45
Diseases of the Aorta Mohamed Ashraf Ahmed., MD
| Date post: | 22-Mar-2017 |
| Category: |
Health & Medicine |
| Upload: | mohamed-ashraf |
| View: | 23 times |
| Download: | 0 times |
Diseases of the Aorta
Mohamed Ashraf Ahmed., MD

• The aorta is the main conduit and reservoir of oxygenated blood in the body.
• Diseases of the aorta account for significant cardiovascular morbidity and mortality worldwide.
• The incidence of aortic diseases is expected to rise with the increasing age of the population
• Diagnostic evaluation of aortic disorders has improved in the last 2 decades, allowing earlier diagnosis and therapeutic intervention.
Anatomy
• 1) The thoracic aorta – Aortic root, from the aortic annulus, including the sinuses
of Valsalva, up to the level just above the sinotubular junction;
– Ascending aorta, from the sinotubular junction to the innominate artery, with an average diameter of 3 cm;
– The arch, from the innominate artery to the left subclavian artery;
– The descending thoracic aorta, with an average diameter of 2.5 cm, which begins after the origin of the left subclavian artery.

• 2) The abdominal aorta begins when the descending thoracic aorta passes through the diaphragm.The abdominal aorta (average diameter, 2.0 cm) is further – Suprarenal – Infrarena


Histology • It is composed of three layers: – The intima is the innermost layer and includes the
single-layered endothelium. – The media is the thickest layer of the aortic wall and is
composed of sheets of elastic tissue, smooth muscle cells, and collagen, which provide the aorta with its tensile strength and distensibility.
– The adventitia is the outermost layer; it is composed of loose connective tissue and contains the vasa vasorum, which constitutes the blood supply to the aortic wall.


Pathologic Processes• 1) Cystic Medial Degeneration
– It is characterized by smooth muscle cell necrosis and apoptosis and by degeneration of elastic fibers within the media of the aortic wall.
– The weakened aortic wall is prone to aneurysm formation and dissection. – Typically seen in connective tissue diseases such as Marfan, Loeys-Dietz,
and Ehlers-Danlos syndromes• 2) Atherosclerosis
– Atherosclerosis can result in weakening of the aortic wall, making it prone to aneurysm formation or dissection.
– Risk factors of smoking, hypertension, hyperglycemia, and atherogenic lipoproteins.
– Atherosclerosis can also lead to the formation of complex atheromatous plaques, which are prone to embolization, resulting in cerebral and peripheral arterial occlusive events.

• 3) Inflammatory Disorders These occur in isolation or in the context of systemic
disorders such as inflammatory vasculitides. They include infectious (Syphilis) and noninfectious
causes (Giant Cell Arteritis, Takayasu’s Arteritis ankylosing spondylitis, rheumatoid arthritis)• 4) Trauma
Aortic Aneurysms
• Aortic aneurysm, refers to enlargement of the aorta beyond its normal diameter.
• A segment of the aorta is called aneurysmal if its maximal diameter is greater than 1.5 times that of the adjacent proximal normal segment. Aneurysm is described as fusiform if it symmetrically involves the entire circumference of the aorta.
• In contrast, a saccular aneurysm involves a localized protrusion of one of an area of the vessel wall.

• The epidemiology, pathophysiology, and management of aortic aneurysm are highly dependent on the anatomic location of the lesion.
• Objective of management is to avoid the potentially lethal complications of aortic rupture or dissection.

Thoracic Aortic Aneurysm• The incidence 10 cases per 100,000 person-years. • The leading causes include – Risk factors of hypertension and smoking, – Genetic syndromes of congenital bicuspid aortic valve,
Marfan syndrome, idiopathic annuloaortic ectasia Loeys-Dietz, Ehlers-Danlos, familial thoracic aortic aneurysm syndrome, and acquired types such as in ankylosing spondylitis syphilis, and trauma.
• Descending TAA may extend distally and involve the abdominal aorta, creating thoracoabdominal aneurysm.

