Early-Onset Neutropenia inSmall-for-Gestational-Age InfantsRobert D. Christensen, MDa,b,c, Bradley A. Yoder, MDa,c, Vickie L. Baer, RNa, Gregory L. Snow, PhDd, Allison Butler, MSd
abstractBACKGROUND: Early neutropenia is more common in small for gestational age (SGA) neonates (birthweight ,10th percentile) than in appropriately grown neonates. However, several aspects of thisvariety of neutropenia are unknown, including the duration, kinetic mechanism, and outcomes.
METHODS:Using 10 years of multihospital records, we studied SGA neonates who, during the firstweek after birth, had neutrophil counts ,1000/mL.
RESULTS: This degree of neutropenia was more common in SGA neonates (6%, 207/3650) than innon-SGA matched controls (1%, 46/3650; P , .001). Neutrophil counts stayed below the lowerreference interval for 7 days. Ratios of immature to total neutrophils were within the referenceinterval, suggesting reduced neutrophil production, not accelerated neutrophil use or destruction.Increased nucleated red cells at birth correlated with decreased neutrophils (P, .001). Neutropeniawas not independently associated with maternal hypertensive disorders, over and above the effectof SGA. Of 201 neutropenic SGA neonates, 129 (64%) also had thrombocytopenia. Sixteen percent ofneutropenic neonates were treated with recombinant granulocyte colony-stimulating factor (rG-CSF) or intravenous immunoglobulin (IVIG), with no reduction in late-onset sepsis or necrotizingenterocolitis (NEC). Regression analysis showed that neutropenia (but not thrombocytopenia in theabsence of neutropenia) was independently associated with increased odds of developingnecrotizing enterocolitis (odds ratio 4.01, 90% confidence interval 2.08 to 7.35, P , .001).
CONCLUSIONS: Neutropenia of SGA is a condition of 1-week duration. It is more closely associatedwith SGA than maternal hypertension (likely owing to neutrophil hypoproduction associatedwith intrauterine hypoxia), often accompanied by thrombocytopenia, not obviously improvedby rG-CSF or IVIG, and associated with an increased risk for NEC.
WHAT’S KNOWN ON THIS SUBJECT: Small forgestational age neonates (weight ,10thpercentile) are at risk for neutropenia during thefirst days after birth. However, the duration,responsible mechanism, and outcomes of thisvariety of neonatal neutropenia are not preciselyknown.
WHAT THIS STUDY ADDS: Six percent of small forgestational age neonates had neutrophils,1000/mL, with an average neutropenia durationof 7 days. Neutropenia was more closely linkedwith small for gestational age status thanmaternal hypertension. This neutropenia isassociated with elevated nucleated red blood cellcount and increased odds of necrotizingenterocolitis.
aWomen and Newborn’s Clinical Program, Intermountain Healthcare, bDivision of Hematology/Oncology, andcDivision of Neonatology, Department of Pediatrics, University of Utah School of Medicine and Primary Children’sHospital, Salt Lake City, Utah; and dStatistical Data Center, LDS Hospital, Salt Lake City, Utah
Drs Christensen and Yoder and Ms Baer conceptualized and designed the study; Drs Christensenand Yoder drafted the initial manuscript; Ms Baer carried out the initial data assembly analyses anddisplay; Dr Snow and Ms Butler carried out the statistical analysis; Ms Baer, Dr Snow, and Ms Butlerreviewed and revised the manuscript; and all authors approved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2015-1638
DOI: 10.1542/peds.2015-1638
Accepted for publication Aug 5, 2015
Address correspondence to Robert D. Christensen, MD, University of Utah Department of Pediatrics,295 Chipeta Way, Salt Lake City, UT 84108. E-mail: [email protected]
Neonates who are born small forgestational age (SGA) (,10thpercentile birth weight for a referencepopulation) are at risk for havingneutropenia in the first days afterbirth.1–6 Various definitions havebeen used for neonatal neutropenia,leading to diversity in the reportedincidence of neutropenia among SGAneonates. Definitions have includedan absolute neutrophil count ,5thpercentile reference range6 or a countof ,1500/mL or ,1000/mL.7
Surely some cases of neutropeniaamong SGA infants, regardless of thedefinition used for neutropenia, arethe result of bacterial sepsis8,9 orneonatal alloimmune neutropenia,10
but most neutropenic SGA neonateshave a different variety ofneutropenia that is sometimestermed “neutropenia of SGA” orneutropenia of infants of motherswith hypertensive disorders.1–6,11–13
Many aspects of that variety ofneonatal neutropenia remain unclear.
As a step toward enhancing theknowledge base of neutropenia ofSGA, we conducted a retrospectiveanalysis of neonates hospitalized inour health care system during the past10 years. This period was selected tocoincide with improvements in ourelectronic data system dating to 2003.Our study aims were (1) to identify allSGA neonates who had a bloodneutrophil concentration ,1000/mLduring the first week after birth (astringent definition for neutropenia)and, within that group, to identify andexclude from further analysis thosewith other explanations forneutropenia such as early-onsetsepsis, alloimmune neutropenia, orany other recognized form ofneutropenia, defining the residualgroup as having the exclusionarydiagnosis of the neutropenia of SGA;(2) to determine the duration of thisvariety of neutropenia; (3) to assessthe mechanism causing this variety ofneutropenia; and (4) to evaluate theoutcomes of neonates with thiscondition.
METHODS
Patient Information
Data were collected retrospectively asdeidentified limited data sets fromarchived Intermountain Healthcarerecords. Intermountain Healthcareis a not-for-profit healthcare systemthat owns and operates 19 hospitalswith labor and delivery units inUtah and Idaho. The informationcollected was limited to theinformation in this report. Patientrecords were accessed if the neonatehad a date of birth from January 1,2004, through December 31, 2013.The Intermountain HealthcareInstitutional Review Board approvedthis deidentified data–only study asnot requiring the consent ofindividual subjects.
