58
ACC-New York, Dec. 12, 2015 No Disclosures Diseases of The Aorta 2016 Understanding & Approach TAA, TAD, AAA, AAR

ACC-New York, Dec. 12, 2015 No Disclosures
Diseases of The Aorta 2016Understanding & Approach
TAA, TAD, AAA, AAR

Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA,AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Th.Ao.An. –TAD: Th.Ao.Dis. – AAA: Abd.Ao.An – AAR: Abd,Ao.Rupt.

1). Classification of Thoracic Aortic Dissection(6 people per 100.000 per year)
VS Ramanath et. al. Mayo Clin Proc. 2009;84:465.CA Nienaber et. al. Circulation 2003;108:628.
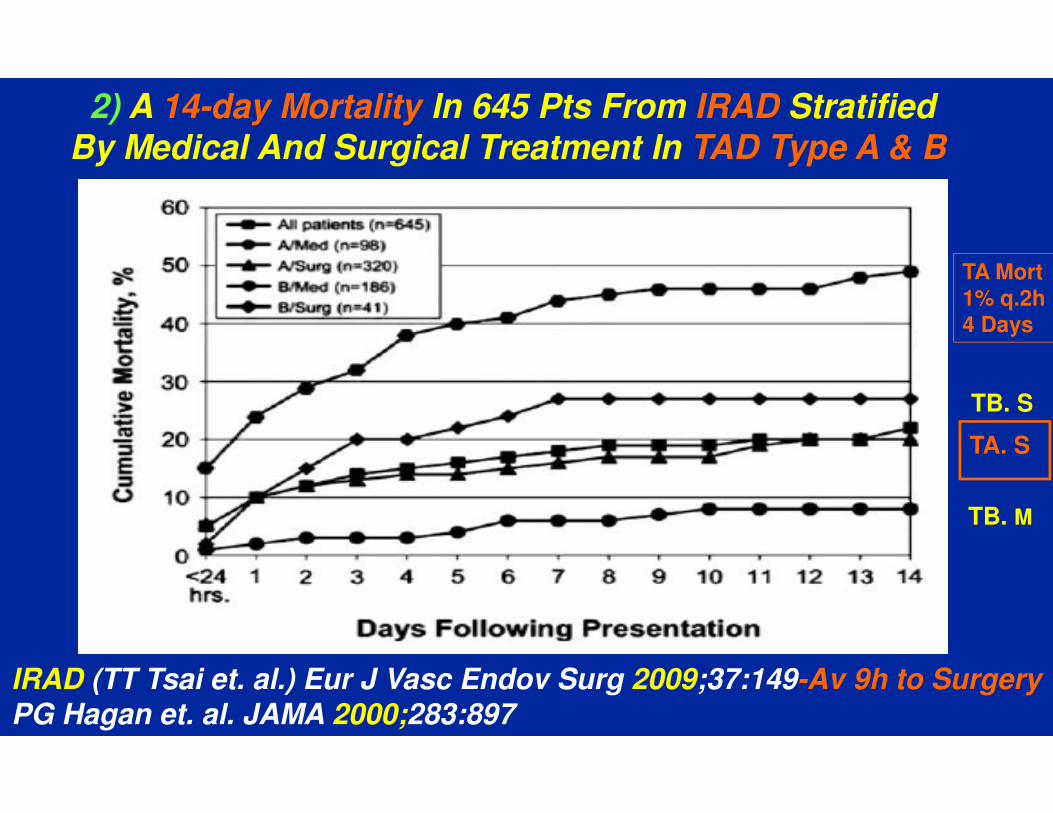
2) A 14-day Mortality In 645 Pts From IRAD Stratified
By Medical And Surgical Treatment In TAD Type A & B
IRAD (TT Tsai et. al.) Eur J Vasc Endov Surg 2009;37:149-Av 9h to Surgery
PG Hagan et. al. JAMA 2000;283:897
TA Mort1% q.2h4 Days
TA. S
TB. S
TB. M

A Evangelista et. al. Nat. Rev. Cardiol. 2013;10:477 – End Doing Both
3) Imaging Modalities In The Diagnosis Of AAS