Clinical presentation• Often asymptomatic at time of presentation.• Physical findings may also be absent. • When signs and symptoms occur, they are often the result of mass
effect. – The enlarging aorta can compress nearby structures, such as the SVC,
trachea, esophagus, and recurrent laryngeal nerve. This can result in the superior vena cava syndrome, stridor, dysphagia, and hoarseness, respectively.
– Progressive dilation of the aortic root can lead to aortic regurgitation, which may produce symptoms of congestive heart failure.
– Enlargement of the aortic sinuses can lead to narrowing of the coronary artery ostia, which may lead to myocardial ischemia and even infarction.
– Blood flow can be static in large aneurysms, predisposing to atheroma and thrombus formation and distal embolization.

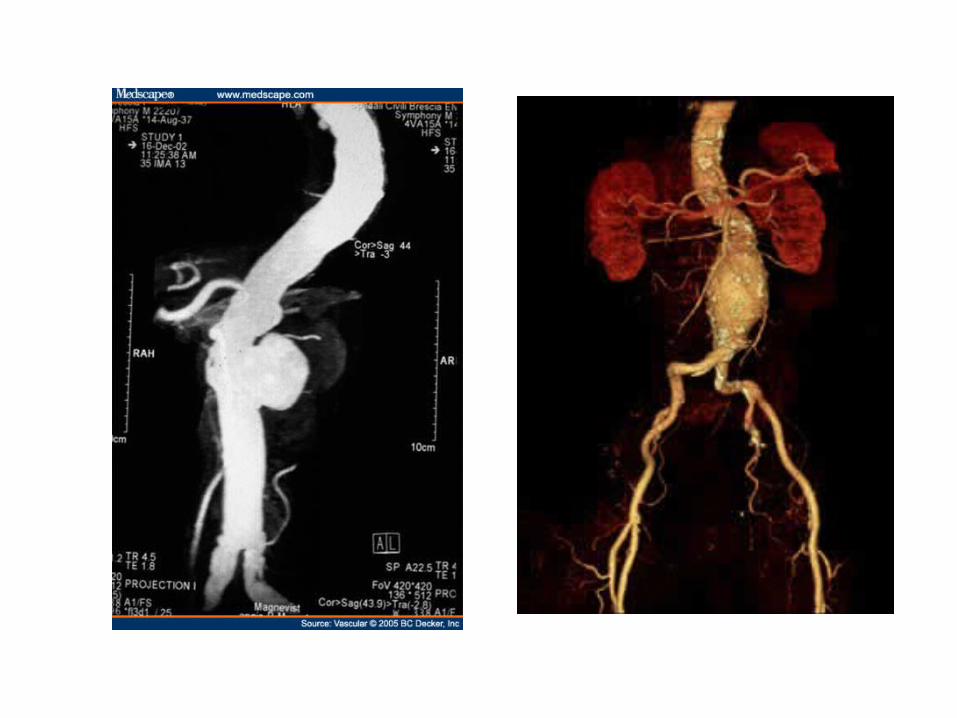
Noninvasive Imaging
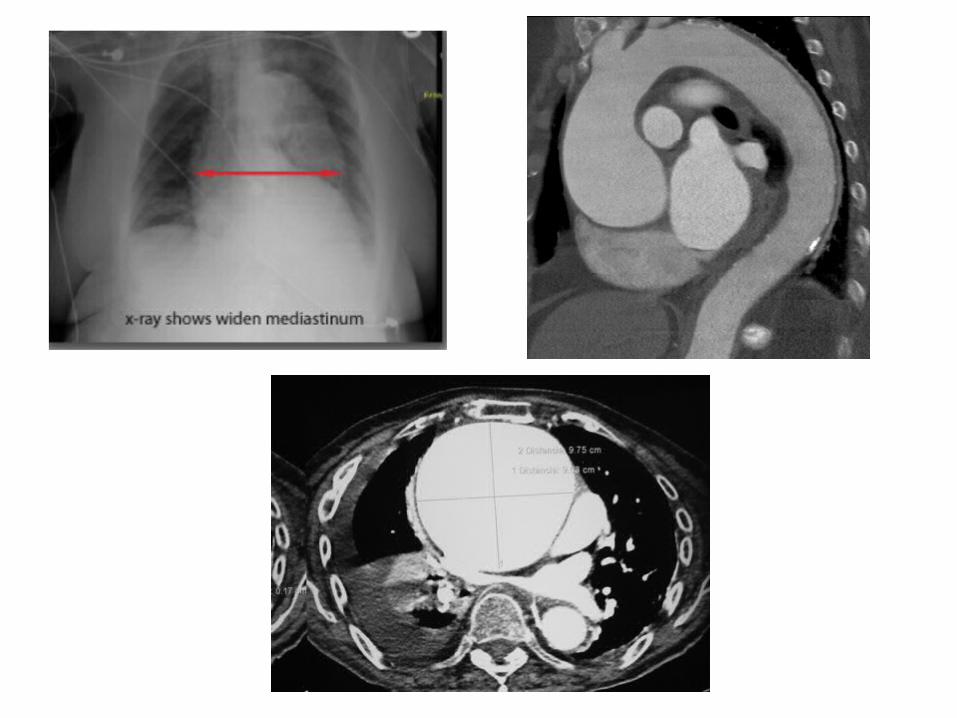
• Chest x-ray as a widened mediastinum or a prominent aortic knob.
• Transthoracic echocardiography is the most common modality for initial diagnosis and monitoring dilation of the aortic root.
• CT scanning and MRA are the preferred techniques to define the entire thoracic aorta and its branch vessels
Medical Treatment
• Beta blockade can slow the rate of thoracic aneurysm expansion in patients with Marfan syndrome.
• ARBs were found to slow the progression rate of aortic root dilation in Marfan patients.