Blood Cell Counts
Leukocyte counts, neutrophil counts,and ratios of immature to totalneutrophils (I/T ratios) weredetermined in all hospitals withthe Beckman Coulter LH750Hematology Analyzer (Fullerton,CA) from 2004 through mid-2012.After mid-2012, blood cell countswere determined using Sysmexcounters (Sysmex America,Lincolnshire, IL). It is standardoperating procedure in allIntermountain Healthcare ClinicalLaboratories to include a manualdifferential cell count on all completeblood counts (CBCs) of infants in thefirst 90 days after birth. All bloodtests were performed in accordancewith Intermountain HealthcareLaboratory Services standardoperating procedures. Leukocytedifferential counts were performed byenumeration by certified medicaltechnologists on Wright-stainedblood smears, counting a minimum of100 nucleated cells per test. Thereference intervals for CBCparameters are those we publishedfrom Intermountain Healthcaredatabases.14
Gestational age was determined byobstetrical assignment unless this
was changed by the neonatologist onthe basis of gestational ageassessment (physical examinationand neurologic-neurodevelopmentalfindings). Neonates were classified asSGA if their weight at birth was,10th percentile for gestational age,using normative values from ourIntermountain Healthcarepopulation.15 Severity of SGA wasclassified according to 3 categories:severe, less than first percentile;moderate, first to fifth percentile; andmild, sixth to 10th percentile. Cases ofmaternal hypertension wereidentified from case-mix recordsusing International Classification ofDiseases, Revision 9 definitions 6425(severe preeclampsia), 6426(eclampsia), or 6427 (preeclampsiaor eclampsia superimposed onexisting hypertension). We did notinclude women with the InternationalClassification of Diseases, Revision 9code 6424 (mild or nonspecific),because in our previous studies wefound that this definition includestransient, resolved, or mildhypertension and that eliminatingthis code reduces heterogeneity.16 Nospecific guidelines for administeringintravenous immunoglobulin (IVIG)and recombinant granulocyte colony-stimulating factor (rG-CSF) weresanctioned by the IntermountainHealthcare NICUs during this period,but general guidelines wereavailable.7 Early thrombocytopeniawas defined as $2 platelet counts,150 000/mL during the first weekafter birth.16
SGA neonates were matched 1:1 withneonates from the same hospitalsborn during the same period of timewho were not SGA. Matching wasperformed on the basis of gestationalage (61 week) and birth month (61month). “Early neutropenia” wasdefined as an absolute neutrophilcount ,1000 neutrophils/mL duringthe first week after birth. Patientswhose data would otherwise qualifyfor inclusion in the neutropenia ofSGA group were excluded if they wererecognized to have another variety of
e1260 CHRISTENSEN et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from
neutropenia, such as early-onsetsepsis or immune-mediatedneutropenia.
A diagnosis of necrotizingenterocolitis (NEC) was recorded ifit qualified as Bell stage $2.17
Spontaneous intestinal perforationwas not included if this entity wasrecognized as the cause of thebowel dysfunction.18 Late-onsetbacterial sepsis (LOS) was recordedif, after day of life 3, $1 bloodcultures were positive in concert withclinical signs interpreted by theattending clinician as clinical sepsisand entered into the clinical record asa case of late-onset culture-positivesepsis.19
Data Collection and StatisticalAnalysis
The program used for data collectionwas a modified subsystem of ClinicalWorkstation (3M, Minneapolis, MN);3M approved the structure anddefinitions of all data points for usewithin the program. Data weremanaged and accessed by authorizeddata analysts. Means and SDs wereused to express values in groups thatwere normally distributed, andmedians and interquartile ranges toexpress values in groups that werenot. Differences in categoricalvariables were assessed by using theFisher exact test or x2 test fornormally distributed data and theTukey biweight estimator for groupsthat were not. Statistical analysis usedStatit (Midas, Tucson, AZ) or the RFoundation package (StatisticalComputing, Vienna, Austria). Themixed-effects model used NIME,version 3.1-105, also from the Rpackage. Statistical significance wasset as P , .05.
RESULTS
Severity and Duration of Neutropenia
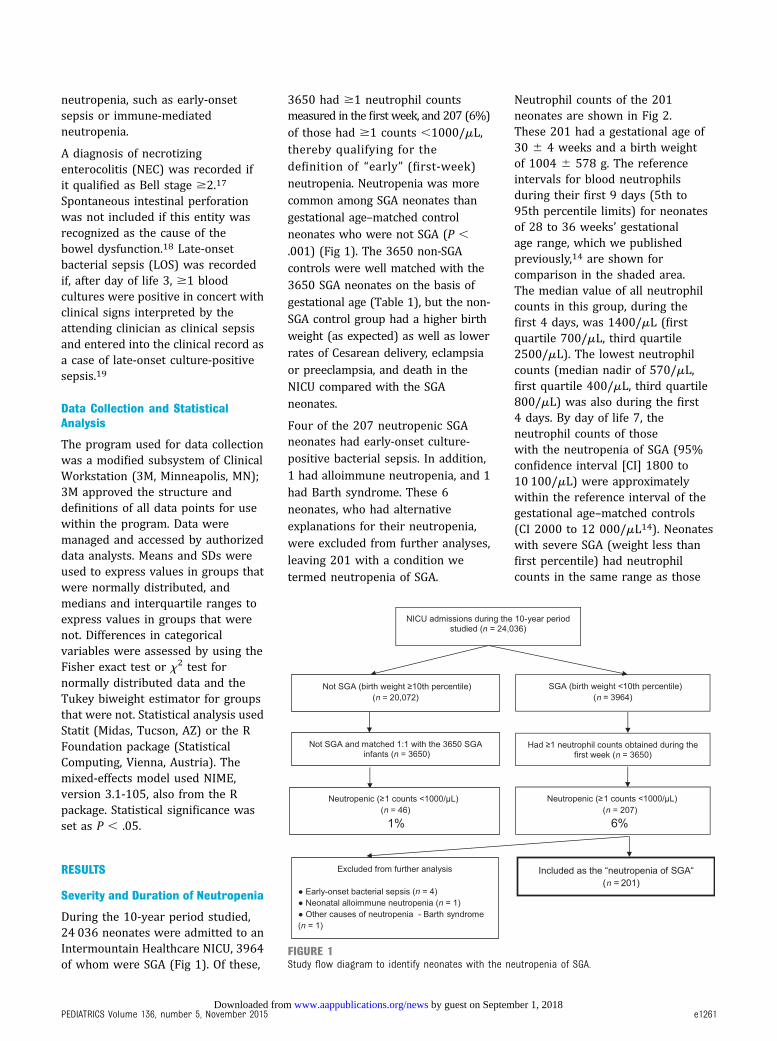
During the 10-year period studied,24 036 neonates were admitted to anIntermountain Healthcare NICU, 3964of whom were SGA (Fig 1). Of these,
3650 had $1 neutrophil countsmeasured in the first week, and 207 (6%)of those had $1 counts ,1000/mL,thereby qualifying for thedefinition of “early” (first-week)neutropenia. Neutropenia was morecommon among SGA neonates thangestational age–matched controlneonates who were not SGA (P ,
.001) (Fig 1). The 3650 non-SGAcontrols were well matched with the3650 SGA neonates on the basis ofgestational age (Table 1), but the non-SGA control group had a higher birthweight (as expected) as well as lowerrates of Cesarean delivery, eclampsiaor preeclampsia, and death in theNICU compared with the SGAneonates.
