ECZEMAS ECZEMAS Cecilia T. Roxas-Rosete, Cecilia T. Roxas-Rosete, FPDS FPDS Consultant, Section of Dermatology Consultant, Section of Dermatology The Medical City Hospital The Medical City Hospital
Transcript
ECZEMASECZEMASCecilia T. Roxas-Rosete, FPDSCecilia T. Roxas-Rosete, FPDS
Consultant, Section of DermatologyConsultant, Section of DermatologyThe Medical City HospitalThe Medical City Hospital
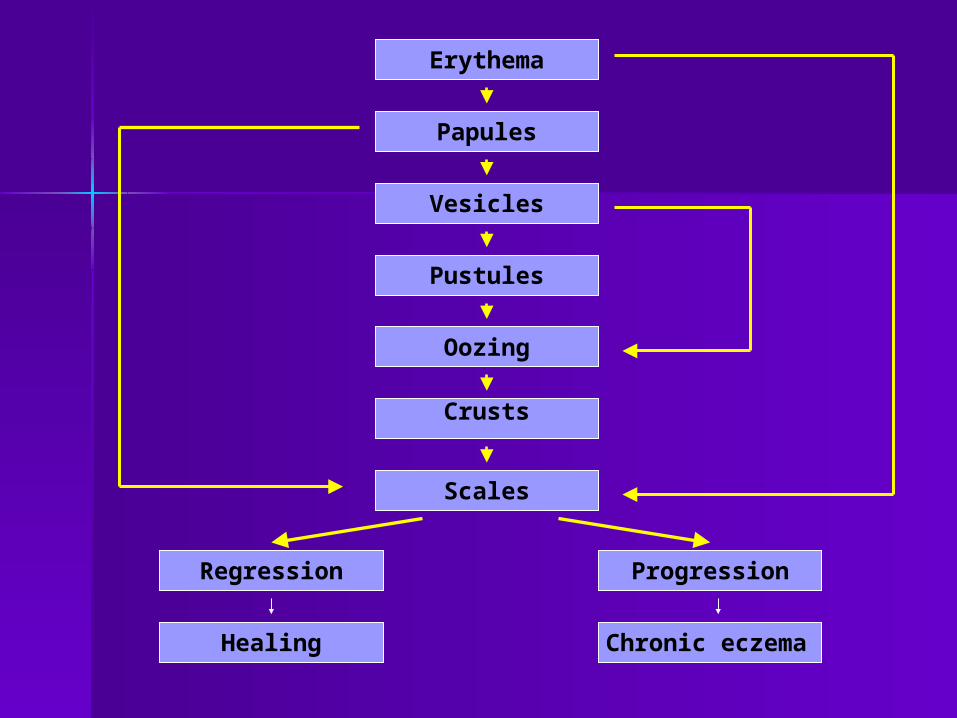
-Greek word ek – zeo “to boil Greek word ek – zeo “to boil or bubble over”or bubble over”
Erythema
Papules
Vesicles
Pustules
Oozing
Crusts
Scales
Chronic eczemaHealing
ProgressionRegression
Series 2007Series 2007 A PEODG and SP Dermatology ExclusiveA PEODG and SP Dermatology Exclusive
Acute EczemaAcute Eczema
Series 2007Series 2007 A PEODG and SP Dermatology ExclusiveA PEODG and SP Dermatology Exclusive
Chronic EczemaChronic Eczema
EPIDEMIOLOGYEPIDEMIOLOGY
Atopic dermatitis (AD) is a chronically Atopic dermatitis (AD) is a chronically relapsing skin disorder that arises relapsing skin disorder that arises most commonly during early infancy, most commonly during early infancy, childhood or adolescencechildhood or adolescence
Usually begins before age 6 monthsUsually begins before age 6 months Remits spontaneously in 65% of Remits spontaneously in 65% of
affected children before age 10 yearsaffected children before age 10 years
EPIDEMIOLOGY:EPIDEMIOLOGY:
STAGESSTAGES
1)1) Infantile – 2 months to Infantile – 2 months to 2 yrs.2 yrs.
2)2) Childhood – 2 to 10 yrs.Childhood – 2 to 10 yrs.
