96
DISEASES OF THE THORACIC AORTA THORSANG CHAYOVAN 19.01.2016
| Date post: | 16-Apr-2017 |
| Category: |
Health & Medicine |
| Upload: | thorsang-chayovan |
| View: | 500 times |
| Download: | 3 times |
DISEASES OF THE THORACIC AORTA
THORSANG CHAYOVAN
19.01.2016

Resources
Diseases of the thoracic aorta
• Normal aorta and aortic variation• Aortic spindle, ductus bump, cervical aortic arch
• Aortic aneurysm• Atherosclerotic aneurysm
• Mycotic aneurysm
• Traumatic aortic injury: blunt aortic injury
• Acute nontraumatic aortic syndromes • Aortic dissection
• Intramural hematoma• Penetrating atherosclerotic ulcer



Aortic spindle

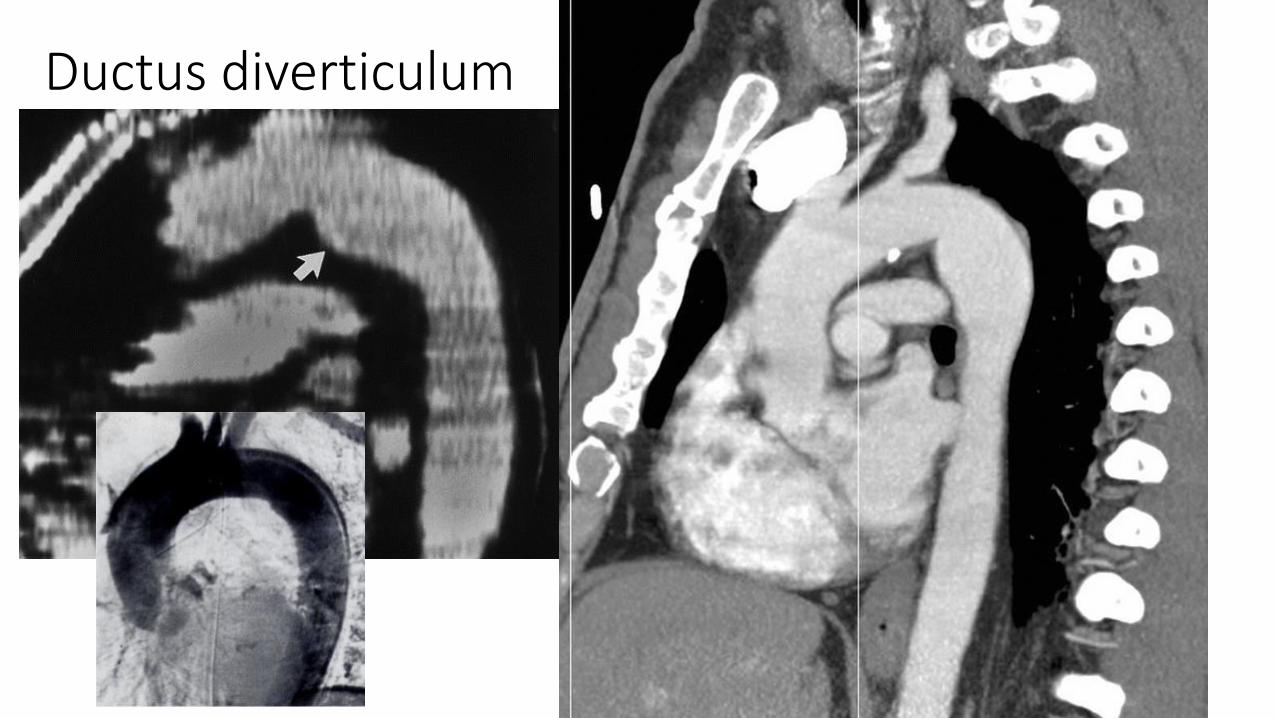
Ductus diverticulum

Atypical ductus diverticulum



Cervical Aortic Arch • Apical mass• Absence of the normal aortic knob• Displacement of the trachea to the side
opposite the arch• Anomalous origins of the great vessels• Right-sided lesions
o Right apical mass-like densityo Absence of aortic knob on lefto Aorta usually descends on left (80%)o Displace the trachea and esophagus forwardo Branching of major vessels may be mirror-
image• Left-sided lesions
o Aortic knob appears at apex of left lungo Aorta usually descends on the left (70%)o Do not usually displace the trachea and
esophagus forwardTürkvatan, Aysel, Fatma Gül Büyükbayraktar, Tülay Ölçer, and Turhan Cumhur. "Congenital Anomalies of the Aortic Arch: Evaluation with the Use of Multidetector Computed Tomography." Korean J RadiolKorean Journal of Radiology 10.2 (2009): 176.

Diameters (cm)

Diameters (cm)
Ascending Descending
Risk for rupture 6 5
Treatment 5.5 6.5
Monitoring 4.5 5.5
• Normal growth rate 0.12cm/year
• Saccular aneurysms--often pseudo-aneurysms from trauma, infection or PAU• Less predictable
• Dimensions given are not applicable
Atherosclerotic aortic aneurysm
• Common degenerative phenomena
• Risk factor: hypertension, age
• Symptoms• Asymptomatic
• Chest pain
• Compression effects -- hoarse voice, atelectasis of the left lung or left lower lobe, dysphagia, right/left PAs


• Complication – rupture• Risk when--Ascending AA > ? cm, descending AA > ? cm
• Ascending AA > 5.5 cm, descending AA > 6.5 cm repaired
• Saccular aneurysms – increased risk for rupture
• Pts with CNT disease -- repair at smaller diameters (5 and 6 cm respectively)
Atherosclerotic aortic aneurysm

• Fusiform; a few are saccular
• Fusiform aneurysms -- aortic arch or descending aorta
• Saccular aneurysms -- descending aorta, (aortic arch)
• Differentiation from masses by • Relationship with the aorta• Presence of curvilinear calcification in its wall – rarely
detectable
• Crescent-shaped thrombus lines the periphery
• Flecks of calcification along the inner margin
Atherosclerotic aortic aneurysm

Mycotic aneurysm of the aorta
• Risk factors• IV drug abuse
• Valvular disease
• Congenital disorders of heart/aorta
• Previous cardiac/aortic surgery
• Adjacent pyogenic infection/vertebral osteomyelitis• Immunocompromised

• Any site in the aorta
• Fever and leukocytosis
• Saccular in shape – tends to rupture
• Mycotic aneurysms VS other saccular aneurysms
• Enlarge rapidly
• Lack of calcium
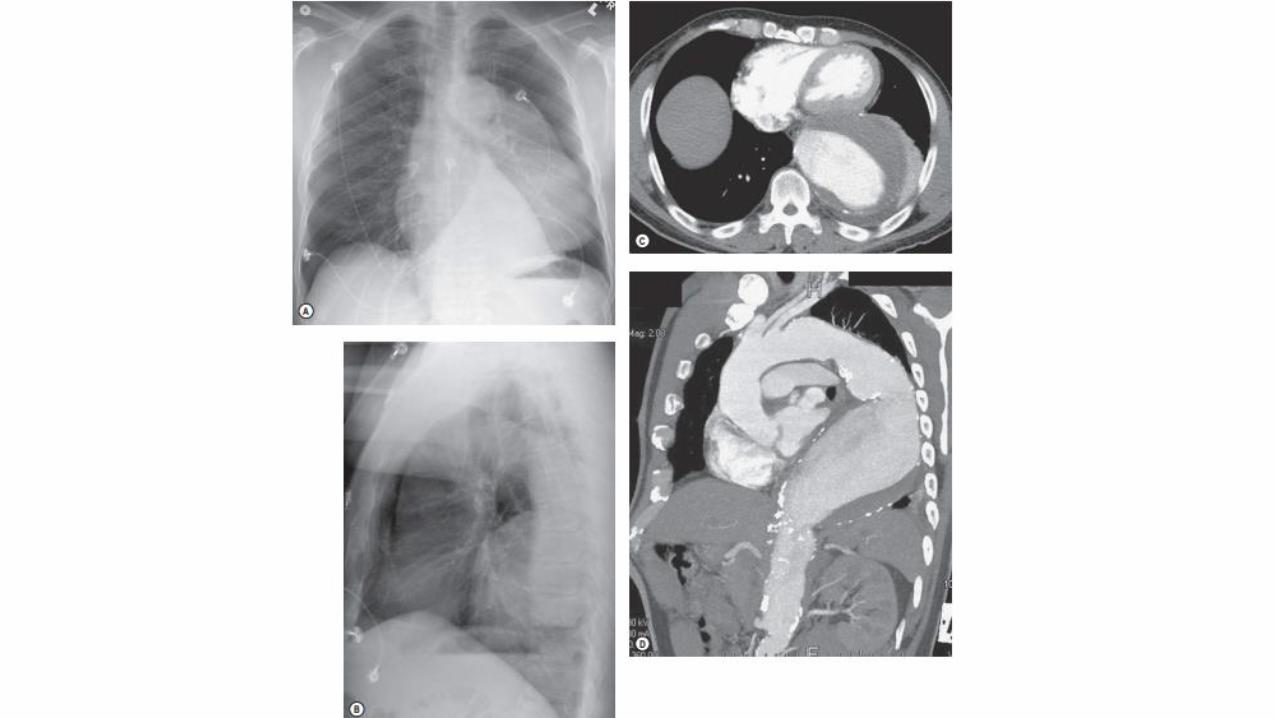
Mycotic aneurysm of the aorta
• Ill-defined aortic wall with evidence of rupture
• Inflammatory changes around the aneurysm with gas bubble
• Periaortic fluid collections
• Thrombus formation within a false lumen after rupture
INFLAMMATION!
Mycotic aneurysm of the aorta