Four of the 207 neutropenic SGAneonates had early-onset culture-positive bacterial sepsis. In addition,1 had alloimmune neutropenia, and 1had Barth syndrome. These 6neonates, who had alternativeexplanations for their neutropenia,were excluded from further analyses,leaving 201 with a condition wetermed neutropenia of SGA.
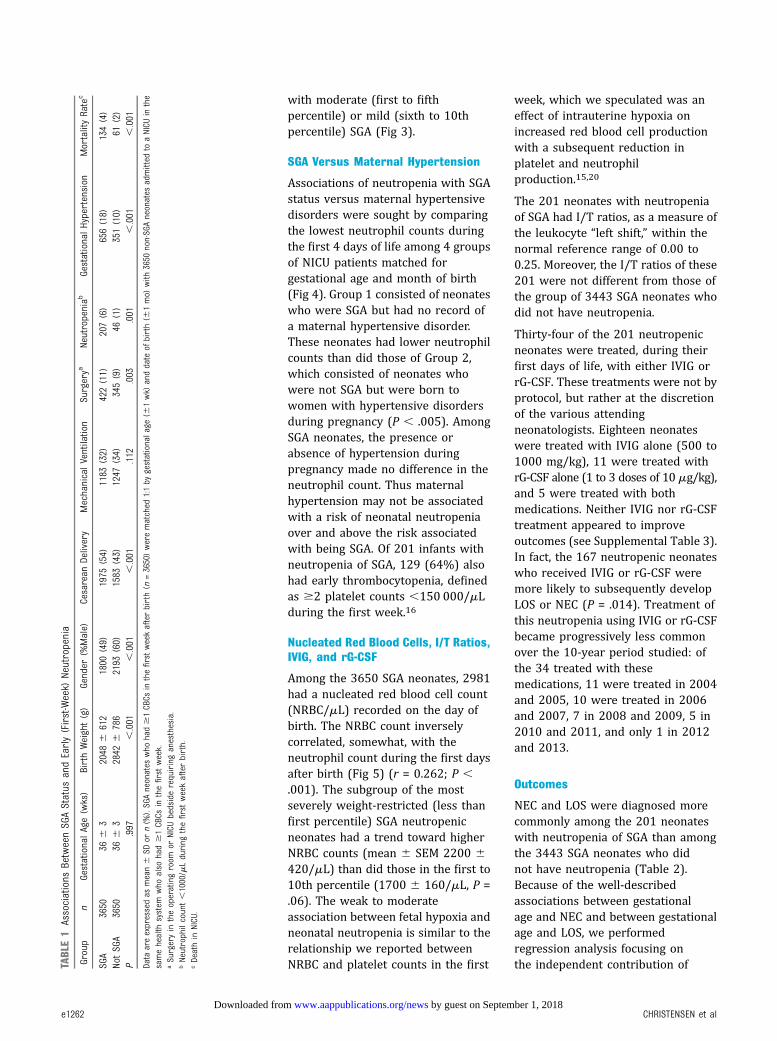
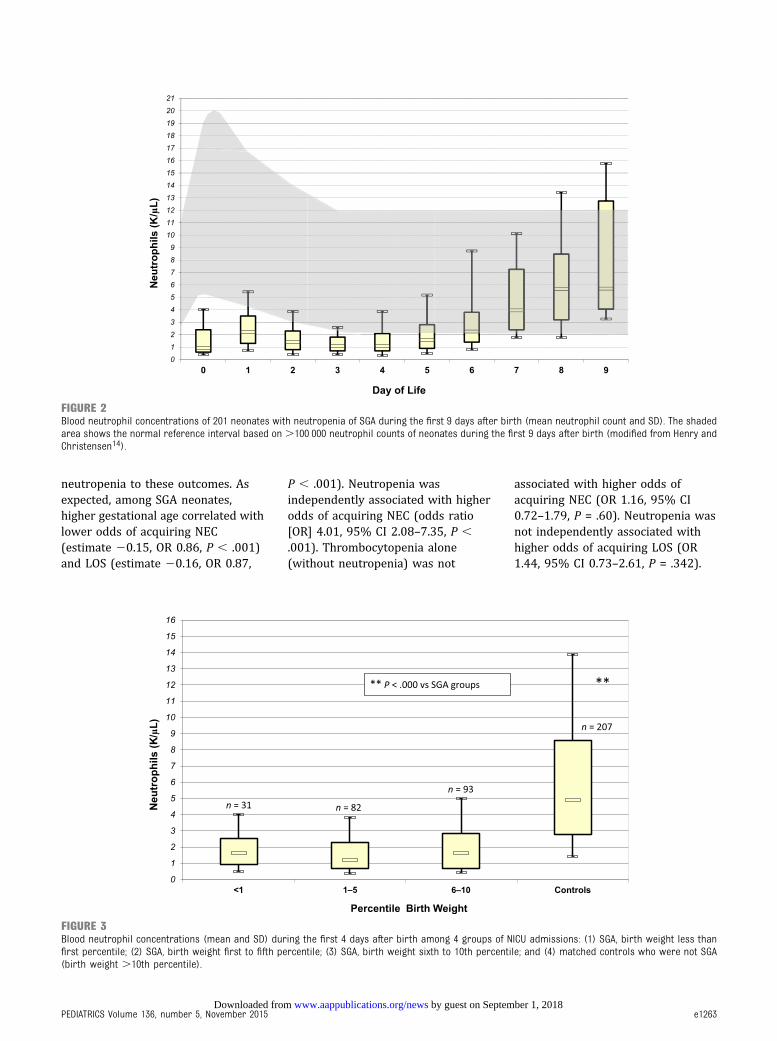
Neutrophil counts of the 201neonates are shown in Fig 2.These 201 had a gestational age of30 6 4 weeks and a birth weightof 1004 6 578 g. The referenceintervals for blood neutrophilsduring their first 9 days (5th to95th percentile limits) for neonatesof 28 to 36 weeks’ gestationalage range, which we publishedpreviously,14 are shown forcomparison in the shaded area.The median value of all neutrophilcounts in this group, during thefirst 4 days, was 1400/mL (firstquartile 700/mL, third quartile2500/mL). The lowest neutrophilcounts (median nadir of 570/mL,first quartile 400/mL, third quartile800/mL) was also during the first4 days. By day of life 7, theneutrophil counts of thosewith the neutropenia of SGA (95%confidence interval [CI] 1800 to10 100/mL) were approximatelywithin the reference interval of thegestational age–matched controls(CI 2000 to 12 000/mL14). Neonateswith severe SGA (weight less thanfirst percentile) had neutrophilcounts in the same range as those
FIGURE 1Study flow diagram to identify neonates with the neutropenia of SGA.
