2016 Capital Area carcinoid Survivors (CACS) Lecture Neuroendocrine Cancer Therapy - Where are we in 2016? Edward M. Wolin, M.D. Director, Neuroendocrine Tumor Program Montefiore Einstein Center for Cancer Care New York, NY
Transcript
2016 Capital Area carcinoid Survivors (CACS) Lecture Neuroendocrine Cancer Therapy -
Where are we in 2016?
Edward M. Wolin, M.D. Director, Neuroendocrine Tumor Program
Montefiore Einstein Center for Cancer Care New York, NY
John Godfrey Saxe One of the most famous versions of the 19th century was the poem "The Blind Men and the Elephant" by John Godfrey Saxe (1816–1887).
And so these men of Hindustan Disputed loud and long, Each in his own opinion Exceeding stiff and strong, Though each was partly in the right And all were in the wrong.
"The Blind Men and the ElephantJohn Godfrey Saxe (1816–1887).
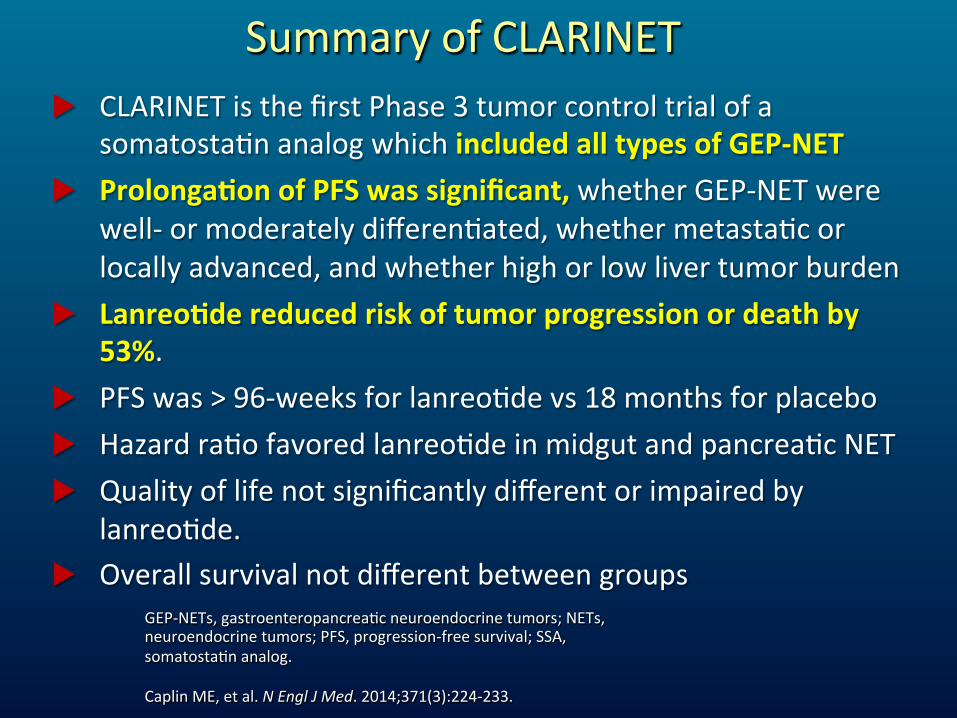
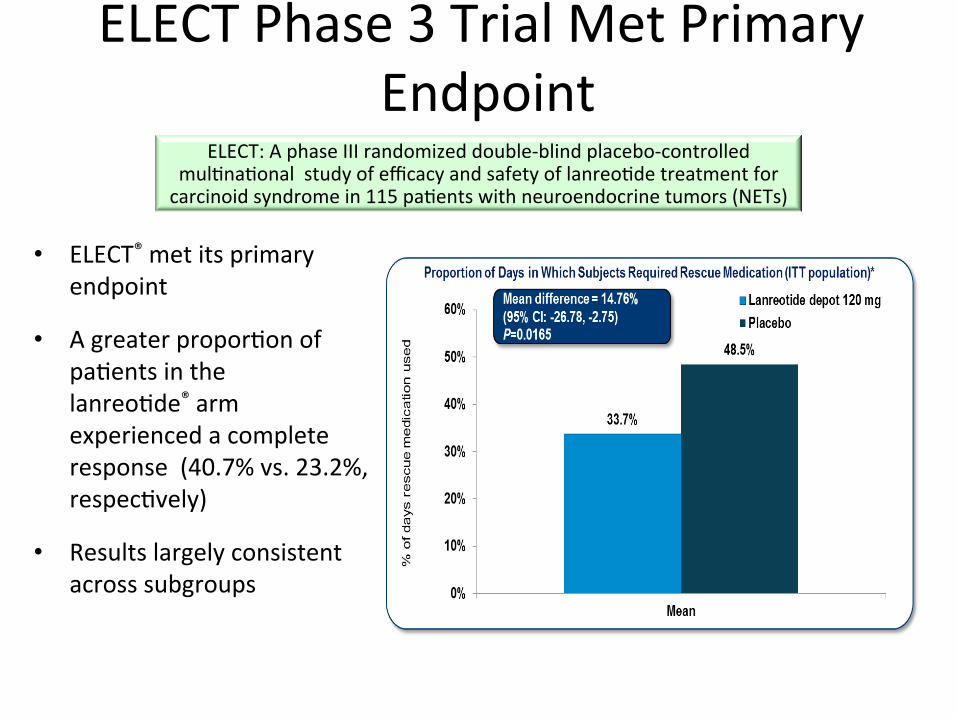
u CLARINETisthefirstPhase3tumorcontroltrialofasomatostaUnanalogwhichincludedalltypesofGEP-NET
u ProlongaDonofPFSwassignificant,whetherGEP-NETwerewell-ormoderatelydifferenUated,whethermetastaUcorlocallyadvanced,andwhetherhighorlowlivertumorburden
u LanreoDdereducedriskoftumorprogressionordeathby53%.
u PFSwas>96-weeksforlanreoUdevs18monthsforplacebou HazardraUofavoredlanreoUdeinmidgutandpancreaUcNETu Qualityoflifenotsignificantlydifferentorimpairedby