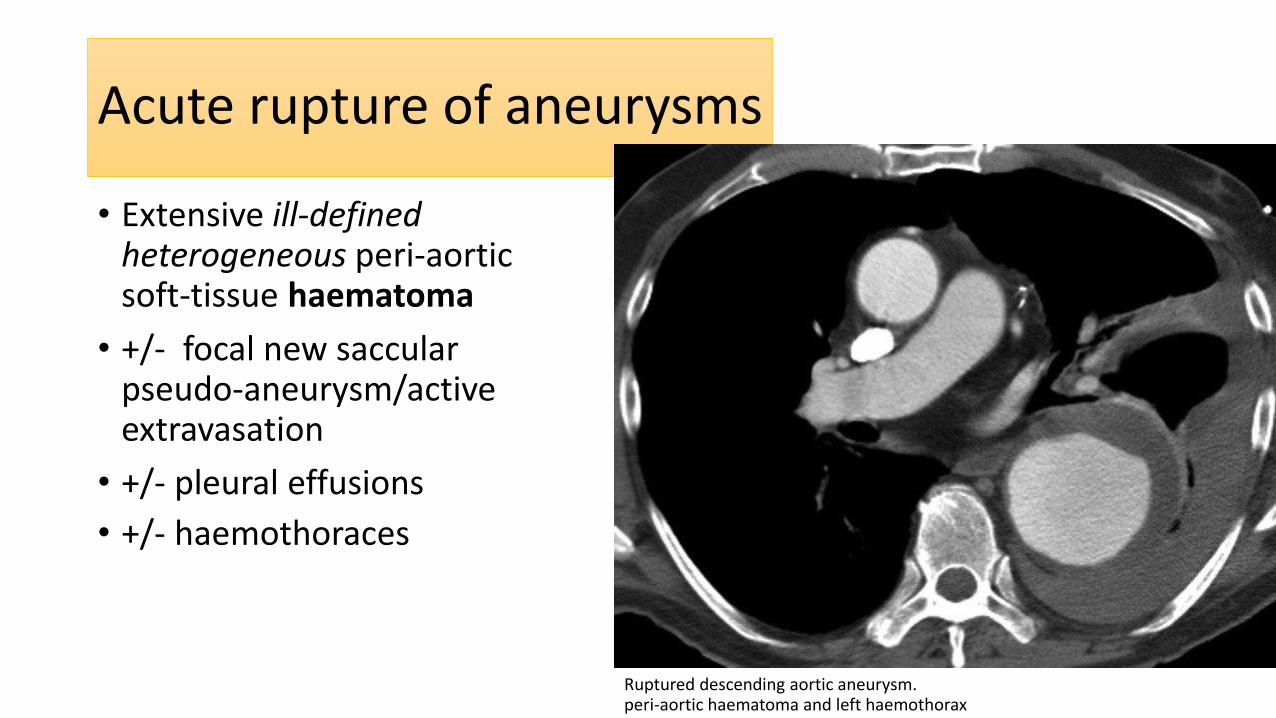
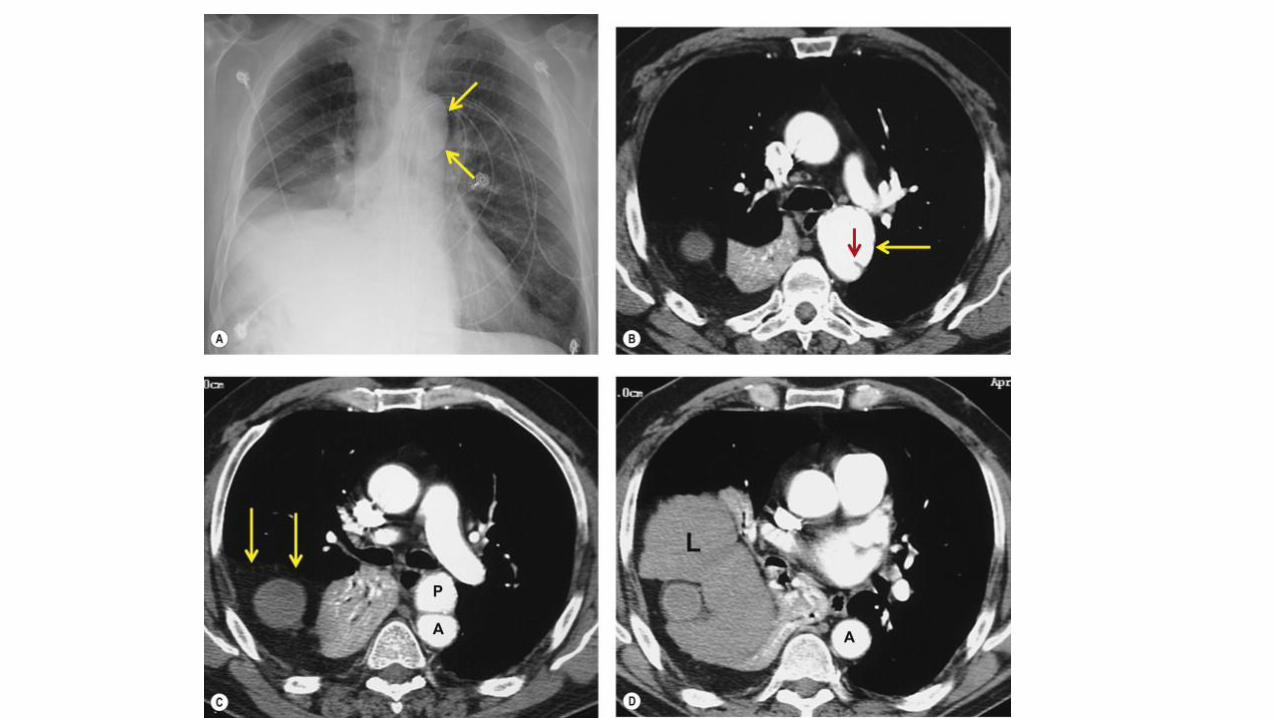
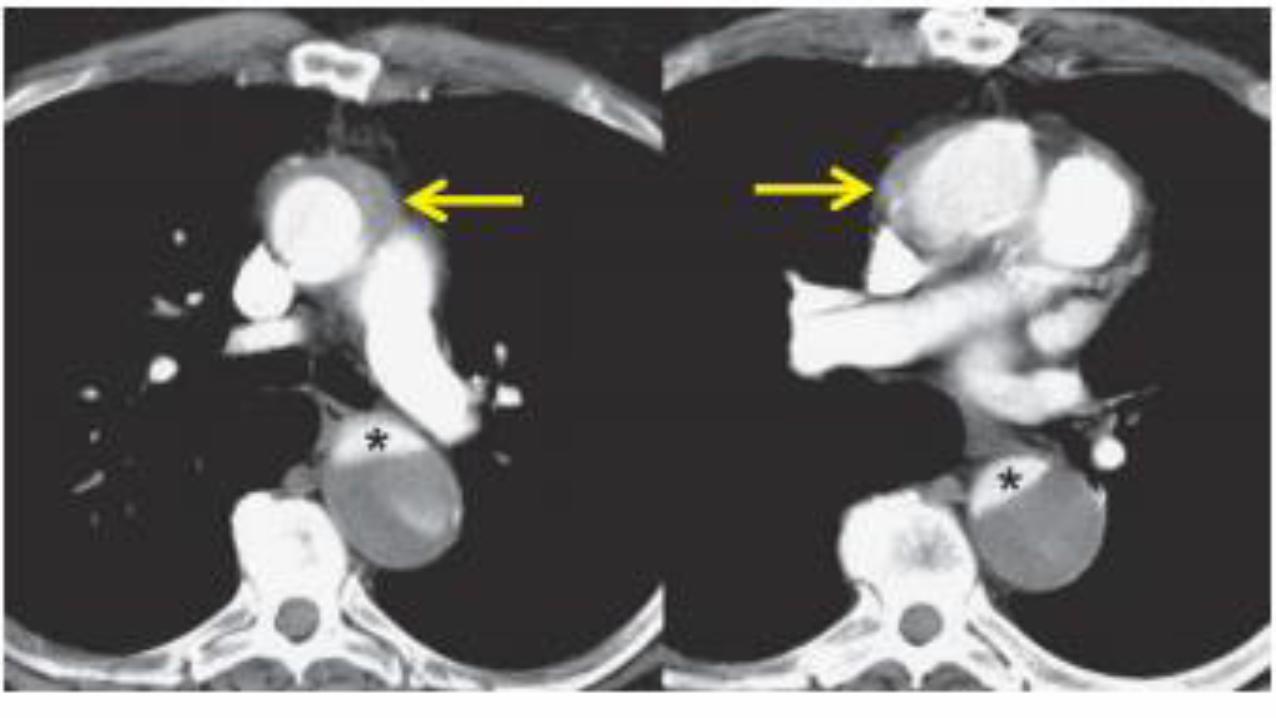
Acute rupture of aneurysms
• Extensive ill-defined heterogeneous peri-aortic soft-tissue haematoma
• +/- focal new saccular pseudo-aneurysm/active extravasation
• +/- pleural effusions
• +/- haemothoraces
Ruptured descending aortic aneurysm. peri-aortic haematoma and left haemothorax