4D Phase Contrast MRI From A Patient With Aortic Dissection
RE Clough et. al. Nat. Rev. Cardiol. 2015;12:103

4) Pathophysiological Features of Marfan’s & Bicuspid Aortopathy
S Verma et. al. N Engl J Med 2014;370:1920

Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA,AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Th.Ao.An. –TAD: Th.Ao.Dis. – AAA: Abd.Ao.An – AAR: Abd,Ao.Rupt.
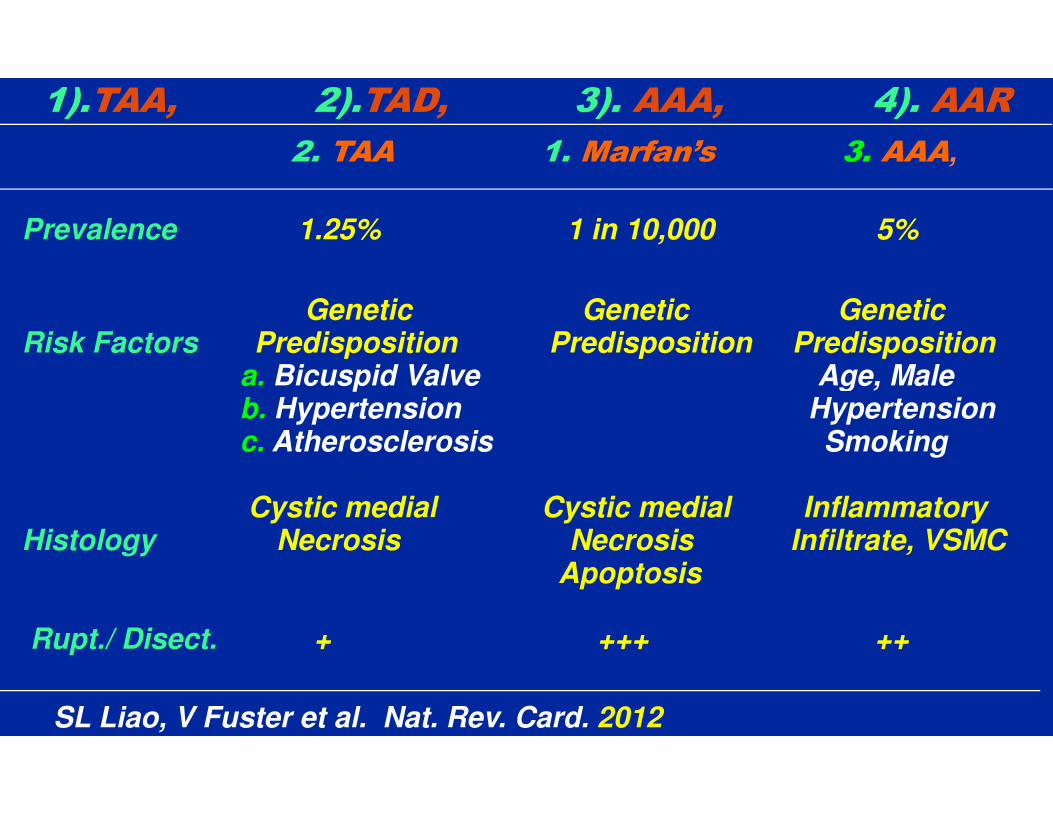
1).TAA, 2).TAD, 3). AAA, 4). AAR
2. TAA 1. Marfan’s 3. AAA,
Prevalence 1.25% 1 in 10,000 5%
Genetic Genetic GeneticRisk Factors Predisposition Predisposition Predisposition
a. Bicuspid Valve Age, Male b. Hypertension Hypertensionc. Atherosclerosis Smoking
Cystic medial Cystic medial InflammatoryHistology Necrosis Necrosis Infiltrate, VSMC
Apoptosis
Rupt./ Disect. + +++ ++
SL Liao, V Fuster et al. Nat. Rev. Card. 2012

Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA, AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Thor. Aort. Aneur. –TAD: Thor. Aort. Dissect. – AAA: Abd. Aort. Aneur.

