34
1 Emerging technologies for the diagnosis, treatment and management of refractory asthma Horizon Scanning Research & Intelligence Centre February 2016

1
Emerging technologies for the diagnosis, treatment and
management of refractory asthma
Horizon Scanning Research & Intelligence Centre
February 2016

2
This report presents independent research funded by the National Institute for Health Research (NIHR). The views expressed in this publication are those of the author(s)
and not necessarily those of the NHS, the NIHR or the Department of Health.
The NIHR Horizon Scanning Research and Intelligence Centre, University of Birmingham, United Kingdom
[email protected] www.hsric.nihr.ac.uk
Copyright © University of Birmingham 2016

3
CONTENTS
EXECUTIVE SUMMARY ................................................................................................................................. 4
ACKNOWLEDGEMENTS ............................................................................................................................... 5
1. INTRODUCTION ....................................................................................................................................... 6
1.1 Background ........................................................................................................................................ 6
1.1.1 Refractory asthma ............................................................................................................... 6
1.1.2 clinical need and burden of disease .................................................................................... 8
1.1.3 Relevant Guidelines and Initiatives ..................................................................................... 8
1.1.4 REVIEW aims ........................................................................................................................ 8
2. METHODS ................................................................................................................................................ 9
2.1.1 Background and current practice ........................................................................................ 9
2.1.2 Expert engagement ............................................................................................................. 9
2.1.3 Filtration ............................................................................................................................ 10
3. RESULTS ................................................................................................................................................. 10
3.1 Overview ...................................................................................................................................... 10
3.1.2 Summary of Emerging Pharmacotherapies .............................................................................. 11
3.1.3 Programmes ............................................................................................................................. 13
3.1.4 Diagnosis and Monitoring ........................................................................................................ 13
3.1.5 Devices ...................................................................................................................................... 13
3.1.6 General comments on Emerging technologies ........................................................................ 14
4. DISCUSSION ........................................................................................................................................... 16
REFERENCES .............................................................................................................................................. 17
APPENDICES ............................................................................................................................................... 18
Appendix 1: Search strategy and terms ....................................................................................... 18
Appendix 2: Technology tables ..................................................................................................... 20
Appendix 3: Research Priorities …………………………………………………………………………………………… ..33

4
EXECUTIVE SUMMARY
This horizon scanning review has been conducted by the NIHR Horizon Scanning Research and Intelligence Centre (HSRIC) and informed by consultation with clinical experts for the NIHR Efficacy and Mechanism Evaluation (EME) Programme. The aim of the review was to identify technologies and programmes that may be of relevance in the future diagnosis, treatment, monitoring and management of refractory asthma. Refractory asthma is a poorly understood heterogeneous disease in which adequate asthma control cannot be achieved in a substantial proportion of patients. Patients with refractory asthma do not respond to current standard therapy, and so experience persistent symptoms, airflow obstruction and frequent exacerbations. A wide range of sources were searched to identify emerging technologies, these included horizon scanning databases, clinical trial registries, commercial databases, news sources and bibliographical databases. These sources were searched using search terms agreed with EME. Once the initial results had been collected they were filtered using pre-determined inclusion and exclusion, leaving a list of technologies believed to be in development for refractory asthma. Sixty-six emerging technologies relevant to this patient group were identified; fifty-one drugs, five programmes, five technologies for diagnosis and monitoring and five medical devices. A detailed table of these technologies was sent to clinical experts and a representative from Asthma UK, who were asked to comment on the innovation of the technologies, user acceptability, the potential benefits of these emerging technologies and potential barriers to their adoption by the NHS. A number of novel therapies and technologies that are in development for refractory asthma were identified. The majority of emerging technologies identified were drugs. Experts indicated that until these individual technologies are fully developed and in use across the UK it is difficult to ascertain if patients with refractory asthma will derive any benefit from them, or if they will be an acceptable treatment option. It is thought that user co-creation would lead to more successful treatment development. Despite the unmet clinical need therapeutic advances for clinical use in asthma have been slow, this is particularly the case for patients with refractory disease. The heterogeneity associated with asthma is considered to be one of the key factors hindering research progress. Current clinical research is focused on overcoming this by grouping refractory asthma patients into clinically meaningful subphenotypes. This grouping may help to identify the patients most likely to benefit from treatment with the novel, often expensive treatments in development.

5
ACKNOWLEDGEMENTS
NIHR HSRIC review team:
Beth Boddice, Horizon Analyst
Dr Sue Simpson, Reviews Team lead
Dr Derek Ward, Medical Advisor
The following experts contributed to the review:
Professor Liam Heany, Professor of Respiratory Medicine, Queen’s University
Belfast.
Professor Stephen Holgate, Medical Research Council Clinical Professor of
Immunopharmacology and Honorary Consultant Physician within Medicine at the
University of Southampton.
Professor Ian Sabroe, Professor of Inflammation Biology Co-Director, Medical
Humanities, Sheffield.
Dr Erika Kennington, Head of Research, Asthma UK.
The NIHR Horizon Scanning Research & Intelligence Centre is grateful to all those who helped us to include both a healthcare professionals’ and potential users’ perspective in this report. We thank them for their time and valuable contributions.

6
1. INTRODUCTION
This horizon scanning review conducted by the NIHR Horizon Scanning Research and Intelligence Centre (HSRIC) and informed by consultation with clinical experts, provides information for the MRC/NIHR Efficacy and Mechanism Evaluation (EME) Programme about technologies and programmes that may be of relevance in the future diagnosis, treatment, monitoring and management of refractory asthma.
1.1 BACKGROUND
1.1.1 REFRACTORY ASTHMA
Refractory asthma is a poorly understood, poorly defined, complex heterogeneous disease in which adequate asthma control cannot be achieved or sustained in a substantial proportion of patients1,2. Refractory asthma encompasses a variety of sub phenotypes of asthma that do not respond to current standard therapy1, resulting in persistent symptoms, airflow obstruction and/or exacerbations. Definitions: Distinguishing refractory asthma from difficult to treat asthma is important, as it identifies the patients who may benefit from novel, often expensive treatments1. A number of definitions can be found in the literature: In 2009, an expert panel proposed a World Health Organisation (WHO) definition of asthma
severity and control and distinguished three types of severe asthma3.
1) Untreated severe asthma 2) Difficult to treat severe asthma (due to adherence issues, inappropriate or incorrect use
of medicines, environmental triggers or co-morbidity) 3) Treatment-resistant severe asthma (including asthma for which control is not achieved
despite the highest level of recommended treatment or asthma which is controlled only with the highest level of recommended treatment).
The National Institute for Health and Care Excellence (NICE) quality standard for asthma
uses the term difficult asthma to describe asthma in adults with persistent symptoms despite treatment at steps 4 or 5 of the British Thoracic Society (BTS)/Scottish Intercollegiate Guidelines Network (SIGN) guideline plus one of the following4:
An event of acute severe asthma which is life threatening, requiring invasive ventilation
within the last ten years.
Requirement for maintenance oral steroids for at least six months at a dose equal to or
above 7.5mg of prednisolone per day or a daily dose equivalent of this calculated over
twelve months.
Two hospitalisations within the last twelve months in patients taking and adherent to
high dose inhaled steroids (greater than or equal to 1,000micrograms of
beclometasone or equivalent)
Fixed airflow obstruction, with a post bronchodilator forced expiratory volume in one
second (FEV1) less than 70% of predicted normal.
1 High doses of inhaled or oral glucocorticosteroids in combination with long-acting β2-agonists (LABA).

7
Difficult asthma in children is defined in the quality standards as: those receiving treatment at stage 3 or 4 of the BTS/SIGN guideline, but still symptomatic, particularly if high dose inhaled steroids have been used, and all children being treated at stage 5 (aged 5 years and older), or stage 4 (younger than 5 years) as per the BTS/SIGN guideline4. Difficult asthma as defined by NICE is likely to include patients who have co-morbidities and poor therapy adherence and use4.
The definition used by NHS England (NHS Standard Contract for Respiratory: severe
asthma) was developed by the Innovative Medicines Initiative5. They suggest that the subgroup with truly severe refractory asthma can be defined and distinguished from patients with ‘problematic’ or ‘difficult’ asthma. The term ‘problematic severe asthma’ includes all asthma and asthma-like symptoms that remain uncontrolled despite the prescription of high-intensity asthma treatment. It is an umbrella term that comprises patients with ‘difficult’ asthma as well as patients with ‘severe refractory’ asthma. The term ‘difficult asthma’ is reserved for asthma that remains uncontrolled despite the prescription of high-intensity asthma treatment due to:
• Persistently poor adherence • Psychosocial factors, dysfunctional breathing, vocal cord dysfunction • Persistent environmental exposure to allergens or toxic substances • Untreated or under treated co morbidities such as chronic rhinosinusitis, reflux disease
or obstructive sleep apnoea syndrome
They recommend that the term ‘severe refractory asthma’ be reserved for patients with asthma in whom alternative diagnoses have been excluded; co morbidities have been treated; trigger factors have been removed (if possible); and adherence with treatment has been checked, but still have poor asthma control, or frequent severe exacerbations, despite the prescription of high-intensity treatment, or can only maintain adequate control when taking systemic corticosteroids5.
The Refractory Asthma Stratification Programme (RASP-UK) have proposed a clinical
stratification of the population of patients with severe asthma into those with corticosteroid-responsiveness (“T2-High” severe asthma) and those with corticosteroid unresponsive disease (“T2-Low” severe asthma)9.
Phenotypes It is recognised that the group of patients with refractory asthma is far from homogeneous and may be subdivided into different phenotypes1. The Severe Asthma Research Programme (SARP) has identified five distinct clinical phenotypes of asthma, these phenotypes are characterised by a number of clinical and physiological features which are thought to reflect underlying immuno-pathologies,. Three of these phenotypes are associated with refractory asthma1:
1) Early onset, severe allergic asthma with low FEV1. 2) Late onset, non-atopic, steroid dependent asthma with fixed airway obstruction. 3) Late onset asthma with reduced lung function in older women with obesity .
Much of the research in this area is focused on clinical phenotypes, characterisation of which may help understand underlying physiology and be used to target treatments1. The ‘Unbiased Biomarkers for the Prediction of Respiratory Disease Outcomes’ (U-BIOPRED) project is being conducted across 11 European countries to identify the distinct phenotypes of severe asthma6.