Acute rupture of aneurysms


Traumatic aortic injury
•Blunt aortic injury
•Only 10–20% survive the initial injury
•Rapid diagnosis of BAI in survivors is critical • 30% of affected patients die in the first 6 hours • 40–50% die in the first 24 hours• Some survives >> a chronic pseudoaneurysm
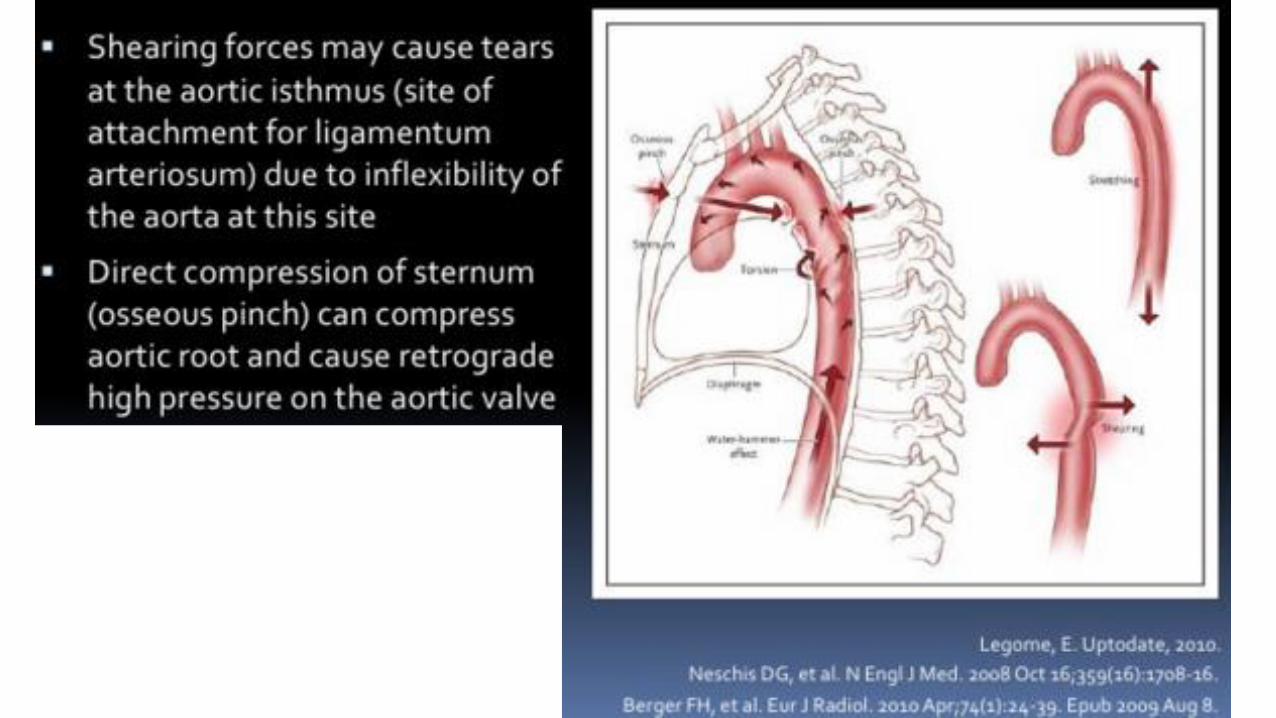

• Site of injury
• 95% at the aortic isthmus
• <5% in the ascending aorta
• 1% in the distal descending aorta
• Rarely in the abdominal aorta
Traumatic aortic injury

Chest radiograph
• Screen for mediastinal hemorrhage• Indirect marker for BAI; however, nonspecific
• DDx: sternal fracture, venous bleeding, spine fractures
• >90% with mediastinal hematoma on CXR not BAI• Erect AP chest at full inspiration > supine detecting a true-negative
mediastinum

• Mediastinal widening at vascular pedicle• Width >8 cm on supine position with
a source-to-detector distance of 100 cm
• Mediastinal/thoracic width >0.25
• Obscuration of the aortic arch• Opacification of the AP window• Shift of trachea to the right• Shift of esophagus to the right• Displaced superior vena cava• Depressed left main bronchus
• Left apical pleural cap• Widened left paraspinal reflection• Widened right paraspinal reflection• Widened right paratracheal stripe• Evidence of significant chest
trauma• Multiple rib fractures (esp. first rib)• Lung contusion• Hemothorax (esp.left)• Pneumothorax
Chest radiograph


CT to rule out BAI?
History of motor vehicle accident at a speed of more than • 16 km/h (unrestrained)• 48 km/h (restrained)
Fall from a height of 7 m




CT: current ‘gold standard’ for BAI diagnosis
Indirect signs of BAI
• Periaortic or perivascular hematoma
Direct signs of BAI
• Focal disruption of the wall
• Extravasation of contrast
• Intimal flap
• Pseudoaneurysm

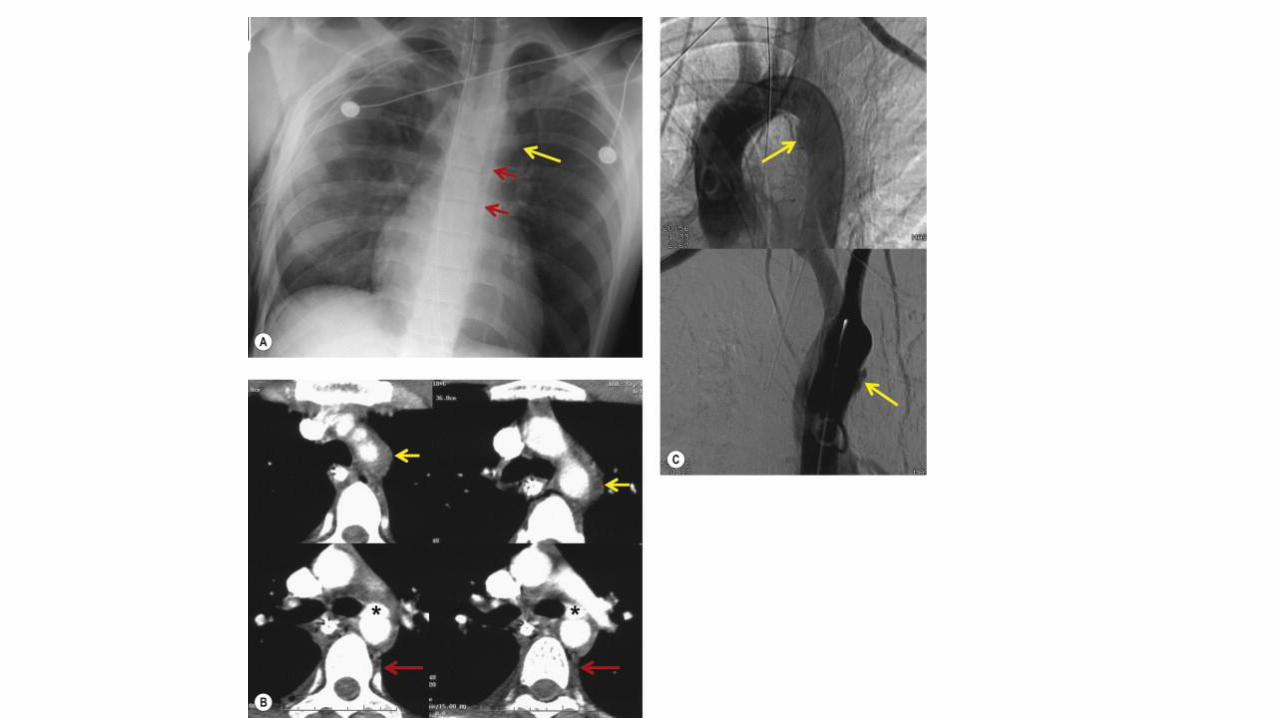
Pseudoaneurysm
• Consequence
• Anteromedial wall of the distal aortic arch-upper descending aorta near the ligamentum arteriosum• Easily contained in a pseudoaneurysm by surrounding structures • On the contrary, posterior laceration >> uncontrolled hemorrhage
• Symptoms• Hoarse--recurrent laryngeal nerve compression• Dysphagia—esophageal compression• Chest pain, dyspnea
• Small aneurysms enlarge >> AP window masses
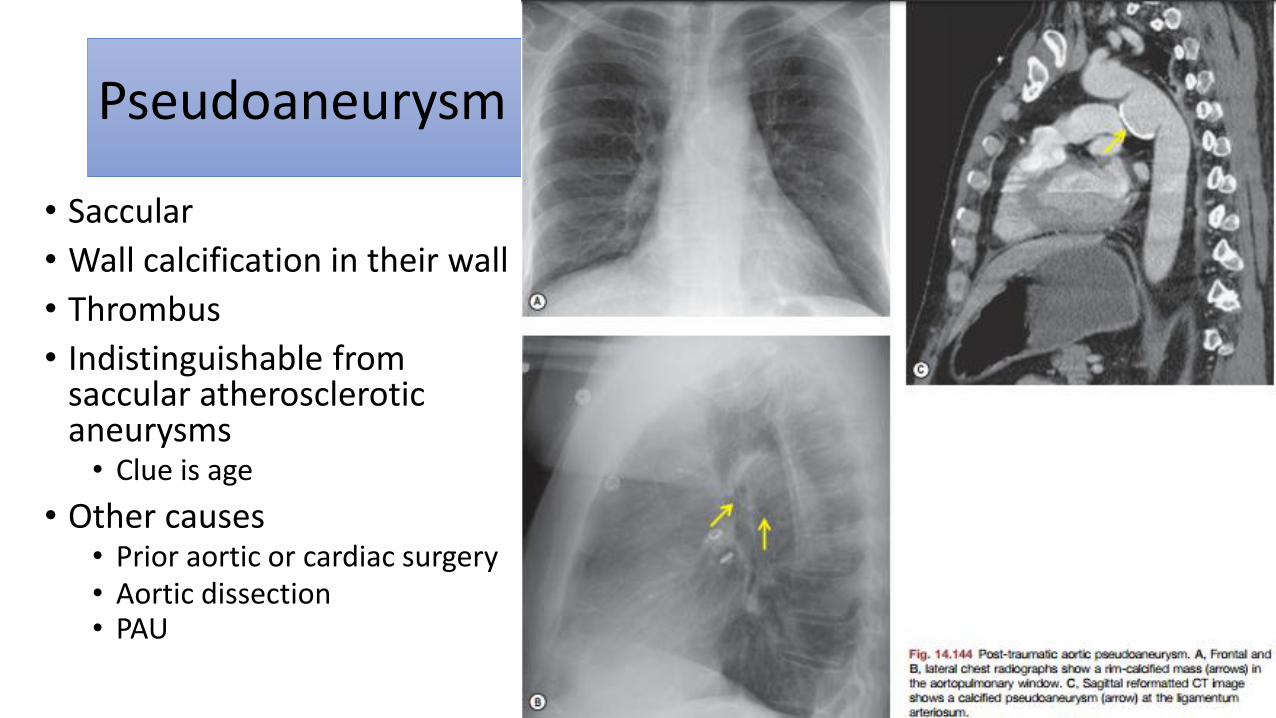
Pseudoaneurysm
• Saccular
• Wall calcification in their wall
• Thrombus
• Indistinguishable from saccular atherosclerotic aneurysms • Clue is age
• Other causes • Prior aortic or cardiac surgery• Aortic dissection• PAU




