are not only less virulent but fail to colonize, as opposed to smooth transparent variant, in the intestine of beige mice fol- lowing oral infection (Reddy and Gangadharam, 1994). tt is possible that exposure to smooth trans- parent variants in the environment could result in colonization in the intestlnz, rc~ultir, g in inf~tion, especially when the CD4 counts arc low. From our experience, formation of smooth transparent colo- ny morphology and its stability overrides the sero- type in determining the virulence of the MAC strains.
Reddy, M.V.. Kishori, P., Luna-He~rera, J., Fa!kinham, J.O., ~rown, S. & Gangadharam, P.R.J. (1994), Comparison of virulence of Mycobacwrium avium complex strains isolated from AIDS and non-AIDS patients. Mkrobial. Pathogen. (in prv~),
Reddy, M.V. & Ctaagadhatam, P.R.J. (1994), Differences in virulence of isogonic variants of Mycobacterium ~vium by oral route. Tuber. Lung Dis. (in press).
Comments on Belisle und P.J. Brennan
In our mammoth study of virulence of MAC iso- lates from AIDS patients, non-AIDS patients and en- vironmental isolates (Reddy et al., 1994), we carefully studied the colony morphologies of these isolates in relation to virulmce to beige mice. In fact, we have been observing 5 different colony morphologies in the MAC strains. Smooth transparent (SmT), smooth opaque (SmO) and rough opaque (R$O) are typical, as described by the authors. In addition, we encoun- ter a large number of strains forming colony morphology intermediate (IM) between smooth
transparent and smooth opaque; the colonies are smooth opaque, and the raised centre margin may be irregular or smooth. This colony morpilology has been described by Meylan et al. (1990) as well. The final types less frequently seen, are the pinpoint (PP) types of colonies; they could be transparent or opaque. The glycolipid profile of the pinpoint colo- nies was different than that of SmT or SmO forms (unpublished data). Figure i can be viewed as a diagrammatic representation of the colony morphol- ogies seen in MAC.
In addition to formation of SmT colonies, the virulence of MAC strains also depends on the sta- bility of the colony morphology. In our experience, rough opaque (RgO) forms, the least frequently en- countered colony morphology from patients' isolates, were less virulent to beige mice (unpublished data). Usually g g o forms revert to SmT rather than SmO, which cotdd be one of the reasons for some of the earlier investigators' observations of its high virtflence.
It is very important to describe the colony mor- phology of the strain used by all investigators. Simi- larly, susceptibility testing should always be done with the SmT variant, as there is a difference in sus- ceptibility among the isogonic variants; finally, we should try to stick to uniform nomenclature and ab- breviations of colony morphology.
Reddy, M.V., Kishori, P., Luna-Hetrera, J., Falkinham, J.O., Brown, S. & Gangadharam, P.R.J. (1994), Compatiso~i of virulence of Mycobacterium avium complex strains isolated from AIDS and non-AIDS patients. Microbial. Pathogen. (in press).
Meylan, P.R., Richman, D.D. & Korabluth. R.S. (1990), Characterization and growth in human macrophagcs of Mycobacterium avium complex strains isolated from the blood of patients with acquired immunodefi- cle~:cy syndrome. Infect. Immun., 58, 2564-2568.
M. Denis:
I found all the papers submitted to the Forum interesting and very informative. A tremendous
L A B O R A T O R Y A N ~ CLINICAL ASPECT~ ~/:" M. AVIUM EPIDEMIC 259
amount of effort is now being directed towards vn- derstanding the immunopathogenesis of M. ~' ium infection in ~he cor, tex!. of AIDS, as well as toward new chemotherapet~*i¢ regimens. Many groups ~re examining such diverse areas as microbc-viru~ inter- actions, impact of viral proteins on macrophage func- tion, etc. Also, AIDS is characterized by a dysregulated cytokine profile, with a decrease in im- munoregulatory lymphokines (i.e. IL2, IFN'0, and an increase in the release of proinflammatory cytokines, especially at mucosal surfaces (i.e. alveo- lar maerophages). These lymphokine dysfunctions are likely to be important in determining the exqui- site smceptibility of AIDS subjects to opgortunistic microbial infections. We and others have recently described the binding of cytokiaes to mycobacteria (Denis and Grogs, 1991). The impfication of this phenomenon, particularly in vivo, is still unclear and deserves further study, h is clear that M. avium in- fections occur in AIDS patients after the HI¥1 vi- rus has ravaged the immune system; however, g . avium and its component parts probably hasten im- munosuppression. Much effort is now focused on dissecting the pathological potential of the different cell envelope constituents o f M avium. This area of study may well provide important insight into the host-parasite relationship, and suggest new avenues of chemotherapeutic intervention.
