5/22/2009 1 EEG in Status Epilepticus Paul A. Garcia, M.D. For discussion today • Recognizing Seizures • Recognizing Status • Assessing Treatment …hard to define, but "I know it when I see it" Potter Stewart on pornography Inter-observer Agreement • Experienced: Kappa= 0.5 • Inexperienced: Kappa= 0.29 • Agreement also dependent upon pattern Ronner HE et al, Seizure. in press
Transcript
5/22/2009
1
EEG in Status Epilepticus
Paul A. Garcia, M.D.
For discussion today
• Recognizing Seizures
• Recognizing Status
• Assessing Treatment
…hard to define, but "I know it when I see it "
Potter Stewart on pornography
Inter-observer Agreement
• Experienced: Kappa= 0.5
• Inexperienced: Kappa= 0.29
• Agreement also dependent upon pattern
Ronner HE et al, Seizure. in press
5/22/2009
2
Seizure pattern examples
5/22/2009
3
5/22/2009
4
Less agreement
5/22/2009
5
5/22/2009
6
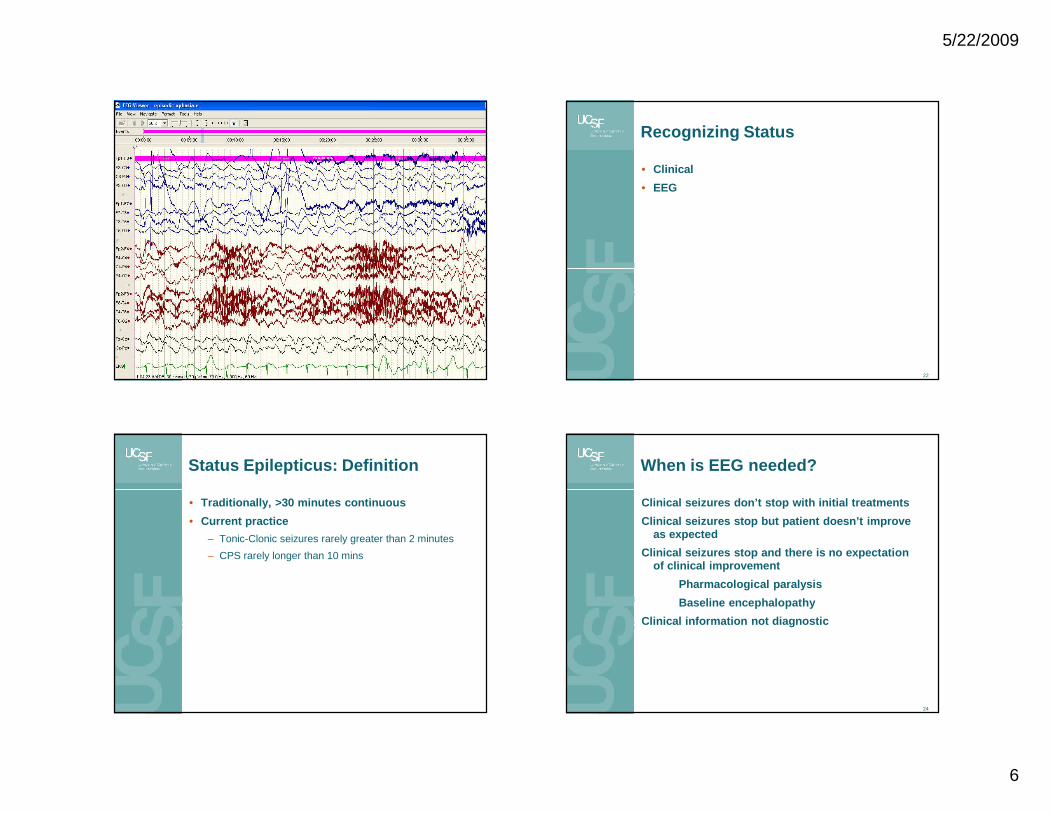
Recognizing Status
• Clinical
• EEG
22
Status Epilepticus: Definition
• Traditionally, >30 minutes continuous
• Current practice
– Tonic-Clonic seizures rarely greater than 2 minutes
– CPS rarely longer than 10 mins
When is EEG needed?
Clinical seizures don’t stop with initial treatment s
Clinical seizures stop but patient doesn’t improve as expected
Clinical seizures stop and there is no expectation of clinical improvement
Pharmacological paralysis
Baseline encephalopathy
Clinical information not diagnostic
24
5/22/2009
7
EEG patterns of status epilepticus
• Most clear when the patterns approach what we recognize as “ictal” based on experience with discrete seizures
• Some EEG patterns are common to seizures, normal physiological function and encephalopathy
















![Focal hemodynamic patterns of status epilepticus detected ... · epilepticus or subtle status epilepticus [4]. Electroenceph-alogram (EEG), the diagnostic gold standard, may not be](https://static.documents.pub/doc/80x56/6074493ed430437ef144c30f/focal-hemodynamic-patterns-of-status-epilepticus-detected-epilepticus-or-subtle.jpg)









