Understanding nutrition-related symptoms, complications and health-related quality of life in patients with gastroenteropancreatic neuroendocrine tumours Erin Clare Laing ORCID ID: 0000-0003-1296-6948 Doctor of Philosophy February 2021 Department of Nursing Faculty of Medicine, Dentistry and Health Sciences The University of Melbourne Submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy
Transcript
Understanding nutrition-related symptoms, complications and
health-related quality of life in patients with
gastroenteropancreatic neuroendocrine tumours
Erin Clare Laing
ORCID ID: 0000-0003-1296-6948
Doctor of Philosophy
February 2021
Department of Nursing
Faculty of Medicine, Dentistry and Health Sciences
The University of Melbourne
Submitted in total fulfilment of the requirements of the degree of
Doctor of Philosophy
iii
Abstract
Gastroenteropancreatic neuroendocrine tumours (GEP NET) can lead to complex
symptoms and reduced health-related quality of life (HRQoL). The management of
GEP-NETs is challenging. To date there has been development of clinical practice
guidelines and consensus guidelines for GEP-NETs; however, the supportive care needs
and optimal nutritional management of patients affected by GEP-NETs remains under-
researched and evidence to guide clinical practice is lacking. These malignancies have
the potential to significantly impact on patient morbidity, HRQoL and nutrition due to
the tumour location, functional status (secretion of hormones), symptoms and
treatment. A limited number of published cross-sectional studies have indicated the
presence of nutritional issues among patients with a GEP NET, including malnutrition
(in 14-25%) and the presence of vitamin (niacin and fat-soluble vitamin) deficiencies.
There is mostly anecdotal evidence for dietary change among patients with a GEP NET,
and few studies have explored this phenomenon and its impact on patients.
The aim of this thesis was to comprehensively describe the nutritional complications of
GEP NET, and to explore the nutritional knowledge and practices of health
professionals managing patients with a NET, enabling the first summary of NET health
professional practices in regard to nutrition. A prospective longitudinal mixed-methods
study was undertaken to comprehensively explore the prevalence of nutritional
complications in patients diagnosed with a GEP NET. Patients recruited to this study
had reduced HRQoL, specifically social functioning; and the presence of anxiety,
depression and financial toxicity was observed. Common symptoms, reported in 40-
80% of participants, were fatigue, abdominal discomfort, pain, bloating, wind/gas and
diarrhoea. Results of this study showed that malnutrition was prevalent in up to 29%
of patients, as was weight loss (up to 51%), loss of muscle mass (up to 62%) and
dietary change (up to 56%), and all nutritional complications remained so over the six-
month study period. Patient interviews conducted during the study period
demonstrated the negative impact of a GEP NET diagnosis on patient’s HRQoL, and
that dietary change and food restriction was often initiated by patients in response to
iv
their symptom burden. Nutrition and dietary information/management was identified
by patients as an un-met need. Results of an exploratory mixed-methods health
professional study showed that only 38% of NET health professionals are routinely
performing screening for nutrition-related complications. Nutrition advice and
management was varied and inconsistent, with health professionals identifying a lack
of NET-specific nutrition evidence and guidelines as barriers to their practice.
Results of the studies reported in this thesis contribute evidence and knowledge
towards the presence and severity of nutritional complications among patients with a
GEP NET, which are often under-recognised and impact on patient HRQoL. Results also
provide the first summary of NET health professional nutrition-related practices.
Results highlight the importance of identifying nutritional complications in this unique
patient group and provide key insights into the nutrition risk factors relevant to
patients with a GEP NET. This thesis will contribute to the future development of NET-
specific nutrition guidelines and establishment of a robust nutrition risk screening
process for NETs.
v
Declaration
This is to certify that:
i. This thesis comprises only my original work towards the PhD except where
indicated in the preface,
ii. Due acknowledgement has been made in the text to all other material used,
iii. This thesis is fewer than 100,000 words in length, exclusive of tables, maps,
bibliographies and appendices
Signed
………………………………………………………………
vii
Preface
This thesis and the work that contributed to it was carried out primarily by the PhD
candidate, Erin Laing, with contribution from all supervisors (Professor Meinir
Krishnasamy, Dr Nicole Kiss and Professor Michael Michael). Statistical support was
received from statistician Associate Professor Karla Gough, with the statistical planning
and analysis undertaken by EL.
The results of the comprehensive literature review in Chapter 1 were published in April
2020. This manuscript was written in collaboration with my supervisors (MK, NK, MM)
and the final published version has been included in Chapter 1.
The research protocol for the Phase 1 longitudinal mixed-methods study in Chapter 2
was published in December 2018. This manuscript was written in collaboration with
my supervisors (MK, NK, MM) and a statistician (KG), and the final published version
has been included in Chapter 2.
The results of the international online survey of NET health professionals, discussed in
Chapter 6, have been prepared as two manuscripts for publication. These manuscripts
were written in collaboration with my supervisors (MK, NK, MM) and a statistician
(KG). The word document of final approved manuscripts is included as unpublished
material in Chapter 6. EL conceived and designed the study with assistance from NK,
MM, MK and KG. EL conducted recruitment and data collection. EL performed data
analysis with assistance from KG. EL drafted the manuscript. All authors revised the
manuscripts critically for important intellectual content and approved the final version
for submission. The final version of these manuscripts included in Chapter 6 are
planned for submission to a journal in October 2020.
The research presented in this thesis was primarily supported by funding received
from the Victorian Cancer Agency, Victorian Government, Melbourne, Australia; and
Austin Health, Melbourne, Australia; through the Olivia Newton John Cancer, Wellness
viii
and Research Centre (ONJCWRC) Supportive Care Research PhD Scholarship awarded
to EL in December 2016. EL received funding through this scholarship towards their
PhD stipend and research costs. EL received initial seed funding for their PhD stipend
between August to December 2016 from the Nutrition and Speech Pathology
Department, and Neuroendocrine Unit at Peter MacCallum Cancer Centre, Melbourne,
Australia. EL received additional funding from Ipsen Australia and NeuroEndocrine
Cancer Australia (formerly Unicorn Foundation Australia) towards PhD research costs.
Funding sources were not involved in the conception, preparation or writing of any
research studies or manuscripts.
ix
Acknowledgements
The journey to PhD completion has been full of hard work and some challenges,
combined with inspiring moments and contributions from surrounding researchers,
clinicians, patients, and support people all of who I wish to thank.
