Epilepsy Q: What is epilepsy? A: Epilepsy is a brain disorder. It occurs when the electrical signals in the brain are disrupted. This change in the brain leads to a seizure. Seizures can cause brief changes in a person's: • Body movements • Awareness • Emotions • Senses, such as taste, smell, vision, or hearing People with epilepsy have repeated seizures.
Transcript
Epilepsy
Q: What is epilepsy?
A: Epilepsy is a brain disorder. It occurs when the electrical signals in the brain are disrupted. This change in the brain leads to a seizure. Seizures can cause brief changes in a person's:
• Body movements
• Awareness
• Emotions
• Senses, such as taste, smell, vision, or hearing People with epilepsy have repeated seizures.
Myth or Fact
Myth #1 --- Epilepsy is rare
Fact --- More than 2.5 million Americans have epilepsy.
Myth #2 --- Epilepsy is contagious
Fact --- You cannot catch epilepsy from another person! Therefore it is not contagious.
Myth or Fact
Myth #3 --- Epilepsy is a psychological condition
Fact --- Epilepsy is a medical condition. Seizures are the result of an excessive and disorderly discharge of electrical energy in the brain.
Myth #4 --- Epilepsy is a form of mental illness
Fact --- Epilepsy is a functional, physical problem, not a mental one. Its an umbrella term that describes about twenty different types of seizure disorders.
Myth or Fact
Myth #5 --- Persons with epilepsy are “epileptics.”
Fact --- Persons with epilepsy are individuals who experience chronic, recurrent seizures and prefer being described as "persons with epilepsy.“
Myth #6 --- You have to be born with epilepsyFact --- Epilepsy often first appears in children and young adults, although anyone can develop epilepsy at any time.
Myth or FactMyth #7 --- Epilepsy is a lifelong disorderFact --- Epilepsy is not necessarily a lifelong disorder. Many persons with epilepsy will not have seizures or require medication all of their lives.
Myth #8 --- You can’t prevent epilepsyFact --- While no specific cause can be pinpointed in a majority of epilepsy cases, some causes, such as severe head injuries experienced in falling from a bicycle or sustained in an automobile accident, have been identified. This is why helmet safety is so important for children as a preventive measure.
Myth or FactMyth #9 --- Epilepsy cannot be treated or
curedFact --- There is no known cure for epilepsy. However, modern treatment methods can achieve full control of seizures in a majority of cases. According to the EFA, 80 percent of those on medication have complete control of seizures. Within the past 15 years, several new drugs have been developed to help control seizures, and surgery is an option for some patients. Many people who have epilepsy lead productive, normal lives. Currently there is no cure, but some children tend to outgrow the condition.
Myth or Fact
Myth #10 --- Epilepsy is a disease
Fact --- Epilepsy is a neurological condition characterized by recurring seizures. Epilepsy is not a disease or a mental illness, and it does not signal emotional instability or lack of intelligence. According to the Epilepsy Foundation of America (EFA), 9 percent of the population will have a seizure at some point in their lives. Of this group, 3 percent will develop epilepsy.
Myth or Fact
Myth #11 --- All seizures are the sameFact --- There are more than 20 forms of seizure disorders. The intensity and duration of the seizure depends on how many and what type of brain cells are affected. Seizures are not painful and range from convulsions to momentary lapses of attention. People with mild seizures may even be unaware they’ve had one. Seizures may occur minutes, days or years apart, depending on how well they are controlled by medication