Kaplan-Meier median PFS Pasireotide: 11.8 months, 95% CI [11.0–not reached] Octreotide: 6.8 months, 95% CI [5.6–not reached] Hazard ratio = 0.46, 95% CI [0.20–0.98]
Total events = 38
26
P = 0.045 (log-rank test)
Wolin et. al., A multicenter, randomized, blinded, phase III study of pasireotide LAR versus octreotide LAR in patients with metastatic neuroendocrine tumors (NET) with disease-relatedsymptoms inadequately controlled by somatostatin analogs. J Clin Oncol 31, 2013 (suppl; abstr 4031)
Schematic Representation of a Drug for Imaging and Targeted Therapy
Molecular Address • Antibodies, minibodies,
Affibodies, SHALs, Aptamers
• Regulatory peptides and analogs thereof
• Amino Acids
Target • Antigens
(e.g. CD20, HER2)
• GPCRs • Transporters
Reporting Unit • 99mTc, 111In, 67Ga
• 64Cu, 68Ga • Gd3+
Cytotoxic Unit • 90Y, 177Lu, 213Bi • 105Rh, 67Cu, 186,188Re
Courtesy Helmut Mäcke (modified)
Targeted Molecular Imaging and Therapy The Key-Lock Principle
Lock Key 68Ga, 90Y, 177Lu
pharmacokineDc/biodistribuDonmodifier
ChelatorLinkerLigandTarget
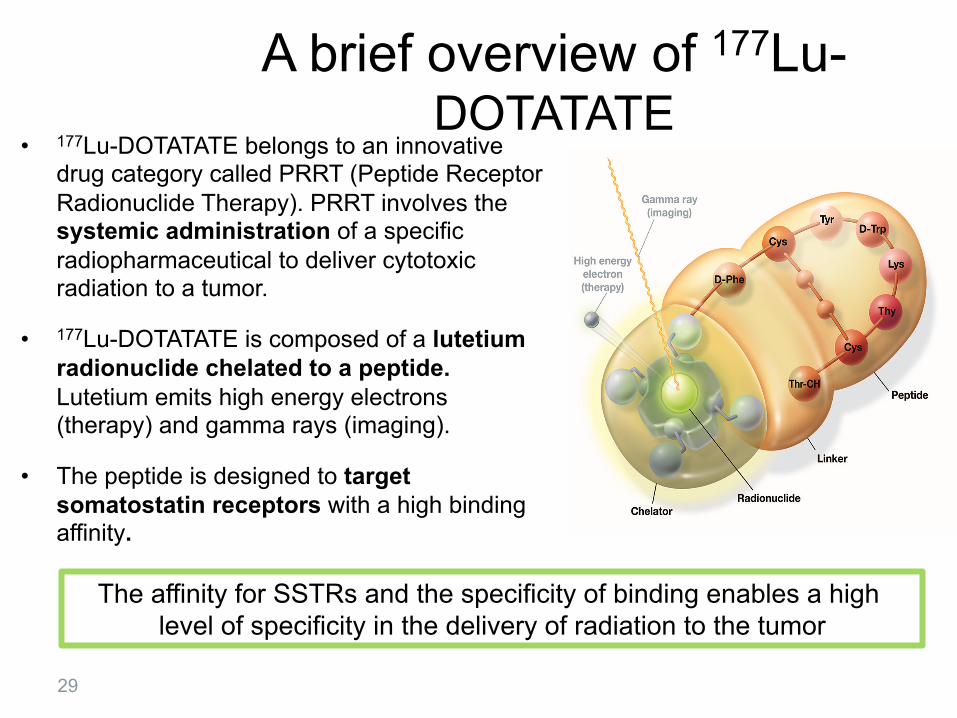
A brief overview of 177Lu-DOTATATE
• 177Lu-DOTATATE belongs to an innovative drug category called PRRT (Peptide Receptor Radionuclide Therapy). PRRT involves the systemic administration of a specific radiopharmaceutical to deliver cytotoxic radiation to a tumor.
