29
Enhanced Recovery After Surgery (ERAS) in paediatrics Koen Huysentruyt
| Date post: | 14-Mar-2019 |
| Category: |
Documents |
| Upload: | nguyendien |
| View: | 222 times |
| Download: | 0 times |

Enhanced Recovery After Surgery(ERAS) in paediatrics
Koen Huysentruyt

Overview
l Introduction
l Preoperative nutritional assessment
l Preoperative fasting guidelines
l Metabolic response to surgical stress in children
l Postoperative early oral nutrition
l Current experience for ERAS in children
l Conclusion
2

ERAS elements
3
PreoperativeIntraoperative
Postoperative
ü Preadmission counselingü Fluid & CHO loadingü No prolonged fastingü No/selective bowel
preparationü Antibiotic prophylaxisü Thromboprophylaxisü No premedication
ü Short-acting anesthetic agentsü Epidural anestesia/analgesiaü No drainsü Avoidance of salt & water
overloadü Maintanace of normothermiaü Surgical techniques
ü Epidural anesthesia/analgesiaü No nasogastric tubesü Prevention of nausea/vomitingü Avoidance of salt & water
overloadü Audit of compliance outcomes
Scott et al. Acta Anaesthesiologica Scandinavica 2015
ü Early removal of catheterü Early oral nutritionü Early mobilisationü Non-opioid oral
analgesia/NSAIDsü Stimulation of gut motility
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
ERAS

Preoperativecounselling
Preoperativepreparation Admission
IntraoperativeManagement
Recovery Room
Post-operativeManagement
Discharge
SUCCESS
FAILURE
Adapted from “The Slight Edge”, by Jeff Olsen
ERAS: aggregation of marginal gains to provide large benefits
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

ERAS in paediatrics ?
5
Majority of paediatric surgery is outpatient
Need for age-dependent protocols
Children are not small adults
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Prevalence of under-nutrition:general vs surgical population
Hecht et al. Clinical nutrition 2014 ;; Huysentruyt et al. Acta paediatrica 20136
Surgical20%
Paediatric80%
7%
93%
Under-nutrition
No undernutrition
Europe (2014)
General population
Belgium (2013)Surgical
10%
Infectious62%
Other28%
13%
87%
Under-nutrition
No undernutrition
Surgical vs paediatric under-nutrition: p=0.897
Surgical vs paediatric under-nutrition: p=0.230
General population
Nutritional status
Nutritional status
(7.1% under-nutrition)
(11.2% under-nutrition)
(5.6% under-nutrition)
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Preoperative assessment & surgical outcome
7 Wessner & Burjonrappa. Journal of Pediatric Surgery 2014
Inclusion of 6 articles in review:• 3 prospective cohort studies
• 3 retrospective chart studies
IntroductionNutritional assessmentPre-op fasting Metabolic responsePostop feedingCurrent evidence for ERASConclusion

Study specifics
8
Setting Design N Nutrition assessment Outcome
Canada, 2007 Prospective 175 SGNA, albumin, transferrin, WFA, HFA, BMI, MUAC, TSF, hand grip strength
30d mortality, surg/infcomplic., LoS, Ab use
Major (non-cardiac) thoracic or abdominal surgery
Cardiac surgery
Secker & Jeejeebhoy. Am J of Clin Nutr 2007;; Leite et al. Nutrition 2005;; Radmanet al. J Thorac Cardiovas Surg 2014;; Vivanco et al. Bol Med Hosp Infant Mex 2010;; Wakita et al. Nutr Clin Pract 2011;; Toole et al. Congenit Heart Dis 2014
Setting Design N Nutrition assessment Outcome
Japan, 2011 Retrospective 36 PNI, WFA, HFA, WFA Mortality, PICU LoS, mech vent, LoS
Brazil, 2005 Prospective 30 Albumin, WFA, HFA, WFH 30d mortality, LoS, inf
Mexico, 2010 Retrospective 289 WFA at birth, BMI LoS>6d, mortality
USA/Guetamala2014
Prospective(2 centres)
41/30
TSF, albumin, pre-albumin 30d mortality, PICU LoS, mech vent., inotropics
USA, 2014 Retrospective 121 WFH, HFA LoS, PICU LoS, mechvent.
IntroductionNutritional assessmentPre-op fasting Metabolic responsePostop feedingCurrent evidence for ERASConclusion

