EFFECT OF GLYCOPYRROLATE ON ANTRAL MOTILITY, GASTRIC EMPTYING, AND INTESTINAL TRANSIT* Robert Young and David C. H. Sun Mount Alto Veterans Adminidralion Hospital, George Washington University School of Medicine, and Georgetown University School of Medicine, Washington, D.C. In our previous study' on the effect of glycopyrrolate on basal gastric secre- tion, we found that the optimal effective dose would suppress acidity to pH 4.5 or higher in all 16 patients. In addition to the gastric hypersecretion, the patient with uncomplicated duodenal ulcer often has rapid gastric emptying. Some depression of the rapid gastric emptying would be desirable, but ex- cessive delay would be objectionable as it might increase the gastric phase of gastric secretion? For this reason glycopyrrolate, a new anticholinergic drug, was studied in 16 patients with duodenal ulcer, with regards to its effect on antral motility, gastric emptying, and intestinal transit. Method Eject of glycopyrrolate on antral motility. The first part of this study was related to the effect of glycopyrrolate on antral motility, measured by a balloon pressure transducer recording system in 10 patients. The patients, after an overnight fast, and having received no medication the day before the test, reported to the laboratory at 8:OO A.M. The patient was intubated with a Rehfuss tube. A thin latex bag with a capacity of 25 to 35 cc. was tied over the distal end of the tube. Prior to insertion of the tube, each bag was checked for air leaks. The volume of air necessary to fill the bag without tension on its walls was determined prior to testing. At the end of each study, before the tube was withdrawn, the air remaining in the balloon was removed and its volume noted. In no case was there air leakage during the time of the study. The proximal end of the Rehfuss tube was connected to a water-filled Statham transducer placed at a height of 11 cm. from the fluoroscopic table representing the posterior body surface. Respirations were monitored by a Sanborn pneumograph bellows. Permanent recordings of the proceeding were obtained on a Sanborn multichannel heat-sensitive recorder. All patients were studied supine on the fluoroscopic table. The metal Rehfuss tip was placed just below the angulus allowing the inflated balloon to rest in the antrum. The position of the tip of the tube and the balloon was checked fluoroscopically initially, during, and at the termination of the pro- ceedings. The antral motility was recorded for a control period of at least 15 to 30 minutes. At this time, glycopyrrolate, in a dose of 0.2 or 0.5 mg., was administered subcutaneously. Recording was continued for 1 hour or more or until antral activity returned to premedication level. Six patients with chronic duodenal ulcer were studied. Two studies were made on each patient on different days and each subject served as his own control. The technique of this study has been described previ~usly.~ In brief, after an overnight fast and having received no medication on the day before the test, *This study was supported in part by a grant from The National Foundation for In- dependent Medical Research, Washington, D.C., and A. H. Robins, Co., Inc. Richmond, Va. 174 Eject of glycopyrrolate on gastric emptying and intestinal transit.
Transcript
EFFECT OF GLYCOPYRROLATE ON ANTRAL MOTILITY, GASTRIC EMPTYING, AND INTESTINAL TRANSIT*
Robert Young and David C. H. Sun Mount Alto Veterans Adminidralion Hospital, George Washington University School of Medicine,
and Georgetown University School of Medicine, Washington, D.C.
In our previous study' on the effect of glycopyrrolate on basal gastric secre- tion, we found that the optimal effective dose would suppress acidity to p H 4.5 or higher in all 16 patients. In addition to the gastric hypersecretion, the patient with uncomplicated duodenal ulcer often has rapid gastric emptying. Some depression of the rapid gastric emptying would be desirable, but ex- cessive delay would be objectionable as it might increase the gastric phase of gastric secretion? For this reason glycopyrrolate, a new anticholinergic drug, was studied in 16 patients with duodenal ulcer, with regards to its effect on antral motility, gastric emptying, and intestinal transit.
Method Eject of glycopyrrolate on antral motility. The first part of this study was
related to the effect of glycopyrrolate on antral motility, measured by a balloon pressure transducer recording system in 10 patients. The patients, after an overnight fast, and having received no medication the day before the test, reported to the laboratory a t 8:OO A.M. The patient was intubated with a Rehfuss tube. A thin latex bag with a capacity of 25 to 35 cc. was tied over the distal end of the tube. Prior to insertion of the tube, each bag was checked for air leaks. The volume of air necessary to fill the bag without tension on its walls was determined prior to testing. At the end of each study, before the tube was withdrawn, the air remaining in the balloon was removed and its volume noted. In no case was there air leakage during the time of the study. The proximal end of the Rehfuss tube was connected to a water-filled Statham transducer placed at a height of 11 cm. from the fluoroscopic table representing the posterior body surface. Respirations were monitored by a Sanborn pneumograph bellows. Permanent recordings of the proceeding were obtained on a Sanborn multichannel heat-sensitive recorder.