Denis, M. & Oregg, E.O. (199I), Cytok~nes as growth fac- tors for microbes/parasites; a review. Res. Alicro- biol., 142, 979.983.
H. Shirat,;uehi, J.L. Johnson and J.J. Ellner:
In this Forum, several papers have b~en present- ed describing the importance of colonial morpholo- gy as a virulence factor for M. avium growth in human mononuelear phagocytes. Drug resistance and the severe, usually irreversible, immunosuppressed state of most patients with disseminated M. avium infection further enhance the pathogenicity of this organism and complicate treatment.
Differences in colonial morphology reflect changes in the expression of key mycobacterial cell wall constituents. Quantitative and qualitative differ- ences in the glycopepfidofipid (GPL) expression have been described in studies of zl,l. avium strains with differing colonial morphology. Modulation of mononuclear phagocyte effector functions by these mycobacterial cell wall components may contribute significantly to M. avium pathogenicity.
Further work has been presented describing various effects of cytokines on mononuelear phago- cyte effector functions against M. avium. Data from these experiments performed utilising in vitro muno- cyte/macrophage infection models are variable and
sometimes confusing; many of these differences are probably attributable t~ differences in experimental conditions and strain-to-strain differences in M. avium strains used. The use of animal model~ such as ;he beige mouse may decrease some of this varia- bility and represents a significant advance in impor- tant areas such as in vivo drug susceptibility testing.
N. Rastngi and W. Barrow:
With regard to ¢pidemio!ogy, it i~ still not appar- ent whether AIDS patients are previously hffccted with M. avium or whether they become infected with M. ovium following infection with H|V. The discus- sion by Falkenheim points out that if infection with M. avium is due to reactivation of organisms ac- quired previously, then infection would be the highest in the southeastern United States where the organism is most commonly isolated; however, isolation rates arc higher in other regions that have a low incidence ofM. avium in the environment. On the other hand, Faikenheim points out that if one assumes that M. avium infection results from a recent acquisition of the organism, that is also difficult to r~oncile be- cause the highest numbers of M. avium are found in the southeastern United States environment, an area that has the lowest prevalence of M. avium in- fections in AIDS patients. However, it is important to point out Thoen's discussion concerning chang- ing incidence rates for M. avium in animals. For e~.ample, there has been a marked decrease in the to- tal percentage of M. cvium serovars I and 2 in swine from 1983-1992. There has also been a marked in- crease in the isolation of 3/I. avium serovars 4 and 8 in swine, probably as the result of increased herd sizes. These facts may also suggest that previous in- cidence rates for humans and the environment may have changed dvripg the last 10-12 years, and that maybe some of the previous numbers do not reflect an accurate assessment of human exposure to M. avium during that period.
With regard to laboratory issues, Cgawford reported on two rapid methods that are important in culturing M. avium, the r~diometric tqJactec) method and the biphasic culture system "'Septi-Chek AFB" fBecton Dickinson). These are important tools in improved :ulturing of M. a'¢ium. Once organisms are isolated, they can be identified by analysis of mycolic acid.3 using HPLC, a rapid, reliable and use- ful technique that is now computerized for easier and more rapid analysis of data. HPLC analysis of mycotic acid is useful for identifying all mycobac- terial species, not just. M. avium and M. tuberculo- sis. Use of DNA probe methods can also be used once the organism has been cultured, and are rao,-e im- proved because of a chemilm~inescent label which dele:es the necessity for radioactive waste. Nucleic amplification methods offer an important tool for
260 l l t h F O R U M I N MICROBIOLOGY
rapid identification of mycobacteria directly r u m clinical material; however, when applied to clinical ~pecimens, they currently lack sensitivity, Crawford also discussed the importance of characterization of genes encoding targets of drug resistmlce so that they can he use~ to determine drug resistance in clinical specimens; however this approach will not be as use- ful with M. avium as with M. tuberculosis.