To my supervisors Mei Krishnasamy, Nicole Kiss and Michael Michael, thank you for
your unwavering support and inspiration. I have considered myself very lucky to have
such a dedicated and supportive supervision team throughout my PhD. Mei, I thank
you for your constant leadership and encouragement, I have learnt so much from you
about research and your passion for helping patients through research has been an
inspiration. Nicole, I thank you for pushing me to commence a PhD and for the
constant support, nutrition expertise and opportunities you’ve provided throughout
the process. Michael, I thank you for your guidance and professional insight, and for
helping me shape a profile in the NET clinical and research space.
To my advisory committee, led by Anna Boltong, and including Snezana Kusiljic and
Judy Bauer, thank you for all your professional advice and support. To Karla Gough,
thank you for your invaluable guidance and support with my statistical analysis. I have
appreciated learning from you. To the Cancer Nursing Research team, I really valued
my time sitting in your department, and thank you for your support, research guidance
and friendship. I particularly wish to thank Cath Devereux and Carol Jewell who
assisted me as co-facilitators during my health professional focus groups.
To the Peter Mac Nutrition and Speech Pathology team, your support and interest in
my research has been very encouraging and kept me motivated. Special thanks to
Jenelle Loeliger and Belinda Steer for supporting me to work part-time and develop as
a clinician researcher. Thanks to Kirsty Rowan and Jacq Black for assisting with data
collection when I had to take leave.
x
To the NET unit and multidisciplinary team at Peter Mac, thank you for welcoming me
into the team as a dietitian and researcher. I am thankful to work so closely with such
as professional and patient-cantered group. Thank you to Niall Tebbutt at Austin
Health for assisting to coordinate recruitment at that site.
I’d like to acknowledge my funders, including the Victorian Cancer Agency and Austin
Health (ONJCRWC) scholarship that supported and enabled me to complete this PhD. I
also wish to acknowledge NeuroEndocrine Cancer Australia (formerly the Unicorn
Foundation) and Ipsen Australia for additional funding support towards my PhD
research. To all the staff at NeuroEndocrine Cancer Australia, your passion for helping
people living with NETs is inspirational. Special thanks to Simone Leyden and Kate
Wakelin who have consistently supported my research and continued to raise
awareness of nutrition needs among people with NETs.
Steve Jobs once said, ‘The only way to do great work is to love what you do’, which is
how I have felt throughout my PhD. I have learnt so much about the experiences of
patients with NETs and have enjoyed telling their story through my research. As a
researcher and a clinician this has been invaluable, and I will continue to love working
with and supporting these patients throughout my career. Thank you to all the
patients and health professional participants who invested their time for my research
and brought much enthusiasm to help drive nutrition research for NETs.
Finally, thank you so much to my family, my husband Josh, and my son Hayden. Josh,
thank you for your patience, and for putting up with my PhD talk and late-night work.
Your constant love and support has kept me going right to the end. To Hayden, you are
too young to appreciate what I have been working on, but your birth during my PhD
candidature has provided a positive distraction and kept me grounded.
xi
Table of Contents
Abstract............................................................................................................................. iii
Declaration ........................................................................................................................ v
Preface ............................................................................................................................. vii
Acknowledgements .......................................................................................................... ix
Chapter 1: Introduction and literature review ................................................................. 1
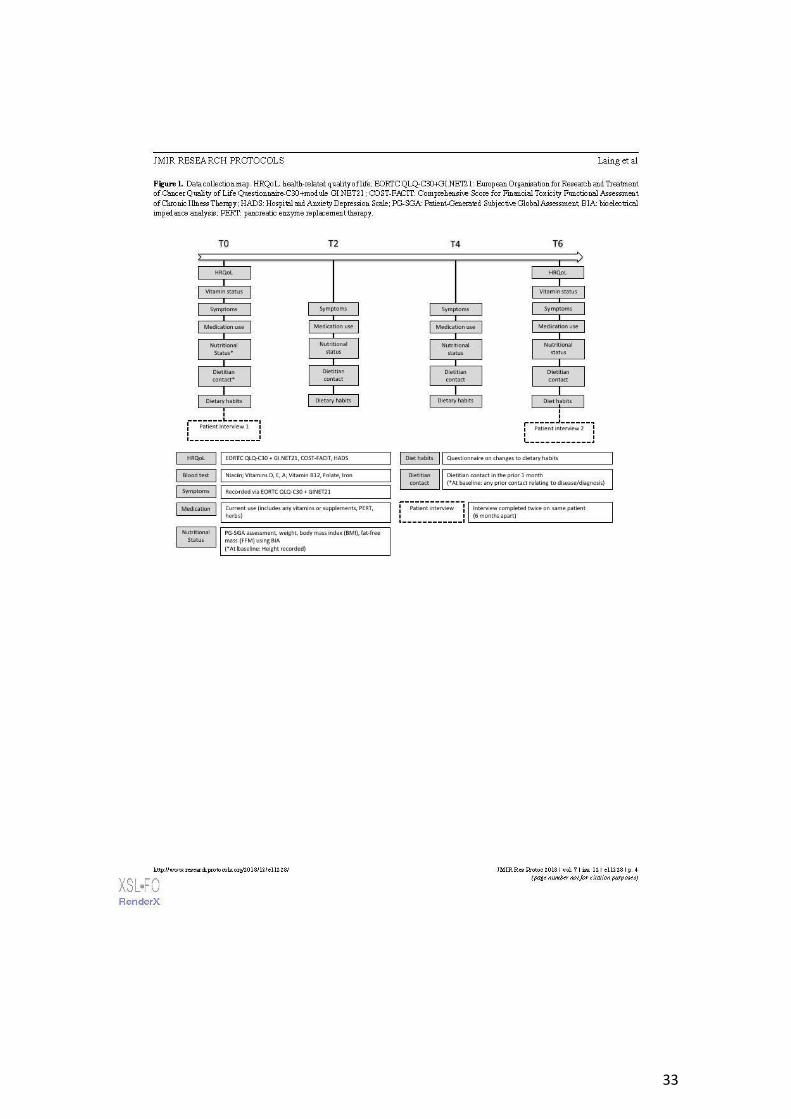
Dietitian contact was recorded using a 5-item questionnaire designed specifically for
the study, and from information in the medical records where available. The
questionnaire required participants to report if they had contact with a dietitian in the
month prior to data collection at T0, T2, T4 and T6. The location of dietitian contact,
47
source of referral and reason for contact were recorded using the questionnaire,
attached in Appendix 1. For questions where participants were able to select multiple
answers (Question 5), this was indicated in the title of the question and verbally
discussed with the participant by the researcher.