PEDIATRICS Volume 136, number 5, November 2015 e1261 by guest on September 1, 2018www.aappublications.org/newsDownloaded from
with moderate (first to fifthpercentile) or mild (sixth to 10thpercentile) SGA (Fig 3).
SGA Versus Maternal Hypertension
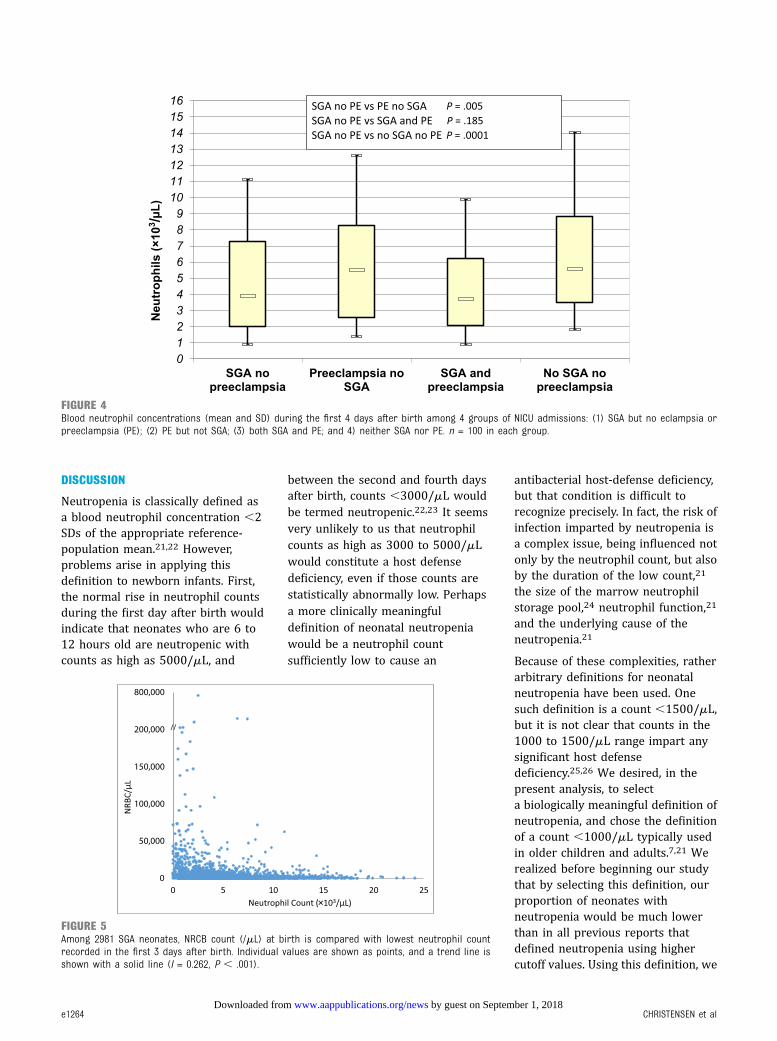
Associations of neutropenia with SGAstatus versus maternal hypertensivedisorders were sought by comparingthe lowest neutrophil counts duringthe first 4 days of life among 4 groupsof NICU patients matched forgestational age and month of birth(Fig 4). Group 1 consisted of neonateswho were SGA but had no record ofa maternal hypertensive disorder.These neonates had lower neutrophilcounts than did those of Group 2,which consisted of neonates whowere not SGA but were born towomen with hypertensive disordersduring pregnancy (P , .005). AmongSGA neonates, the presence orabsence of hypertension duringpregnancy made no difference in theneutrophil count. Thus maternalhypertension may not be associatedwith a risk of neonatal neutropeniaover and above the risk associatedwith being SGA. Of 201 infants withneutropenia of SGA, 129 (64%) alsohad early thrombocytopenia, definedas $2 platelet counts ,150 000/mLduring the first week.16
Nucleated Red Blood Cells, I/T Ratios,IVIG, and rG-CSF
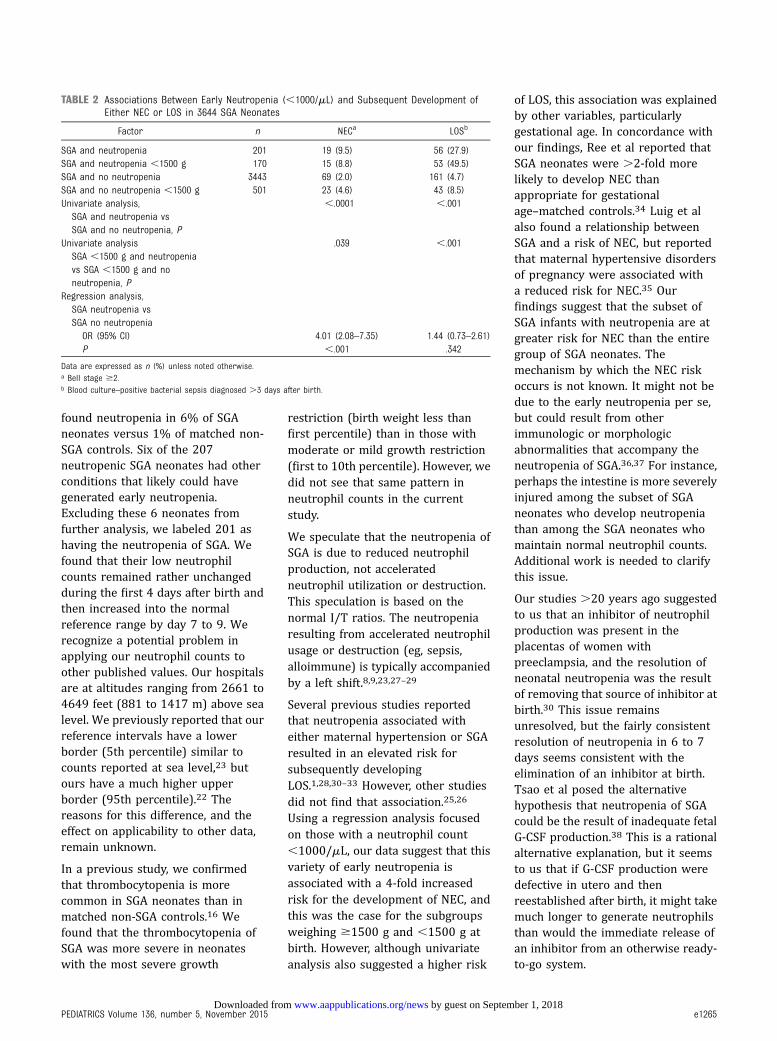
Among the 3650 SGA neonates, 2981had a nucleated red blood cell count(NRBC/mL) recorded on the day ofbirth. The NRBC count inverselycorrelated, somewhat, with theneutrophil count during the first daysafter birth (Fig 5) (r = 0.262; P ,.001). The subgroup of the mostseverely weight-restricted (less thanfirst percentile) SGA neutropenicneonates had a trend toward higherNRBC counts (mean 6 SEM 2200 6420/mL) than did those in the first to10th percentile (1700 6 160/mL, P =.06). The weak to moderateassociation between fetal hypoxia andneonatal neutropenia is similar to therelationship we reported betweenNRBC and platelet counts in the first
week, which we speculated was aneffect of intrauterine hypoxia onincreased red blood cell productionwith a subsequent reduction inplatelet and neutrophilproduction.15,20
The 201 neonates with neutropeniaof SGA had I/T ratios, as a measure ofthe leukocyte “left shift,” within thenormal reference range of 0.00 to0.25. Moreover, the I/T ratios of these201 were not different from those ofthe group of 3443 SGA neonates whodid not have neutropenia.