As discussed by Mangura and Reiehman, and by Dautzenberg, certain single drug therapies have been used clinically, bt:t as was pointed out, in order to achieve any significant improvement in disease with M. aviu#:, treatment will require multiple drug ther- apy. This was also discussed in the paper by Young, Bermudez and lnderlied, in which they pointed out that single drug therapy using elarP.hromyein or azithromycin resulted in 80 % effectiveness; however, when the single therapy was used for more than three months, treatment was associated with in- creased MIC, overt resistance and recrudescence of disease. Dn,_g resistance is a major problem with M. aviurn and is different than that observed with M. tuberculosis. In the ease of M. avium, the cell enve- lope architecture plays an important role in determin- ing drag penetration.
Certain ceil envelope constituents such as arabinogalactan and the serovar-specific glycopep- tidolipid antigens (GPL) apparently play an impor- tant role in drug resistance because they may act as a permeability barrier to optimum drug penetration (Suzuki and Inamine). It wall be useful to have addi- tional information regarding the genetics of resistance genes (Suzuki and InamJne) and biosyntlaetic path- ways involved in cell envelope synthesis (see papers by Belisle and Brennan and gastogi and Barrow) so that more specific drug combinations can be deve- loped for effective clinical use. As pointed out by Suzuki and lnamine, one of the difficulties with 34. avium is the inability to transform with DNA. It is also apparent that differences in colony types of M. avium are important in determining different host responses with respect to various cytokines and other immunomodulators (Gangadharam and Reddy, De- nis, and Shiratsuchi, Johnson and Eliner). As sug- gested by Belisle and Brennan and by Rastogi and Barrow, cell er~velope architecture and specific com- ponents in the cell envelope play an important role in the ability of that organism to affect host responses and in the ability of the organism to modulate host responses by inducing various immunomodulators. Genetic studies have identified some genes involved in lipid biosynthesis (discussed by Suzuki and Ina- mine) and GPL biosynthesis (Belisle and Brennan), and some potential precursors in GPL biosynthesis have been identified (Belisle and Brennan, and Rasto- gi and Barrow). Hopefully, these studies will help to define specific drug targets that can be exploited in developing better antimycobaeterial therapy.
lu studying M. avium pathogenicity, it is impor- tant to realize that the organism is an intrace]lular parasite; therefore, animal models are important in order to obtain reliable answers about pathogenici- ty and drug therapy. As discussed by Gangadharam and Reddy, the beige mouse model satisfies most of the essential criteria to study host-parasite interac- tions between M. avium and an AIDS patient. Also important for similar studies are macrophage cell lines such as J774, and human monucyte-derived macrophages. In addition to being susceptible to in- fection, theae models can be used for consistent results, are easy to handle, and can also he used for chemotherapeutic testing.
Regarding assessment of drugs and clirdcal effica- cy, Heifers discussed the various media and the ad- vantages and disadvantages in using various combi- nations for isolation and identification of M. aviumo He pointed out the importance of using 7HI1 agar for isolation ofM. avium because L-J slants are not as efficient for cultivating the organism. Combined use of 7HII agar plates and Bootee 12B broth vials result in overall recovery rates for M. aviurn isolates. He stated that radiometric detection of growth is comparable to actual growth curves and that Bactec can be used eft~tively to determine MIC values. As pointed out by Heifets, it can be assumed that if a strain is resistant to a drug in vitro, that drug will probably not work in that patient. If the strain is sus- ceptible in vitro, then other parameters such as pharma- cokinetic information are important in determining successful response to therapy, Young, Bormudoz and Inderlied caution about eaablishing interpretive stan- dards for in vitro susceptibility testing of M. avium and in extrapolating from an in vitro effect to poten- tial clinical efficacy. The authors suggest that immune- therapy has not, in general, been very successful and suggest more work is necessary for improved results.