Anthropometric assessmentHFA BMI/WFH TSF MUAC
Secker, Canada
ü LoS LoS LoS LoS
complic . complic. complic. complic .
mortality mortality mortality mortality
Wakita, Japan
LoS LoS
mechanical ventilation
mechanicalventilation
Vivanco-Munoz, Mexico
ü mortality
Radman, USA/Guatemala
ü LoS (USA) LoS (Guat.)
ü mechanical ventilation (USA) mechanical ventilation (Guat.)
Toole, USA
ü LoSinverse ?
LoS
mechanical ventilation
mechanical ventilation
9 Wessner & Burjonrappa. Journal of Pediatric Surgery 2014
IntroductionNutritional assessmentPre-op fasting Metabolic responsePostop feedingCurrent evidence for ERASConclusion

Biochemical assessment
l Albumin• Leite (Brazil):
• post-‐op infections• mortality
• Secker (Canada):• post-‐op infections• minor complications• LoS• Albumine in normal
range for all children!
• Radman (USA/Guat):• mech ventilation (USA)
l Pre-albumin• Radman (USA/Guat):
• mech ventilation (USA)
Wessner & Burjonrappa. Journal of Pediatric Surgery 201410
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Subjective assessment
11 Wessner & Burjonrappa. Journal of Pediatric Surgery 2014;; Secker & Jeejeebhoy. Am J Clin Nutr 2007
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

l “Children encouraged to drink clear fluids up to 2h before elective surgery”• Applies for neonates, infants and children• Comfort ↑, thirst ↓, risk of dehydration ↓• Permitted volume does not impact intragastric
volume of pH
l “Breast milk safe up to 4h beforeelective surgery”
l “Other milk safe up to 6h before elective surgery”
12
Preoperative fasting guidelinesIntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Smith et al. Eur J Anaesthesiol 2011;; American Society of Anesthesiologists Committee on Standards and Practice Parameters. Anesthesiology 2011

Metabolic responses to surgery
l Operative trauma = “controlled injury”
Triggers range of inflammatory pathways
l Can be the setting for deleterious effects• Systemtic inflammatory response syndrome• Prolonged catabolism of body stores
l Different in children from adults
McHoney et al. Eur J Pediatr Surg 200913
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