Junquiera LC, Carneiro J:Basic Histology Text and Atlas, 11th ed. McGraw-Hill Access Medicine. 2005.
STRUCTURE NORMAL AORTA FUNCTION
ELASTINFibrillin TGF-bMMPs
SMC
COLLAGEN
VASAVASORUM
DISTENSION
ACTIVITY> Mucoid
RESISTANCE
NUTRITION

1). Mutant Fibrillin 1 in the Regulation of Aorta Homeostasis
I El-Hamamsy et. al. Nat Rev Cardiol. 2009;6:771.
?

Junquiera LC, Carneiro J:Basic Histology Text and Atlas, 11th ed. McGraw-Hill Access Medicine. 2005.
STRUCTURE 1) AORTIC ANEURYSM - MFS DYSFUNCTION
< Fibrillin > TGF> MMPs< ELASTIN
>SMC< SMC
< COLLAGEN
< VASAVASORUM
< DISTENSION
> ACTIVITY>Collagen> Mucoid
< RESISTANCE
< NUTRITION

1,2a) TAA/TAD – MARFAN’S / BIC. – 2bc) HYPERT. / ATHER
FBN1Mutation
↓ Fibrillin
↑TGF-β
↑MMP↓ TIMP
Rupture
↓ Collagen
AneurysmFormation
CMD
↑Stiffness
↓ Elastin↑ Collagen
DegenerativeDiseases
VSMC
↑ Proteases
↑ dp/dt↑ Aortic diameter↑ BP
SL Liao, V Fuster et al. Nat. Rev. Cardiol. 2012
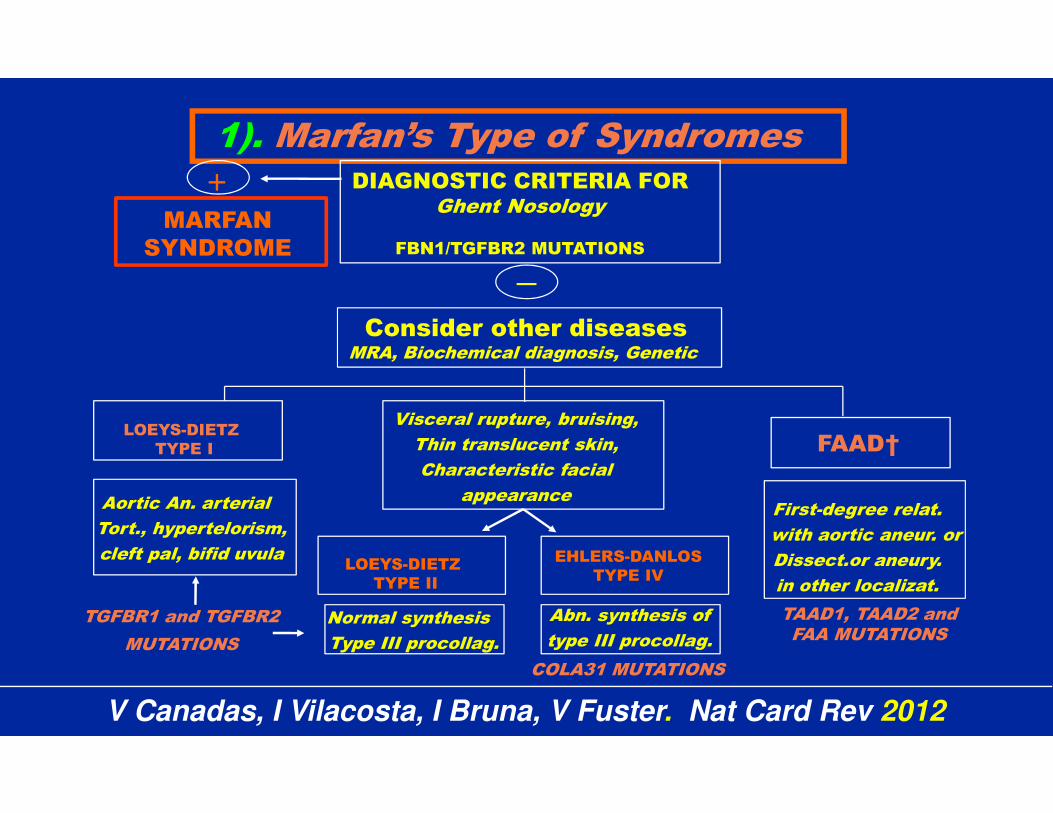
1). Marfan’s Type of SyndromesDIAGNOSTIC CRITERIA FOR
Ghent Nosology
FBN1/TGFBR2 MUTATIONS
LOEYS-DIETZ
TYPE I
MARFAN
SYNDROME
Visceral rupture, bruising,
Thin translucent skin,
Characteristic facial
appearance
Consider other diseasesMRA, Biochemical diagnosis, Genetic
LOEYS-DIETZ
TYPE II
EHLERS-DANLOS
TYPE IV
FAAD†
First-degree relat.
with aortic aneur. or
Dissect.or aneury.
in other localizat.
Aortic An. arterial
Tort., hypertelorism,
cleft pal, bifid uvula
Normal synthesis
Type III procollag.
Abn. synthesis of
type III procollag.
TAAD1, TAAD2 andFAA MUTATIONS
TGFBR1 and TGFBR2
MUTATIONS
COLA31 MUTATIONS
+
V Canadas, I Vilacosta, I Bruna, V Fuster. Nat Card Rev 2012