Minimal aortic injury (MAI)
• A small (less than 1 cm) intimal flap
• No other aortic abnormality
• No or minimal periaortic hematoma
• Incidence 10%
• Confirmed either by surgery or by endovascular ultrasound
• Follow-up >> resolved or a small pseudoaneurysm
• Hemodynamically stable patients, can be managed conservatively, but followed

Acute nontraumatic aortic syndromes
• Aortic dissection, intramural hematoma, and penetrating atherosclerotic ulcer
• Atherosclerosis, systemic hypertension
• Elderly adults
• Often clinically indistinguishable

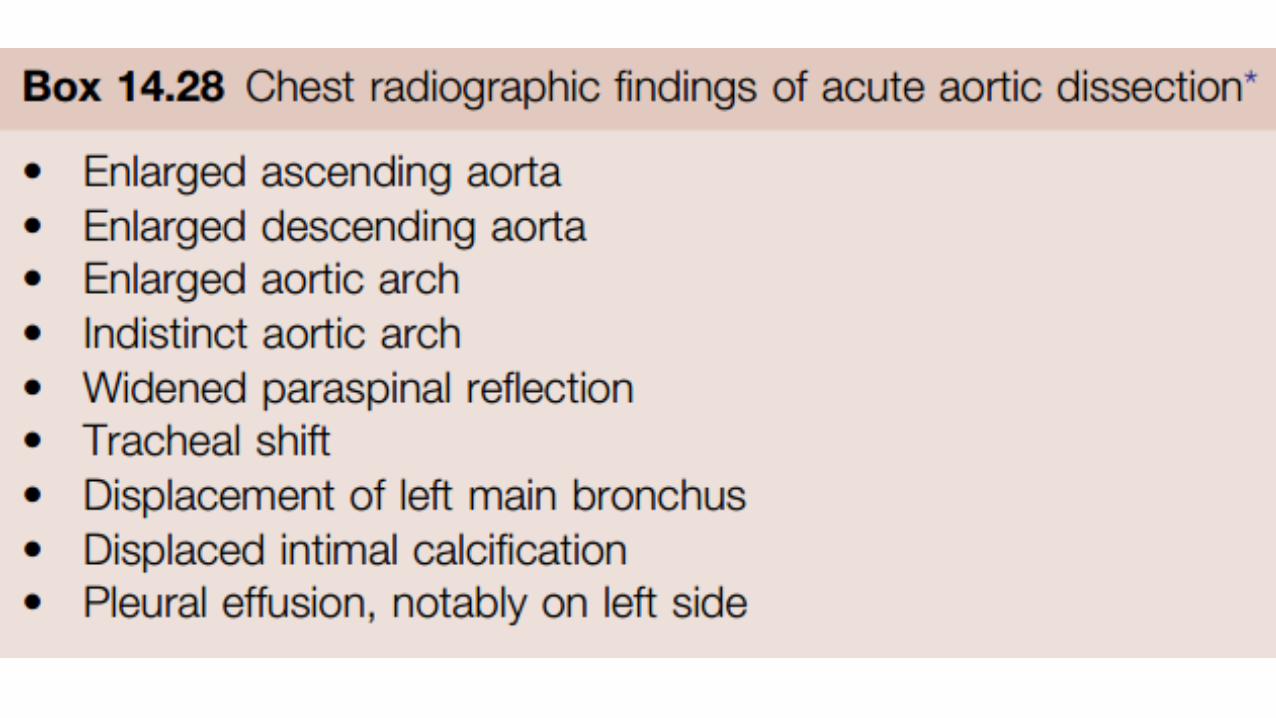
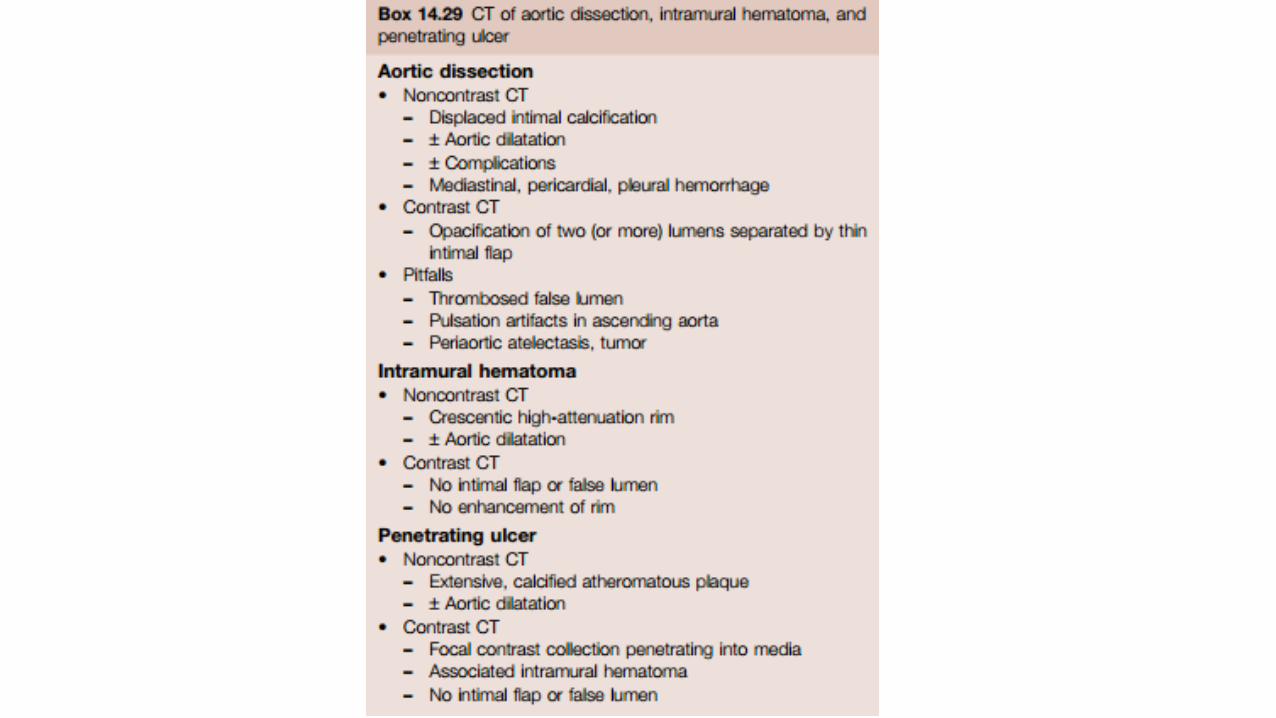
Aortic dissection
• Blood collections in aortic media communicate with the lumen through intimal tear
• Progressive separation (intima-media) >> false channel
• The dissection channel usually spirals >> false lumen is…• anterior and right in the ascending aorta
• posterior and left in the descending aorta
• Predisposing factors: HT, atherosclerosis, CNT d/o, Turner syndrome, pregnancy, and cocaine
• Classification: acute (first 14 days) or chronic (after 14 days)
Worse prognosis Aneurysm >> rupture