8
1.1.2 CLINICAL NEED AND BURDEN OF DISEASE
Clinical Need and Burden of Disease The global prevalence of asthma is estimated to be 300 million3, with 18% of the UK population having a confirmed diagnosis5
. The lack of a consistent definition means estimates of the true size of the sub-group of patients with refractory asthma is unknown1. There is a significant economic burden associated with refractory asthma. In a recent study, which used data from the British Thoracic Society Difficult Asthma Registry, treatment costs for patients in the UK were estimated to be £2,912-£4,217 per patient7. Most of this cost was attributed to medication, although management of frequent exacerbations is also significant. Treatment for patients with refractory asthma was reported to cost more compared to other chronic conditions including chronic obstructive pulmonary disease (COPD), stroke and type 2 diabetes7. Results from this study suggest that effect of interventions or new therapies should consider a medication reduction strategy7.
1.1.3 RELEVANT GUIDELINES AND INITIATIVES
NICE Quality Standard (QS25) Asthma, February 2013 (Quality statement 11 specifically relates to difficult asthma)4.
British Thoracic Society/Scottish Intercollegiate Guidelines Network. British Guideline on the management of asthma, October 20148.
There are a number of existing research initiatives focusing on asthma including:
The NIHR Translational Research Partnership (TRP) in inflammatory respiratory diseases which considers studies in asthma amongst other inflammatory conditions (http://www.nocri.nihr.ac.uk/services/translational-research-partnerships/inflammatory-respiratory-disease/) .
Three NIHR biomedical research units (BRUs) have a focus on respiratory disease, each of which has a specific focus on severe asthma - Leicester NHS Trust and The University of Leicester; The Royal Brompton and Harefield NHS Foundation Trust with Imperial College London; and Southampton University NHS Trust and the University of Southampton.
The MRC has recently jointly funded the Refractory Asthma Stratification Programme (RASP-UK) a partnership between The MRC, Asthma UK and a group of pharmaceutical companies (http://www.rasp.org.uk/). The objective of this programme is to change the management of severe asthma to a stratified approach9.
Asthma UK funds a number of research projects and two research centres, and is involved with a variety of external projects such as RASP-UK and the European Asthma Research and Innovation Partnership (EARIP) (https://www.asthma.org.uk/research/future/).
1.1.4 REVIEW AIMS
To identify new and emerging technologies for the diagnosis, treatment, monitoring and management of refractory asthma. Inclusion criteria
Technologies in development for the diagnosis, treatment, monitoring and management of refractory asthma.
Technologies aimed at adults and children.
All developers (commercial sponsors, academic research institutes etc.)
Technologies being developed in all countries.

9
Technologies in all stages of clinical development, but with a focus on developments in phase I and II.
Exclusion criteria
Technologies in development for other types of asthma (e.g. acute asthma, unless the technologies are also being specifically targeted at patients with refractory disease)
Technologies which are already widely used for this patient group within the NHS.
2. METHODS
2.1.1 BACKGROUND AND CURRENT PRACTICE
We initially undertook scoping searches to obtain background information on refractory asthma including clinical need, burden of disease and the various terms and definitions used in relation to this patient group (refractory asthma, severe asthma, persistent asthma, difficult to control asthma, etc.). This helped us to develop a list of appropriate search terms and to formulate our search strategy. At this point we also researched the established care pathway and current treatments being used to manage refractory asthma. Identification of relevant technologies We developed a search strategy to identify relevant new and emerging technologies the sources used included:
a) Bibliographical databases (e.g. Medline). b) Clinical trial registries: ClinicalTrials.gov, UKCRN portfolio database and WHO
International Clinical Trials registry platform (ICRTP). c) Commercial R&D databases: Adis Insight, Pharmaprojects and Globaldata. d) Horizon scanning databases/websites e.g. HSRIC internal database, AHRQ (US),
CADTH (Canada), HPACT (Australia). e) News sources e.g. Clinica. f) Relevant UK and International professional organisations.
These online sources were searched using the search terms agreed with EME in the initial protocol. Further information on the search strategy and search terms used are provided in Appendix 1.
2.1.2 EXPERT ENGAGEMENT
Five clinical experts and the Head of Research at Asthma UK were invited and agreed to contribute to the horizon scanning review. Initially those involved were asked to suggest any new and emerging technologies for refractory asthma that they were aware of. Later in the review they were sent tables of identified technologies and asked to provide their comments on:
Innovation of the technologies.
Issues around user acceptability.
Potential benefits for patients, carers and the NHS.
Potential barriers to adoption into routine practice.
The evidence base so far and what kind of further research may be needed.

10
2.1.3 FILTRATION
Primary filtration A first filtration of the long list of identified potential new and emerging technologies was carried out by checking the initially available information against our inclusion and exclusion criteria, and also removing any obvious duplicates. Secondary filtration Technologies remaining after the final filtration were more closely researched to confirm that they were not duplicates and that they met the inclusion and exclusion criteria by gaining further information on : development status, indication, status of any clinical trials and to check drug codes and names (to eliminate overlap/duplication). In addition, information was collected, where available on estimated licence or launch dates.
3. RESULTS
3.1 OVERVIEW
Figure 1 details the number of technologies identified and excluded throughout the identification and filtration process. We identified 66 emerging technologies that met our inclusion criteria; 51 drugs, five programmes, five technologies for diagnosis and monitoring and five medical devices. We excluded technologies not specific to this patient group as far as possible, however some technologies thought to be in development for an undefined asthma indication were included, either because the specific patient group had not yet been established, or because we required further information about the technologies to exclude them. This is particularly the case for drugs in phase I (11 technologies) or unknown clinical trial phases (four technologies), as well as one of the devices identified. Appendix 2 includes three technology tables that provide details of the identified technologies. These tables were sent to our expert advisory group and any comments they provided about specific technologies have been included in the tables. Furthermore general comments about emerging technologies for refractory asthma have been included at the end of the results section.

11
Figure 1: Identification and Filtration Process
included
Potential technologies from initial search results
(n = 1,138)
Non-relevant & duplicate results removed during
identification (n =507)
Technologies (n =631)
Iden
tifi
cati
on
Technologies (n =313)
Technologies excluded based on titles/brief
information (n = 318)
Technologies (n = 131)
P
rim
ary
Filt
rati
on
Se
con
dar
y fi
ltra
tio
n
Technologies excluded/not relevant or duplicate based
on further information (n = 182)
Technologies included in the final report
(n = 66)
Tech
no
logi
es
Technologies excluded following further
investigation (n= 65)