Indications for Surgical Treatment• Dissection and rupture are the most-feared complications
of TAA, and prevention of these conditions is the purpose of elective surgical aortic repair.
• Size is clearly a risk factor and the principal indicator for dissection and rupture.
• Recommendations for surgical repair are 5.5 cm for a degenerative ascending TAA and 6.0 cm for a descending TAA.
• Patients with Marfan syndrome, Loeys-Dietz, bicuspid aortic valve, or family history of premature aortic instability should be considered for earlier repair.

Abdominal Aortic Aneurysm• AAA represents the most common form of arterial
aneurysm. • 75% of AAAs are infrarenal. • Atherosclerosis is the dominant risk factor in the
development of an AAA. • Additional risk factors associated with AAA are
– Male gender (four to five times more common in men)– Increasing age, smoking, and hypertension. – There is a clear familial predisposition to AAA, and relatives of
affected patients have up to a 30% increased risk for developing an AAA.
Clinical presentation• Asymptomatic AAA is often diagnosed on physical
examination by abdominal palpation.• The most common symptom is pain, which is usually
steady. The pain may be a localized abdominal pain or may radiate to the back, flank, or groin.
• Sudden onset of severe abdominal and back pain suggests rupture, representing a surgical emergency. Fewer than one third of patients with rupture present with the classic triad of pain, pulsatile abdominal mass, and hypotension.
• Atheroembolism may be the first manifestation of an AAA.

• Noninvasive Imaging– Ultrasonography, – CT scanning, aortography, and MRA.
• Medical Treatment– Beta blockade with careful control of hypertension – Smoking should be discontinued.

Indications for Surgical Treatment
• Mortality from an AAA is primarily related to rupture. • As with thoracic aneurysms, increasing size is the
indicator of rupture risk. • An aortic diameter of 5.0 to 5.5 cm is recommended
as an indication for prophylactic surgery in asymptomatic AAA patients.
• Aneurysms that expand rapidly (>0.5-1.0 cm/year) are also associated with an increased risk of rupture and are thus considered for elective surgical repair.

• Endovascular Stent-Graft Repair• An alternative therapeutic option for AAA
repair is the percutaneous placement of an endovascular stent-graft.