Aortic dissection

Aortic dissection: Stanford
• Type A
>> AR
>> Rupture into pericardium Tamponade
>> Compress arteries from AA+coronary arteries
• Type B dissections >> Sx if…• Persistent symptoms• Progression of dissection• Ischemic complications
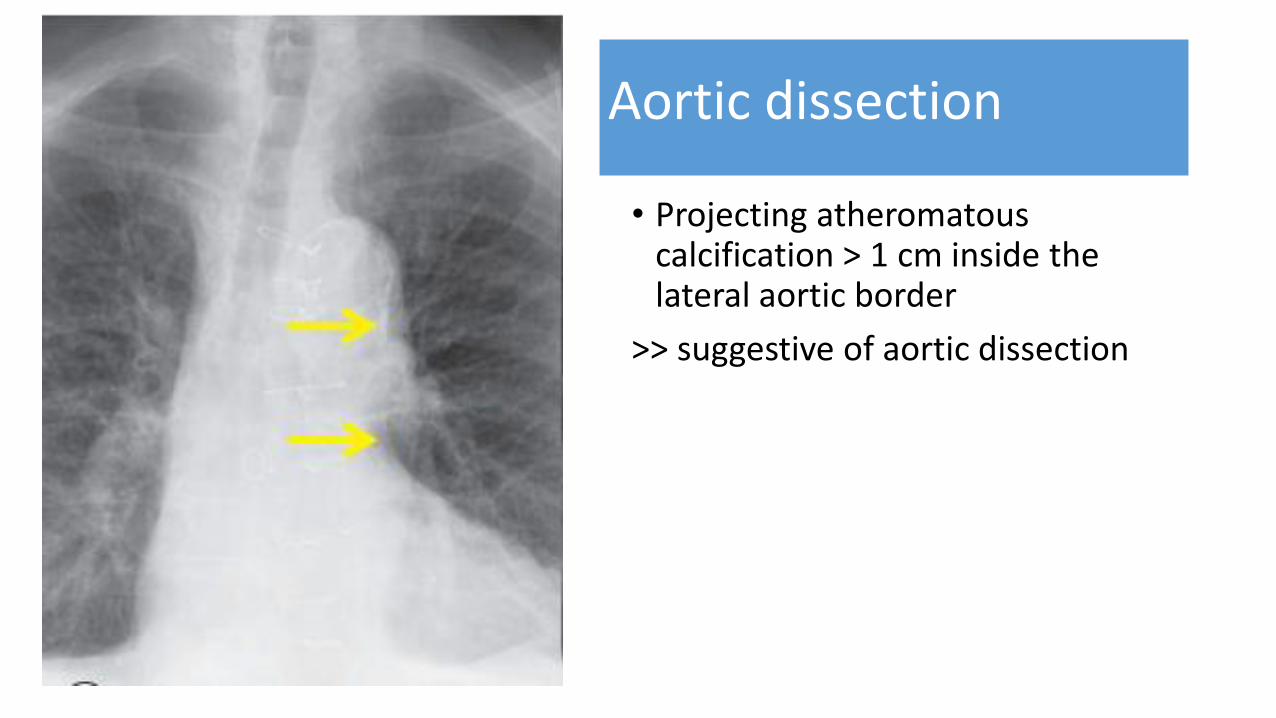
Aortic dissection
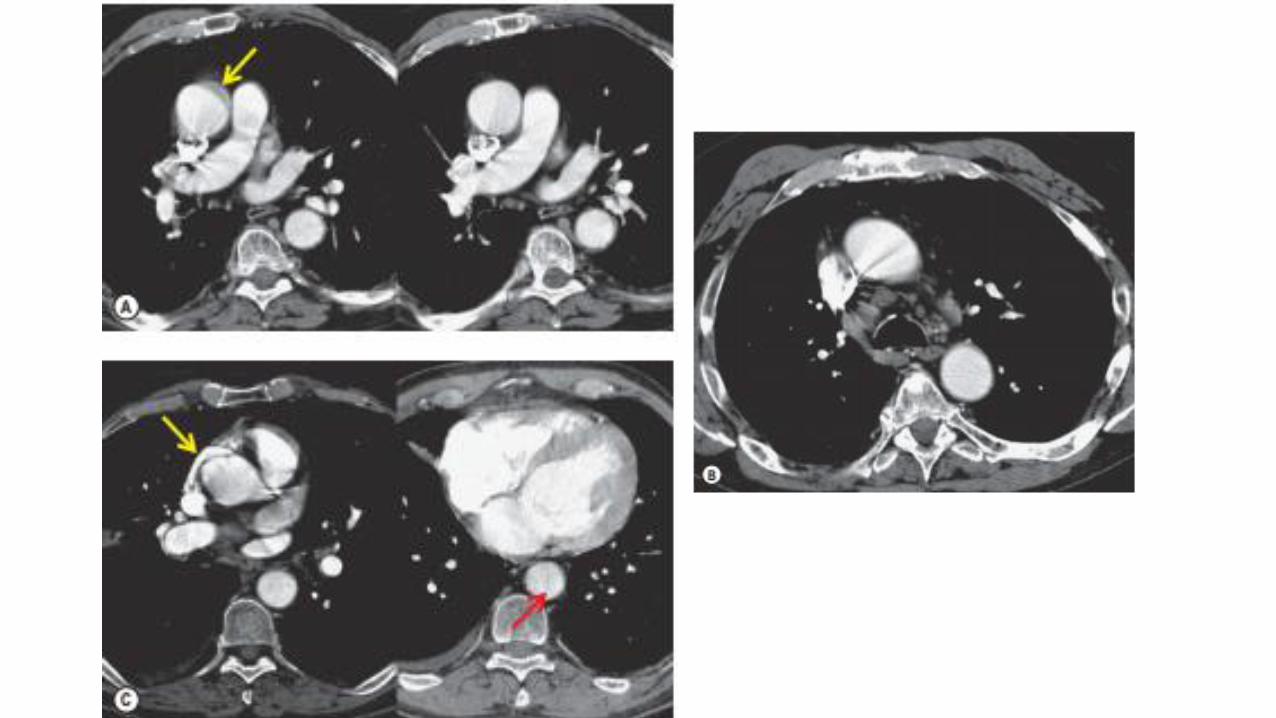
• Projecting atheromatous calcification > 1 cm inside the lateral aortic border
>> suggestive of aortic dissection




Intimal flap VS streak artifact
• Intimal flaps are gently curved structures of uniform thickness conforming to the configuration of the aorta
• Streak artifacts are straight, vary in thickness; extending outside the aorta

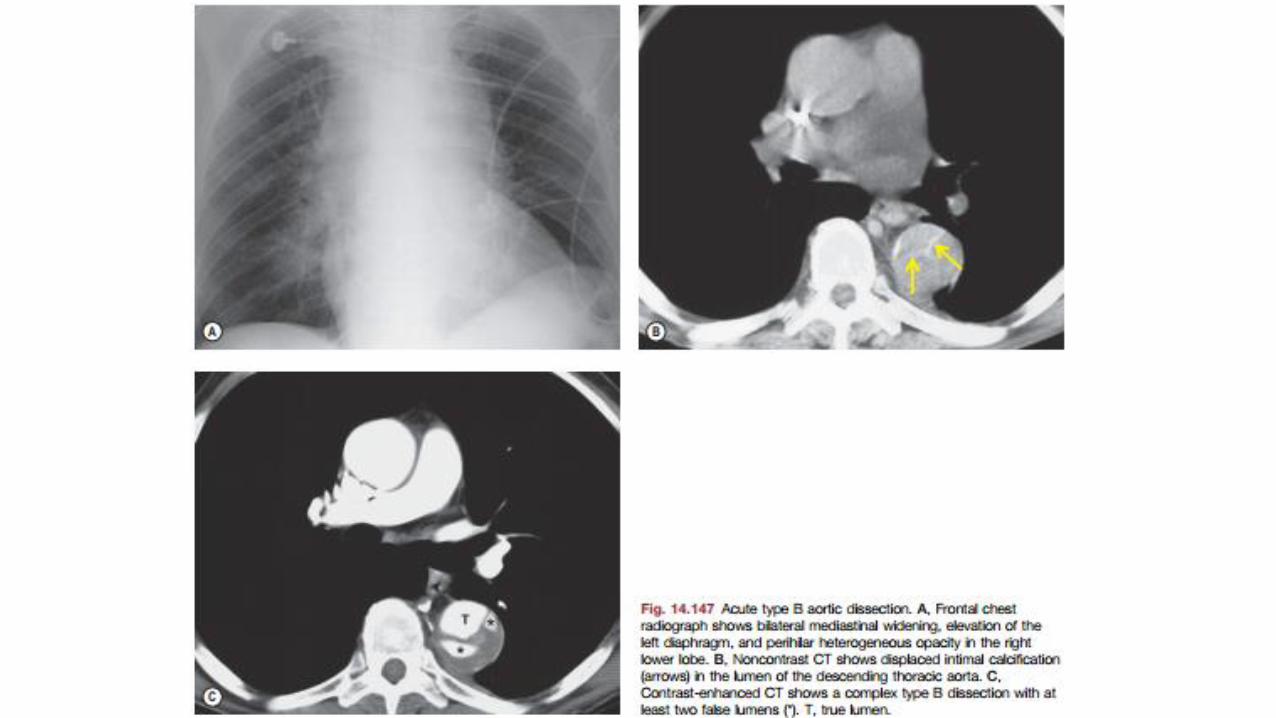
False VS true lumen
False lumen
• Larger
• Cobwebs-- Thin strands of tissue
• ‘Beak’ sign--blood in the false channel undermines the intimal flap
• Slower flow
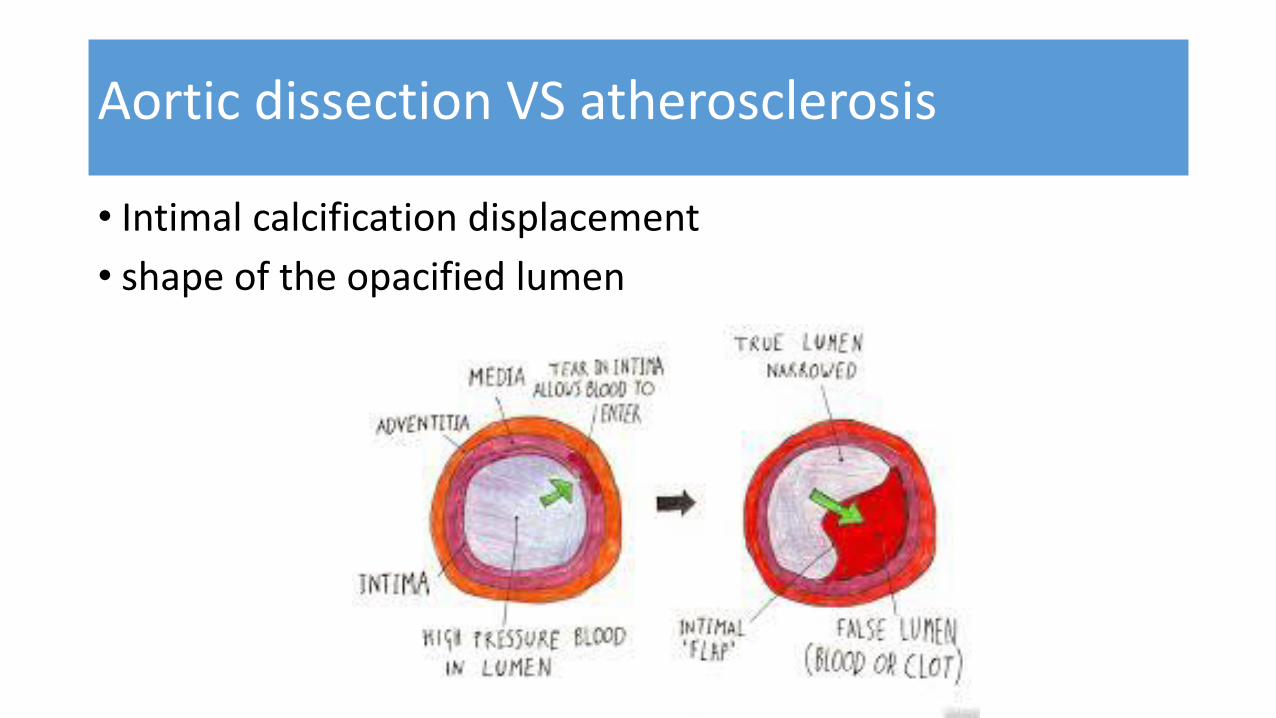
• Intimal calcification displacement
• shape of the opacified lumen
Aortic dissection VS atherosclerosis