2a) Bicuspid Aortic Valve - Morphology Features That Influence the Pattern of Aortopathy
S Verma et. al. N Engl J Med 2014;370:1920 – Types 1,2,3

R Mahadevia et. al. Circulation. 2014;129:673
Bicuspid Aortic Cusp Fusion Alters Aortic3D flow Patterns, Wall Shear Stress & Aortopathy

1Group -2abc) Pathways In TAA–Fibrillin?,TGF-b
E Gillis et. al. Circ Res. 2013;113:327
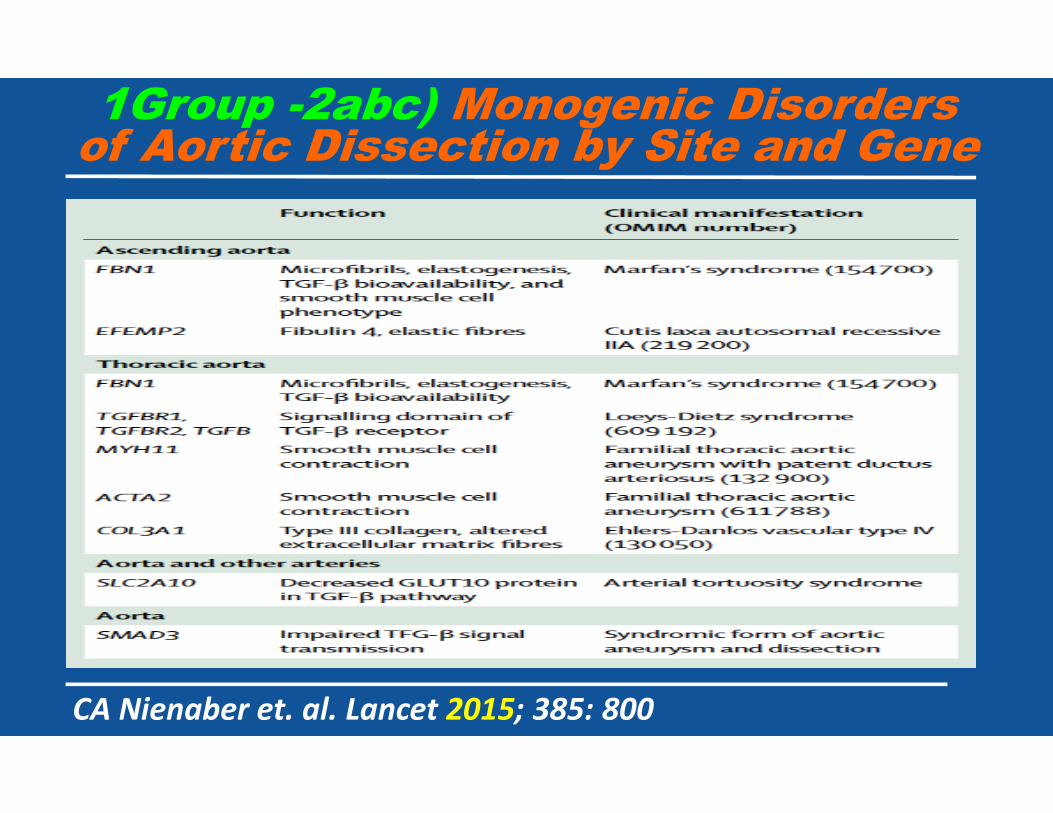
CA Nienaber et. al. Lancet 2015; 385: 800
1Group -2abc) Monogenic Disorders of Aortic Dissection by Site and Gene
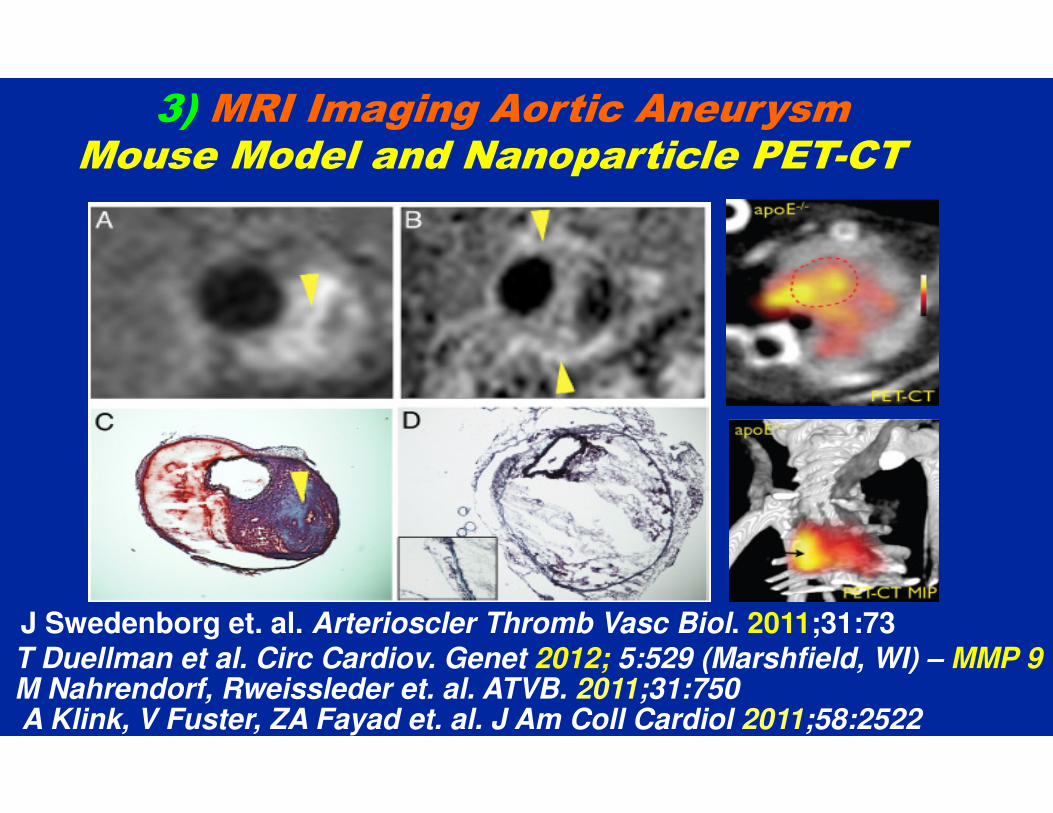
J Swedenborg et. al. Arterioscler Thromb Vasc Biol. 2011;31:73T Duellman et al. Circ Cardiov. Genet 2012; 5:529 (Marshfield, WI) – MMP 9M Nahrendorf, Rweissleder et. al. ATVB. 2011;31:750A Klink, V Fuster, ZA Fayad et. al. J Am Coll Cardiol 2011;58:2522
3) MRI Imaging Aortic Aneurysm Mouse Model and Nanoparticle PET-CT

Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA,AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Th.Ao.An. –TAD: Th.Ao.Dis. – AAA: Abd.Ao.An – AAR: Abd,Ao.Rupt.

dp / dtmax
BP
3
2
1.Arterial
Diameter
Hemodynamic Factors - Dilatation To Dissection
1 - EK Prokop, RF Palmer, MW Wheat. Circ Res 1970; 27:121 –TURKEY DISSECTION

Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA,AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Th.Ao.An. –TAD: Th.Ao.Dis. – AAA: Abd.Ao.An – AAR: Abd,Ao.Rupt.