All patients were studied supine on the fluoroscopic table. The metal Rehfuss tip was placed just below the angulus allowing the inflated balloon to rest in the antrum. The position of the tip of the tube and the balloon was checked fluoroscopically initially, during, and a t the termination of the pro- ceedings. The antral motility was recorded for a control period of a t least 15 to 30 minutes. At this time, glycopyrrolate, in a dose of 0.2 or 0.5 mg., was administered subcutaneously. Recording was continued for 1 hour or more or until antral activity returned to premedication level.
Six patients with chronic duodenal ulcer were studied. Two studies were made on each patient on different days and each subject served as his own control. The technique of this study has been described previ~usly.~ In brief, after an overnight fast and having received no medication on the day before the test,
*This study was supported in part by a grant from The National Foundation for In- dependent Medical Research, Washington, D.C., and A. H. Robins, Co., Inc. Richmond, Va.
174
Eject of glycopyrrolate on gastric emptying and intestinal transit.
Young & Sun : Glycopyrrolate and Digestive Functions 175 the patient was given either placebo or 2 mg. of glycopyrrolate orally at 8:30 A.M. At 9:OO A.M., an Ewald meal of 2 slices of dry toasted bread and 150 cc. of water was given. This was immediately followed by a barium-water mix- ture, consisting of 120 gm. of barium sulfate suspended in 150 cc. of water. At 1O:OO A.M., 11:OO A.M. , and 1:oO P.M., anteroposterior supine 14 X 17-in. X-ray films of the abdomen were taken. The amount of barium retained in the stomach as well as the position of the advancing barium column in the intestine were estimated by two observers and the averages of these figures
FIGURE 1. Antral motility recording before and alter the administration of glycopyrrolate, 0.5 mg. subcutaneously.
recorded. In view of the difficulty in estimating exactly the per cent of barium remaining in the stomach, the degree of retention was arbitrarily divided into five catagories designated as 75, 50, 25, 5 (trace), and0 percent (empty). The position of the head of the barium column in the intestine was recorded with regards to the proximal or distal portion of the particular portion of the in- testinal tract under observation.
Resulls
Eject of glycopyrrolate on antral motility. A typical recording of antral motility before and after the administration of 0.5 mg. of glycopyrrolate sub- cutaneously was shown in FIGURE 1. During the control period, both Type I
176 Annals New York Academy of Sciences and Type I1 waves were observed for a period of 42 minutes. Subcutaneous administration of glycopyrrolate produced a complete suppression of Type I1 activity for 43 minutes after a latent period of 29 minutes.
Case No.
1 2 3 4 5
FIGURE 2. Effect of 0.2 mg. of glycopyrrolate, administered subcutaneously, on antra motility.
TABLE 1 THE EFFECT OF SUBCUTANEOUSLY ADMINISTERED GLYCOPYRROLATE ON ANTRAL MOTILITY
Dose
mg. 0.5 0.5 0.5 0.5 0.5
21 8
No effect
8 8
29 7 5
Latent period
6 7 8 9
10
Wave type I I Wave type II
0 . 2 0 .2 0 . 2 0 . 2 0 . 2
No effect No effect No effect No effect
2 25
No effect 6
29
Duration of effect
Wave type I 1 Wave type 11
min. 120 1 105
I
FIGURE 2 shows the effect of 0.2 mg. of glycopyrrolate subcutaneously on antral motility. A control period of 19 minutes showed the presence of both Type I and Type I1 waves. Glycopyrrolate, in a dose of 0.2 mg., produced a complete suppression of the Type I1 wave for 38 minutes after a latent period of 29 minutes. There was no effect on the Type I wave.
Young & Sun: Glycopyrrolate and Digestive Functions 177 TABLE I lists the effect of glycopyrrolate on antral motility in all 10 patients.
There were 5 patients on each dose. Glycopyrrolate, in a dose of 0.5 mg., produced a complete suppression of the Type I1 wave in each of the 5 pa- tients. The duration of effect varied from 43 minutes to greater than 130 minutes. On the other hand, 0.2 mg. of glycopyrrolate produced suppression of Type I1 waves in 4 of the 5 patients. Type I motility was not affected in any case by glycopyrrolate 0.2 mg. subcutaneously although the height and frequency of the Type I contractions was often de- creased.
Minimal side effects were noted with equal frequency a t both dosages and consisted merely of slight dryness of the mouth.
The latent period varied from 5 to 29 minutes.
The duration of effect varied from 33 to 57 minutes.