Although ~ precise picture of M. avium pathoge- nicity cannot be visualized with the current knowledge that has been developed, certain aspects of that pathogenicity have been put in place. It is very dear, for example, that cytokines and other immune mediators .~.uch as PGE2 play an important role not only in the control of M. avium infections, but also in the ability of that intraceliular parasite to modify host responses and contribute to the development of severe disseminated infections in AIDS patients, It As also apparent that colony morphotypes are impor- tant in determining host responses and that factors associated with those morphotypes may ultimately determine the ability of that organism to sueces~ful~ ly cause disease in an immunocompromised host.
However, even though certain immuuomodula- tory events have been defined f,3r some morphotypes, there are still questions to be answered and puzzles to be solved. For example, it is interesting to note that the transparent colony type ofM. aviurn, which
L A B O R A T O R Y A N D CLINICAL ASPECTS OF M. AVIUM EPIDEMIC 261
is considered to be the more "'virulent" form, is less able to induce certain c~okines such as TNFc~ ~han the "less virulent" dome-opaque colony type {dis- cussed by Shiratsuchi, Johnson and EIIneO, This is important in explaining virulence for that morpho- type, because increased levels of TNFet would he detrimental to M. avium survival. On the other hand, it has also been demonstrated that HIV replication in vitro is increased by cytokines such as TNFct. Why then, is the opaque colony type, which induce~ great- er levels of TNF~, not the more virulent form in the context of HIV infection, since it can induce greater levels of TNF~, which would theoretically cause in- creased HIV replication?
It will be important for investigators to fully de- fine the specific cytokines and time sequence that takes place with regard to the apparently complex cy- cle of immunomodnlation in an M. avium infection. Northern blot analysis, such those discussed by Shiratsuchi, Johnson and EHner, are important methods for demonstratipg the complex changes that are taking place at the molecular level. It will also be important for investigators to identify specific M. avium components that contril~ute to pathogenicity and understand the molecular basis for each of these components (see paper by Suzuki and Inarnine, and also paper by Belisle and Brennan), as well as the in- teractions that take place between M. avium and hos~ macrophages (see paper by Gangadharam and Red- dy, and glso paper by Denis). Another interesting point about the host/parasite interactions was marie by Denis, Apparent~ly, AIDS p~tients have several
lipid metabolism dysfunctions, including an increased serum level of trigtyceridcs. As suggested by Denis, these might serve as growth-enhancing lipide. This may be an interesting area of study because it is known that the composition of cell envelope llpids is modified by changing the various hydrocarbon sources when cultivating mycobaeteria, Perhaps this may help to explain som~ of the :¢lectivity for cer- tain colony types from AIDS patients that revert to a different colony type when cultured on laboratory media. In addition, this may offer some answers regarding the development of drug resistance tlmt ap- pears to be greater in vivo than in vitro.
Many questions will have to be answered before a complete picture of M. avium pathogenicity can be developed. One thing is apparent. The events as- sociated ~ith M. avium pathogenicity are very com- plex and it will take the work of many investigators to conclusively determine the detailed cascade of events occurring in Mo avium infections. It will be important for investigators to continue to study specific events taking place in M. avium infections and also specific components associated with the or- ganism itself. We feel that this Forum has succeed- ed in its goal of formulating an updated piaure of the M. avium complex and its importance as a major clinical problem in the management of AIDS. We thank the participants far their willingness to con- tribute to thi~ endeavor and hope that this Forum will be a useful tool for other interested scientists to bet- ter understand this clinically important opportunis- tic pathogen.
Key-words: My¢obaeterium ~tvium, Drug susceptibility, Immune response, Pathogemcity; Epid~-m!iolog~J, Forum.