Thirty-four of the 201 neutropenicneonates were treated, during theirfirst days of life, with either IVIG orrG-CSF. These treatments were not byprotocol, but rather at the discretionof the various attendingneonatologists. Eighteen neonateswere treated with IVIG alone (500 to1000 mg/kg), 11 were treated withrG-CSF alone (1 to 3 doses of 10 mg/kg),and 5 were treated with bothmedications. Neither IVIG nor rG-CSFtreatment appeared to improveoutcomes (see Supplemental Table 3).In fact, the 167 neutropenic neonateswho received IVIG or rG-CSF weremore likely to subsequently developLOS or NEC (P = .014). Treatment ofthis neutropenia using IVIG or rG-CSFbecame progressively less commonover the 10-year period studied: ofthe 34 treated with thesemedications, 11 were treated in 2004and 2005, 10 were treated in 2006and 2007, 7 in 2008 and 2009, 5 in2010 and 2011, and only 1 in 2012and 2013.
Outcomes
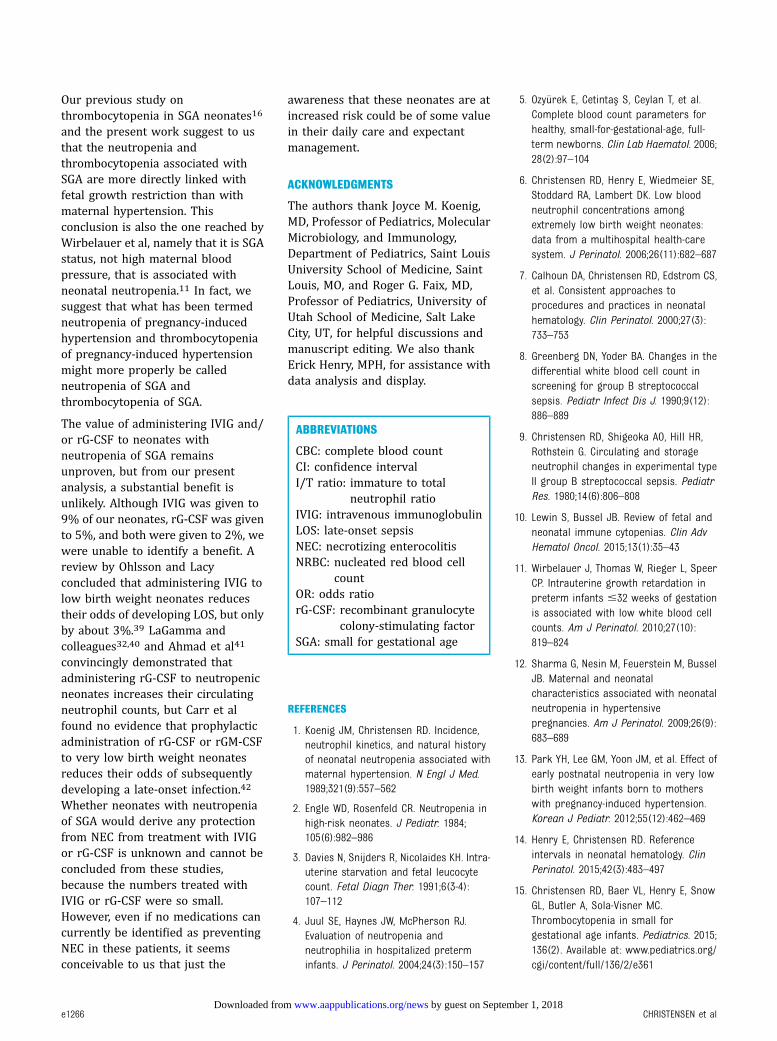
NEC and LOS were diagnosed morecommonly among the 201 neonateswith neutropenia of SGA than amongthe 3443 SGA neonates who didnot have neutropenia (Table 2).Because of the well-describedassociations between gestationalage and NEC and between gestationalage and LOS, we performedregression analysis focusing onthe independent contribution ofTA
BLE1
Associations
BetweenSGAStatus
andEarly(First-Week)
Neutropenia
Group
nGestationalAge(wks)
BirthWeight(g)
Gender
(%Male)
Cesarean
Delivery
MechanicalVentilation
Surgerya
Neutropeniab
GestationalHypertension
MortalityRatec
SGA
3650
366
32048
6612
1800
(49)
1975
(54)
1183
(32)
422(11)
207(6)
656(18)
134(4)
NotSGA
3650
366
32842
6786
2193
(60)
1583
(43)
1247
(34)
345(9)
46(1)
351(10)
61(2)
P.997
,.001
,.001
,.001
.112
.003
.001
,.001
,.001
Data
areexpressedas
mean6
SDor
n(%
).SGAneonates
who
had$1CBCs
inthefirstweekafterbirth(n
=3650)werematched
1:1by
gestationalage
(61wk)
anddate
ofbirth(6
1mo)
with
3650
non-SGAneonates
admitted
toaNICU
inthe
samehealth
system
who
also
had$1CBCs
inthefirstweek.
aSurgeryin
theoperatingroom
orNICU
bedsiderequiringanesthesia.
bNeutrophilcount,1000/mLduring
thefirstweekafterbirth.
cDeathin
NICU.
e1262 CHRISTENSEN et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from
neutropenia to these outcomes. Asexpected, among SGA neonates,higher gestational age correlated withlower odds of acquiring NEC(estimate 20.15, OR 0.86, P , .001)and LOS (estimate 20.16, OR 0.87,
P , .001). Neutropenia wasindependently associated with higherodds of acquiring NEC (odds ratio[OR] 4.01, 95% CI 2.08–7.35, P ,.001). Thrombocytopenia alone(without neutropenia) was not
associated with higher odds ofacquiring NEC (OR 1.16, 95% CI0.72–1.79, P = .60). Neutropenia wasnot independently associated withhigher odds of acquiring LOS (OR1.44, 95% CI 0.73–2.61, P = .342).