TAD - J Sanz, A Einstein, V Fuster. In Acute Aortic Disease. Ed. J Elefteriades - 2010
Time
Baseline2) Vasodilator
(i.e., Nitroprusside)
(3) Beta blockade
1) TAD – Hemodynamic Approach

2) MFS - IMPACT OF ββββ BLOCKERS ON AORTIC ROOT DIAMETER
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Age (y.o.)
Ao
rtic
Dia
me
ter
(mm
)
10
15
20
25
30
35
40
45
Control Group: slope = 1.15±0.08
Treatment Group: slope = 1.04±0.05
M Ladouceur et al., AJC 2007; 99:406 (Paris)
Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA,AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Th.Ao.An. –TAD: Th.Ao.Dis. – AAA: Abd.Ao.An – AAR: Abd,Ao.Rupt.

COMPARE: evaluated the effect of losartan on aortic dilatation rate in
adults with Marfan syndrome (MFS). Patients with MFS have an increased
risk of life-threatening aortic complications, mostly preceded by aortic
dilatation. A total of 233 patients (47% female) underwent randomization
to losartan 50-100mg/d (n=116) or no additional treatment (n=117). Follow-
up was 3.1 ± 0.4 years.
End Points Losartan Control p
1. Aortic-root enlargement (mm) 0.77 1.35 0.014
No aortic-root growth (%) 50 31 0.022
2. Previous root replacem.: significant lower aortic arch expaansion
MARFAN SARTAN: 300 patients, 1ary EP-root diameter, 2ary EP-clinical
M Groenink et al., EHJ 2013; Aug 21 - Netherlands
1a) TAA in Marfan’s (and Other?) - ARBs Look Promising

1b) Atenolol vs Losartan in Children and Young Adults
with Marfan’s Syndrome
We conducted a randomized trial comparing losartan with atenolol in children and young adults with Marfan’s syndrome. The primary outcome was the rate of aortic-root enlargement, over a 3-year period. Secondary outcomes included the rate of change in the absolute diameter of the aortic root; the rate of change in aortic regurgitation; the time to aortic dissection, aortic-root surgery, or death; somatic growth; and the incidence of adverse events. A total of 21 clinical centers enrolled 608 participants, 6 months to 25 years of age (mean [±SD] age, 11.5±6 years. We found no significant difference in the rate of aortic-root dilatation between the two treatment groups over a 3-year period.
RV Lacro et al., NEJM 2014; 371:2061 – American Study

1c). Marfan Sartan: A Randomized, Double-Blind,Placebo-Controlled Trial
A double-blind, randomized, multi-centre, placebo-controlled, add on trial comparing Losartan (50 mg when < 50 kg, 100 mg otherwise) vs. placebo in patients with MFS according to Ghent criteria, age > 10 years old, and receiving standard therapy. 303 patients, mean age 29.9 years old, were randomized. The two groups were similar at baseline, 86% receiving ββββ-blocker therapy. The median follow-up was 3.5 years. Losartan was able to decrease blood pressure in patients with MFS but not to limit aortic dilatation during a 3-year period in patients > 10 years old. ββββ-blocker therapy alone should therefore remain the standard first line therapy in these patients.
O Milleron et al., Eur Heart J 2015; 36:2160 – French Study

O Milleron et. al. Eur Heart J. 2015;36:2160 – French Study
Marfan Sartan: A Randomized, Double-blind, Placebo-controlled Trial - Aortic Root Dilatation

Understanding - TAA, TAD, AAA, AAR - 2016
• Definition, Mortality, Imaging, ECM (4)
• Types, Demographics (TAA,TAD,AAA,AAR) (5)
• Etiology, Pathogenesis (TAA,TAD,AAA,AAR)
Dysfunctional Structure (5)
Hemodynamics (3)
Approach to Hemodynamics (2)
Approach to Dysfunctional Structure (1)
• Interventional (TAA,TAD,AAA,AAR) (4)
TAA: Th.Ao.An. –TAD: Th.Ao.Dis. – AAA: Abd.Ao.An – AAR: Abd,Ao.Rupt.