12
3.1.2 SUMMARY OF EMERGING PHARMACOTHERAPIES
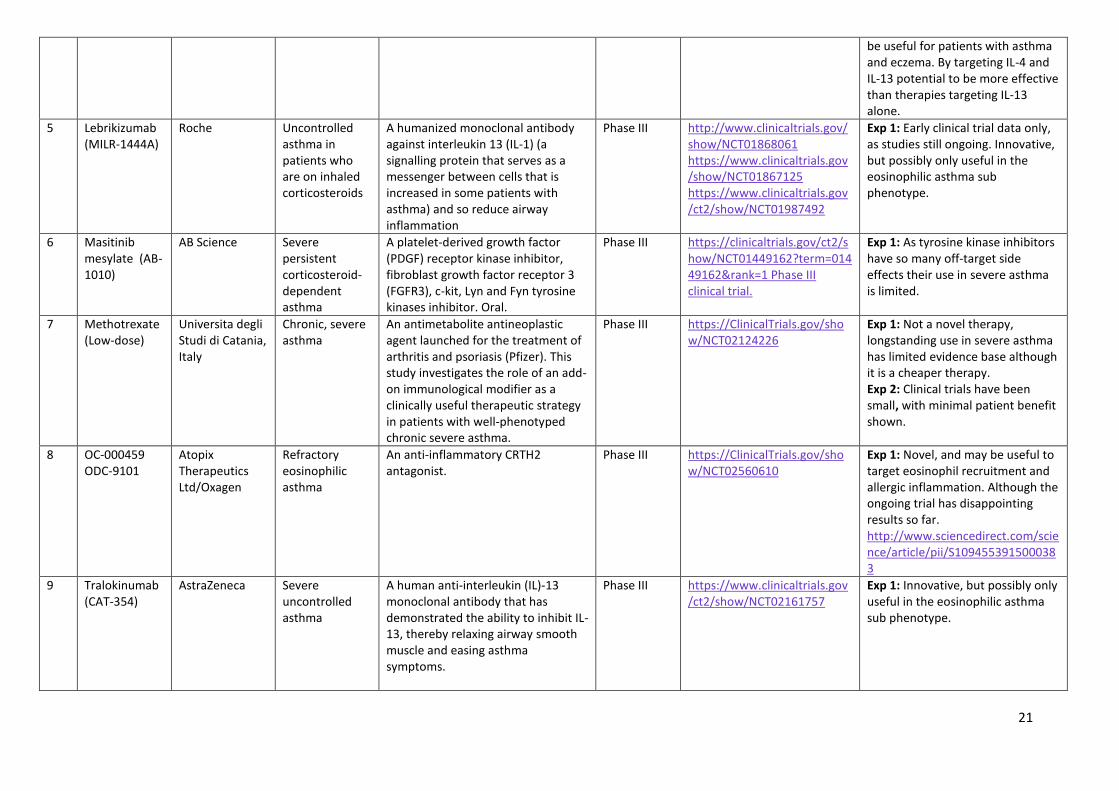
Pre-registration Mepolizumab and reslizumab, two anti-interleukin monoclonal antibodies, are the closest to being available for clinical use for the treatment of severe or inadequately controlled asthma. Mepolizumab is currently approved in the EU for severe refractory asthma and severe eosinophilic asthma, although it is still undergoing NICE appraisal. Publication of this appraisal is anticipated in July 201610. Reslizumab is pre-registration in the EU for inadequately controlled asthma in patients with elevated blood eosinophils. Phase III There are seven drugs in phase III trials, four of which are monoclonal antibodies (benralizumab, dupilumab, lebrikizumab and tralokinumab). The other three drugs are masitinib (a platelet derived growth factor), methotrexate (an antimetabolite anti-neoplastic agent) and an oral small molecule prostaglandin D2 (CRTH2) antagonist (OC-000459). Phase II The majority of drugs currently in development for refractory asthma are in ongoing phase II clinical trials. We identified 38 technologies in phase II development for this patient group, although for some technologies, the exact indication for which they will be licensed is not yet confirmed.
Severe/severe refractory asthma - There are eight drugs in phase II trials for severe
asthma: a CRH2 antagonist (fevipiprant), a calcium antagonist (gallopamil), a human anti-
TNF alpha antibody (golimumab), an oral signal transduction inhibitor (imatinib mesylate),
a highly selective potent agonist for peroxisome proliferator activated receptor-gamma
(pioglitazone), a combination of roflumilast and montelukast, aerolised carbon dioxide
and nebulised perfluorooctyl (S1226) HMG COA reductase inhibitors (statins) are also in
phase II trials for severe asthma.
Inadequately/poorly controlled asthma - There are four drugs in phase II trials for
poorly controlled asthma, these include: an oral CRTH2 receptor agonist (ADC-3680),
allogeneic mesenchymal umbilical cord derived stem cells (intranasal mesenchymal
trophic factors), a high affinity immunoglobulin E inhibitor anti-IGE monoclonal antibody
(ligelizumab) and a fully humanised monoclonal antibody (MAb) against thymic stromal
lymphopoietin (tezepelumab).
Persistent Asthma - There are six drugs in development for persistent asthma at phase
II. These include: an oral CRTH2 agonist (ARRY-502), a humanised IgG1 MAb (BI-
655066), a phosphoinositide 3-kinase-delta inhibitor (GSK-2269557), a macrolide lactone
antibiotic and immunosuppressive (tacrolimus), a histamine H4 receptor agonist
(toreforant) and a drug with unidentified pharmacologic activity (MK-1029).
Moderate to severe asthma - There are seven phase II drugs in development for
moderate to severe asthma, these include: topical auricular anaesthesia of the vagus
nerve (antipyrine benzocaine otic solution); an adrenergic receptor agonist (bedoradine);
two different antisense oligonucleotides, one which binds to the mRNA for the common ß-
subunit of IL-3, IL-5 and GM-CSF, the other binds to the mRNA for the CCR3 receptor; an
oral inhibitor of 5-lipoxygenase activating protein (FLAP) (fiboflapon); a combination of
the antibodies VAK-694 and QAX-576, an interleukin 13 (IL13) and IL4 antagonist; and
OBX-258, an inhaled antisense molecule (DNAzyme) targeting GATA-3 (SB-010).

13
Asthma/chronic asthma - Pemirolast, a histamine release inhibitor, and RPL-554 a dual
type-3 and type-4 cyclic nucleotide phosphodiesterase, are both in phase II development
for asthma, and although we could not find information directly linking these drugs to the
treatment of severe asthma, they may be indicated for patients refractory to current
inhaled therapies.
Phase I/II and phase I There were 11 technologies identified in phase I/II or phase I clinical trials. We included one technology in a phase I/II trial (CNTO-3157), a monoclonal antibody targeting TLR3. The remaining 10 technologies are in phase I trials, and include four technologies with unidentified pharmacological activity (AZD-8871, BI-1021958, BI-1060469 and CNTO-7160). Other technologies at this phase include: a muscarinic agonist (AZD-8999), a small oral molecule that binds specifically to Nck and interferes with the interaction between TCR and Nck (AX-024 hydrochloride), a CD34+ regulatory cell therapy (CLBS-03), a phosphodiesterase type 4 (PDE4) inhibitor (HPP-737), an anti-IL-13 monoclonal antibody (MEDI-7836), and an inhibitor of cyrosolic phospholipase A2 (ZPL-5212372). Unknown Status We included four drugs with an unknown clinical trial status. Botulinum toxin type A, dabigatran (a direct thrombin inhibitor), macrolide antibiotics (e.g. azithromycin) and magnesium sulphate are all thought to be in development, with academic sponsors, for a range of asthma indications including vocal cord dysfunction, airway inflammation, severe asthma and severe asthma following standard treatment failure. These approaches represent the repurposing of well-established drugs not currently used in the management of airways disease and not licensed for the treatment of asthma.
3.1.3 PROGRAMMES
We identified five programmes relevant to this review. Two are listed in ClinicalTrials.gov as being in phase III trials: the effect of aerobic training and the effect of weight loss in obese patients with difficult to treat asthma. The other programmes: breathing retraining, a tailored pulmonary rehabilitation programme and a phenotype based management programme are in clinical trials, but their phase could not be determined. All of these programmes appear to be targeting patients with severe or difficult to treat asthma.
3.1.4 DIAGNOSIS AND MONITORING
We identified five technologies for the diagnosis and management of severe asthma. These included two theranostic assays intended to guide therapy with lebrikizumab and tralokinumab (including tests to determine levels of periostin and DPP4), all of which were in unknown phases of development. Swansea University are developing a miniaturised, low cost optical eNO sensor for home monitoring (a project funded by the NIHR i4i programme). Two other monitoring devices included are NIOX MINO a point of care test for assessing airway inflammation (this is currently available for clinical use in the UK) and a device for monitoring fractional exhaled nitric oxide (FENO), which is in ongoing trials.
3.1.5 DEVICES
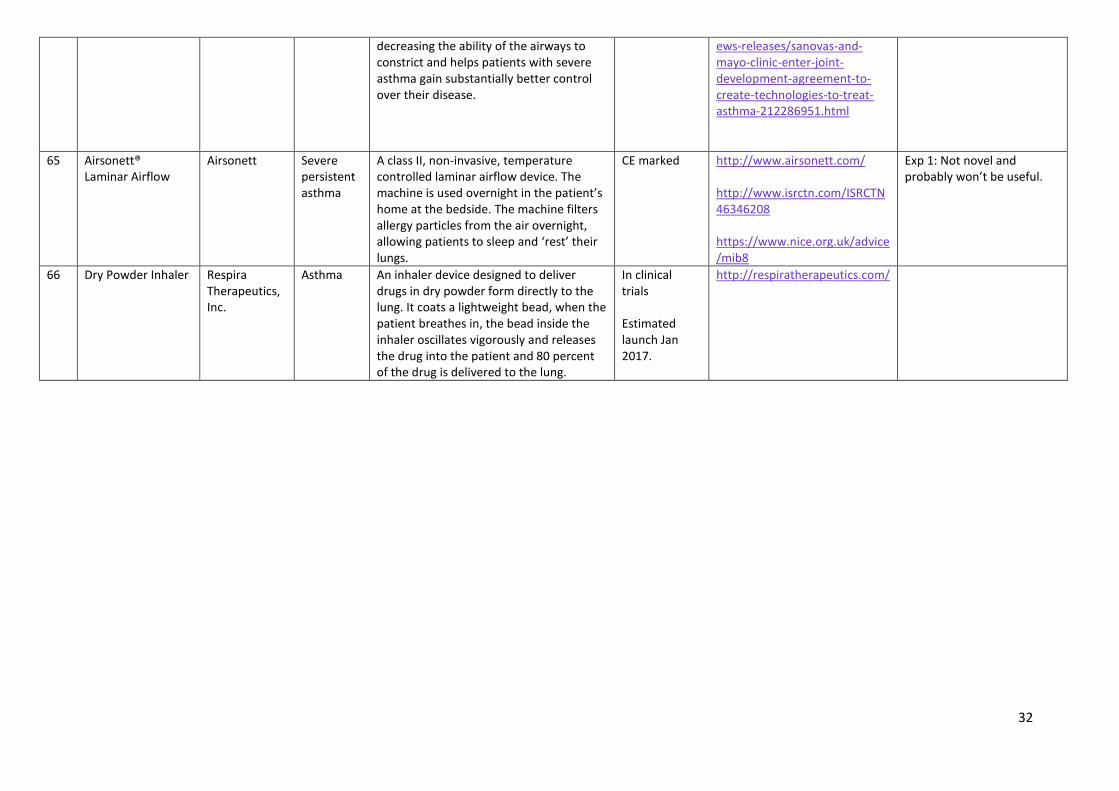
We identified five devices during our search. Two of these are CE marked and reportedly available for clinical use, the Alair system and Airsonett, both for severe asthma. An inhaler (dry powder inhaler device), a bronchial thermoplasty tool, and bronchial smooth muscle neutraliser are all expected to launch in 2017.
14
3.1.6 GENERAL COMMENTS ON EMERGING TECHNOLOGIES
The Head of Research at Asthma UK provided input on the development of technologies for asthma that have been informed by a number of research projects that Asthma UK either fund or are involved in. User acceptability Until technologies are fully developed it is difficult for patients to comment on how acceptable individual technologies are likely to be. User acceptability (particularly for drugs) in this patient group is influenced by factors including: type of formulation/method of administration, taste/texture (general pleasantness/unpleasantness of taking it), number of times it has to be taken per day, and the perceived improvement to quality of life (both immediate and longer term). The likelihood and severity of side effects associated with pharmacotherapy are also a significant consideration and will impact on adherence to medication regimes. Patients and professionals working with Asthma UK feel there is scope for, and would favour an approach where patients are involved in co-creating products. This may result in a reduction of the development of unsuitable treatments for asthma. Prioritising research The following information has been provided by Asthma UK in confidence and summarises findings from the European Asthma Research and Innovation Partnership (EARIP) Consortium, a 3-year project, supported by the European Commission. Diagnostics In 2015, a systematic review which summarises the state of play in asthma diagnostics was produced. From this, 21 possible research gaps were identified and a Delphi exercise undertaken to prioritise them in terms of potential impact of research investment in each technique or tool for people with asthma (see abstract in Appendix 3). After two rounds of the Delphi, 11 of these techniques/tools scored above 3 and were further discussed and ranked at a consensus workshop. These were:
Exhaled nitric oxide (FENO) as a tool to guide the adjustment of inhaled corticosteroid
dose in primary, secondary and tertiary care.
FENO as a tool in the diagnosis of asthma in patients older than 5 years of age.
Tools to measure volatile organic compounds (VOCs) in exhaled breath condensate.
Serum periostin as a biomarker of allergic asthma as a tool for diagnosis and/or
monitoring.
New biological markers of asthma (e.g. genomics, proteomics and metabolomics) as a
tool for diagnosis and/or monitoring.
New/improved tools to monitor lung function in the clinical setting.
Bronchodilation test as a tool for diagnosis and/or monitoring.
Assessing variability over time as a tool for diagnosis.
Refinement of symptom scores e.g. Asthma Control Test.
Prediction of future asthma in preschool children with reasonable accuracy.
Definition of standardised, normal values and cut-offs of lung functions tests at any age
in EU populations for diagnosis and/or monitoring.
Discussion was broadly positive about all of these priorities with the exception of FENO which was highly controversial; roughly equal proportions of the experts in the room were either very positive or very negative about the potential impact of FENO. Following discussion the top three areas were felt to be:

15
Prediction of future asthma in preschool children with reasonable accuracy.
New biological markers of asthma (e.g. genomics, proteomics and metabolomics) as a
tool for diagnosis and/or monitoring.
Tools to measure volatile organic compounds (VOCs) in exhaled breath condensate.
Monitoring In 2015, a systematic review which summarises the state of play in asthma monitoring was produced. From this, 19 possible research gaps were identified and a Delphi exercise undertaken to prioritise them in terms of potential impact of research investment in each technique or tool for people with asthma (see abstract in Appendix 3). After two rounds of the Delphi, 14 of these techniques/tools scored above 3 and were further discussed and ranked at a consensus workshop. These were:
New information technologies (internet, mobile phones, apps, etc...) to improve self-
management.
Strategies to achieve adherence to daily controller therapy in those with persistent
asthma.
Developing and evaluating multifaceted (complex) interventions to improve adherence.
Determine the effectiveness of goals set by the patients to improve self-management.
The impact (including cost-effectiveness) of shared decision making, including practical
approaches to delivery.
The determinants of good adherence with daily controller therapy.
Further investigation of factors affecting adherence in adolescent patients.
Tools to continually monitor adherence in real time (e.g. pharmacy collection, chips in
inhalers etc.).
Provision of personalised asthma self-management plans and education for all people
with asthma tailored to the individual and their condition.
The support of the healthcare system (both at national and local level) to implement
supported self-management.
Behavioural strategies included in educational interventions to improve patient
outcomes.
Incorporating shared decision making into practice to improve patient outcomes.
Annual checking of inhaler technique for all patients.
Integration of self-management into national asthma care policy, and training for all
professionals involved in asthma care to improve patient outcomes.
Following discussion the top three areas were felt to be:
Provision of personalised asthma self-management plans and education for all people
with asthma tailored to the individual and their condition. This should be supported by
the healthcare system (both at national and local level) and needs including training for
all professionals involved in asthma care
Behavioural strategies included in educational interventions to improve patient
outcomes
New information technologies (internet, mobile phones, apps, etc...) to improve self-
management. This would include tools to monitor adherence in real time, although with
a lesser importance.

16
Other research prioritises Other areas prioritised for research include:
A greater understanding of asthma triggers (including the role of infections, the indoor environment, the outdoor environment and the working environment) and how the individual patients respond to these triggers.
Being able to identify those at increased risk of asthma or needing urgent or emergency care for asthma.
Understanding different types of asthma (this has implications for the refractory asthma patient group and research into phenotypes) to personalise treatment.
Understanding when and how to change regular medication i.e. to step up or step down
4. DISCUSSION
We identified a number of interesting and novel therapies and technologies that are in development for refractory asthma. The majority of emerging technologies identified are drugs, but within these it was often difficult to ascertain the exact patient indication, particularly early in development. We also identified a number of programmes, diagnostics and medical devices in development for clinical use in this patient group. The main difficulty we encountered whilst conducting our search for emerging technologies was dealing with the numerous terms and definitions used to describe the refractory asthma patient group. Refractory asthma is a complex condition with no single agreed definition; therefore, the companies and research centres conducting trials within this area use a broad range of terms to describe and record the patient group under study. This made it difficult to exclude a number of technologies that didn’t have a clearly defined patient group. Despite the unmet clinical need, therapeutic advances for clinical use in asthma have been slow; this is particularly the case for patients with refractory disease. The heterogeneity associated with asthma is considered to be one of the key factors hindering research progress. Current clinical research is focused on overcoming this by grouping refractory asthma patients into clinically meaningful sub-phenotypes12-14. This grouping may help to identify the patients most likely to benefit from treatment with the novel, often expensive treatments in development.

17
REFERENCES
1. Reinier RL and Bel EH. Severe refractory asthma: an update. European Respiratory Review. 2013;
22: 227-235.
2. Heaney LG, Brightling CE et al. Refractory asthma in the UK: cross-sectional findings from a UK
multicentre registry. Thorax 2012; 70: 376-378.
3. Bush A and Zar HJ. WHO Universal Definition of Severe Asthma. Current opinion in allergy and
clinical immunology 2011; 2: 111-21.
4. National Institute for Health and Care Excellence. Asthma. NICE Quality Standard (QS25). London:
NICE; February 2013.
5. NHS England. NHS Standard Contract for Respiratory: severe asthma (adult). London: NHS England
2013.
6. U Biopred. What is the project? http://www.europeanlung.org/en/projects-and-research/projects/u-
biopred/what-is-the-project/ Accessed 25 September 2015.
7. O Neil S, Sweeny J et al. The cost of treating severe refractory asthma in the UK: an economic
analysis from the British Thoracic Society Difficult Asthma Registry. Throax 2015; 70: 376-378.
8. British Thoracic Society/Scottish Intercollegiate Guidelines Network. British Guideline on the
management of asthma (Revised 2014). SIGN 141. Edinburgh: Health Improvement Scotland;
October 2014.
9. Refractory Asthma Stratification Programme. http://www.rasp.org. Accessed 15 February 2016.
10. National Institute for Health and Care Excellence. Mepolizumab for treating severe eosinophilic
asthma. NICE Technology Appraisal in development. Expected July 2016.
11. Brusselle GG, VanderStichle C et al. Azithromycin for prevention of exacerbations in severe asthma
(AZISAST): a multicentre randomised double-blind placebo-controlled trial. Thorax 2013; 68: 322-
329.
12. Multidimensional endotypes of asthma: topological data analysis of cross-sectional clinical,
pathological, and immunological data. Hinks T, Zhou X, Staples K, Dimitrov B, Manta A, Petrossian
T, Lum P, Smith C, Ward J, Howarth P, Walls A, Gadola SD, Djukanović R. Lancet. 2015 Feb 26;
385 Suppl 1:S42. doi: 10.1016/S0140-6736(15)60357-9.
13. Hinks TS, Zhou X, Staples KJ, Dimitrov BD, Manta A, Petrossian T, Lum PY, Smith CG, Ward JA,
Howarth PH, Walls AF, Gadola SD, Djukanović R. Innate and adaptive T cells in asthmatic patients:
Relationship to severity and disease mechanisms. J Allergy Clin Immunol. 2015 Aug;136(2):323-33.
doi: 10.1016/j.jaci.2015.01.014. Epub 2015 Mar 5
14. Hinks TS, Brown T, Lau LC, Rupani H, Barber C, Elliott S, Ward JA, Ono J, Ohta S, Izuhara K,
Djukanović R, Kurukulaaratchy RJ, Chauhan A, Howarth PH. Multidimensional endotyping in patients
with severe asthma reveals inflammatory heterogeneity in matrix metalloproteinases and chitinase 3-
like protein 1. J Allergy Clin Immunol. 2016 Jan 28. pii: S0091-6749(15)03117-6. doi:
10.1016/j.jaci.2015.11.020. [Epub ahead of print]