Triggered by an interplay of Triggered by an interplay of factorsfactors
1.1. GeneticGenetic
2.2. ImmunologicImmunologic
3.3. EnvironmentalEnvironmental
Hanifin &Rajka’s Diagnostic Hanifin &Rajka’s Diagnostic Criteria for Atopic DermatitisCriteria for Atopic DermatitisMust have > 3 major criteria & > 3 Must have > 3 major criteria & > 3 minor criteriaminor criteria
Major Criteria:Major Criteria: PruritusPruritus Personal or family history of atopic Personal or family history of atopic
Chronic or chronically relapsing courseChronic or chronically relapsing course Typical distribution and morphologyTypical distribution and morphology
> infants: facial and extensor involvement> infants: facial and extensor involvement> children & adults: flexural lichenification > children & adults: flexural lichenification and linearityand linearity
Hanifin & Rajka’s Diagnostic Hanifin & Rajka’s Diagnostic Criteria for Atopic DermatitisCriteria for Atopic Dermatitis
Minor Criteria:Minor Criteria: XerosisXerosis Icthyosis/keratosis pilaris/palmar Icthyosis/keratosis pilaris/palmar
hyperlinearityhyperlinearity Type I skin test reactivityType I skin test reactivity Elevated serum IgEElevated serum IgE Early age at onsetEarly age at onset Tendency to skin infection (Staph aureus & HS Tendency to skin infection (Staph aureus & HS
I)I) Hand / foot dermatitisHand / foot dermatitis
Hanifin & Rajka’s Diagnostic Hanifin & Rajka’s Diagnostic Criteria for Atopic DermatitisCriteria for Atopic Dermatitis
ant. subscapular cataractsant. subscapular cataracts Dennie-Morgan foldDennie-Morgan fold Orbital darkeningOrbital darkening Pityriasis albaPityriasis alba
Hanifin & Rajka’s Diagnostic Hanifin & Rajka’s Diagnostic Criteria for Atopic DermatitisCriteria for Atopic Dermatitis
Minor Criteria:Minor Criteria: Itch when sweatingItch when sweating Intolerance to wool and lipid solventsIntolerance to wool and lipid solvents Food intoleranceFood intolerance Perifollicular accentuationPerifollicular accentuation White dermographism / delayed White dermographism / delayed
blanchingblanching Course influenced by Course influenced by
SEBORRHEIC SEBORRHEIC DERMATITISDERMATITIS common chronic skin disordercommon chronic skin disorder infants / adultsinfants / adults often assoc with increased sebum often assoc with increased sebum
production (seborrhea) of face & production (seborrhea) of face & scalpscalp
2-5% of the population2-5% of the population affects males > femalesaffects males > females often assoc with HIV (85%), often assoc with HIV (85%),
parkinsonismparkinsonism
Etiology – Inflammatory Rx to yeast Etiology – Inflammatory Rx to yeast (Pityrosporum Ovale)(Pityrosporum Ovale)
assoc with emotional stressassoc with emotional stress sites – legs, arms, dorsum of sites – legs, arms, dorsum of
handshands
Dyshidrotic Dyshidrotic eczemaeczema
Lichen simplex Lichen simplex chronicuschronicus
CONTACT DERMATITISCONTACT DERMATITIS
Any pruritic skin disorder that results Any pruritic skin disorder that results when a particular substance comes in when a particular substance comes in contact with the skincontact with the skin
Inflammation of the skin with Inflammation of the skin with spongiosis or intercellular edema of the spongiosis or intercellular edema of the epidermisepidermis
A common cause of occupational A common cause of occupational disabilitydisability
A form of extrinsic eczemaA form of extrinsic eczema
1.1. Irritant CD – Skin reaction resulting Irritant CD – Skin reaction resulting from exposure to an offending agent.from exposure to an offending agent.
2. Allergic CD – results from repeated 2. Allergic CD – results from repeated exposure to an allergen or compound exposure to an allergen or compound due to DELAYED hypersensitivity RXdue to DELAYED hypersensitivity RX
Severity of the reaction is related to the Severity of the reaction is related to the amount and duration of exposure to the amount and duration of exposure to the irritant.irritant.
Most cases are acute in onset - Most cases are acute in onset - symptoms develop within seconds of symptoms develop within seconds of exposure.exposure.
Prolonged exposure to a low-level irritant Prolonged exposure to a low-level irritant (soap, water) can lead to chronic ICD.(soap, water) can lead to chronic ICD.