2.5.11 Dietary habits
A 5-item questionnaire designed specifically for this study was used to record changes
to participant dietary habits as a result of their NET diagnosis or treatment. Design of
the questionnaire was informed by the comprehensive literature review discussed in
Chapter 1. Validated food frequency questionnaires are available for use with cancer
patients, but most include more than 70-items, but the burden of completion was
deemed greater than the potential gain of information. Before recruitment, three NET
patient advocates from the NeuroEndocrine Cancer Australia (formerly the Unicorn
Foundation) Consumer Advisory Group completed the 5-item questionnaire to
determine its readability and completion time. Only minor changes to wording of the
questionnaire were required after this testing. The final dietary questionnaire is
attached in Appendix 1. Questions where participants were able to select multiple
answers (Questions 2-5) had this either indicated in the title of the question or were
indicated verbally to participants by the researcher.
2.5.12 Medication use
Participants were asked to report all current medication use in consultation with the
researcher at each data collection time-point. Only the medications considered
relevant to nutrition and the treatment of nutrition-related symptoms (vitamin
supplements, herbal or complimentary medicines including probiotics, pancreatic
enzymes, anti-diarrhoeal, anti-emetics) were reported in the study results. Some
participants reported use of a multivitamin which is defined as a supplement
containing a combination of multiple vitamins and minerals.
48
2.5.13 Patient interviews (qualitative)
The research design and methodology of patient interviews conducted as the
qualitative arm of the Phase 1 research study will be discussed in detail in Chapter 5,
along with results.
2.5.14 Statistical analysis
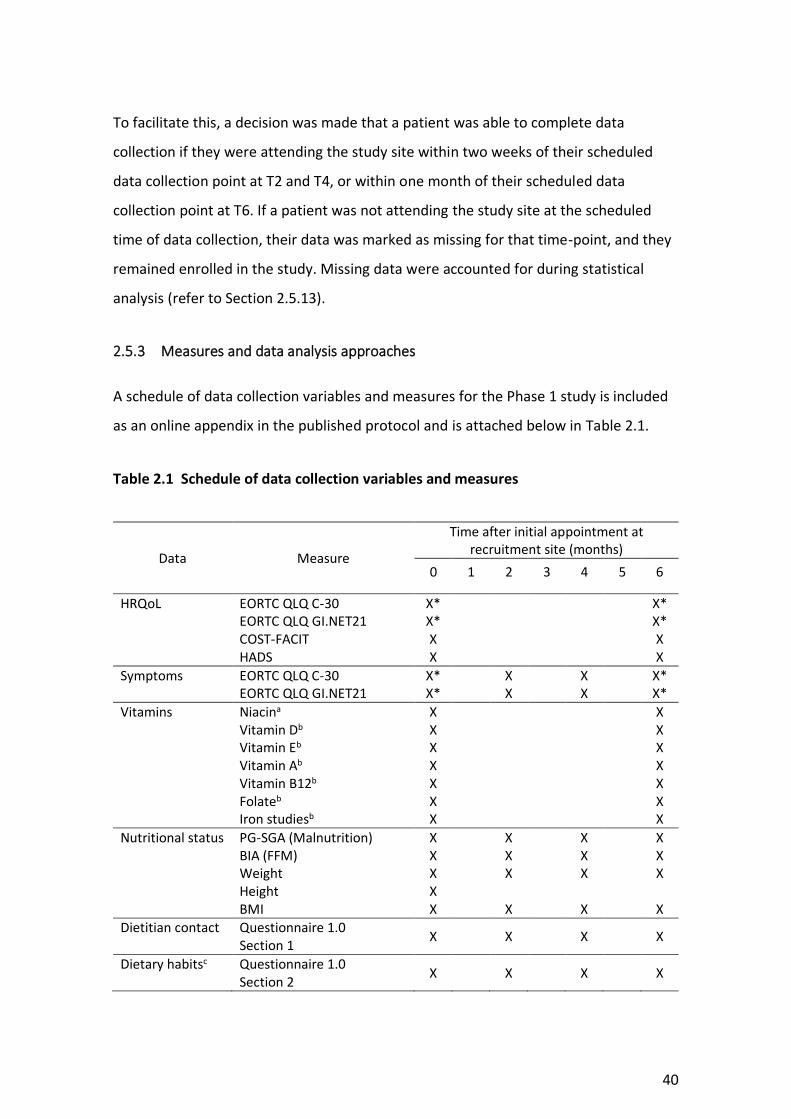
Additional detail of statistical analysis methods after publication of the protocol paper
are described as below.
Responses to patient-reported outcome measures were scored according to author
guidelines. Where relevant, recodes were applied as described above. Descriptive
statistics were used to summarise patient demographic and clinical characteristics, and
responses to patient-reported outcomes measures (EORTC QLQ-C30, EORTC QLQ-
GI.NET21, COST-FACIT and HADS) at each assessment. These included counts and
percentages for nominal valued variables; and means and standard deviations or
medians and interquartile ranges, as appropriate, for continuous valued variables.
Analysis of outcomes assessed by the EORTC measures was carried out by a fitting
linear mixed model to each outcome separately using the ‘lme4’ package. Models
included a fixed effect for time, as well as a random participant effect; an unstructured
covariance structure was used to guard against model misspecification. All models
were estimated via maximum likelihood. Differences between baseline and T6
assessments were estimated with 95% confidence intervals. Effect size estimates, as
described by Kazis and colleagues (Kazis, Anderson and Meenan, 1989), were used to
characterise the size of observed differences. These are interpreted as per Cohen’s d,
with 0.2, 0.5 and 0.8, reflecting small, medium and large-sized differences, respectively
(Cohen, 1988).
McNemar’s test was used to assess differences between proportions of participants
who were malnourished at follow-up assessments compared with baseline. Confidence
49
intervals (95%) were calculated using the method described by Carlin and Doyle (Carlin
and Doyle, 2001).