FIGURE 2Blood neutrophil concentrations of 201 neonates with neutropenia of SGA during the first 9 days after birth (mean neutrophil count and SD). The shadedarea shows the normal reference interval based on .100 000 neutrophil counts of neonates during the first 9 days after birth (modified from Henry andChristensen14).
FIGURE 3Blood neutrophil concentrations (mean and SD) during the first 4 days after birth among 4 groups of NICU admissions: (1) SGA, birth weight less thanfirst percentile; (2) SGA, birth weight first to fifth percentile; (3) SGA, birth weight sixth to 10th percentile; and (4) matched controls who were not SGA(birth weight .10th percentile).
PEDIATRICS Volume 136, number 5, November 2015 e1263 by guest on September 1, 2018www.aappublications.org/newsDownloaded from
DISCUSSION
Neutropenia is classically defined asa blood neutrophil concentration ,2SDs of the appropriate reference-population mean.21,22 However,problems arise in applying thisdefinition to newborn infants. First,the normal rise in neutrophil countsduring the first day after birth wouldindicate that neonates who are 6 to12 hours old are neutropenic withcounts as high as 5000/mL, and
between the second and fourth daysafter birth, counts ,3000/mL wouldbe termed neutropenic.22,23 It seemsvery unlikely to us that neutrophilcounts as high as 3000 to 5000/mLwould constitute a host defensedeficiency, even if those counts arestatistically abnormally low. Perhapsa more clinically meaningfuldefinition of neonatal neutropeniawould be a neutrophil countsufficiently low to cause an
antibacterial host-defense deficiency,but that condition is difficult torecognize precisely. In fact, the risk ofinfection imparted by neutropenia isa complex issue, being influenced notonly by the neutrophil count, but alsoby the duration of the low count,21
the size of the marrow neutrophilstorage pool,24 neutrophil function,21
and the underlying cause of theneutropenia.21
Because of these complexities, ratherarbitrary definitions for neonatalneutropenia have been used. Onesuch definition is a count ,1500/mL,but it is not clear that counts in the1000 to 1500/mL range impart anysignificant host defensedeficiency.25,26 We desired, in thepresent analysis, to selecta biologically meaningful definition ofneutropenia, and chose the definitionof a count ,1000/mL typically usedin older children and adults.7,21 Werealized before beginning our studythat by selecting this definition, ourproportion of neonates withneutropenia would be much lowerthan in all previous reports thatdefined neutropenia using highercutoff values. Using this definition, we
FIGURE 4Blood neutrophil concentrations (mean and SD) during the first 4 days after birth among 4 groups of NICU admissions: (1) SGA but no eclampsia orpreeclampsia (PE); (2) PE but not SGA; (3) both SGA and PE; and 4) neither SGA nor PE. n = 100 in each group.
FIGURE 5Among 2981 SGA neonates, NRCB count (/mL) at birth is compared with lowest neutrophil countrecorded in the first 3 days after birth. Individual values are shown as points, and a trend line isshown with a solid line (I = 0.262, P , .001).
e1264 CHRISTENSEN et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from
found neutropenia in 6% of SGAneonates versus 1% of matched non-SGA controls. Six of the 207neutropenic SGA neonates had otherconditions that likely could havegenerated early neutropenia.Excluding these 6 neonates fromfurther analysis, we labeled 201 ashaving the neutropenia of SGA. Wefound that their low neutrophilcounts remained rather unchangedduring the first 4 days after birth andthen increased into the normalreference range by day 7 to 9. Werecognize a potential problem inapplying our neutrophil counts toother published values. Our hospitalsare at altitudes ranging from 2661 to4649 feet (881 to 1417 m) above sealevel. We previously reported that ourreference intervals have a lowerborder (5th percentile) similar tocounts reported at sea level,23 butours have a much higher upperborder (95th percentile).22 Thereasons for this difference, and theeffect on applicability to other data,remain unknown.
In a previous study, we confirmedthat thrombocytopenia is morecommon in SGA neonates than inmatched non-SGA controls.16 Wefound that the thrombocytopenia ofSGA was more severe in neonateswith the most severe growth
restriction (birth weight less thanfirst percentile) than in those withmoderate or mild growth restriction(first to 10th percentile). However, wedid not see that same pattern inneutrophil counts in the currentstudy.
We speculate that the neutropenia ofSGA is due to reduced neutrophilproduction, not acceleratedneutrophil utilization or destruction.This speculation is based on thenormal I/T ratios. The neutropeniaresulting from accelerated neutrophilusage or destruction (eg, sepsis,alloimmune) is typically accompaniedby a left shift.8,9,23,27–29
Several previous studies reportedthat neutropenia associated witheither maternal hypertension or SGAresulted in an elevated risk forsubsequently developingLOS.1,28,30–33 However, other studiesdid not find that association.25,26
Using a regression analysis focusedon those with a neutrophil count,1000/mL, our data suggest that thisvariety of early neutropenia isassociated with a 4-fold increasedrisk for the development of NEC, andthis was the case for the subgroupsweighing $1500 g and ,1500 g atbirth. However, although univariateanalysis also suggested a higher risk
of LOS, this association was explainedby other variables, particularlygestational age. In concordance withour findings, Ree et al reported thatSGA neonates were .2-fold morelikely to develop NEC thanappropriate for gestationalage–matched controls.34 Luig et alalso found a relationship betweenSGA and a risk of NEC, but reportedthat maternal hypertensive disordersof pregnancy were associated witha reduced risk for NEC.35 Ourfindings suggest that the subset ofSGA infants with neutropenia are atgreater risk for NEC than the entiregroup of SGA neonates. Themechanism by which the NEC riskoccurs is not known. It might not bedue to the early neutropenia per se,but could result from otherimmunologic or morphologicabnormalities that accompany theneutropenia of SGA.36,37 For instance,perhaps the intestine is more severelyinjured among the subset of SGAneonates who develop neutropeniathan among the SGA neonates whomaintain normal neutrophil counts.Additional work is needed to clarifythis issue.