1a) TAA - Indications For Surgery
• ≥≥≥≥ 40 mm with indication for elective AVR (BAV etc)
• ≥≥≥≥ 45 mm in MFS
• ≥≥≥≥ 50 mm in BAV (?)
• ≥≥≥≥ 55 mm for an ascending aortic aneurysm,
• ≥≥≥≥ 60 mm for a descending aortic aneurysm;
• ≥≥≥≥ 70 mm in high-risk comorbidities;
• Growth rate ≥≥≥≥ 10 mm per year in <55 mm diameter
• Recurrent symptoms, Evidence of proximal dissect.
L Cozijnsen et al., Circ 2011; 123:924
Ince, CA Nienaber. Nature CV Med 2007; 4:418

M Gaudino et. al. J Thorac Cardiovasc Surg 2015;150:1120
1b) Temporal Trends In The Overall Number Of Aortic Root Procedures And By Type Of Operation

Predictors of Early and Medium-Term Outcome of 200 Consecutive Aortic Valve and Root Repairs
Between 2003 and 2013, 200 consecutive patients (149 men,
51 women; mean age, 52.1 years) with significant aortic
regurgitation and aortic root enlargement underwent aortic
valve repair and associated root reconstruction. Root
management consisted of either root remodeling or
reimplantation with Dacron prostheses. Early mortality was
2%, and early repair failure was 3%. Survival at a mean
follow-up of 48.6 ± 34.3 months was 94%, with a freedom from
reoperation of 91%. Repair failure and reoperation were
associated with bicuspid valve and complex leaflet repair.
MJ Jasinski et al., J Thorac Cardiovasc Surg 2015; 149:123 (Poland)

1c). Risk of Aortic Surgery After Definite Bicuspid Aortic Valve Diagnosis (n=416)
HI Michelena et. al. JAMA 2011;306:1104.

1d) Children With Marfan’s Or Loeys-dietz’s (N=35)Freedom From Reoperation And Actual Survival
0 12 24 36 48 60 72 840
10
20
30
40
50
60
70
80
90
100
Months After Operation
Survival
Reoperation
Even
t-F
ree S
urv
ival
(%)
ACEI postop, valve-sparing root replacement , and mitral valve repair have low reoperative risk
MD Everett, AT Yetman et al., JTCS 2009; 137:1327 (Salt Lake City, Denver)

2a). Contained Acute Aortic Syndrome
RE Clough et. al. Nat. Rev. Cardiol. 2015;12:103
RR Baliga et. al. J Am Coll Cardiol Img 2014;7:406
6-15% - CT / MR Diameter 16 mm, Rupture within 10 days
Early & Late Outcomes of Acute Type A Aortic Dissection With Intramural Hematoma
Between 2000 and 2013, we performed 418 repairs for acute
type A aortic dissection: 64 patients or 15% had type A IMH
and 354 patients 85% with typical dissection. With IMH, the
time from presentation to repair was, by strategy, longer
(median, 67 vs 6 hours), but no mortality occurred within 3
days of presentation. Mortality with IMH did not differ from
typical dissection (10.9% vs 14.7%). Although expectant repair
within 3 days may be applied, the purposeful delay imparted
little advantage.
AL Estrera et al., J Thorac Cardiovasc Surg 2015; 149:137 (Houston)

Acute Type A Intramural HematomaAnalysis of Current Management Strategy
AL Estrera et al., J Thorac Cardiovasc Surg 2015; 149:137 (Houston)
No mortality occurred within 3 days of presentation. Mortality with IMH
did not differ from typical dissection (10.9% vs 14.7%).
Best cutoff to Predict Events: 16 mm (Hematoma) - Often Type A