Due to sample size limitations statistical sub-analysis of the difference in nutritional
outcomes (malnutrition status) between sub-groups defined by disease- and
treatment-related characteristics was not performed. Instead, crosstabulations were
used to generate the joint frequency distributions of patients based on nutritional
status and disease and treatment characteristics (NET site, NET grade).
Scoring and descriptive analysis was performed in SPSS Version 25 (Chicago, IL, USA).
Mixed model analysis was performed in R Version 3.6.1, using the ‘lme4’ and ‘lsmeans’
packages. Kazis effect sizes were calculated manually in Excel.
51
Chapter 3: Nutrition-related symptoms and health-related
quality of life in people with NETs
This chapter describes results from the Phase 1 longitudinal mixed-methods study of
patients with GEP NETs, and focuses on nutrition-related symptoms and HRQoL, as
described by patients who took part in the study.
The chapter includes details of participant demographics, clinical characteristics,
symptomatology and HRQoL. It begins with an overview of published literature
relevant to these findings. Nutritional outcomes from the Phase 1 study are discussed
in Chapter 4.
3.1 Introduction
Patients with GEP NETs can experience numerous and complex symptoms relating to
the presence of their disease or various treatment modalities (Burgess, 2005; Kaupp-
roberts, Srirajaskanthan and Ramage, 2015). Up to 30 percent of patients with GEP
NETs have carcinoid syndrome, whereby their tumours secrete endogenous amine
hormones, in particular serotonin, which can give rise to symptoms including flushing,
fatigue, severe diarrhoea, food intolerance, restlessness and fluctuations in mood and
pain (Haugland et al., 2013; Kaupp-roberts, Srirajaskanthan and Ramage, 2015). NET
related symptoms may persist for long periods (median 9.2 years) prior to diagnosis,
and have the potential to place substantial HRQoL burden on the patient and health
service utilisation impact on the health care system (Vinik et al., 2010; Kaupp-roberts,
Srirajaskanthan and Ramage, 2015; Singh et al., 2017). Although potential side-effects
of the disease and its treatment have been documented (Kaupp-roberts,
Srirajaskanthan and Ramage, 2015), there is limited published information on the
incidence and prevalence of symptoms and description of their impact on patients
themselves, particularly in an Australian population. The specific impact on nutritional
status is also still largely unknown
52
Presenting symptoms from a NET can be a result of the mass tumour effect, such as
bowel obstruction, pain, bleeding and jaundice; generalized symptoms of cancer
presence, such as fatigue, low appetite, cachexia and loss of weight; or hormonal
effects, such as flushing, diarrhoea, reflux, gastric ulceration, bowel ischemia, glucose
intolerance and hypoglycaemia (Burgess, 2008). In people with NETs symptoms are
generally related to the secretion of hormones (Pearman et al., 2016).
Many of the symptoms experienced by people with NETs can potentially affect
nutritional intake and nutritional requirements. For example, altered glucose
metabolism has implications for carbohydrate requirement and intake (Sheard et al.,
2004). Symptoms such as abdominal pain and loss of appetite can cause patients to
alter their dietary intake, putting them at risk of weight loss and malnutrition (Borre et
al., 2018). Diarrhoea can be associated with nutrient malabsorption, electrolyte
disturbance and dehydration, particularly if steatorrhea is present (Van Der Horst-
Schrivers et al., 2004). The diverse nature of symptoms experienced by people with a
NET can also result in significant delays to or misdiagnosis (Toth-Fejel and Pommier,
2004). People with NETs, particularly those with carcinoid syndrome, are commonly
misdiagnosed with other conditions such as irritable bowel syndrome, food allergies or
intolerances (Toth-Fejel and Pommier, 2004). Treatment for these conditions regularly
involves dietary modification and can lead people to alter their diets unnecessarily.
Various treatment modalities are used for disease and symptom control in patients
with GEP NETs. These may include surgery (curative or debulking, including bowel and
nodal resection, pancreatectomy or liver resection), somatostatin analogue treatment
(SSA, lanreotide or octreotide), chemotherapy, peptide-receptor targeted radiotherapy
(PRRT) and targeted therapy such as everolimus and sunitinib (Öberg et al., 2012). All
of these treatments have the potential to cause side-effects and symptoms that impact
HRQoL and nutritional health. Curative surgery may be performed if disease is localised
or palliative non-curative “debulking” resection may be used to assist with symptom
control and to improve quality of life (Ramage et al., 2012). Side-effects of
gastrointestinal surgery depend on the location and extent of resection but can include
53
altered gut function, and malabsorption by reduced absorptive surface, bacterial
overgrowth or blind loops (Lambert, 2008). SSA treatments have an anti-secretory
effect by inhibiting secretion of bioactive peptides, hence reducing hormone related
symptoms. In addition SSAs have tumoural anti-proliferative effects in patients with
NETs, preventing or reducing risk of disease progression (Rinke et al., 2009; Caplin et
al., 2014). Adverse effects of SSAs have been reported and include abdominal pain,
nausea, constipation, diarrhoea, cholelithiasis, steatorrheoa and disturbances of
glucose homeostasis (Caplin et al., 2014; Lamarca et al., 2018). SSA treatment can also
influence the secretion of intestinal fluid, pancreatic enzymes and bile acids, thus
impacting digestion and absorption processes (Fröjd et al., 2007; Modlin et al., 2010).
The symptoms experienced by people affected by NETs impact their physical and
mental well-being (Fröjd et al., 2007; Haugland et al., 2009; Kaupp-roberts,
Srirajaskanthan and Ramage, 2015; Pearman et al., 2016). The most commonly
occurring symptoms reported to impact HRQoL are fatigue, diarrhoea and flushing
(Haugland et al., 2009; Kaupp-roberts, Srirajaskanthan and Ramage, 2015; Pearman et
al., 2016). In an international survey of 1928 patients, most participants (71%)
reported that a NET diagnosis had substantially negatively impacted their personal
life, resulting in reduced energy levels and ability to perform household chores (Singh
et al., 2017). In an online survey of 663 German patients with NETs, the increased
frequency of bowel movements and presence of flushing were associated with
decreased quality of life (Pearman et al., 2016). Observational studies have also
identified that NET patients experience distress as a result of symptoms of fatigue and
diarrhoea, which impact people’s ability to perform daily physical activities (Larsson,
Haglund and Von Essen, 2003; Fröjd et al., 2007). People living with NETs in the US,
Norway and Sweden have been shown to have significantly lower HRQoL than the
general population when matched for age and gender (Fröjd et al., 2007; Haugland et
al., 2009; Beaumont et al., 2012).