• 177Lu-DOTATATE is composed of a lutetium radionuclide chelated to a peptide. Lutetium emits high energy electrons (therapy) and gamma rays (imaging).
• The peptide is designed to target somatostatin receptors with a high binding affinity.
The affinity for SSTRs and the specificity of binding enables a high level of specificity in the delivery of radiation to the tumor
29
Lutathera®Mechanism of Action
30
Intravenous injection
Concentration into neuroendocrine tumor (NET) sites
Lutathera binds to somatostatin receptors type 2 (sstr2) overexpressed by NETs
Lutathera is internalized in the NET cell
Lutathera delivers radiation within the cancer cell
Radiation induces DNA strand breaks causing tumor cell death
32 Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
Hazard Ratio [95% CI] 0.209 [0.129 – 0.338] p < 0.0001
N = 229 (ITT) Number of events: 90
• 177Lu-Dotatate: 23 • Oct 60 mg LAR:
67
All progressions centrally confirmed and independently reviewed for eligibility (SAP)
Octreotide LAR 60 mg Median PFS: 8.4 months
177Lu-Dotatate Median PFS: Not reached
Overall Survival (interim analysis)
33 Presentation Presidential Session II of the 18th ECCO – 40th ESMO – European Cancer Congress 2015, 27 September 2015, abstract 6LBA, Vienna
N = 229 (ITT) Number of deaths: 35
• 177Lu-Dotatate: 13 • Octreotide 60 mg LAR: 22
P < 0.0186
0.5
Inclusion Criteria Expanded Access
1. Presence of metastatic or locally advanced, inoperable (curative intent) midgut carcinoid tumor. 2. Ki-67 index < 20%. 3. Patients progressive on SSA (any dose) at the time of enrollment Recist NOT required) 4. Patients > 18 years of age. 5. Target lesions overexpressing somatostatin receptors according to an appropriate imaging method (e.g. 111In-pentetreotide (Octreoscan) imaging or 68Ga-DOTA0-Tyr3-Octreotate imaging) (Bodei et al., 2014).
