15
Developing and Delivering a Liaison Psychiatry Service Stella Morris Consultant Liaison Psychiatrist Department of Psychological Medicine Hull Royal Infirmary [email protected]
| Date post: | 16-Jul-2015 |
| Category: |
Healthcare |
| Upload: | daniel-rankine |
| View: | 730 times |
| Download: | 1 times |

Developing and Delivering a Liaison Psychiatry Service
Stella MorrisConsultant Liaison PsychiatristDepartment of Psychological MedicineHull Royal Infirmary
Outline
• Hull service development 1997 – 2015
• Current clinical model
• Priorities for the Hull Service in 2015
• How liaison services can help with crisis care
Acute Hospitals (1997)Royal Hull Hospitals Trust Beds
Hull Royal Infirmary (A&E) 721
Hull Maternity Hospital 163
Kingston General Hospital 120
Princess Royal Hospital 166
East Yorkshire Acute Trust
Castle Hill Hospital 529
Regional Services to 1.2m for renal, oncology and neurosciences
Mental Health input via sector teams and 1 nurse in A&E (on secondment) plus 2 social workers (funded by social services)

Initial Team and Service Provision (1997)Consultant - part-time
Mental health nurse - full-time
Secretary - part-time
Referrals - Hull Royal Infirmary only
No GP referrals
16 - 65 years
A&E - clinical input via mental health nurse

Developments - 12001 - Cognitive Behavioural Therapist
(Funding Acute Trust - waiting list initiative money)
2003/4 - Resources withdrawn from A&E / Self Harm Service
(Social Services reorganisation)
- Directly targeted PCT commissioners
- A&E / Self Harm Service re-established
Monday – Friday 9am to 8pm
(Funding Hull and East Riding PCTs)
2004 - Development of Chronic Fatigue Syndrome Service
(Centrally Funded)

Developments - 2
2007 - Business case for Specialist Community Perinatal Mental Health Service (Stimulated by NICE guidelines and recognition of clinical need locally)
2007/8 - A&E / Self-Harm Service
7 days a week, 9am – 8pm
Ageless
(Funding from Hull and East Riding PCTs)

Developments - 32010 – Investment of 1.2M from Hull PCT
To establish: Older Peoples Liaison Service
Learning Disability Service
Specialist Community Perinatal Mental Health Service
To extend: Existing Liaison Services

Acute Hospitals (2015)
Hull and East Yorkshire Hospitals Trust
BedsHull Royal Infirmary (A&E) 739(plus 93 Maternity Beds, 40 Dialysis Stations>120,000 attendances/ year in A&E)
Castle Hill Hospital 658
Regional Services to 1.5 m for renal, oncology, neurosciencesand trauma
Commissioners – Hull and East Riding CCGs

Clinical Model for the Department of Psychological Medicine 2015
Outpatient Work(referrals from acute services)
Medically Unexplained Symptoms
Neuropsychiatry
Physical illness with co-morbid mental
illness (diabetes / renal /cystic
fibrosis)
Bariatric surgery
Chronic pain
Hospital Mental Health Team (HMHT)via SPOC
Operates 7/7- 8 to 10pm All urgent referrals from A&E and wards at HRI & CHH
16+ (except self-harm - ageless )HMHT includes older peoples team and LD
Outpatient work(referrals from primary care)
Chronic Fatigue Syndrome Service
Perinatal Service
Huntington’s Disease Service

Liaison Service in Hull 2015
• Total staff of 50 (clinical and admin staff)
• Annual budget ~ £ 2M
• 4317 referrals in 2014 (5% increase from 2013)
(3236 seen by HMHT)

Success Factors for the Service
• Growth period mainly 1997 – 2010
Labour government, Initiatives, NICE Guidelines, National drivers
• Developed good relationships with commissioners
• Consistency and persistence
• Clinical champions
• The Hull Factor
• A little bit of luck!
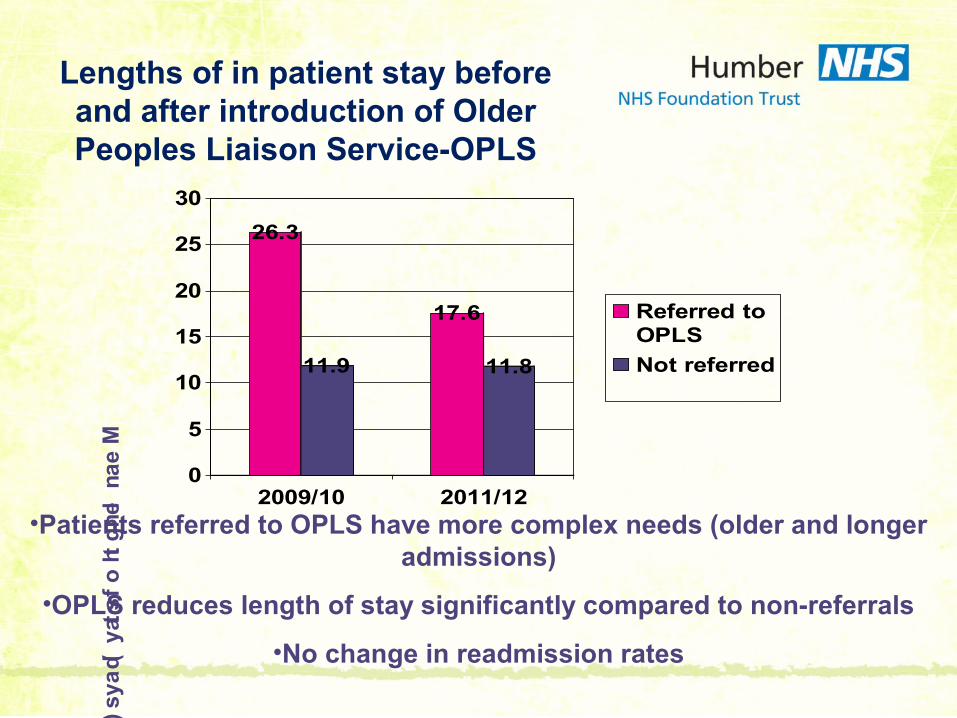
Lengths of in patient stay before and after introduction of Older Peoples Liaison Service-OPLS
26.3
11.9
17.6
11.8
0
5
10
15
20
25
30
2009/10 2011/12
Referred toOPLS
Not referred
Me
an
len
gth
of s
tay (d
ays
)
•Patients referred to OPLS have more complex needs (older and longer admissions)
•OPLS reduces length of stay significantly compared to non-referrals
•No change in readmission rates

The Future • ‘5 year Forward View’ - prevention, partnership working,
breaking down barriers so that care is delivered locally, multi-specialty community provision
• Liaison services have a unique opportunity to support commissioners in helping address the complex physical and mental health needs of its communities. Our challenge is to be part of the discussion that shapes the future

Hull Service Priorities for 2015/6
• 24 hour service to A&E
• Diabetes – proposing an integrated model of care based on the 3DFD model
• Developing a model for the management of medically unexplained symptoms in primary care

Liaison Services, Crisis Care and 5 year forward
• Rapid response for mental health patients within the acute hospital – reduce waits in A&E, reduce lengths of stay for in-patients
• Training – management of delirium, acute behavioural disturbance, mental capacity assessments
• Reduce admissions and improve clinical care – primary care liaison for chronic disease management/medically unexplained symptoms

