Aortic dissection: complications
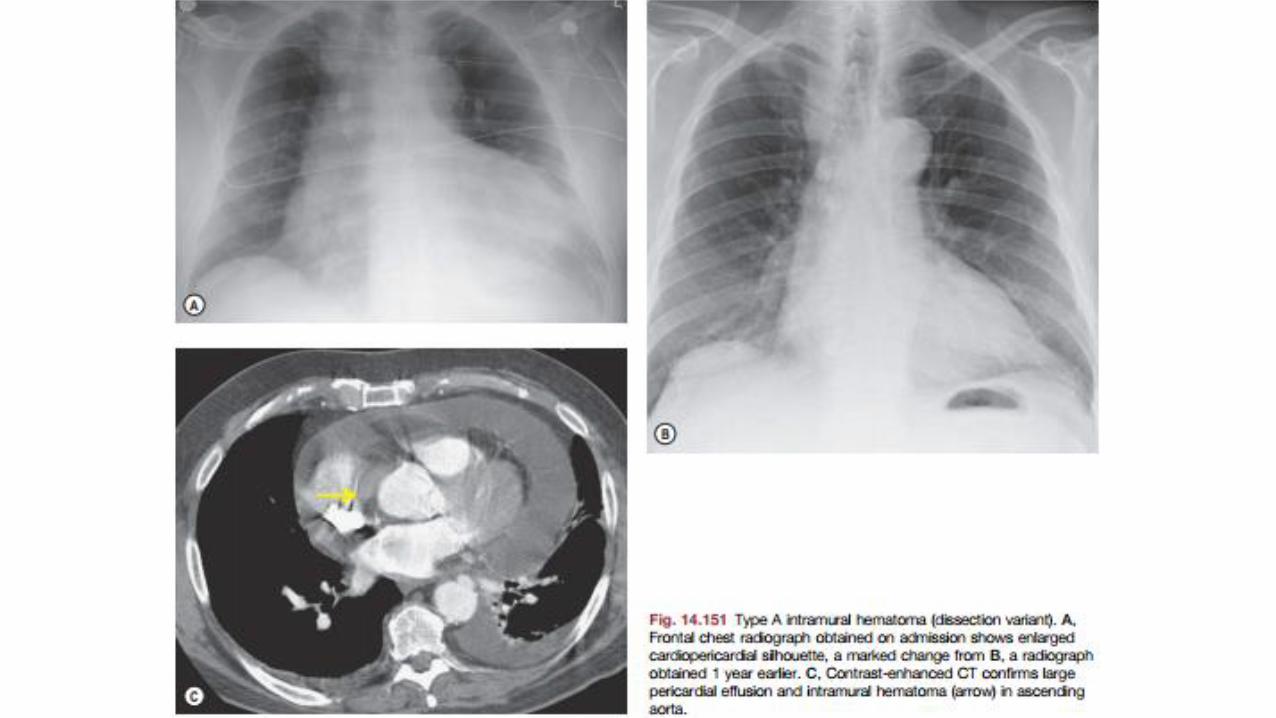
• Type A• Pericardial hemorrhage and tamponade
• Aortic valve rupture
• Acute aortic insufficiency
• Coronary artery dissection or origin from the false lumen with subsequent myocardial perfusion compromise and infarction
• Carotid artery dissection and stroke
• Others: dissection into the aortic branches: renal, bowel, and splenic infarction; aneurysm formation; and hemothorax