54
Whilst this highlights an important need for effective symptom control and side-effect
management in people with NETs, there is limited information available to target
clinical care, research and education for Australians living with NETs, compared with
people living with other gastrointestinal disorders or cancers. Depression and anxiety
have also been reported to be prevalent amongst people with NETs, particularly at
time of diagnosis; however some studies have reported that the mental health of
patients with NETs may not be significantly different from the general population, and
rates of anxiety and depression may remain stable or improve over time from
diagnosis (Larsson et al., 2001; Fröjd et al., 2007). These studies were limited by small
sample sizes, n=24 and n=36 respectively, and with high attrition rates, but this picture
is replicated in other cancer groups where the emotional impact of the disease and its
treatment abates over time as people become more familiar with the expectations of
treatment, their treating team, and the shock of diagnosis subsides. Limitations of the
current literature on the HRQoL and symptom burden experienced by people with
NETs include, the heterogeneity of participant samples and the inconsistent
methodological approaches (Chau et al., 2013; Martini et al., 2016). For example,
most studies have used generic HRQOL measures to assess HRQoL with NET cohorts,
with only a few having used the NET specific module, EORTC QLQ GI.NET21 which is
validated and designed to assess quality of life in patients with gut and pancreatic NETs
(Yadegarfar et al., 2013).
The remainder of this chapter describes results from the Phase 1 longitudinal mixed-
methods study of patients with GEP NETs, including participant demographics, clinical
characteristics, symptomatology and HRQoL. Nutritional outcomes from the Phase 1
study are presented in Chapter 4.
3.2 Aims and objectives
As set out in Chapter 2, the aim of Phase 1 was:
To describe the impact of GEP NETs and their treatment on patients’ nutritional status
and HRQoL.
55
3.2.1 Objectives
1. To describe the nutrition-related symptoms and HRQoL of people living with a
GEP NET, including:
a. The prevalence and severity of patient-reported physical symptoms
b. Anxious and depressive symptomatology
c. Financial burden
d. Health-related quality of life
2. To explore any differences in HRQoL scores between baseline (T0) and six-months
(T6)
This was a prospective, embedded mixed-methods longitudinal study as described in
Chapter 2, Section 2.4.
3.4 Results
3.4.1 Patients
During the study recruitment period (June 2017 – June 2018), 188 newly referred
patients attending Upper Gastrointestinal (UGI) and NET clinics at study sites, were
available to assess their eligibility for the study. Thirty patients being investigated for a
GEP NET diagnosis were screened but were deemed ineligible after they received a
revised diagnosis of squamous cell carcinoma or adenocarcinoma. Other reasons for
ineligibility included: patient was for observation only (n=24), was receiving primary
medical treatment outside of the study site (n=19), NET disease found to be
completely resected and in remission (n=15), and patient was greater than 6 weeks
from initial referral to the study site (n=14). Of the 75 patients assessed as eligible, 61
patients were recruited to the study (Figure 3.1). Two participants were withdrawn
from the study immediately after recruitment and initial baseline data collection due