Importance of 18F-FDG PET/CTThe role of 18F-FDG PET/CT in the assessment of response totherapy is limited, primarily because NENs are slow-growingtumors and glucose metabolism does not necessarily increasein slow-growing, well-differentiated tumors. In addition, nodefinitive therapy exists that influences the metabolism di-rectly enough to be assessed by 18F-FDG. It has been postu-lated that18F-FDG PET should be performed only if SSTRimaging is negative.56 The main use of 18F-FDG PET in diag-nosis of NEN depends on the grade of differentiation and/oraggressiveness of NEN and has been proposed for compre-hensive tumor assessment in intermediate- and high-gradetumors (Fig. 8).45,57 Intense metabolic activity, reflected on18F-FDG PET scans, can still be an important prognostic in-dicator, being related to an outgrowth of aggressive tumorclones, suggesting a poor prognosis. However, functional im-aging with both 68Ga-DOTATATE and 18F-FDG has shown toaddress different biological properties of the neuroendocrinetumor lesions in patients planned for PRRNT.57
In a preliminary study at Zentralklinik Bad Berka, we se-lected 25 subjects at random from a group of 505 patientswith metastasized NEN who were scheduled for treatmentwith PRRNT (138 lesions) and compared pre- and posttreat-ment images acquired using 68Ga-DOTANOC PET/CT (mo-lecular response), 18F-FDG PET/CT (metabolic response),
and contrast-enhanced CT (morphological response).58 A re-sponse index was calculated for each lesion from PET imagesbased on the pre- and posttreatment SUVmax. RECIST criteriawere applied to the contrast-enhanced CT data. All lesionswere categorized as partial responders, stable disease, or PD.No correlation was observed between any of the 3 modalities;for example, 68Ga-DOTANOC PET classified 70.6% of thelesions as partial responders, whereas FDG-PET put 43.8%into this category, and CT, just 17.6%. The sensitivity andspecificity of 68Ga-DOTANOC PET to predict response toradiopeptide therapy were calculated as 89% and 71%, re-spectively. 68Ga-DOTANOC PET/CT was found to be supe-rior to 18F-FDG PET/CT and morphological imaging for earlyand better prediction of response to PRRNT. Furthermore, amatching pattern between receptor expression and glucosemetabolism was observed to increase with the grade of NEN;therefore, in high-grade NENs, a concurrence between thechanges in glucose metabolism and SSTR expression, ie, on18F-FDG PET/CT and 68Ga-DOTANOC PET/CT, respec-tively, after PRRNT was noticed. Also, higher tumor remis-sion rate was correlated with a high baseline SUVmax on SSTRPET/CT. This finding is consistent with previous studies, andPRRNT was confirmed to be an effective therapy option forNEN patients expressing adequate densities of SSTRs on thetumors.21 In another recent study, 68Ga-DOTATATE PET/CT
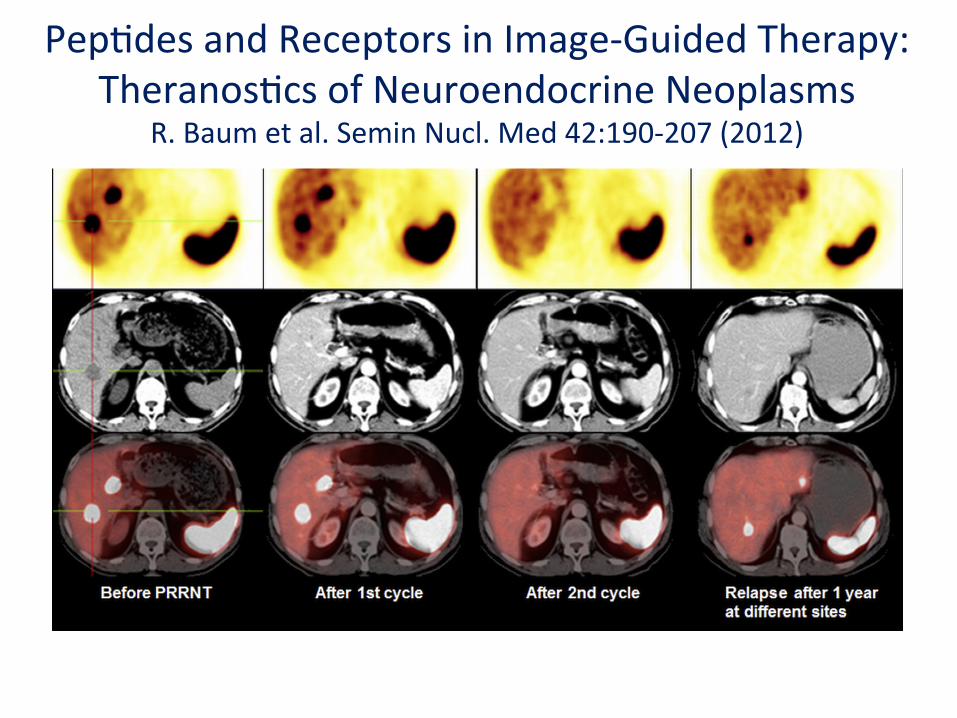
Figure 7 Molecular response as demonstrated by receptor PET/CT using the SMS analog 68Ga-DOTANOC in a patientwith liver metastases of a NEN before and after the first and second cycle of peptide receptor radionuclide therapy(PRRNT); relapse in the liver (after complete remission as shown by CT and PET) is first detected by SMS-receptorimaging (molecular response precedes morphology).