McHoney et al. Eur J Pediatr Surg 2009;; Basics in Clinical Nutrition, fourth edition14
Cytokine response
• Targets: thymocytes, neutrophils, T and B cells, skeletal muscle, hepatocytes, osteoblasts
• Actions: immunoregulation, inflammation, fever, anorexia, °acute phase protein, muscle proteolysis
IL-1αIL-1β
•Targets: fibroblasts, endothelium, skeletal muscle, hepatocytes, osteoblasts
•Actions: immunoregulation, inflammation, fever, anorexia, °acute phase protein, muscle proteolysis
TNF-α
•Targets: thymocytes, T and B cells, hepatocytes•Actions: immune cell differentiation, °acute phase proteinIL-6
•Targets: monocytes, SMC’s, ....•Actions: supresses the production of pro-inflammatory cytokines
IL-10
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Factors affecting response
l Age
l Nutrition and fasting
l Anaesthesia
l Operative stress & surgical approach
l Temperature
McHoney et al. Eur J Pediatr Surg 2009;; Bölke et al. Pediatric Research 2002.15
IntroductionNutritional assessmentPre-op fasting & CHO loadingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Teitelbaum & Coran. Nutrition 199816
Metabolic responses to surgeryIntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
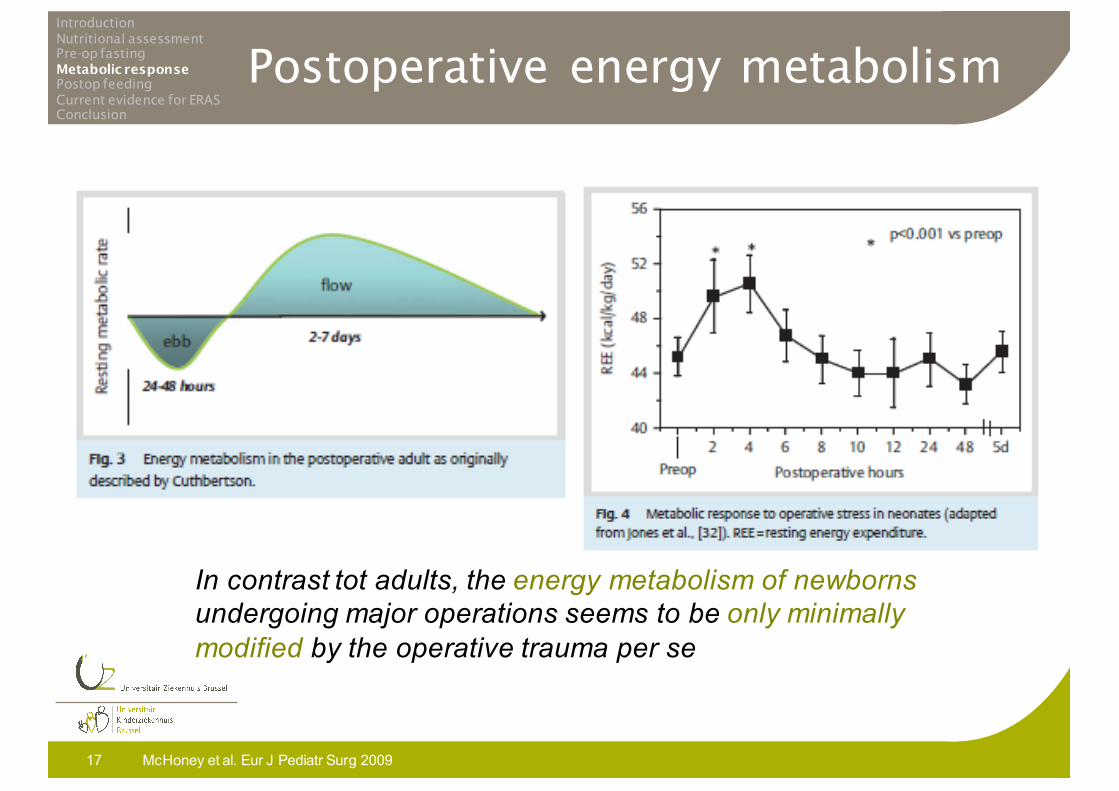
Postoperative energy metabolism
McHoney et al. Eur J Pediatr Surg 200917
In contrast tot adults, the energy metabolism of newborns undergoing major operations seems to be only minimally modified by the operative trauma per se
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Postoperative feeding
l Oral intake when possible, avoid unnessecary NG tube placement
l Avoid opioids if possiblel Pyloromyotomy:• Oral feeding possible as early as 2h
postoperatively• Full enteral intake within 24-48h after
operation• Gradual increase vs liberal intake ?• Post-op vomiting related to degree of pre-op
elektrolyte disturbances and dehydration
18
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Holland-Gunz & Günther Der Chirurg 2009;; St Peter et al. J Pediatr Surg 2008;; Adibe et al. J Pediatr Surg 2014