18
APPENDICES
Appendix 1: Identification sources and search terms Source Website
General internet Website
Google https://www.google.co.uk/
ZETOC – British Library Database http://zetoc.jisc.ac.uk/
Horizon scanning databases
NIHR HSRIC ‘in-house’ technology database Not available online
ECRI Institute http://www.ecri.org
AHRQ Healthcare Horizon Scanning System
http://effectivehealthcare.ahrq.gov/index.cfm/who-is-involved-in-the-effective-health-care-program1/ahrq-horizon-scanning-system/
EuroScan www.euroscan.org
CADTH https://www.cadth.ca
NIHR BRCs, BRU, CRF, HTC and DEC dataset Not available online
Drug specific sources
Pharmaprojects https://citeline.com/products/pharmaprojects/
Adis http://bi.adisinsight.com/
Pharma Times http://www.pharmatimes.com/
Scrip http://www.scripintelligence.com/home/
MedTech specific sources
Clinica MedTech http://www.clinica.co.uk/
GlobalData Medical http://www.globaldata.com/
Medical News Today http://www.medicalnewstoday.com/
MedGadget http://www.medgadget.com/
Fierce Network – Fierce Diagnostics: Medical Imaging
http://www.fiercediagnostics.com/topics/medical-imaging
Clinical trial registries
ClinicalTrials.gov http://clinicaltrials.gov/
UKCRN portfolio database http://public.ukcrn.org.uk/search/
WHO International Clinical Trials registry platform (ICRTP)
http://apps.who.int/trialsearch/AdvSearch.aspx
Regulatory authorities
European Medicines Agency (EMA)
http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/landing/epar_search.jsp&mid=WC0b01ac058001d124
US Food and Drug Administration http://www.fda.gov/medicaldevices/productsandmedicalprocedures/
Bibliographic databases
Ovid MEDLINE(R) In-process & Other Non-indexed Citations (to current date)
http://www.elibrary.bham.ac.uk/

19
Search terms
Severe refractory asthma
Refractory asthma
Severe asthma
Difficult to control asthma
Difficult to treat asthma
Treatment resistant asthma
Problematic asthma
Persistent asthma
Other relevant terms included:
Diagnosis
Monitoring
Treatment
Management

20
Appendix 2: Technology Tables
Table 1: Pharmacotherapy No. Technology
Name Developer/ Sponsor
Indication Brief Description/Mechanism of action
Status Notes Advisory group comments
Licensed
1 Mepolizumab (Nucala; SB-240563; Bosatria)
GlaxoSmithKline Severe refractory asthma, severe eosinophilic asthma
An anti-interleukin-5 humanised IgG1 monoclonal antibody. Interleukin-5 stimulates the production, activation and maturation of eosinophils.
Licensed https://clinicaltrials.gov/ct2/show/NCT01000506?term=NCT01000506&rank=1 . Launched in US and approved in EU Still undergoing NICE appraisal.
Exp 1: Innovative. Biological therapies with once monthly administration have good tolerability and may be suitable for home administration. Barriers to use include: cost - may have to be given in hospital. However, it will be valuable in eosinophilic asthma.
Pre-registration
2 Reslizumab (Cinquil, SCH-55700, CDP-835)
Teva Pharmceuticals Ltd
Inadequately controlled asthma in patients with elevated blood eosinophils
An anti-interleukin-5 monoclonal antibody that stimulates the production, activation and maturation of eosinophils.
Pre-registration in EU
https://ClinicalTrials.gov/show/NCT01508936 https://ClinicalTrials.gov/show/NCT02559791
Exp 1: Similar benefits to mepolizumab - innovative with good tolerability, although clinical trials have possibly been less detailed.
Phase III
3 Benralizumab (BIW-8405)
AstraZeneca Adults and adolescents aged 12 years and over with uncontrolled asthma
A fully humanized anti-interleukin-5 receptor (IL-5R) alpha chain monoclonal antibody. Claims to directly deplete eosinophils, a class of white blood cell implicated in the pathology of asthma and other inflammatory diseases, and neutralises the activity of interleukin-5, which is believed to play a key role in the growth and development of eosinophils.
Phase III Launch expected in 2017.
Number of trials ongoing: https://ClinicalTrials.gov/show/NCT02322775. https://clinicaltrials.gov/ct2/show/NCT01928771 https://clinicaltrials.gov/ct2/show/NCT02075255 https://clinicaltrials.gov/ct2/show/record/NCT02417961
Exp 1: Interesting concept, novel idea. Has cost and accessibility limitations’, requiring hospital administration.
4 Dupilumab (REGN-668)
Sanofi, Regeneron Pharmaceuticals
Severe steroid dependent asthma
A fully human MAb targeting IL-4 receptor alpha (IL4Ra). It blocks both IL-4 and IL-13 signalling.
Phase III https://clinicaltrials.gov/ct2/show/NCT02528214
Exp 1: This therapy may be used as a total treatment plan for total atopic disease burden. This could
21
be useful for patients with asthma and eczema. By targeting IL-4 and IL-13 potential to be more effective than therapies targeting IL-13 alone.
5 Lebrikizumab (MILR-1444A)
Roche Uncontrolled asthma in patients who are on inhaled corticosteroids
A humanized monoclonal antibody against interleukin 13 (IL-1) (a signalling protein that serves as a messenger between cells that is increased in some patients with asthma) and so reduce airway inflammation
Phase III http://www.clinicaltrials.gov/show/NCT01868061 https://www.clinicaltrials.gov/show/NCT01867125 https://www.clinicaltrials.gov/ct2/show/NCT01987492
Exp 1: Early clinical trial data only, as studies still ongoing. Innovative, but possibly only useful in the eosinophilic asthma sub phenotype.
6 Masitinib mesylate (AB-1010)
AB Science Severe persistent corticosteroid-dependent asthma
A platelet-derived growth factor (PDGF) receptor kinase inhibitor, fibroblast growth factor receptor 3 (FGFR3), c-kit, Lyn and Fyn tyrosine kinases inhibitor. Oral.
Phase III https://clinicaltrials.gov/ct2/show/NCT01449162?term=01449162&rank=1 Phase III clinical trial.
Exp 1: As tyrosine kinase inhibitors have so many off-target side effects their use in severe asthma is limited.
7 Methotrexate (Low-dose)
Universita degli Studi di Catania, Italy
Chronic, severe asthma
An antimetabolite antineoplastic agent launched for the treatment of arthritis and psoriasis (Pfizer). This study investigates the role of an add-on immunological modifier as a clinically useful therapeutic strategy in patients with well-phenotyped chronic severe asthma.
Phase III https://ClinicalTrials.gov/show/NCT02124226
Exp 1: Not a novel therapy, longstanding use in severe asthma has limited evidence base although it is a cheaper therapy. Exp 2: Clinical trials have been small, with minimal patient benefit shown.
8 OC-000459 ODC-9101
Atopix Therapeutics Ltd/Oxagen
Refractory eosinophilic asthma
An anti-inflammatory CRTH2 antagonist.
Phase III https://ClinicalTrials.gov/show/NCT02560610
Exp 1: Novel, and may be useful to target eosinophil recruitment and allergic inflammation. Although the ongoing trial has disappointing results so far. http://www.sciencedirect.com/science/article/pii/S1094553915000383
9 Tralokinumab (CAT-354)
AstraZeneca Severe uncontrolled asthma
A human anti-interleukin (IL)-13 monoclonal antibody that has demonstrated the ability to inhibit IL-13, thereby relaxing airway smooth muscle and easing asthma symptoms.
Phase III https://www.clinicaltrials.gov/ct2/show/NCT02161757
Exp 1: Innovative, but possibly only useful in the eosinophilic asthma sub phenotype.