The Acute Aortic Syndromes
Acute Aortic dissection Intramural hematoma Intimal tear without hematoma Penetrating atherosclerotic ulcer Rupture of aortic aneurysm Aortic trauma

Aortic Dissection
• Aortic dissection involves splitting of the aortic wall within the media, which results in the formation of an aortic false lumen that courses along with a true lumen.
• The hallmark of aortic dissection is an intimal tear, which allows access of pulsatile high-pressure blood into the aortic media, separating it from the outer layers. Often, the so-called intimal flap is usually an intimal-medial flap.
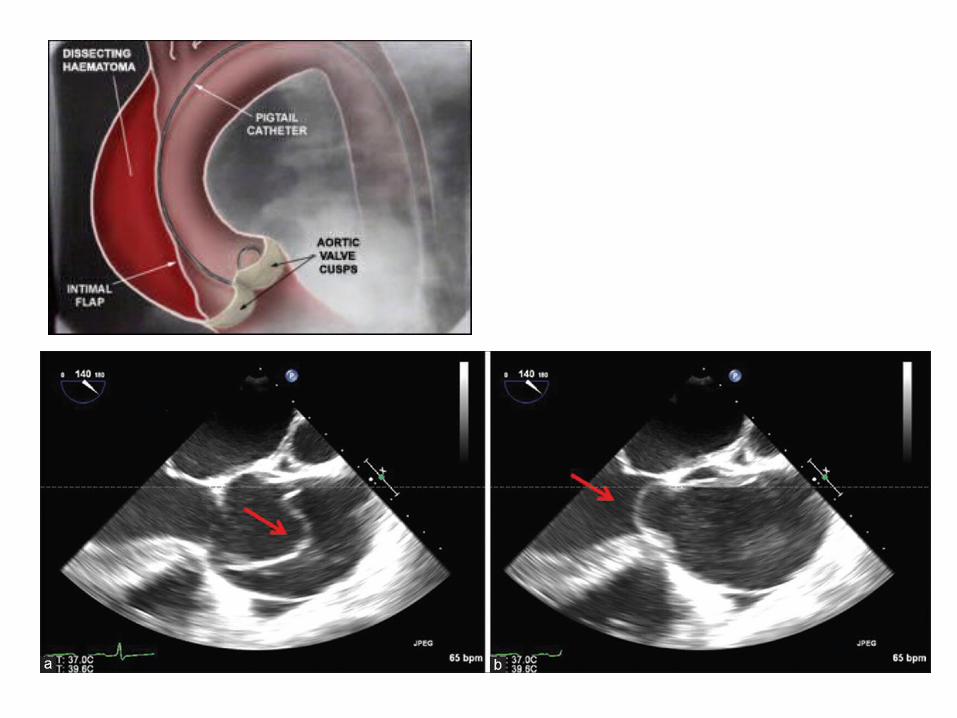
• The initiating event of dissection may be a tear in the intima. Alternatively, primary rupture of the vasa vasorum can result in an intramural hematoma, which secondarily leads to an intimal tear as blood vents from the intramural space.
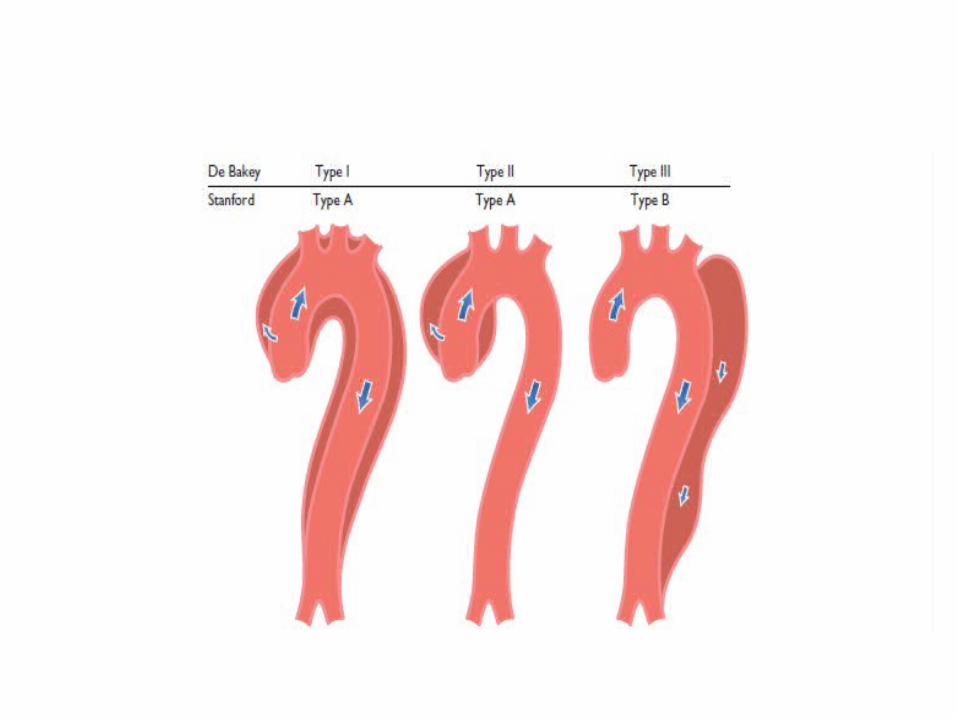