Our studies .20 years ago suggestedto us that an inhibitor of neutrophilproduction was present in theplacentas of women withpreeclampsia, and the resolution ofneonatal neutropenia was the resultof removing that source of inhibitor atbirth.30 This issue remainsunresolved, but the fairly consistentresolution of neutropenia in 6 to 7days seems consistent with theelimination of an inhibitor at birth.Tsao et al posed the alternativehypothesis that neutropenia of SGAcould be the result of inadequate fetalG-CSF production.38 This is a rationalalternative explanation, but it seemsto us that if G-CSF production weredefective in utero and thenreestablished after birth, it might takemuch longer to generate neutrophilsthan would the immediate release ofan inhibitor from an otherwise ready-to-go system.
TABLE 2 Associations Between Early Neutropenia (,1000/mL) and Subsequent Development ofEither NEC or LOS in 3644 SGA Neonates
Factor n NECa LOSb
SGA and neutropenia 201 19 (9.5) 56 (27.9)SGA and neutropenia ,1500 g 170 15 (8.8) 53 (49.5)SGA and no neutropenia 3443 69 (2.0) 161 (4.7)SGA and no neutropenia ,1500 g 501 23 (4.6) 43 (8.5)Univariate analysis,
SGA and neutropenia vsSGA and no neutropenia, P
,.0001 ,.001
Univariate analysisSGA ,1500 g and neutropeniavs SGA ,1500 g and noneutropenia, P
Data are expressed as n (%) unless noted otherwise.a Bell stage $2.b Blood culture–positive bacterial sepsis diagnosed .3 days after birth.
PEDIATRICS Volume 136, number 5, November 2015 e1265 by guest on September 1, 2018www.aappublications.org/newsDownloaded from
Our previous study onthrombocytopenia in SGA neonates16
and the present work suggest to usthat the neutropenia andthrombocytopenia associated withSGA are more directly linked withfetal growth restriction than withmaternal hypertension. Thisconclusion is also the one reached byWirbelauer et al, namely that it is SGAstatus, not high maternal bloodpressure, that is associated withneonatal neutropenia.11 In fact, wesuggest that what has been termedneutropenia of pregnancy-inducedhypertension and thrombocytopeniaof pregnancy-induced hypertensionmight more properly be calledneutropenia of SGA andthrombocytopenia of SGA.
The value of administering IVIG and/or rG-CSF to neonates withneutropenia of SGA remainsunproven, but from our presentanalysis, a substantial benefit isunlikely. Although IVIG was given to9% of our neonates, rG-CSF was givento 5%, and both were given to 2%, wewere unable to identify a benefit. Areview by Ohlsson and Lacyconcluded that administering IVIG tolow birth weight neonates reducestheir odds of developing LOS, but onlyby about 3%.39 LaGamma andcolleagues32,40 and Ahmad et al41
convincingly demonstrated thatadministering rG-CSF to neutropenicneonates increases their circulatingneutrophil counts, but Carr et alfound no evidence that prophylacticadministration of rG-CSF or rGM-CSFto very low birth weight neonatesreduces their odds of subsequentlydeveloping a late-onset infection.42
Whether neonates with neutropeniaof SGA would derive any protectionfrom NEC from treatment with IVIGor rG-CSF is unknown and cannot beconcluded from these studies,because the numbers treated withIVIG or rG-CSF were so small.However, even if no medications cancurrently be identified as preventingNEC in these patients, it seemsconceivable to us that just the
awareness that these neonates are atincreased risk could be of some valuein their daily care and expectantmanagement.
ACKNOWLEDGMENTS
The authors thank Joyce M. Koenig,MD, Professor of Pediatrics, MolecularMicrobiology, and Immunology,Department of Pediatrics, Saint LouisUniversity School of Medicine, SaintLouis, MO, and Roger G. Faix, MD,Professor of Pediatrics, University ofUtah School of Medicine, Salt LakeCity, UT, for helpful discussions andmanuscript editing. We also thankErick Henry, MPH, for assistance withdata analysis and display.
ABBREVIATIONS
CBC: complete blood countCI: confidence intervalI/T ratio: immature to total
3. Davies N, Snijders R, Nicolaides KH. Intra-uterine starvation and fetal leucocytecount. Fetal Diagn Ther. 1991;6(3-4):107–112
4. Juul SE, Haynes JW, McPherson RJ.Evaluation of neutropenia andneutrophilia in hospitalized preterminfants. J Perinatol. 2004;24(3):150–157
5. Ozyürek E, Cetintas S, Ceylan T, et al.Complete blood count parameters forhealthy, small-for-gestational-age, full-term newborns. Clin Lab Haematol. 2006;28(2):97–104
6. Christensen RD, Henry E, Wiedmeier SE,Stoddard RA, Lambert DK. Low bloodneutrophil concentrations amongextremely low birth weight neonates:data from a multihospital health-caresystem. J Perinatol. 2006;26(11):682–687
7. Calhoun DA, Christensen RD, Edstrom CS,et al. Consistent approaches toprocedures and practices in neonatalhematology. Clin Perinatol. 2000;27(3):733–753
8. Greenberg DN, Yoder BA. Changes in thedifferential white blood cell count inscreening for group B streptococcalsepsis. Pediatr Infect Dis J. 1990;9(12):886–889
9. Christensen RD, Shigeoka AO, Hill HR,Rothstein G. Circulating and storageneutrophil changes in experimental typeII group B streptococcal sepsis. PediatrRes. 1980;14(6):806–808
11. Wirbelauer J, Thomas W, Rieger L, SpeerCP. Intrauterine growth retardation inpreterm infants #32 weeks of gestationis associated with low white blood cellcounts. Am J Perinatol. 2010;27(10):819–824
12. Sharma G, Nesin M, Feuerstein M, BusselJB. Maternal and neonatalcharacteristics associated with neonatalneutropenia in hypertensivepregnancies. Am J Perinatol. 2009;26(9):683–689
13. Park YH, Lee GM, Yoon JM, et al. Effect ofearly postnatal neutropenia in very lowbirth weight infants born to motherswith pregnancy-induced hypertension.Korean J Pediatr. 2012;55(12):462–469
14. Henry E, Christensen RD. Referenceintervals in neonatal hematology. ClinPerinatol. 2015;42(3):483–497