22
Phase II
10 ADC-3680 Pulmagen Therapeutics
Inadequately controlled asthma
An oral small-molecule prostaglandin D2 (CRTH2) receptor antagonist.
Phase II https://www.clinicaltrials.gov/ct2/show/NCT01730027
Exp 1: Novel, and may be useful to target eosinophil recruitment and allergic inflammation.
11 Antipyrine-benzocaine otic solution.
Global United Pharmaceutical Corporation
Moderate to severe asthma
The hypothesis is that topical auricular anaesthesia of the vagus nerve decreases the need for the usage of rescue inhalers in moderate to severe asthma in adults.
Phase II https://ClinicalTrials.gov/show/NCT02153541
Exp 1: Novel, but seems unlikely to work.
12 ARRY-502 Array BioPharma
Persistent asthma
An oral CRTH2 receptor antagonist. Development is suspended until a collaboration is finalized.
Phase II https://ClinicalTrials.gov/show/NCT01561690
Exp 1: Novel, and may be useful to target eosinophil recruitment and allergic inflammation
13 ASM-8 Pharmaxis Moderate to severe asthma
Antisense therapy consisting of 2 different oligonucleotides. One of the oligonucleotides binds to the mRNA for the common ß-subunit of IL-3, IL-5 and GM-CSF; the other binds to the mRNA for the CCR3 receptor. Inhaled as a solution.
Phase II https://www.clinicaltrials.gov/ct2/show/NCT01380236
Exp 1: CCR3 targeting may be useful as it prevent eosinophil recruitment; however, it is difficult to deliver drugs to the eosinophils.
14 Bedoradrine MediciNova Moderate to severe asthma
A novel, highly selective ß2-adrenergic receptor agonist. Intravenous.
Phase II http://investors.medicinova.com/phoenix.zhtml?c=183833&p=irol-newsArticle&ID=1724606&highlight=). http://www.kissei.co.jp/e_contents/rd/pipeline/ https://www.clinicaltrials.gov/ct2/show/NCT00679263
Exp 1: There are already a number of good beta agonists available and it is highly unlikely that this intravenous administration would be used outside of accident and emergency departments.
15 BI-655066 Boehringer Ingelheim
Severe persistent asthma
A humanized IgG1 monoclonal antibody that binds and neutralizes the p19 subunit of IL-23. Interleukin 23 antagonist.
Phase II https://ClinicalTrials.gov/show/NCT02443298
Exp 1: In very early development, but has potential to be a novel, treatment for non-eosinophilic asthma.

23
16 Fevipiprant (QAW-039)
Novartis Severe uncontrolled asthma
A CRTH2 antagonist. Oral. Phase II http://www.clinicaltrials.gov/ct2/show/NCT01253603 http://clinicaltrials.gov/ct2/show/NCT01785602 http://www.clinicaltrials.gov/ct2/show/NCT01804400
Exp 1: In very early development, but has potential to be a novel, treatment for non-eosinophilic asthma
17 Fiboflapon (GSK-2190915)
GlaxoSmithKline Moderate to severe asthma who have elevated sputum neutrophils
An oral inhibitor of 5-lipoxygenase-activating protein (FLAP). It prevents the synthesis of leucotrienes that trigger inflammation.
Phase II https://www.clinicaltrials.gov/ct2/show/NCT00812929
Exp 1: Targeting leukotrienes as has so far not been effective.
18 Gallopamil Abbvie University Hospital, Bordeaux
Severe asthma Calcium antagonist launched for angina, trialled to evaluate the effect of gallopamil on airway remodeling in patients with severe asthma.
Phase II https://ClinicalTrials.gov/show/NCT00896428 https://www.ncbi.nlm.nih.gov/pubmed/25633090?dopt=Abstract
Exp 1: Doubt this will be useful. Exp2: Current clinical trials have been stopped early due to safety issues.
19 Golimumab, (CNTO-148)
Merck and Co. /Centocor
Severe persistent asthma
A human anti-TNF-alpha antibody, administered subcutaneously.
Phase II EUCTR2004-000046-21-HU. https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2004-000046-21 https://clinicaltrials.gov/ct2/show/NCT00207740
Exp 1: Previous studies with anti-TNF (etanercept) have not been promising.
20 GSK-2269557 GlaxoSmithKline Persistent, uncontrolled asthma
Highly selective inhaled phosphoinositide 3-kinase-delta (PI3K-delta) inhibitor. Inhaled powder.
Phase II https://clinicaltrials.gov/ct2/show/NCT02567708
Exp 1: Novel and interesting, but involves many signalling pathways.
21 Imatinib mesylate (Glivec, Gleevec, Zoleta)
Brigham and Women's Hospital, Harvard Clinical Research Institute,
Severe refractory asthma, poorly controlled
An oral signal transduction inhibitor, developed by Novartis as an anticancer. It is a specific inhibitor of Bcr-Abl tyrosine kinase, PDGF-associated tyrosine kinase, and c-kit kinase.
Phase II https://ClinicalTrials.gov/show/NCT01097694
Exp 1: Not novel, numerous side effects and not useful for this patient group.

24
National Heart, Lung, and Blood Institute (all US)
22 Intranasal mesenchymal trophic factors
Translational Biosciences
Poorly controlled asthma
Allogeneic mesenchymal trophic factors derived from human umbilical cord tissue-derived mesenchymal stem cells. Intranasal infusion
Phase II http://clinicaltrials.gov/ct2/show/NCT02192736
Exp 1: Novel, but too speculative.
23 L-arginine supplements
University of California, National Institute of Health (NIH), National Heart Lung and Blood Institute National
Moderate to severe asthma
Nitric oxide is an important marker of airway inflammation in asthma. Nitric oxide may have a protective role in patients with moderate to severe asthma. The investigators believe that a natural amino acid, L-arginine, that augments nitric oxide levels can decrease asthma exacerbations and improve the asthma care of moderate to severe asthma patients.
Phase II https://ClinicalTrials.gov/show/NCT00280683 http://grantome.com/grant/NIH/R01-HL105573-03
Exp 1: Not novel, although not tried on this patient group yet, but probably unlikely to be useful.
24 Ligelizumab (QGE-031)
Novartis Asthma in patients not adequately controlled by other medications
A high affinity immunoglobulin E inhibitor (anti-IgE) monoclonal antibody.
Phase II https://www.clinicaltrials.gov/ct2/show/study/NCT02336425 https://www.clinicaltrials.gov/ct2/show/NCT01716754
Exp 1: Could be useful, this pathway is already targeted clinically with omalizumab, but competitor molecules are needed.
25 MK-1029 Merck & Co. Persistent asthma that is not controlled with montelukast
Unidentified pharmacological activity. Oral.
Phase II https://ClinicalTrials.gov/show/NCT01624974.
26 Pemirolast (CRD-007)
RSPR Pharma Asthma Histamine release inhibitor. Oral tablet. Phase II trial in Denmark for asthma where patients still have reversibility despite inhaled therapy with both steroids and LABA. No suggestion that the asthma is severe, but potentially refractory to current inhaled therapies
Phase II https://www.clinicaltrialsregister.eu/ctr-search/trial/2011-004667-76/SE). https://clinicaltrials.gov/ct2/show/NCT02615080
Exp 1: Not going to be useful for this patient group.

25
27 Pioglitazone hydrochloride (Actos)
National Heart, Lung, and Blood Institute (NHLBI)
Severe refractory asthma
A highly selective and potent agonist for the peroxisome proliferator-activated receptor-Gamma (PPAR Gamma) Launched for diabetes type 2 (Takeda). Studies in murine models of allergic asthma have shown that PPAR Gamma agonists down-regulate allergen-mediated airway inflammation and airway hyper-responsiveness.
Phase II https://clinicaltrials.gov/show/NCT00994175
Exp 1: Not going to be useful for this patient group.
28 QBX-258 Novartis Pharmaceuticals
Moderate-to-severe asthma
A combination of antibodies VAK-694 and QAX-576. Interleukin 13 (IL13) and IL4 antagonist. IV infusion.
Phase II http://www.clinicaltrials.gov/ct2/show/study/NCT01479595
29 Roflumilast in combination with and montelukast
Takeda Pharma A/S
Severe uncontrolled asthma.
A combination of roflumilast a phosphodiesterase IV (PDE IV) inhibitor and montelukastoral a leucotriene D4 (LTD4) receptor antagonist.
Phase II https://clinicaltrials.gov/ct2/show/NCT01765192
Exp 1: There are too many side effects associated with PDE IV inhibitors.
30 RPL-554 Verona Pharma/ Vernalis
Chronic asthma A dual type 3 and type 4 cyclic nucleotide phosphodiesterase inhibitors (PDE3 and PDE4 inhibitor) that has bronchodilatory and anti-inflammatory actions and also the potential to stimulate increases in mucociliary clearance via its proven ability to activate Cystic fibrosis transmembrane conductance regulator (CFTR).
Phase II https://www.clinicaltrials.gov/show/NCT02427165
31 S-1226 SolAeroMed Inc.
Asthma (mild and severe), rescue therapy
Consists of aerosolized carbon dioxide (CO2) and nebulised perfluorooctyl bromide (perflubron delivered via inhalation.
Phase II Estimated launch Dec 2018.
http://www.solaeromed.com/
32 SB-010 Sterna Biologicals
Moderate-to-severe Th2-driven asthma
An inhaled antisense molecule (DNAzyme) targeting GATA-3.
Phase II https://clinicaltrials.gov/ct2/show/NCT01577953?term=SB-010&rank=1 http://www.sterna-biologicals.com/pipeline/disease-areas.html#asthma