Classification of Aortic DissectionExtent of Aortic Involvement Type
DeBakey
Originates in ascending aorta, propagates to involve descending aorta I
Confined to ascending aorta II
Confined to descending thoracic aorta IIIa
Involves descending aorta, extending to abdominal aorta IIIb
Stanford
Involves ascending aorta A
Restricted to descending aorta B

Signs and Symptoms• Usually between 5th and 7th decades of life• More common in males.• Patients typically present with the acute onset of pain, which
occurs in up to 96% of cases. • Pain is often most severe at its onset and described as a tearing,
ripping, or stabbing sensation. Often, the pain is migratory, a crucial component of the history, reflecting propagation of the dissection. – Involvement of the ascending aorta results in anterior chest or neck pain,– Involvement of the descending thoracic aorta results in intrascapular or
subscapular pain from, – Involvement of thoraco abdominal aortia results in lower back and left
flank pain.

• Hypertension on presentation is common, more so in distal dissection, although hypotension can be seen if complications have developed, particularly in proximal dissections.
• The dissection may compromise flow to the great vessels and lead to pulse deficits.
• If the dissection involves the aortic root, commissural involvement of the aortic valve can lead to aortic regurgitation. A diastolic murmur is evident in these cases.
• Dissections can involve the ostia of the coronary arteries, resulting in acute myocardial ischemia and infarction.

• The dissection can extend proximally into the pericardial space, resulting in pericardial effusion and tamponade.
• Rupture into the pericardial space represents a common mode of death in patients with aortic dissection.

• Malperfusion syndromes with acute lower extremity, renal, or mesenteric ischemia can be seen in descending aortic dissections.
• Focal neurologic deficits can occur with involvement of the great vessels. Compromise of spinal artery perfusion may result in paraparesis.

Diagnostic Testing
• Chest X ray may be normal in cases of dissection. • Mediastinal widening, present in about 60% of cases. • Rupture into the pleural or pericardial space
manifests as pleural effusions or an enlarged cardiac silhouette.
• ECG can be normal but often shows nonspecific ST-T wave changes. Involvement of the coronary artery ostia can result in ST-segment elevation, representing an acute myocardial injury pattern.

• Transthoracic echocardiography can on occasion identify a proximal or even distal dissection flap. Even if a flap is not seen, the presence of aortic dilation, aortic regurgitation, or an unexplained pericardial effusion can be important clues in the diagnostic consideration of dissection in a patient with chest pain.
• More definitive diagnostic modalities include transesophageal echocardiography (TEE), Computed tomography (CT) and Magnetic resonance angiography (MRA).


Treatment
• Medical treatment:– β-adrenergic blockade (or IV verapamil and
diltiazem) should be initiated as soon as the diagnosis of dissection is considered.
– In patients who are hypertensive, IV beta blockade and sodium nitroprusside are the treatment agents of choice.

• Dissections that involve the ascending aorta (proximal, type A) require urgent surgical therapy because there is a very high early mortality rate (approaching 1%-2% per hour for the first 24-48 hours).

• Dissections that involve the descending aorta (distal, type B) should initially be treated medically.
• Data suggest that medical therapy is the preferred initial treatment, with surgery guided by a complication-specific approach.

• Surgery should be considered for the following indications: – Evidence of organ ischemia secondary to
compromise of the branch vessels.– Persistent pain; aneurysm formation, particularly if
saccular; and retrograde dissection to a proximal extent.
– Distal (type B) dissections in Marfan syndrome patients carry a poor prognosis and have thus led to recommendations of early aortic surgery.

THANK YOU FOR ATTENTION

