ALLERGIC CONTACT ALLERGIC CONTACT DERMATITIS (ACD)DERMATITIS (ACD)Due to repeated exposure to a Due to repeated exposure to a
substance to which the substance to which the individual is sensitizedindividual is sensitized
A cell-mediated type IV A cell-mediated type IV delayed hypersensitivity delayed hypersensitivity reactionreaction
Series 2007Series 2007 A PEODG and SP Dermatology ExclusiveA PEODG and SP Dermatology Exclusive
Application of contact allergens Application of contact allergens (Ag) (Ag)
Release of cytokines by Release of cytokines by keratinocytes, Langerhans cells keratinocytes, Langerhans cells and other cells within the skinand other cells within the skin
Cytokines activate Langerhans Cytokines activate Langerhans cells which uptake the antigen cells which uptake the antigen and emigrate into the regional and emigrate into the regional lymph nodeslymph nodes
During this process, the During this process, the Langerhans cells mature into Langerhans cells mature into dendritic cells; the antigen is dendritic cells; the antigen is processed, re-expressed on the processed, re-expressed on the surface and finally presented to surface and finally presented to naïve T cells in the regional lymph naïve T cells in the regional lymph nodenode
Upon appropriate antigen Upon appropriate antigen presentation, T cells bearing the presentation, T cells bearing the appropriate T cell receptor appropriate T cell receptor clonally expand and become clonally expand and become effector T cells. effector T cells.
Effector T cells recirculate into the Effector T cells recirculate into the periphery where they may later periphery where they may later meet the antigen again. meet the antigen again.
Common Allergens In Common Allergens In the General Populationthe General Population
NACDG 1998NACDG 1998
1.1. NickelNickel
2.2. FragrancesFragrances
3.3. NeomycinNeomycin
4.4. Balsam of PeruBalsam of Peru
5.5. ThimerosalThimerosal
PCDSG 2000PCDSG 2000
1.1. NickelNickel
2.2. Potassium Potassium DichromateDichromate
3.3. Fragrance MixFragrance Mix
4.4. CobaltCobalt
5.5. Paraben MixParaben Mix
ACD: NickelACD: Nickel
ACD: NickelACD: Nickel
ACD: NickelACD: Nickel
ACD: FragranceACD: Fragrance
ACD: Colorant in ACD: Colorant in ToothpasteToothpaste
ACD: Fragrance in ACD: Fragrance in DeodorantDeodorant
Common Occupational Common Occupational AllergensAllergens Rubber accelerating chemicals Rubber accelerating chemicals
Series 2007Series 2007 A PEODG and SP Dermatology ExclusiveA PEODG and SP Dermatology Exclusive
ACD due to contact with ACD due to contact with acrylatesacrylates
ACD: ChromateACD: Chromate
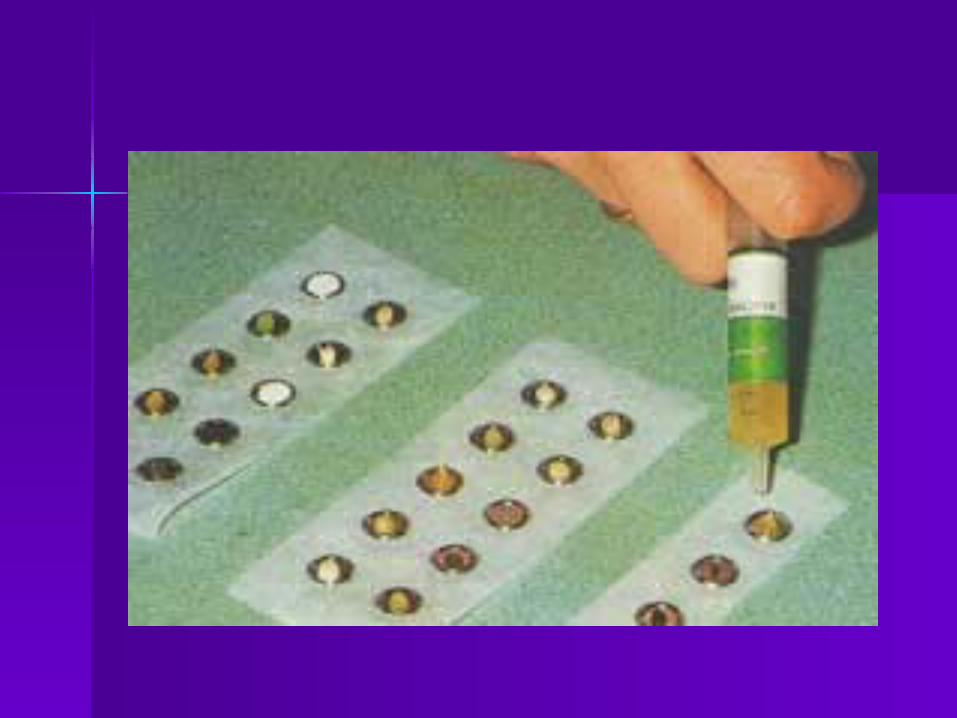
Patch TestPatch Test
Only objective diagnostic tool for Only objective diagnostic tool for the definitive diagnosis of allergic the definitive diagnosis of allergic contact dermatitiscontact dermatitis
May aid in differentiating ACD May aid in differentiating ACD from ICDfrom ICD
Patch Test: TechniquePatch Test: Technique
1.1. Test substances Test substances appropriately diluted. appropriately diluted. Standardized kits Standardized kits available. available.