Incidence
• Over a lifetime, 5-7 percent of us have a seizure
• 30 to 60 per 100,000 persons have epilepsy• Common in very young children• Most common neurological disorder of
• An epileptic disorder characterized by a cluster
of signs and symptoms which occur together
• Factors taken into consideration include seizure
type, etiology, genetics, anatomy, precipitating
factors and the interictal EEG
Proposed by ILAE in 1985, revised in 1989 currently
under revision
Generalized seizures
• Electrical abnormality throughout cerebral cortex
• Grand mal or generalized tonic-clonic seizures
• Absence or petit mal
• Atonic seizures
Generalized Tonic-Clonic Seizures
• Person stiffens, falls, and convulses, losing consciousness
• EEG abnormal in more than 2/3 of cases• Cause in young children due to infection, metabolic
disorder or trauma• In older individuals, usually due to trauma or tumor• Outcome dependent upon age, cause, and ability to
control seizures• Approximately 40 percent retarded
Absence or Petit Mal Seizures
• Temporary lapse of consciousness that starts and ends abruptly
• Brief periods of lack of awareness; may be unusual movements
• Usual age of onset is 4 to 8 years• High genetic predisposition• Over 50 percent go into remission after adolescence• Generally normal IQ; only 5 percent retarded
• Localized seizure disorder which lasts a few minutes and is characterized by motor or sensory phenomena in a hand, arm or body part
• Includes Jacksonian seizures in which seizure moves sequentially from one area to another on the same side of the body
• Most frequent between 5-15 years of age• 25 percent of post traumatic seizures of this type• Outcome dependent upon where seizure origin is
located; frontal lobe hard to control• Generally normal IQ
Complex partial seizures
• Also called psychomotor or temporal lobe seizures• Individual loses awareness• Repetitive motor behaviors occur• Last 1 to a few minutes• Recovery includes confusion, irritability• Accounts for 2/3 of all epilepsies• Multifactorial causes: Genetic predisposition,
prenatal trauma, brain lesions
Generalized Partial Seizures
• Sometimes partial seizures develop into full body seizures
• Usually this is when they are uncontrollable
Febrile Seizures
• Brief seizure in a child which occurs in conjunction with a high fever
• Occur in about 3 percent of young children• Peak occurrence between 9 to 20 months• Over 65 percent do not have subsequent seizure• If have multiple seizures, or associated with other
anomalies (CP), then likely to have impact on intellect
• Seems to run in families
Neonatal Seizures
• May have a variety of causes: Trauma, metabolic, or infection
• If have multiple neonatal seizures, 40 percent mortality rate
• 35 percent have mental retardation
• If metabolic, especially due to drug withdrawal, outlook is better
Objectives
• How to investigate possible seizures– History of greatest importance
• How to approach epilepsy syndromes
• How to predict seizure recurrence
• How to choose an anti-epileptic drug
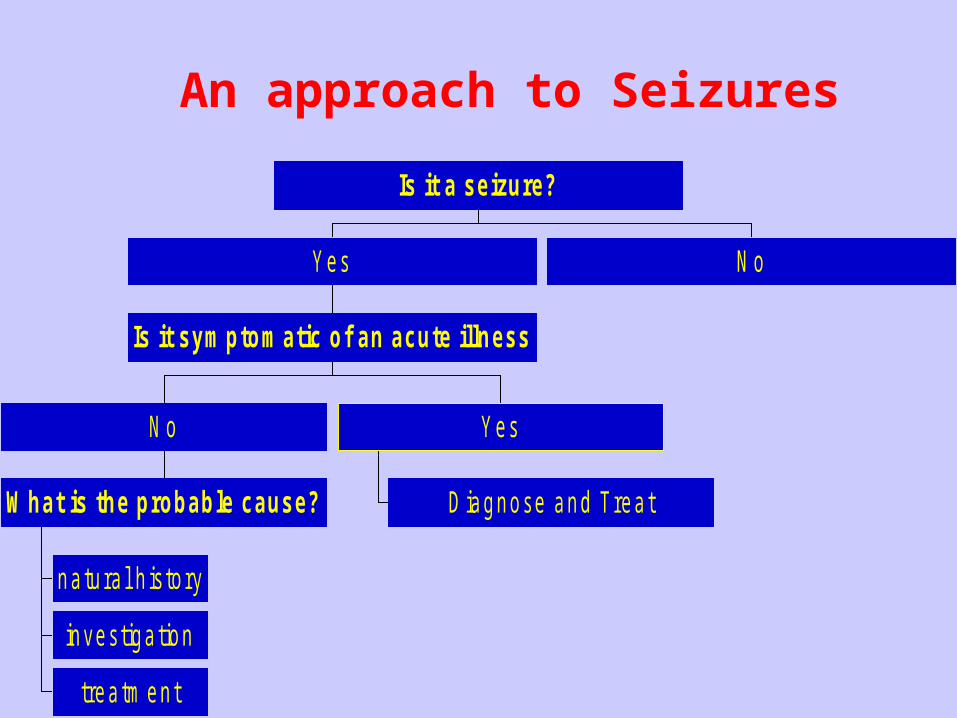
An approach to Seizures
natura l h istory
investiga tion
treatm ent
What is the probable cause?
N o
D iagnose and Treat
Yes
Is it symptomatic of an acute illness
Yes N o
Is it a seizure?
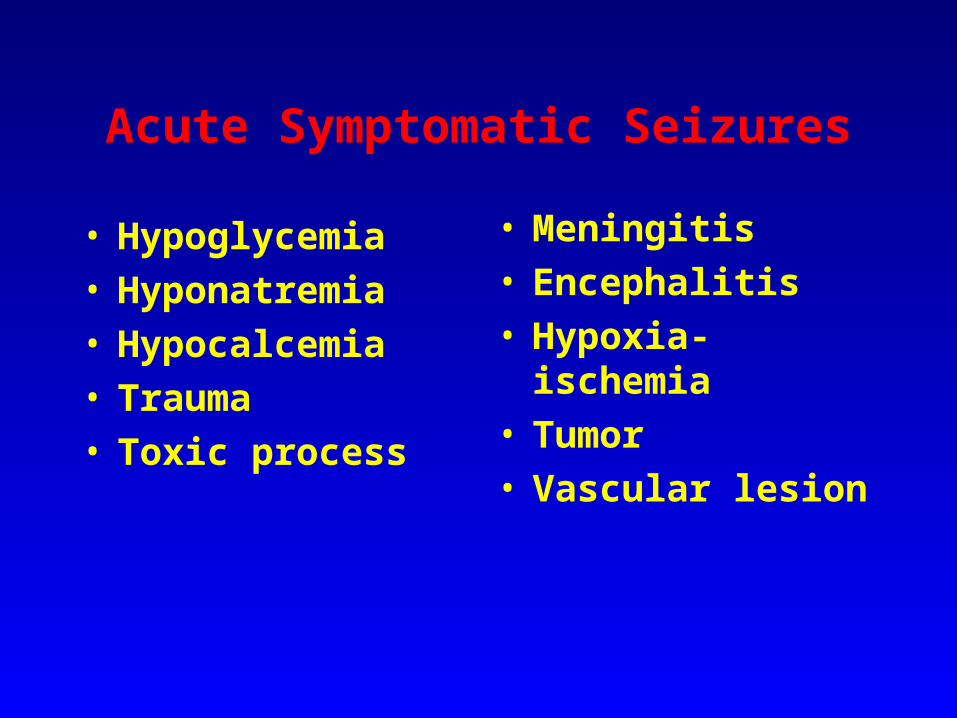
Acute Symptomatic Seizures
• Hypoglycemia• Hyponatremia• Hypocalcemia• Trauma • Toxic process