Peptides and receptors in image-guided therapy 199
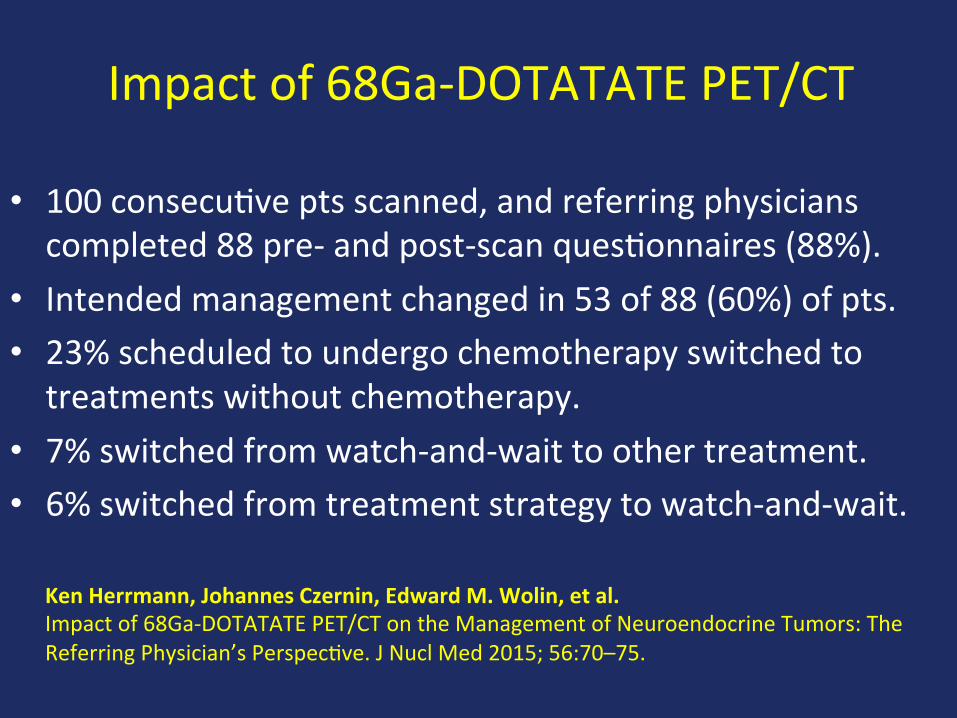
AddedValueof68Ga-DOTATATEPET/CT
Mojtahedi A, Am J Nucl Med Mol Imaging 2014;4(5):426-434
Patients with advanced pNET, N = 410 Stratified by: • WHO PS • Prior
Chemotherapy
Crossover
1:1
Concurrent somatostatin analogs allowed
RANDOMI ZE
Primary endpoint: • PFS (RECIST)
Secondary endpoints: • Response, OS, biomarkers, safety, and PK
Randomization August 2007 - May 2009
Phase III Double Blind Placebo Controlled Trial
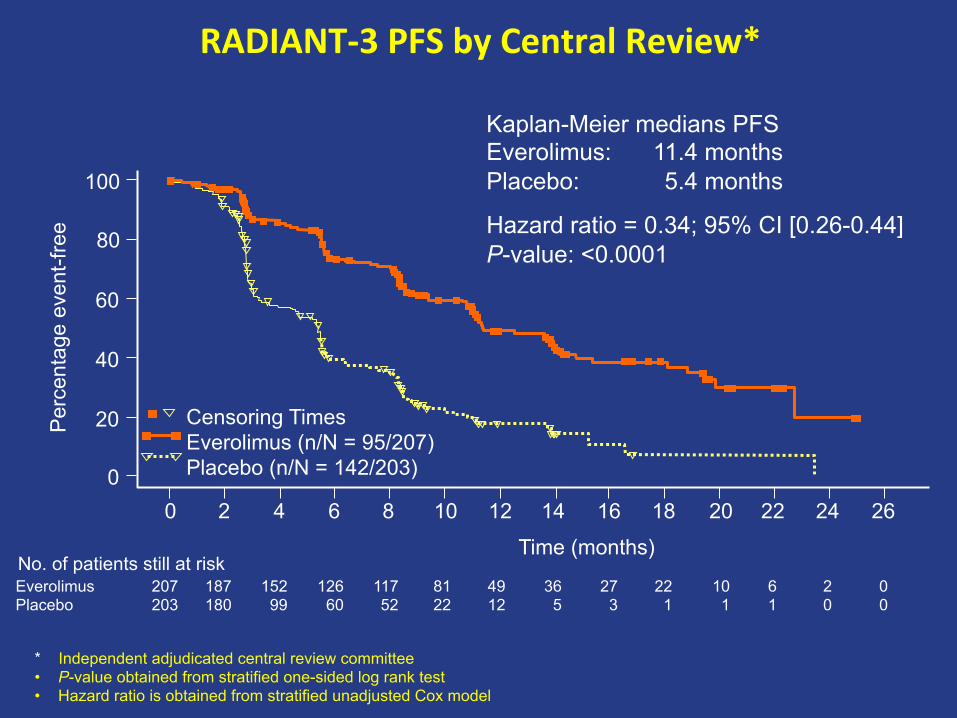
RADIANT-3PFSbyCentralReview*
* Independent adjudicated central review committee • P-value obtained from stratified one-sided log rank test • Hazard ratio is obtained from stratified unadjusted Cox model
Hazard ratio = 0.34; 95% CI [0.26-0.44] P-value: <0.0001
No. of patients still at risk Everolimus Placebo
207 203
187 180
152 99
126 60
117 52
81 22
49 12
36 5
27 3
22 1
10 1
6 1
2 0
0 0
Time (months)
100
80
Per
cent
age
even
t-fre
e
Censoring Times Everolimus (n/N = 95/207) Placebo (n/N = 142/203)
60
40
20
0 0 2 4 6 8 10 12 14 16 18 20 22 24 26