Early And Late Outcomes Of Acute Type A Aortic Dissection With Intramural Hematoma
AL Estrera et. al. J Thorac Cardiovasc Surg 2015;149:137

2b) Acute Type A Aortic Dissection: Comparing Bicuspid vs Tricuspid Valve
Between 1995 and 2011, 460 consecutive patients had acute type A aortic dissection - 91.6% with TAV and
8.4% with BAV. Patients with BAV have a distinctive dissection pattern with the entry tear frequently located in the aortic root and—despite their younger
age—are subject to substantial hospital mortality. For BAV patients, composite root replacement yields an outcome equal to an age- and gender-matched normal
population.
CD Etz et al., Eur J Cardio-Thoracic Surg 2015; 48:142

JM Zhu et. al. J Thorac Cardiovasc Surg. 2015;150: 101
2c). Neoaortic Arch From The Inside

Circulation. 2014;129:1610

2d) Irad – Type B Dissection – Survival Curve (N=300)
100
75
50
25
0
Su
rviv
al
rate
(%
)
300 600 900 1200
Log rank P =.61
Surgical (11%)Endovascular (11%)Medical (18%)
29%10%10%
Hospital Mortality
IRAD (Tsai TT et al.) Circulation 2006; 114:2226 –
IRAD (S Trimarchi et al.) Circulation 2010; 122:1283
Worst Prognosis: Hypotension, Pleural Effusion, Renal Failure
Refractory Pain & Hypertension
Days

RP Cambria. Advances at Mass General. 2015
Site of TEVAR Implementation

RO Afifi et. al. Circulation 2015;132:748
Outcomes of Patients With Acute Type B Aortic Dissection

3). Annual Risk of Rupture of AAA
K Craig Kent. N Engl J Med 2014;371:2101

Screening for AAA: U.S. Preventive ServicesTask Force Recommendation Statement
• The USPSTF recommends 1-time screening for AAA with
ultrasonography in men aged 65 to 75 years who have ever smoked. (B
recommendation)
• The USPSTF recommends that clinicians selectively offer screening
for AAA in men aged 65 to 75 years who have never smoked (C
recommendation)
• The USPSTF concludes that the current evidence is insufficient to
assess the balance of benefits and harms of screening for AAA in
women aged 65 to 75 years who have ever smoked. (1 statement)
• The USPSTF recommends against routine screening for AAA in women
who have never smoked. (D recommendation)
ML LeFevre et al., Ann Intern Med 2014; 161:281

4) Growth Rate for Small AAA – Meta-Analysis
Small AAAs of 3.0 cm – 5.4 cm in diameter are monitored by ultrasound
surveillance. The intervals between surveillance scans should be
chosen to detect an expanding aneurysm prior to rupture. Studies were
identified for inclusion through a systematic literature search through
December 2010. Study authors were contacted, which yielded 18 data
sets providing repeated ultrasound measurements of AAA diameter over
time in 15,471 patients. Predictions of the risk of exceeding 5.5-cm
diameter and of rupture within given time intervals were estimated.
Growth rates increased on average by 0.59 mm per year. In contrast to
the commonly adopted surveillance intervals in current AAA screening
programs, surveillance intervals of several years may be clinically
acceptable for the majority of patients with small AAA.
The RESCAN. JAMA 2013; 309:806 – JL Duncan BMJ 2012; 344:e2958 > 25 mm LT Risk
JM Guirguis-Blake et al., Ann Intern Med 2014; 160:321 – Validated Prospectively

ML Schermerhorn et. al. NEJM 2015;373:328
Long-Term Outcomes of Abdominal Aortic Aneurysm in the Medicare Population

Annual Proportion of Elective
Endovascular & Open Repairs for AAA in the US
K Craig Kent. N Engl J Med 2014;371:2101

ACC-New York, Dec. 12, 2015 No Disclosures
Diseases of The Aorta 2016Understanding & Approach
TAA, TAD, AAA, AAR






R Fattori et. al. J Am Coll Cardiol 2013;61:1661Medical Rx 1548, Surgical Rx 1706, TEVAR 3457
Interdisciplinary Expert Consensus Document on Management of TAD Type B - Complications

