G L Y C O P Y R O L L A T E 2 N G
PLACEBO
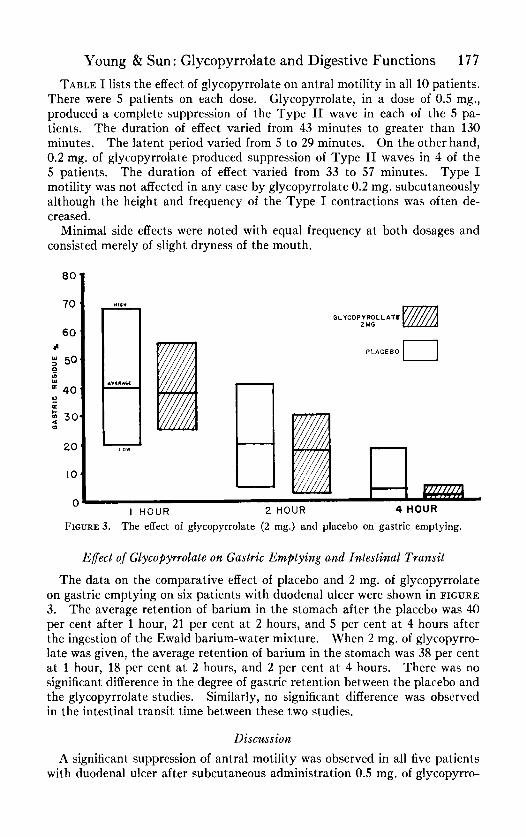
FIGURE 3. The effect of glycopyrrolate (2 mg.) and placebo on gastric emptying.
Effecl o j Glycopyrrolate on Gastric Emptying and Intestinal Transit
The data on the comparative effect of placebo and 2 mg. of glycopyrrolate on gastric emptying on six patients with duodenal ulcer were shown in FIGURE 3. The average retention of barium in the stomach after the placebo was 40 per cent after 1 hour, 21 per cent at 2 hours, and 5 per cent a t 4 hours after the ingestion of the Ewald barium-water mixture. When 2 mg. of glycopyrro- late was given, the average retention of barium in the stomach was 38 per cent a t 1 hour, 18 per cent a t 2 hours, and 2 per cent a t 4 hours. There was no significant difference in the degree of gastric retention between the placebo and the glycopyrrolate studies. Similarly, no significant difference was observed in the intestinal transit time between these two studies.
Discussion A significant suppression of antral motility was observed in all five patients
with duodenal ulcer after subcutaneous administration 0.5 mg. of glycopyrro-
178 Annals New York Academy of Sciences late. Suppression of Type I1 wave, the peristaltic wave, was observed in four of five patients after subcutaneous administration of 0.2 mg. of glycopyrrolate. However, no significant delay in gastric emptying was observed in six patients a t 1?4 and 2p2 hours after oral ingestion of 2 mg. of glycopyrrolate. Excessive delay in gastric emptying for any reason is physiologically undesirable in the peptic ulcer patient inasmuch as stasis of food in the antrum of the stomach has been shown to cause a prolongation of the antral hormonal phase of gastric secretion.* In addition, epigastric discomfort, fullness and pain, and bouts of nausea and “retention vomiting” had been noted in patients with excessive delay in gastric emptying on an anticholinergic drug with a potent antimotility effect. A satisfactory anticholinergic durg must have a wide differential in action between the effective dose of the drug that inhibits secretion and the action of that dose on motility.
Summary Glycopyrrolate in a dose of 0.5 mg. subcutaneously completely suppressed
the Type I1 antral waves in all five cases and the Type I wave in four of the five cases. When 0.2 mg. was given subcutaneously, complete suppression of Type I1 wave was observed in four of five patients without effect on the Type I wave. Glycopyrrolate in a dose of 2 mg. orally did not effect gastric emptying or intestinal transit time. Side effects were minimal and limited to merely a slight dryness of the mouth noted only on subcutaneous injection.
Acknowledgment The authors gratefully acknowledge the technical assistance of Miss Alice
Young.
References 1. SUN, D. C. H. Comparative study on the effect of glycopyrrolate and propanthe-
2. EVANS, S. O., JR., J. M. ZUBIRAN, J. D. MCCARTHY, S. H. RAGIN, E. R. WOODWARD, & L. Stimulating efTect of vagotomy on gastric secretion in Heiden-
3. SUN, D. C. H., H. SHAY & H. WOLOSHIN. Effect of tricyclamol on gastric empty-
1962. line on basal gastric secretion.
R. DRAGSTEDT. hain pouch dogs. Am. J. Physiol. 174: 209.
ing and intestinal transit. Am. J. Digest. Diseases. 4: 282.