15. Christensen RD, Baer VL, Henry E, SnowGL, Butler A, Sola-Visner MC.Thrombocytopenia in small forgestational age infants. Pediatrics. 2015;136(2). Available at: www.pediatrics.org/cgi/content/full/136/2/e361
e1266 CHRISTENSEN et al by guest on September 1, 2018www.aappublications.org/newsDownloaded from
16. Christensen RD, Henry E, Kiehn TI, StreetJL. Pattern of daily weights among lowbirth weight neonates in the neonatalintensive care unit: data froma multihospital health-care system. JPerinatol. 2006;26(1):37–43
17. Walsh MC, Kliegman RM. Necrotizingenterocolitis: treatment based onstaging criteria. Pediatr Clin North Am.1986;33(1):179–201
18. Gordon PV, Attridge JT. Understandingclinical literature relevant tospontaneous intestinal perforations. AmJ Perinatol. 2009;26(4):309–316
20. Christensen RD, Baer VL, Yaish HM.Thrombocytopenia in late preterm andterm neonates after perinatal asphyxia.Transfusion. 2015;55(1):187–196
21. Jacobson CA, Berliner N. Neutropenia. InGreer JP, Arber DA, Glader B, List AF,Means Jr, RT, Paraskevas F, Rodgers GM,eds. Wintrobe’s Clinical Hematology, 13thEd. Philadelphia: Lippincott, Williams &Wilkins, 2014:1279
22. Schmutz N, Henry E, Jopling J,Christensen RD. Expected ranges forblood neutrophil concentrations ofneonates: the Manroe and Mouzinhocharts revisited. J Perinatol. 2008;28(4):275–281
23. Manroe BL, Weinberg AG, Rosenfeld CR,Browne R. The neonatal blood count inhealth and disease. I. Reference valuesfor neutrophilic cells. J Pediatr. 1979;95(1):89–98
24. Erdman SH, Christensen RD, Bradley PP,Rothstein G. Supply and release ofstorage neutrophils. A developmentalstudy. Biol Neonate. 1982;41(3–4):132–137
25. Teng R-J, Wu T-J, Garrison RD, Sharma R,Hudak ML. Early neutropenia is notassociated with an increased rate of
nosocomial infection in very low-birth-weight infants. J Perinatol. 2009;29(3):219–224
26. Paul DA, Leef KH, Sciscione A, Tuttle DJ,Stefano JL. Preeclampsia does notincrease the risk for culture provensepsis in very low birth weight infants.Am J Perinatol. 1999;16(7):365–372
27. Schelonka RL, Yoder BA, desJardins SE,Hall RB, Butler J. Peripheral leukocytecount and leukocyte indexes in healthynewborn term infants. J Pediatr. 1994;125(4):603–606
28. Mouzinho A, Rosenfeld CR, Sanchez PJ,Risser R. Effect of maternal hypertensionon neonatal neutropenia and risk ofnosocomial infection. Pediatrics. 1992;90(3):430–435
29. Doron MW, Makhlouf RA, Katz VL, LawsonEE, Stiles AD. Increased incidence ofsepsis at birth in neutropenic infants ofmothers with preeclampsia. J Pediatr.1994;125(3):452–458
30. Koenig JM, Christensen RD. Themechanism responsible for diminishedneutrophil production in neonatesdelivered of women with pregnancy-induced hypertension. Am J ObstetGynecol. 1991;165(2):467–473
31. Cadnapaphornchai M, Faix RG. Increasednosocomial infection in neutropenic lowbirth weight (2000 grams or less)infants of hypertensive mothers. JPediatr. 1992;121(6):956–961
32. La Gamma EF, Alpan O, Kocherlakota P.Effect of granulocyte colony-stimulatingfactor on preeclampsia-associatedneonatal neutropenia. J Pediatr. 1995;126(3):457–459
33. Kocherlakota P, La Gamma EF.Preliminary report: rhG-CSF may reducethe incidence of neonatal sepsis inprolonged preeclampsia-associatedneutropenia. Pediatrics. 1998;102(5):1107–1111
34. Ree IM, Smits-Wintjens VE, Rijntjes-Jacobs EG, et al. Necrotizing enterocolitis
in small-for-gestational-age neonates:a matched case-control study.Neonatology. 2014;105(1):74–78
35. Luig M, Lui K; NSW & ACT NICUS Group.Epidemiology of necrotizing enterocolitis,Part II: Risks and susceptibility ofpremature infants during the surfactantera: a regional study. J Paediatr ChildHealth. 2005;41(4):174–179
36. Li J, Li H, Mao H, et al. Impaired NK cellantiviral cytokine response againstinfluenza virus in small-for-gestational-age neonates. Cell Mol Immunol. 2013;10(5):437–443
37. Neta GI, von Ehrenstein OS, Goldman LR,et al. Umbilical cord serum cytokinelevels and risks of small-for-gestational-age and preterm birth. Am J Epidemiol.2010;171(8):859–867
38. Tsao PN, Teng RJ, Tang JR, Yau KI.Granulocyte colony-stimulating factor inthe cord blood of premature neonatesborn to mothers with pregnancy-inducedhypertension. J Pediatr. 1999;135(1):56–59
39. Ohlsson A, Lacy JB. Intravenousimmunoglobulin for preventing infectionin preterm and/or low birth weightinfants. Cochrane Database Syst Rev.2013;7:CD000361
40. La Gamma EF, De Castro MH. What is therationale for the use of granulocyte andgranulocyte-macrophage colony-stimulating factors in the neonatalintensive care unit? Acta Paediatr Suppl.2002;91(438):109–116
41. Ahmad M, Fleit HB, Golightly MG, LaGamma EF. In vivo effect of recombinanthuman granulocyte colony-stimulatingfactor on phagocytic function andoxidative burst activity in septicneutropenic neonates. Biol Neonate.2004;86(1):48–54
42. Carr R, Modi N, Doré C. G-CSF and GM-CSF for treating or preventing neonatalinfections. Cochrane Database Syst Rev2003;3:CD003066
PEDIATRICS Volume 136, number 5, November 2015 e1267 by guest on September 1, 2018www.aappublications.org/newsDownloaded from
originally published online October 12, 2015; Pediatrics Allison Butler
Robert D. Christensen, Bradley A. Yoder, Vickie L. Baer, Gregory L. Snow andEarly-Onset Neutropenia in Small-for-Gestational-Age Infants
ServicesUpdated Information &
015-1638http://pediatrics.aappublications.org/content/early/2015/10/06/peds.2including high resolution figures, can be found at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/blood_disorders_subBlood Disorders_subhttp://www.aappublications.org/cgi/collection/hematology:oncologyHematology/Oncologyhttp://www.aappublications.org/cgi/collection/neonatology_subNeonatologysubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on September 1, 2018www.aappublications.org/newsDownloaded from