l Limited experience of “fast-track surgery” in paediatrics• Mixed procedures (pyeloplasty, appendectomy, bowel
anastomosis, fundoplication, hypospadia repair, nephrectomy)
• Ambulatory surgery
• Colonic surgery • Cardiac surgery
19
ERAS in paediatrics ?IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Mixed procedures:The Hannover criteria
20
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Reismann et al. J Ped Surg 2007;; Reismann et al. Langenbecks Arch Surg 2009;; Reismann et al, Eur J Pediatr Surg 2012
Element Definition of successful application
Analgesia Pain intensity <1/3 of the maximum scale points at the evening of the day of operation
Postoperative nutrition Full oral nutrition by the evening of the 2nd
postoperative day (without nausea/vomiting)
Postoperative mobilisation 2-score points at the evening of the 2nd
postoperative day
Applicability of minimallyinvasive surgery
No conversion and no postoperative complication with any adverse effect in procedures suitable for MIT
Hospital stay Significantly shorter compared to national data for similar patients in hospitals with a similar case mix index and similar structure
Postoperative symptoms No nausea or vomiting
Complications No complications
Patient/parental evaluation Satisfaction (>90%) of patients/parents, (<10%) readmission

21
Mixed proceduresIntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Holland-Gunz & Günther Der Chirurg 2009.;; Reismann et al. J Ped Surg 2007;; Reismann et al. Langenbecks Arch Surg 2009;; Reismann et al, Eur J Pediatr Surg 2012;; Schukfeh et al, Eur J Pediatr Surg 2014;; Dingemann et al, World J Urol 2010
Hannover 2007 (university hospital)• Pyeloplasty, appendectomy, bowel anastomosis, fundoplication,
hypospadia repair, nephrectomy• Excluded: additional diseases, reoperation, perforated appendicitis
113/159
Hannover 2009 (university hospital) adapted pain protocol• Elective abdominal, thoracic or urological surgery• Excluded: age ≤4 weeks, prematurity, reoperation, pectus excavatum
repair, consulted decision based on general condition and co-morbidities
155/436
Hannover 2012 (university hospital) feasibility study• Elective abdominal, thoracic or urological surgery• Excluded: age ≤4 weeks, prematurity, need for post-op PICU admission
182/203
Hannover 2014 (non-university hospital)• Pyeloplasty, appendectomy, pyloromyotomy, fundoplication, hypospadia
repair, nephrectomy • Excluded: age ≤4 weeks and >16 years
143/143

Mixed procedures:Hannover 2007 study
l Pain control• Mean pain scores >1/3 on the evening of operation• Due to restricted opioid use on the day of operation ?
l Mobilisation• Completed after mean of 29.5±17 h
l Oral nutrition• Completed after mean of 15±14 h
l Postoperative complications• n=2 (pain and revision of bleeding after hypospadia
repair)
l Patient/parent satisfaction• Not satisfied: n=2
22
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Reismann et al. J Ped Surg 2007

Mixed procedures:Hannover 2009 study
l Pain control:
l Mobilization:
23
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
2007 study 2009 study
Reismann et al. Langenbecks Arch Surg 2009