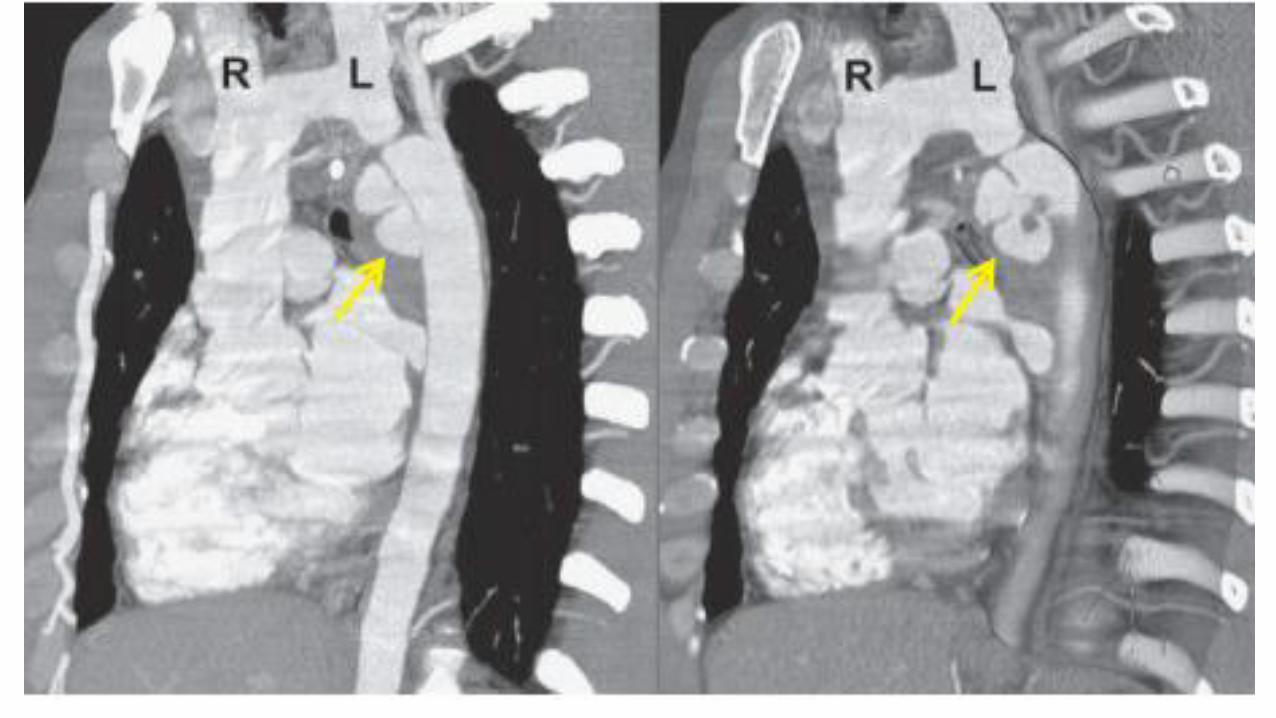
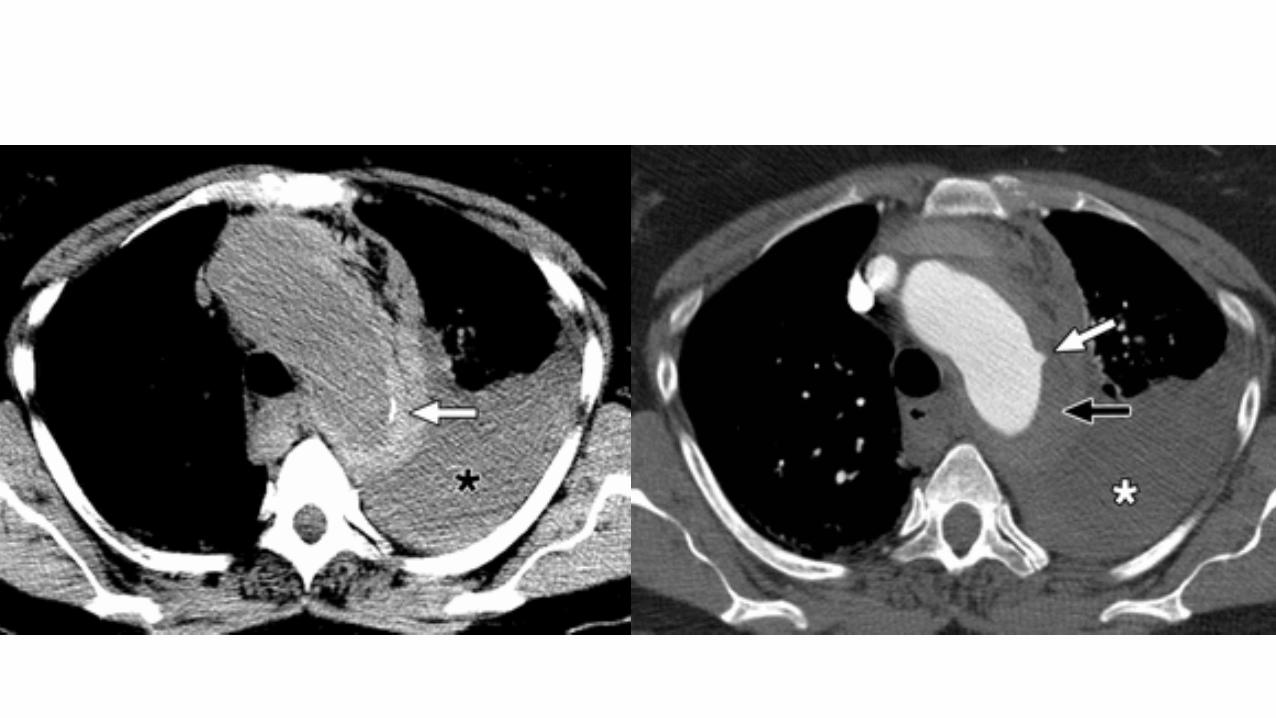
Intramural hematoma
• Intramural hematoma without intimal flap
= Noncommunicating aortic dissection
= Atypical dissection
Cause:
• Intramural ischemia
• Bleeding from the vasa vasorum, trauma, or PAU
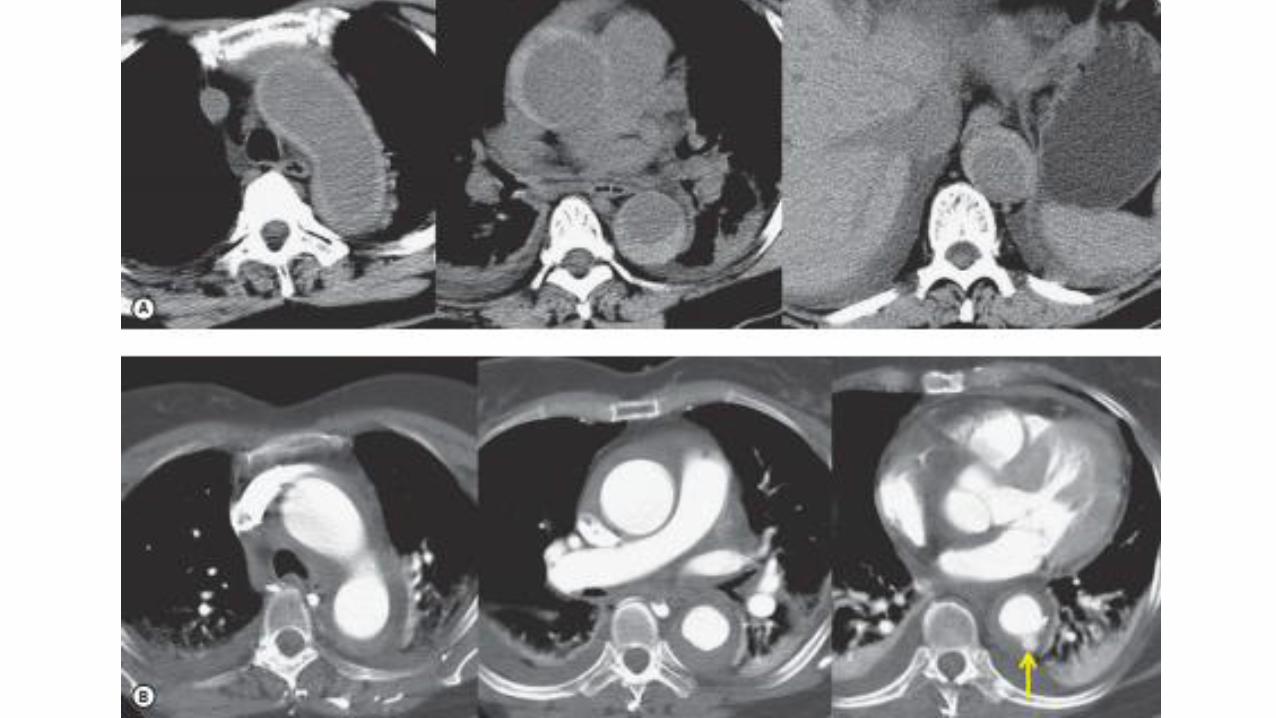
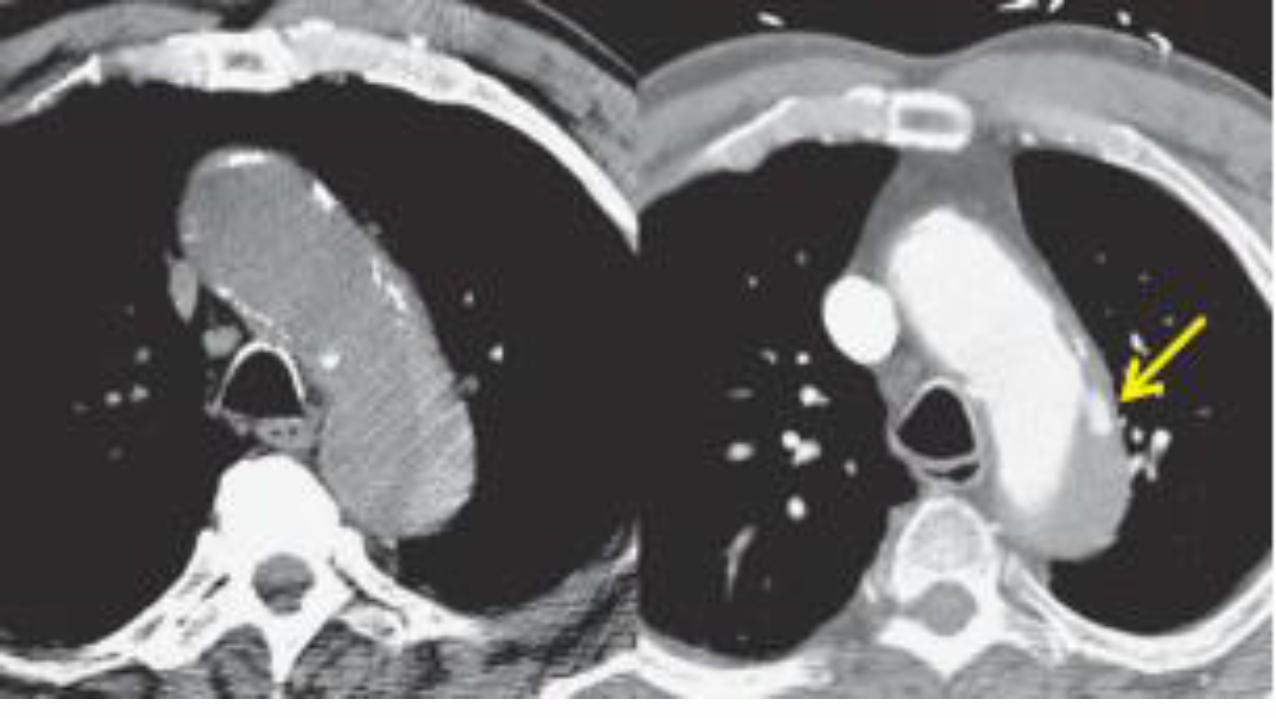
• Focal protrusions of contrast through atheroma into the aortic wall
• NCCT: A crescentic hyperdense rim in the aortic wall
• No contrast flowing in the false lumen
• Calcified atheroma on the displaced internal intima
• VS chronic smooth intraluminal thrombus
• Follow-up imaging of IMH--contrast can develop in the haematoma
= ulcer-like projections
= a new intimal tear, PAU or a branch pseudoaneurysm
Intramural hematoma



Intramural hematoma
Stablilize
Progress
• Aneurysm
• Aortic dissection
Regress
Intramural hematoma

IMH: predictors of a poor outcome
• Type A
• Aortic diameter >50 mm
• Wall thickness >11 mm
• Ulcer-like projections in the hematoma

• Type A >> open Sx
• Type B >> medication unless complications
• Type A IMH without complications
>> medication
Intramural hematoma