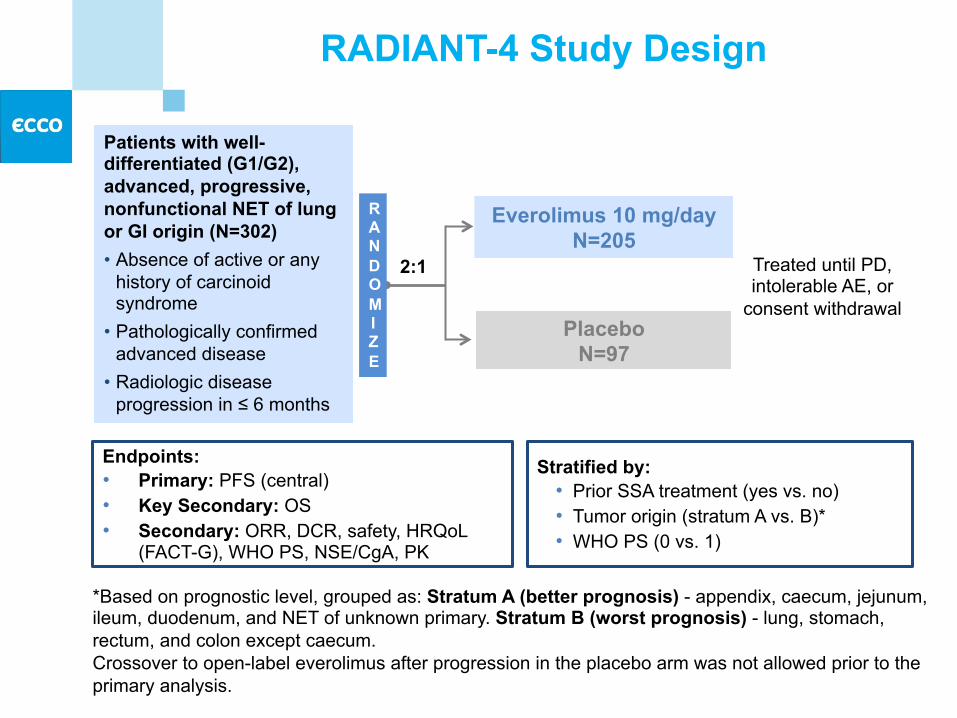
RADIANT-4 Study Design
*Based on prognostic level, grouped as: Stratum A (better prognosis) - appendix, caecum, jejunum, ileum, duodenum, and NET of unknown primary. Stratum B (worst prognosis) - lung, stomach, rectum, and colon except caecum. Crossover to open-label everolimus after progression in the placebo arm was not allowed prior to the primary analysis.
Patients with well-differentiated (G1/G2), advanced, progressive, nonfunctional NET of lung or GI origin (N=302) • Absence of active or any
history of carcinoid syndrome
• Pathologically confirmed advanced disease
• Radiologic disease progression in ≤ 6 months
2:1
RANDOMI ZE
Placebo N=97
Stratified by: • Prior SSA treatment (yes vs. no) • Tumor origin (stratum A vs. B)* • WHO PS (0 vs. 1)
RADIANT-4 Primary Endpoint: PFS by Central Radiology Review
52% reduction in the relative risk of progression or death with everolimus vs placebo
HR = 0.48 (95% CI, 0.35-0.67); P < 0.00001
P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model. CI, confidence interval; HR, hazard ratio.