Mixed procedures:Feasibility study
24
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Successful implementation of fast-track elements
Reismann et al, Eur J Pediatr Surg 2012
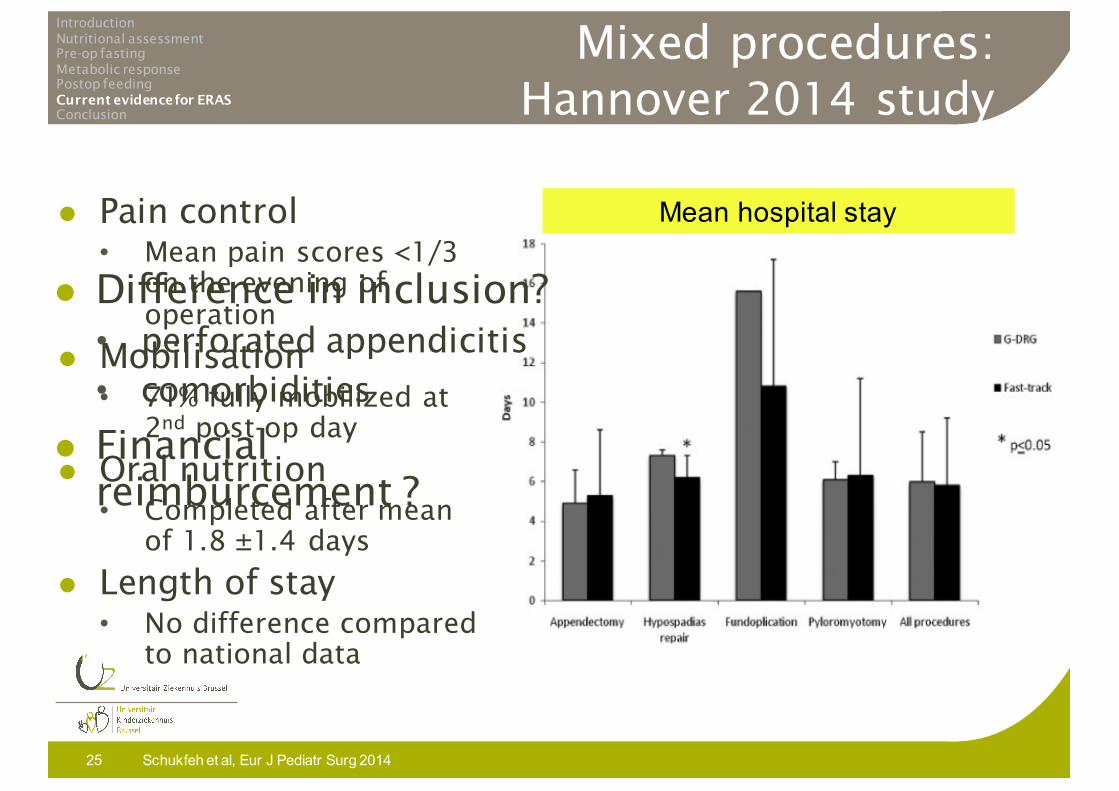
Mixed procedures:Hannover 2014 study
l Pain control• Mean pain scores <1/3
on the evening of operation
l Mobilisation• 71% fully mobilized at
2nd post-op day
l Oral nutrition• Completed after mean
of 1.8 ±1.4 days
l Length of stay• No difference compared
to national data
Schukfeh et al, Eur J Pediatr Surg 201425
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Mean hospital stay
l Difference in inclusion?• perforated appendicitis• comorbidities
l Financial reimburcement ?

Ambulatory surgery
l Children >7 years post-op randomly sent to PACU (standard, no parents present) or second-stage recovery unit (parents present):
Ramesh et al. Anesth Analg 200126
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

Colonic surgery
l Prospective Italian study (2009)• 46 children (38 Hirschprung, 8 IBD)
• 100% oral feeding on post-op day 1• 100% discharge before post-op day 5
• 2 re-admissions
Mattioli et al. J Laparoendoscop Adv Surg Techn 200927
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Fast-track protocol• Pre-op: standardized bowel preparation, Ab, standardized fasting, full pre-op evaluation
• Intra-op:muscle-sparing approach• Post-op: avoiding drain, early removal of NG tube, pain control, minimize opioids

Colonic surgery
l Retrospective US study (2014)• 71 children (all Crohn’s disease)
• 45 fast-track vs 26 conventional
Vrecenak & Mattei. J Pediatr Surg 201428
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion
Protocol• Pre-op: “counseled”• Intra-op: laparoscopic approach• Post-op: oral intake within 24h, no routine NG tube, rectal suppository if no stool on day 2, minimize opiods, avoiding drain

Conclusion
l Mind the nutritional status also in childrenl No overnight fastingl Metabolic response is different, especially
in small childrenl Paucity of evidence for ERAS in pediatric
surgeryl Current evidence suggests that ERAS can be
implemented safelyl At least in selected patients, ERAS can lead
to shorter hospital stay
29
IntroductionNutritional assessmentPre-op fastingMetabolic responsePostop feedingCurrent evidence for ERASConclusion

