to changes in their diagnosis or treatment plan causing them to no longer meet
56
eligibility criteria; therefore, data from 59 participants was used for analysis. Figure 3.1
outlines the recruitment process and data available at each data collection time-point.
There were 35 counts of missing data due to a participant not attending the study site
at the time they were due for data collection. In total 28 of 59 (47%) participants had
complete data sets at all four time-points.
Whilst there were two recruitment sites, Peter MacCallum Cancer Centre and Austin
Health, 58 of 59 participants were recruited from the Peter MacCallum Cancer Centre.
As this study was undertaken in part-fulfilment of a PhD, participant recruitment and
data collection were undertaken by the same person (Coordinating principal
investigator (CPI), PhD student) at both sites. As the CPI was based at the Peter
MacCallum Cancer Centre, they had regular access to multidisciplinary meeting and
clinic lists which were used for screening potential participants. At Austin Health
screening of patients was undertaken by the site principal investigator (PI), who
communicated details of potential participants to the CPI, who then approached the
patient about the study. Over the recruitment period the CPI was notified of two
potential participants at Austin Health, of which one was eligible and approached to
participate.
57
EXCLUDED AT RECRUITMENT (total n = 127) INELIGIBLE (n = 113)
Observation only/not returning n = 24 Resected disease/remission n = 15 Treatment outside recruitment site n = 19 NET primary location outside GI tract n = 5 >6 weeks post initial appointment n = 14 Diagnosis/plan unclear n = 3 Revised diagnosis, not NET n = 30 Not new to service n = 2 End-stage disease/palliative n = 1
ELIGIBLE BUT NOT RECRUITED (n = 14) Declined participation n = 9 Researcher away/unwell n = 2 Missed in clinic n = 2 Unable to contact n = 1
Assessed for eligibility n = 188
Total recruited n = 61
DATA AVAILABLE FOR ANALYSIS
Baseline (T0) n = 59 Two-month follow-up (T2) n = 45
Four-month follow-up (T4) n = 39
Six-month follow-up (T6) n = 47
T2 MISSING DATA (n = 14)
Not attending site n = 13
Deceased (withdrawn) n = 1
WITHDRAWN (n = 2)* Revised diagnosis/not NET n = 1 Primary treatment for other cancer n = 1 *Excluded from all analysis
T0
T4
MISSING DATA (n = 19) Not attending site n = 16 Palliative/not returning (withdrawn) n = 2
Transfer to another hospital (withdrawn) n = 1
T6
MISSING DATA (n = 8) Not attending site n = 6 Deceased (withdrawn) n = 1 Personal reasons (withdrawn) n = 1
Figure 3.1 Participant recruitment map according to STROBE criteria
58
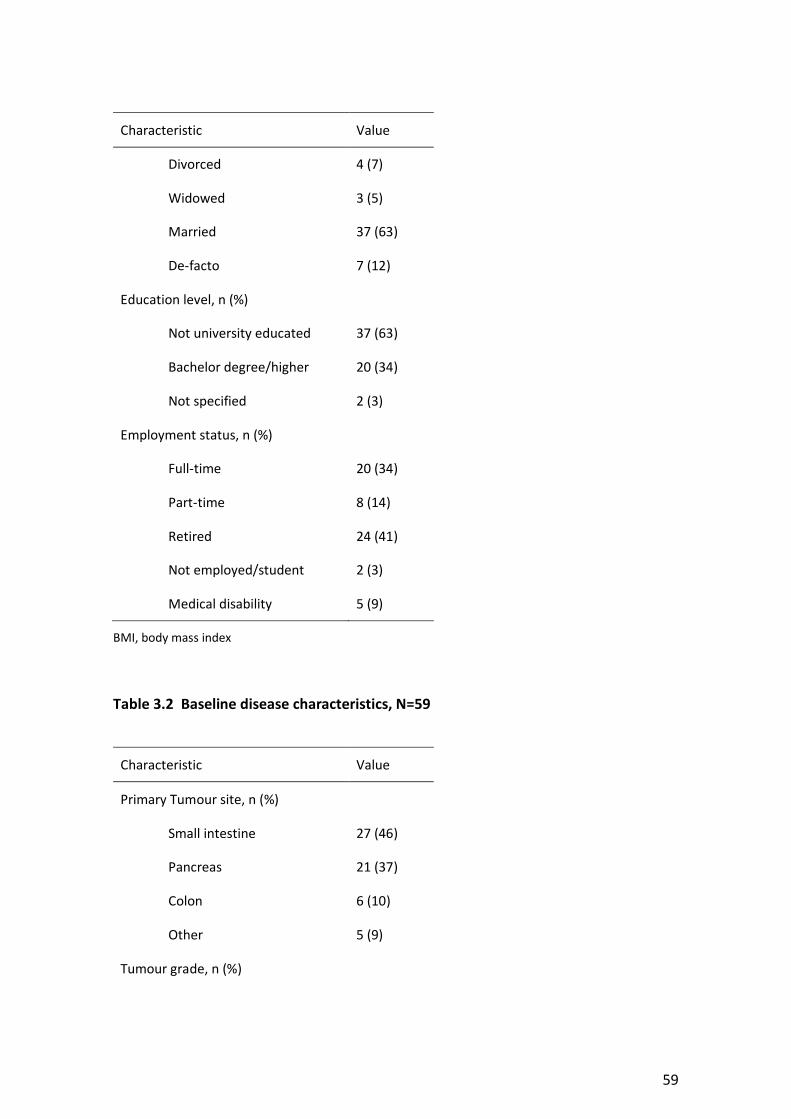
Baseline demographic and disease characteristics are shown in Tables 3.1 and 3.2. Only
eight participants (14%) had a functional tumour classification documented in their
medical notes. Fourty two (73%) participants had been diagnosed with a NET for less
than six months. Four (7%) participants were diagnosed with a NET several years prior
to participation in this study. These participants had been diagnosed and received
treatment primarily at health services in other Australian states and outside Australia,
and at time of recruitment, had been recently referred to a study site for specialist NET
care. Nine participants (15%) were residents in New Zealand who had travelled to the
study site for specialist NET care. All other participants (n=50/85%) were Australian
residents.
Table 3.1 Baseline demographics, N=59