Some Common Allergens Some Common Allergens Used in Patch TestingUsed in Patch Testing
Nickel - JewelryNickel - Jewelry Balsam of Peru - Perfumes, citrus fruitsBalsam of Peru - Perfumes, citrus fruits Dichromate - Cement, leather, matchesDichromate - Cement, leather, matches Paraphenylenediamine - Hair dyes, Paraphenylenediamine - Hair dyes,
5. Relate relevance of positive 5. Relate relevance of positive reactions to clinical dermatitis reactions to clinical dermatitis cautiously. Careful history and cautiously. Careful history and review of skin exposures must review of skin exposures must establish significanceestablish significance
Photocontact eczemaPhotocontact eczema
Require exposure to sunlight following Require exposure to sunlight following topical application of certain chemicalstopical application of certain chemicals
Long wave UVA – action spectrumLong wave UVA – action spectrum Topical photosensitizers – PPD in hair Topical photosensitizers – PPD in hair
dyes, PABA esters in sunscreening dyes, PABA esters in sunscreening agents, halogenated salicylates in soaps agents, halogenated salicylates in soaps and cosmetics & topical sulfonamidesand cosmetics & topical sulfonamides
Topical photoirritants – psoralens in Topical photoirritants – psoralens in perfumesperfumes
Consultant, Section of Consultant, Section of DermatologyDermatology
The Medical City HospitalThe Medical City Hospital
PsoriasisPsoriasis
EPIDEMIOLOGYEPIDEMIOLOGY Age of onset: 20 to 50 y/oAge of onset: 20 to 50 y/o Sex: M=FSex: M=F Heredity: PolygenicHeredity: Polygenic Pathogenesis: Alteration of the Pathogenesis: Alteration of the