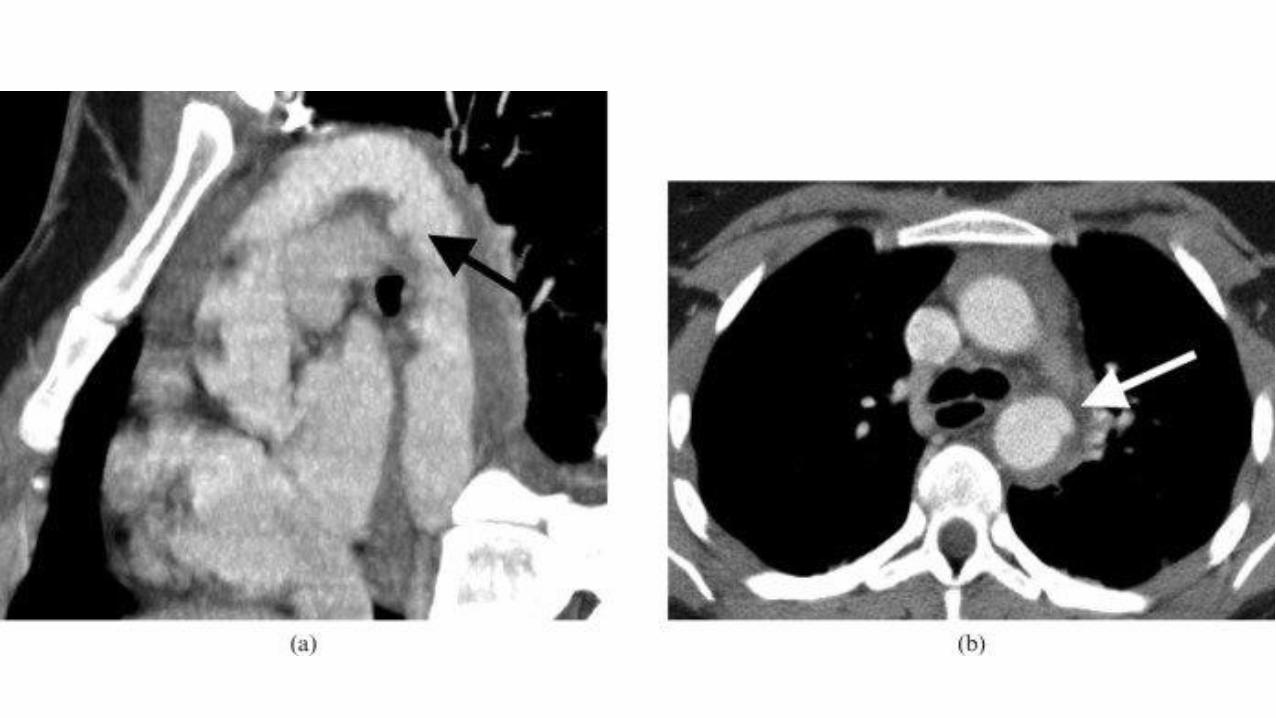
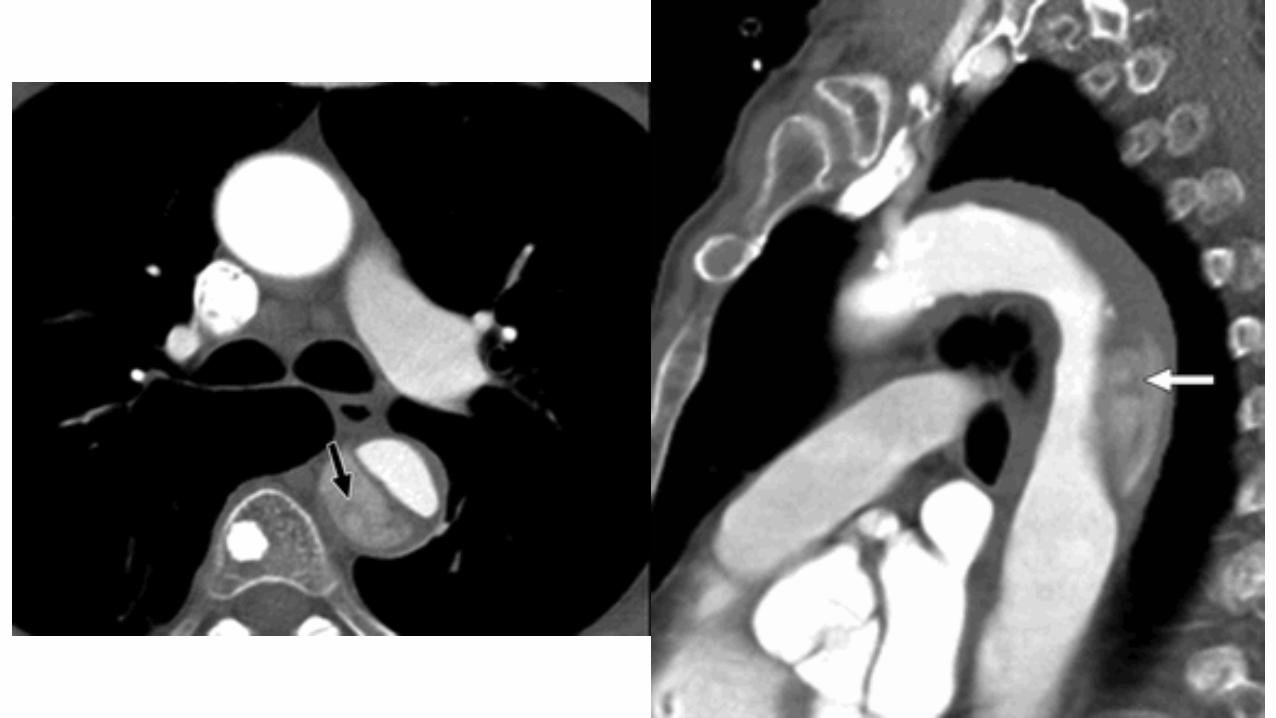
Penetrating atherosclerotic ulcer
• Progressive ulceration of an atheromatous plaque
• Ulcer -- most frequent in the descending aorta, penetrates the internal elastic lamina > intramural hematoma >> resolve/progress to aortic rupture/classic dissection
• Ulcerated aorta may be more prone to rupture than typical dissection
PAU-induced IMH Classic aortic IMH
limited in longitudinal extent more diffuse

• A focal contrast-filled outpouching through the aortic wall with limited intramural hematoma
• Unless the ulcer is complicated by classic dissection, an intimal flap is not seen
• Displacement of intimal calcification is common alike dissection
Penetrating atherosclerotic ulcer

http://radiopaedia.org/articles/penetrating-atherosclerotic-ulcer



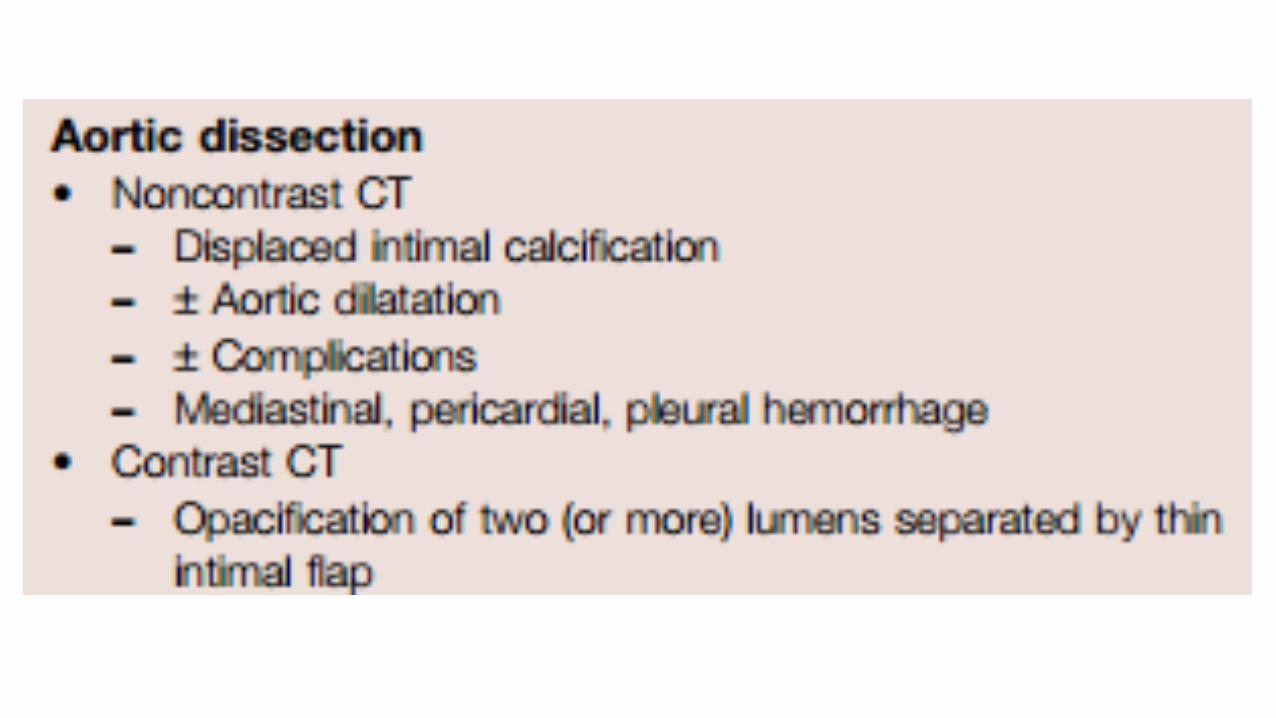
Disease NCCT CECT
Aortic dissection Medial displacement of intimal calcifications
Intimal flap แยก true and false
lumens; cobweb sign—residua of incompletely dissected media
Intramural hematoma High-attenuation crescentricthickening of the aortic wall
High attenuation of wall ไม่ชดั;
aortic wall thickening
Penetrating atherosclerotic ulcer
Can be seen only if complicated (accompanied by aortic dissection or intramural hematoma)
Localized ulceration penetrating through aortic intima into aortic wall
Acute nontraumatic aortic syndromes

Q & A
• Normal aorta and aortic variation• Aortic spindle, ductus bump, cervical aortic arch
• Aortic aneurysm• Atherosclerotic aneurysm
• Mycotic aneurysm
• Traumatic aortic injury: blunt aortic injury
• Acute nontraumatic aortic syndromes • Aortic dissection
• Intramural hematoma• Penetrating atherosclerotic ulcer

