Characteristic Value
Age (years), median (IQR) 64 (55, 70)
Weight (kg), median (IQR) 76 (65, 94)
BMI (kg/m2), median (IQR) 27 (24, 31)
Sex
Male, n (%) 39 (66)
Female, n (%) 20 (34)
Ethnicity, n (%)
Caucasian 50 (85)
Asian 5 (9)
Indigenous/Maori 1 (2)
Other Pacific Islander 1 (2)
African American 1 (2)
Marital status, n (%)
Single 8 (14)
59
Characteristic Value
Divorced 4 (7)
Widowed 3 (5)
Married 37 (63)
De-facto 7 (12)
Education level, n (%)
Not university educated 37 (63)
Bachelor degree/higher 20 (34)
Not specified 2 (3)
Employment status, n (%)
Full-time 20 (34)
Part-time 8 (14)
Retired 24 (41)
Not employed/student 2 (3)
Medical disability 5 (9)
BMI, body mass index
Table 3.2 Baseline disease characteristics, N=59
Characteristic Value
Primary Tumour site, n (%)
Small intestine 27 (46)
Pancreas 21 (37)
Colon 6 (10)
Other 5 (9)
Tumour grade, n (%)
60
Characteristic Value
NET G1 17 (29)
NET G2 22 (37)
NEC G3 10 (17)
Other 1 (2)
Unknown 9 (15)
Functional tumour classification, n (%)
Gastrinoma 4 (7)
Insulinoma 2 (3)
Glucagonoma 2 (3)
Unspecified 51 (86)
Metastatic, n (%) 45 (76)
Time from diagnosis, n (%)
<1 month 23 (40)
2-5 months 19 (33)
6-11 months 6 (11)
1-2 years 5 (9)
>3 years 4 (7)
Treatment received for NET, n (%)
Surgery 13 (22)
PRRT 5 (9)
Chemotherapy 8 (14)
SSA 24 (41)
Interferon 1 (2)
Other 2 (3)
No treatment 24 (41)
61
Characteristic Value
Co-morbid conditions with dietary consequences, n (%)
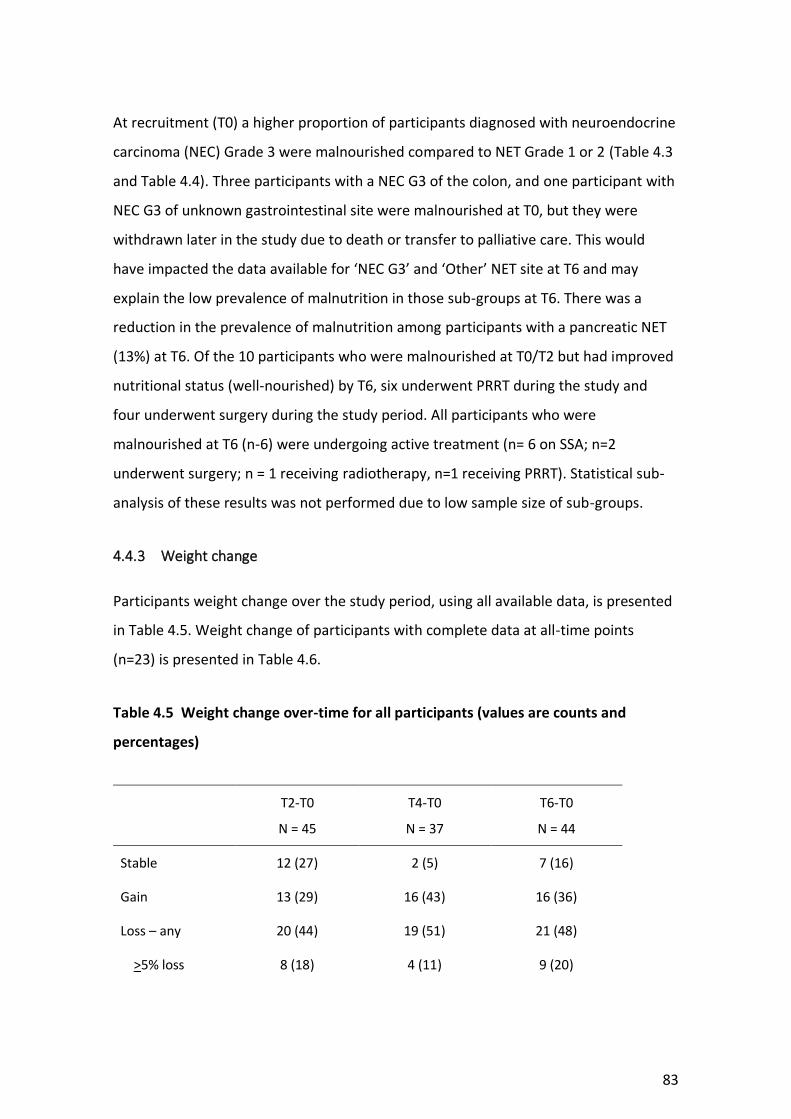
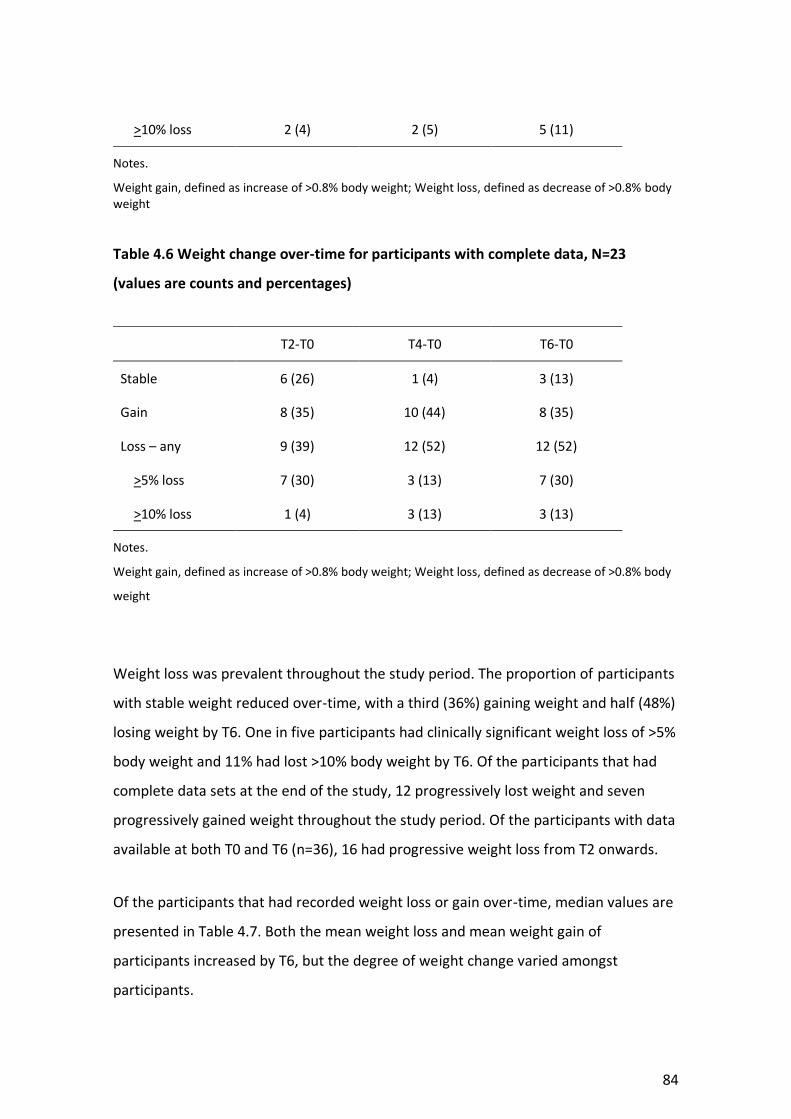
All p > 0.05 for score comparisons between 6 months post-baseline and baseline, excepting GINET21 Endocrine (p = 0.01), Social function (p = 0.02) and Disease-related worries (p = 0.002).
2002) (Bauer et al., 1997; Kondrup et al., 2003; Boléo-Tomé et al., 2012). These
screening tools focus on identification of weight loss, change to total food intake, and
identification of contributing acute disease factors such as surgery, or requirement for
102
intensive care (leading to no nutritional intake for >5 days), in the case of the NRS-
2002. In NET patients, common nutrition-related issues such as symptom burden and
dietary changes, may contribute to nutritional risk, but may not be identified using
current available nutrition screening tools. The applicability and validity of current
nutrition screening tools therefore requires further detailed exploration in a GEP NET
population. The PG-SGA Short Form (PG-SGA SF) may be a suitable nutrition screening
tool for GEP NET patients, as it incorporates the first four questions of the PG-SGA,
including change in amount of food intake, change in energy and daily function,
change in weight and symptoms impacting diet (Gabrielson et al., 2013), which are
factors relevant to nutritional risk in GEP NET patients as found in the Phase 1 study.
The PG-SGA SF has been shown to be a practical and valid nutrition screening tool in
oncology outpatients (Gabrielson et al., 2013; Abbott et al., 2016). Potential symptoms
included in the PG-SGA SF that may be relevant to GEP NET patients include diarrhoea,
pain, loss of appetite and fatigue. The question addressing food intake, is designed to
identify change in total food intake but not detailed changes of food restriction or
avoidance of particular food types, which were identified as common dietary changes
observed in GEP NET patients in our Phase 1 study. Review of current valid nutrition
screening tools and their suitability for use in patient with GEP NETs is recommended.