cell kinetics of keratinocytescell kinetics of keratinocytes
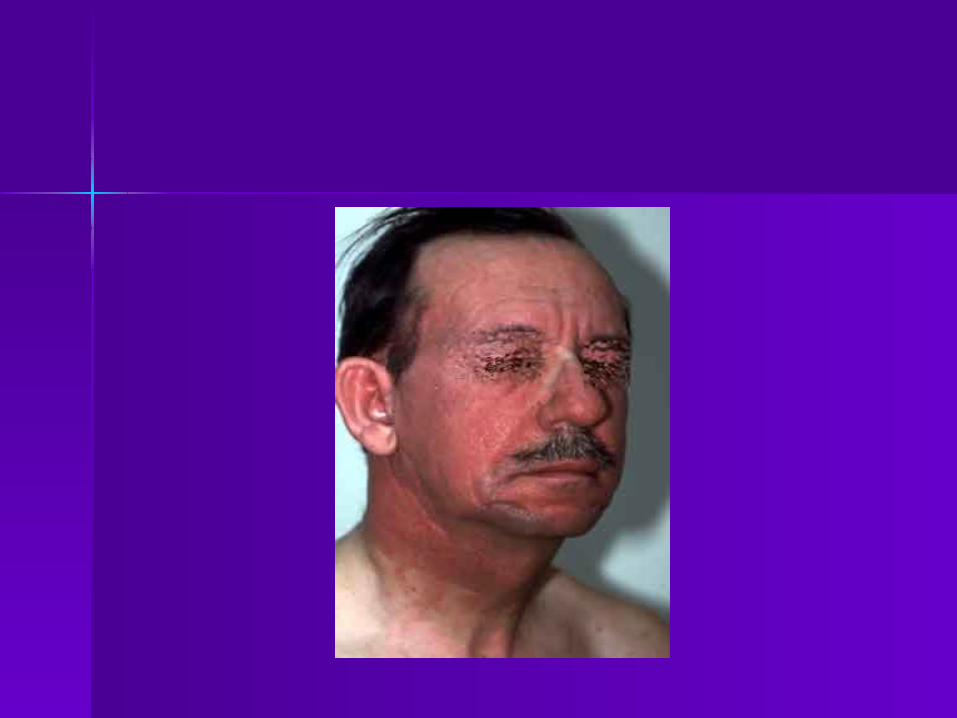
PsoriasisPsoriasis
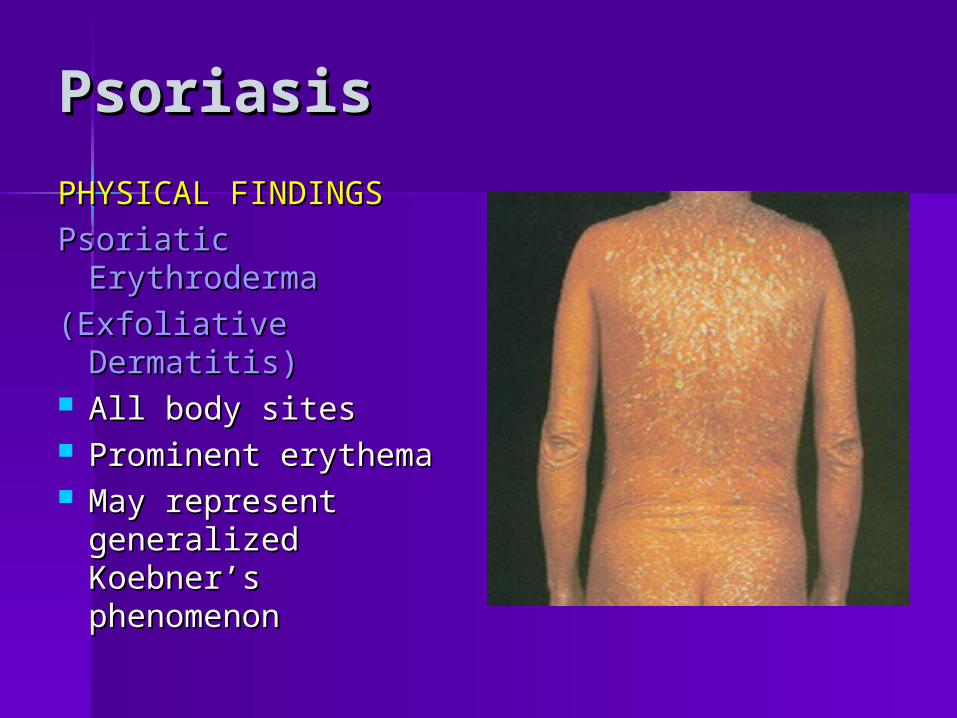
PHYSICAL FINDINGSPHYSICAL FINDINGS
Psoriasis VulgarisPsoriasis Vulgaris Most commonMost common Erythematous well-Erythematous well-
defined papules & defined papules & plaques with large plaques with large amounts of silvery amounts of silvery white scaleswhite scales
Sites: scalp, Sites: scalp, elbows,knees, lumbar elbows,knees, lumbar area area
of von Zumbuschof von Zumbusch Pus are sterilePus are sterile
PsoriasisPsoriasis
TRIGGER FACTORSTRIGGER FACTORS
A. Physical trauma: Koebner’s A. Physical trauma: Koebner’s PhenomenonPhenomenon
various traumatic insult to skinvarious traumatic insult to skin 30%-50% of psoriasis patients 30%-50% of psoriasis patients
give history of koebner’sgive history of koebner’s
PsoriasisPsoriasis
Koebner’s PhenomenonKoebner’s Phenomenon
PsoriasisPsoriasis
TRIGGER FACTORSTRIGGER FACTORS
B. InfectionB. Infection 15%-76% report history of infection15%-76% report history of infection E.g. Streptococcal throat infectionE.g. Streptococcal throat infection
- guttate psoriasis- guttate psoriasis
HIVHIV
- 2.5% develop psoriasis- 2.5% develop psoriasis
PsoriasisPsoriasis
TRIGGER FACTORSTRIGGER FACTORS
C. StressC. Stress 30%-40% adult cases30%-40% adult cases 90% in children90% in children
PsoriasisPsoriasis
TRIGGER FACTORSTRIGGER FACTORS
D. DrugsD. Drugs Corticosteroids – may cause flare-upsCorticosteroids – may cause flare-ups LithiumLithium Beta-Adrenergic blockers, ACE Beta-Adrenergic blockers, ACE