26
33 Statins –Simvastatin Atorvastatin
Various Severe asthma A HMG CoA reductase inhibitor. Phase II https://ClinicalTrials.gov/show/NCT02433535 https://ClinicalTrials.gov/show/NCT01266434 https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12607000179437 http://bmjopen.bmj.com/content/3/8/e003314.full
Exp 1: Not novel, or useful for this patient group.
34 Tacrolimus, tacrolimus inhalation aerosol
Fujisawa GmbH Moderate to severe persistent asthma. Add on therapy to LABA and ICS
Tacrolimus is a macrolide lactone antibiotic with potent immunosuppressive activity. It acts primarily on CD4+ T helper lymphocytes by inhibiting the production of lymphokines, which are required for cell growth and differentiation, principally interleukin-2, at the transcriptional level
Phase II EUCTR2004-002078-45-CZ. https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2004-002079-18
Exp 1: May be useful in some patients, but immunosuppression has not been highly successful.
35 Tezepelumab, AMG-157
Amgen Astra Zenenca
Inadequately controlled, severe asthma
A fully-human MAb against thymic stromal lymphopoietin (TSLP). It blocks the interaction of TSLP with TSLPR. Injectable.
Phase II https://ClinicalTrials.gov/show/NCT02054130
Exp 1: Unclear if this therapy will be important.
36 Toreforant (JNJ-38518168)
Janssen Research & Development, LLC Johnson & Johnson
Uncontrolled, persistent asthma
A histamine H₄ receptor antagonist Phase II http://clinicaltrials.gov/ct2/show/NCT01823016; https://www.clinicaltrialsregister.eu/ctr-search/search?query=2012-004920-39).
Exp 1: Will probably not be useful in this patient group.
Phase I
37 CNTO-3157
MorphoSys/ Johnson & Johnson
Asthma A fully-human monoclonal antibody, targeting TLR3.
Phase I/II http://www.clinicaltrials.gov/ct2/show/NCT01195207
Exp 1: Novel, but unknown potential.
38 AZD-8871 AstraZeneca Asthma Unidentified pharmacological activity. Inhaled powder.
Phase I https://clinicaltrials.gov/ct2/show/NCT02573155

27
39 AZD-8999 AstraZeneca Asthma A muscarinic antagonist-ß 2 agonist (MABA).
Phase I http://www.astrazeneca-annualreports.com/2014/assets/pdf/Therapy_Area_Review.pdf
40 AX-024 hydrochloride
Artax Biopharma
Asthma A small oral molecule that binds specifically to Nck and interferes with the interaction between TCR and Nck.
Phase I http://www.clinicaltrials.gov/ct2/show/NCT02243683
41 BI-1021958 Boehringer Ingelheim
Asthma Unidentified pharmacological activity. Oral
Phase I https://www.clinicaltrials.gov/ct2/show/NCT01541488 https://www.clinicaltrials.gov/ct2/show/NCT02202512
42 BI-1060469 Boehringer Ingelheim
Asthma Unidentified pharmacological activity. Oral.
Phase I http://clinicaltrials.gov/show/NCT01971502 http://www.clinicaltrials.gov/ct2/show/NCT02126865)
43 CLBS-03 Caladrius Biosciences/NeoStem
Steroid resistant asthma
A CD4+ CD127lo/-CD25+ polyclonal T regulatory cell therapy.
Phase I http://www.caladrius.com/our-technologies/t-regulatory-cell-technology/
44 CNTO-7160
Johnson & Johnson
Asthma Unidentified pharmacological activity Phase I https://clinicaltrials.gov/ct2/show/study/NCT02345928
45 HPP-737 vTv Therapeutics
Asthma A novel, potent and selective orally administered phosphodiesterase type 4 (PDE4) inhibitor.
Phase I http://www.sec.gov/Archives/edgar/data/1641489/000156761915000955/s000971x4_s1a.htm). http://vtvtherapeutics.com/pipeline/hpp737
46 MEDI-7836
AstraZeneca Asthma An anti-IL-13 MAb-YTE. Phase I https://www.clinicaltrials.gov/ct2/show/NCT02388347
47 ZPL-5212372
Pfizer Asthma A potent and highly selective inhibitor of cytosolic phospholipase A2 (cPLA2).
Phase I
https://www.clinicaltrials.gov/show/NCT01415102

28
Status Not known
48 Botulinum toxin type A (Botox)
Professor Philip Bardin, Monash Medical Centre, Respiratory and Sleep Medicine
Vocal cord dysfunction in severe asthma
Botulinum Toxin Not known ACTRN12611001270909. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12611001270909
49 Dabigatran Academic Medical Center (AMC), Department of Respiratory Medicine
Airway inflammation and coagulation in severe corticosteroid dependent asthma.
Direct thrombin inhibitor. Not known NTR3312. http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=3312
50 Macrolide antibiotics e.g. azithromycin
University Hospital Ghent University of Nottingham
Severe, non-eosinophilic Asthma
Azithromycin is a semi-synthetic macrolide antibiotic.
Not known/ various
https://clinicaltrials.gov/show/NCT00760838 http://www.ncbi.nlm.nih.gov/pubmed/23291349 http://www.isrctn.com/ISRCTN93221282 http://www.thelancet.com/journals/lanres/article/PIIS2213-2600(14)70107-9/abstract
Exp 1: Maybe useful in neutrophilic asthma. Exp 2: Trial results demonstrated that azithromycin did not reduce the rate of severe exacerbations or lower respiratory tract infections in patients with severe asthma. However, the trial did show that azithromycin for non-esoiniophilic asthma including rate of infection and lung function, so treatment for this patient group warrants further study
11.
51 Magnesium sulphate (intravenous or inhaled)
Various e.g. individual clinician- Maureen Busuttil, Australia
Acute to moderate/ severe asthma following standard treatment failure.
Inorganic salt. Used in addition to standard care. A recent Cochrane review suggests there are potential benefits, but further trials are needed.
Not known https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12612000838819. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3269605/ http://www.evidentlycochrane.net/intravenous-magnesium-sulfate-adults-acute-asthma/

29
Table 2: Programmes
No. Intervention Developer/ Sponsor
Indication Brief Description Status Notes Advisory group comments
52 Effect of aerobic training in moderate or severe asthma
Instituto de Investigação em Imunologia
Moderate and severe asthma
Aerobic training, 30 minutes of breathing exercises twice a week over three months.
Phase III https://ClinicalTrials.gov/show/NCT02033122
53 Effects of weight loss in obese difficult-to-treat asthmatics
University of Sao Paulo General Hospital
Difficult to treat asthma
Weight loss programme: low caloric diet plus orlistat and sibutramine.
Phase III https://ClinicalTrials.gov/show/NCT01
54 Breathing retraining North West Lung Centre, South Manchester University Hospital NHS Trust.
Dysfunctional breathing in severe asthma
To improve thoracic-abdominal co-ordination and hence reduce breathlessness, through breathing retraining with a senior physiotherapist.
In clinical trials
ISRCTN92818360. http://isrctn.com/ISRCTN92818360
55 Asthma-tailored pulmonary rehabilitation programme
University Hospitals of Leicester NHS Trust (UK)
Severe asthma A feasibility study to inform the development of a multicentre randomised controlled trial of an asthma-tailored pulmonary rehabilitation programme versus usual care.
In clinical trials
http://public.ukcrn.org.uk/search/StudyDetail.aspx?StudyID=15370
56 Phenotype based management
Hospital John Hunter Hospital
Severe persistent asthma
Multidisciplinary phenotype based management for people with severe persistent asthma compared to usual care and its impact on health related quality of life.
In clinical trials
ACTRN12612000807853. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12612000807853

30
Table 3: Diagnosis and monitoring
No. Technology Name Developer/ Sponsor
Indication Brief Description Place in therapy
Status Notes Advisory group comments
57 Lebrikizumab companion diagnostic assay (see entry no. 5 in drugs table)
Roche Diagnostics
Severe asthma
Serum periostin levels companion diagnostic test. Enzyme linked immunosorbent assay (ELISA) designed to determine serum periostin levels in asthma patients and helps to guide treatment planning. It provides targeted therapy with lebrikizumab. It is performed on cobase601 analyser.
Diagnosis In clinical trials
http://roche.nsp-reports.ch/10/ar/diagnostics_en/roche_companion_diagnostics.htm http://www.roche.com/med_phc_bohen.pdf
58 Periostin and DPP4 based Companion Diagnostic Assay – tralokinumab (see entry no. 9 in drugs table)
Abbott Diagnostics
Severe asthma
A biomarker based diagnostic assay that measures serum levels of the proteins periostin and DPP4 (dipeptidyl peptidase-4), which have been identified as potential predictive biomarkers of up-regulated IL-13 in severe asthma. It helps in identifying patients who are most likely to benefit from tralokinumab.
Diagnosis In clinical trials
Estimated launch Jan 2020. https://www.astrazeneca.com/our-company/media-centre/press-releases/2015/astrazeneca-abbott-companion-diagnostic-tests-tralokinumab-severe-asthma-13052015.html
59 Minaturised, low-cost, optical eNO sensor for asthma monitoring
Swansea University
Asthma Prototype breath analyser. Elevated levels of nitrogen monoxide (NO) gas in exhaled breath are typically taken as an indication of the inflammation of a patient’s airways. Home monitoring of exhaled NO is generally considered to be prohibitively expensive, because of the high cost of instruments currently on the market. The aim of this work is to produce a cost-effective device.
Diagnosis and monitoring
In clinical trials
Funded by i4i http://www.nihr.ac.uk/funding/funded-research/funded-research.htm?postid=1843
60 NIOX MINO Aerocrine AB Asthma Point of care device for assessing airway inflammation in patients with asthma.
Diagnosis and Monitoring
Available for clinical use in the UK.
http://www.aerocrine.com/

31
61 Monitoring of exhaled nitric oxide (FENO)
Academic Medical Center (AMC), Amsterdam
Severe asthma
Monitoring of exhaled nitric oxide (FENO) to tailor the lowest effective dose of oral corticosteroids in severe asthma.
Monitoring In clinical trials
NTR1146. http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=1146
Exp 1: FeNo has some utility, although this is widely debated. It is widely available. Probably most useful in assessing compliance/adherence.
Table 4: Devices
No. Technology Name Developer/ Sponsor
Indication Brief Description Status Notes Advisory group comments
62 Alair™ System Boston Scientific Limited Assistance Publique - Hôpitaux de Paris
Severe uncontrolled asthma
Bronchial thermoplasty http://www.btforasthma.com/
CE marked In clinical trials
http://www.bostonscientific.com/en-US/products/bronchial-thermoplasty/alair-system.html. https://ClinicalTrials.gov/show/NCT01777360 https://clinicaltrials.gov/ct2/show/NCT01350414 Journal of Allergy & Clinical Immunology. 132(6):1295-302, 2013 Dec.
Exp 1: Likely to be useful in limited number of patients. Exp 2: Therapy is available.
63 Bronchial Smooth Muscle Neutralizer
Pulmogenix, Inc.
Severe asthma
Bronchial Smooth Muscle Neutralizer is a portable device intended for the treatment of asthma. It is designed to deliver a minute electrical charge to stop the bronchial smooth muscles from contracting. It involves the insertion of a catheter into the lung.
In clinical trials
Estimated launch April 2017
64 Bronchial thermoplasty tool
Sanovas Mayo Clinic
Severe asthma
Bronchial thermoplasty tool is a micro-invasive airway management device intended for bronchial smooth muscle modification. It is designed to deliver precisely controlled thermal energy to reduce excess airway smooth muscle associated with airway constriction in patients with asthma. It operates by
In clinical trials Estimated launch April 2017
http://www.sanovas.com/ http://www.fiercemedicaldevices.com/story/mayo-joins-sanovas-develop-lung-clearing-asthma-treatment/2013-06-20 http://www.prnewswire.com/n
32
decreasing the ability of the airways to constrict and helps patients with severe asthma gain substantially better control over their disease.
ews-releases/sanovas-and-mayo-clinic-enter-joint-development-agreement-to-create-technologies-to-treat-asthma-212286951.html
65 Airsonett® Laminar Airflow
Airsonett Severe persistent asthma
A class II, non-invasive, temperature controlled laminar airflow device. The machine is used overnight in the patient’s home at the bedside. The machine filters allergy particles from the air overnight, allowing patients to sleep and ‘rest’ their lungs.
CE marked http://www.airsonett.com/ http://www.isrctn.com/ISRCTN46346208 https://www.nice.org.uk/advice/mib8
Exp 1: Not novel and probably won’t be useful.
66 Dry Powder Inhaler Respira Therapeutics, Inc.
Asthma An inhaler device designed to deliver drugs in dry powder form directly to the lung. It coats a lightweight bead, when the patient breathes in, the bead inside the inhaler oscillates vigorously and releases the drug into the patient and 80 percent of the drug is delivered to the lung.
In clinical trials Estimated launch Jan 2017.
http://respiratherapeutics.com/

33
Appendix 3 – Research Priorities (abstracts for presentation at the American Thoracic Society conference in May 2016)
What are the priorities for future research into diagnostic tools for asthma? A pan-EU consensus exercise
ID 6049 What are the priorities for future research into diagnostic tools for asthma? A pan-EU consensus exercise A38-DIAGNOSTIC MARKERS OF ASTHMA AND COPD Thematic Poster Session SUNDAY, MAY 15, 2016 9:00 AM-4:15 PM
RATIONALE: The diagnosis of asthma is currently based on lung function, clinical history and physical examination and to date there are no accurate objective tests to confirm the diagnosis or to discriminate between different types of asthma. Here we review the state-of-the-art in asthma diagnosis and identify opportunities for future investment based on the likelihood of their successful development, potential for widespread adoption and their perceived impact on people with asthma. This is part of the FP-7-funded European Asthma Research and Innovation Partnership (EARIP) which aims to identify the investment required to bring about significant improvements in asthma outcomes in Europe.
METHODS: European experts on asthma diagnosis worked together to perform an evidence review of existing and novel asthma diagnostic techniques. 21 statements describing the likelihood that further investment in each technique would result in the development of simple, accurate, inexpensive, non-invasive diagnostic tool/s were extracted from the review. Using a two-stage e-Delphi process, a further group of 37 European asthma experts including health professionals, researchers, people with asthma and industry representatives were asked to rank the potential impact of research investment in each technique or tool (score 1-5; 1=very low, 5=very high). In a subsequent expert workshop, statements with a mean score> 3 were further ranked.
RESULTS: 25 and 16 responses were obtained respectively in the 1st and 2nd Delphi rounds. 11 statements scored >3 in the Delphi exercise and were further ranked. The resulting 3 most important statements ranked by experts were: “New biological markers of asthma (e.g. genomics, proteomics and metabolomics) as a tool for diagnosis and/or monitoring”, “Prediction of future asthma in preschool children with reasonable accuracy” and “Tools to measure volatile organic compounds (VOCs) in exhaled breath condensate”. Others included: Definition and standardised, normal values and cut-offs for lung function tests at any age; refinement of symptom scores to assess variability over time; new/improved tools to monitor lung function in the clinical setting; use of bronchodilation test; new biological markers of asthma (e.g. genomics, proteomics, metabolomics); serum periostin as a biomarker of allergic asthma and FeNO as a tool for diagnosis in under 5’s.
CONCLUSIONS: Through careful review and consensus-building among experts, we have identified the techniques most likely to lead to the development of reliable and accurate tools to diagnose asthma and to potentially discriminate between different sub-types of asthma. We will use this information to drive investment in research in these areas.

34
What are the priorities for research into asthma self-management tools: a pan-EU consensus exercise
ID 6016 What Asthma Self-Management Tools and Systems Should Have Higher Priority in Future Research: A Delphi Exercise from the EU A102-HIGHLIGHTS IN PATIENT-CENTERED RESEARCH: METHODS AND OUTCOMES Poster Discussion Session SUNDAY, MAY 15, 2016 2:15 PM-4:15 PM
RATIONALE: Optimisation of asthma self-management requires development of more effective tools that can be embedded in daily life and in healthcare systems. Here we review the state-of-the-art in asthma self-management in order to define future investment based on the likelihood of successful development, potential for widespread adoption and positive impact on people with asthma. This is part of the EU FP-7-funded European Asthma Research and Innovation Partnership which will identify the investment required to bring about significant improvements in asthma outcomes in Europe.
METHODS: We performed a review of the evidence for current and emerging asthma self-management tools and systems. 19 statements describing the likelihood that further investment in each tool/system would result in the development of effective self-management tool/s were extracted from the review. Using a two-stage e-Delphi process, a further group of 41 European asthma experts including health professionals, researchers, people with asthma and industry representatives were asked to rank the potential impact of research investment in each technique or tool (score 1-5; 1=very low, 5=very high). In a subsequent expert workshop, statements with a mean score> 3 were further ranked.
RESULTS: 23 and 18 responses were obtained in the 1st and 2nd Delphi rounds respectively. 14 statements scored >3 in the Delphi exercise and were further ranked. The resulting 3 most important statements were: “Behavioural strategies included in educational interventions to improve patient outcomes”, “Provision of personalised asthma self-management plans and education for all people with asthma tailored to the individual and their condition” and “New information technologies (internet, mobile phones, apps, etc...) to improve self-management”. Other areas included; integration and support of self-management into national healthcare systems and policy, implementation of annual inhaler technique checks, incorporating and evaluating shared decision making (including cost effectiveness) and multiple statements about adherence including tools to continually monitor adherence, factors affecting adherence in adolescents, determinants of good adherence, cost-effectiveness of goals setting, developing and evaluating multifaceted interventions to improve adherence and strategies to achieve adherence to preventer therapy.
CONCLUSIONS: Through careful review and consensus-building among experts, we have identified evidence-based tools and systems most likely to optimise asthma self-management. The emergence of mobile and electronic health applications and the drive to integrate national and regional data and health systems could support this, and we will use our findings to drive investment in research in these areas.