The development of a NET-specific supplement to combine with existing nutrition
screening tools may also need to be considered, if existing validated tools are unable
to capture NET-specific nutrition risks such as dietary change and restriction.
Commonly used nutrition screening tools have been demonstrated to under-diagnose
the presence of muscle wasting, sarcopenia and cancer cachexia when compared with
computed tomography, a gold standard technique for assessment of muscle mass (Ní
Bhuachalla et al., 2018). In data from the Phase 1 study, FFM loss was identified among
several participants who had stable weight and an assessment of well-nourished on
the PG-SGA, indicating deterioration in muscle mass is an underlying and unrecognised
problem in some cases. Clinicians should consider assessment of muscle mass in their
practice using validated body composition measures (BIA, ultrasound, computed
tomography (CT) or magnetic resonance imaging (MRI)) where available, in order to
103
assess underlying muscle mass changes, which is a concept supported by the recently
published GLIM criteria (Jensen et al., 2019). Assessment methods such as BIA, calf
circumference and the subjective muscle mass assessment on the PG-SGA, may be
more accessible and therefore suitable measures to be used in routine clinical practice
by health professionals, in comparison to the use of CT body composition analysis and
MRI. Validated assessment of muscle mass change would be particularly useful to
identify nutritional compromise in patients on prolonged treatment and those
reporting restricted diets, without evidence of overall body weight loss.
4.6 Conclusion
This is the first study to comprehensively assess the occurrence of nutritional
complications over-time among GEP NET patients, concurrently with the dietitian
intervention received. Study results show that malnutrition and nutritional
complications are prevalent but under-recognised among people diagnosed with a GEP
NET. Nutritional complications including weight loss, reduction in FFM and dietary
change are more prevalent than malnutrition, and under-recognised when using
available validated cancer nutrition assessment tools. More than half of the GEP NET
patients in this study reported a dietary change due to their diagnosis and symptoms,
but the precursor to this dietary change and the impact on nutrition and quality of life
requires further evaluation through qualitative methods. The prevalence of vitamin
deficiency was low in this study and larger multi-site trials are required to explore the
risk and prevalence of vitamin deficiency among GET NET patients. Nutritional
complications in GEP NETs are likely multi-factorial, due to the heterogeneous
population and high burden of symptoms. Under-recognition of nutritional
complications can lead to worsening morbidity and HRQoL for patients. Results
highlight the need to determine an appropriate method of screening and identification
of nutritional complications among and specific to GEP NET patients. Further
exploration of the impact of nutritional complications on the HRQoL of patients is also
required. Chapter 5 will consider insights from qualitative interviews completed with a
104
purposive sample of participants from the Phase 1 study and provide an in-depth
description of the occurrence and impact of nutritional issues on HRQoL.
105
Chapter 5: Living with a NET and the impact on nutrition
This chapter describes the aims, methods and insights from qualitative interviews
undertaken with patients within the context of the Phase 1 mixed methods study.
5.1 Introduction
The results of the Phase 1 longitudinal study presented in Chapters 3 and 4 showed
that social function and mental health are negatively impacted by a NET and its
treatment, and also that nutritional complications including weight loss, malnutrition
and dietary change are prevalent. Quantitative data showed that whilst dietary
changes were common, the nature of dietary changes (smaller meals, increased
frequency of eating, avoidance of specific food and drink types) varied amongst
participants. In this chapter, interview data from a purposive sample of Phase 1
participants, provides in depth insight to the types of dietary changes participants
engaged in, reasons why they altered or changed their diets in the way that they did,
and the impact of these changes on their HRQoL. There has been little exploration of
dietary habits among patients living with a NET, and although findings from a series of
small cross-sectional observational studies (Davies and Caplin, 2009; Lind, Wängberg
and Ellegård, 2016; Gallo et al., 2017; Barrea et al., 2018) indicate a similar presence of
dietary change to that described by participants in this study (phase 1), they provide
limited insight to types of changes made by people in response to their disease and
treatment, factors leading to those changes and whether the changes impact people’s
perceptions of their nutritional status and HRQoL.
An important aim of this component of the PhD study was to generate a new
understanding of the changes patients made to their dietary intake, their perceptions
of their nutritional status and symptoms experienced, and the perceived impact of
these on HRQoL. The extent of nutrition advice and intervention received to help
address nutritional issues was also explored to help contextualise patients’ responses
to the impact of nutritional issues. In order to address these aims, a purposive sample
106
of Phase 1 participants were invited to take part in two semi-structured, audio-
recorded interviews at entry to the study and at six month follow up.
5.2 Aims and objectives
5.2.1 Aim
To explore and describe the experiences of people living with a GEP NET, to better
understand the impact of disease and treatment-related nutritional and dietary
changes on HRQoL.
5.2.2 Objectives
1. To explore and describe how and whether NET and treatment-related nutritional
changes impact peoples’ HRQoL
2. To explore and describe whether nutrition needs (nutritional status and dietary
intake patterns) change after a diagnosis of NET
3. To explore and describe what help (if any) participants reported receiving from
clinicians regarding their nutrition issues
5.3 Methodology
The interviews were undertaken within the context of the Phase 1 mixed-methods
study (Chapter 2). They were undertaken to ensure opportunity for patients to
describe their experiences of nutritional changes and impacts through interviews,
offering rich insights to complement the Phase 1 quantitative data. The research
perspective underpinning this qualitative data component was realist, that is, the
intent was to provide participants with an opportunity to report their personal
experience, of nutritional complications and what this meant for them in their unique
contexts.
107
An exploratory, descriptive approach was used to inform the qualitative study. As
described by Braun and Clarke (2006), an exploratory, descriptive approach is used to
generate data when a person describes their reality and experience of a specific event
or occurrence, in their own words (Braun and Clarke, 2006). As such the approach
aligned with the realist perspective underpinning the study. An exploratory, descriptive
approach enables focus on topics of interest, explored through tailored or targeted
interview questions; i.e. in this study, the experience of participants in regard to
nutritional complications (dietary change, weight change), HRQoL and access to
nutrition information. These insights were considered important to guiding future
interventional research and patient-centred, educational and preparatory information
solutions.
Data were generated through semi-structured interviews. A semi-structured format
was chosen to focus participant responses towards topics of interest (nutrition, dietary
change and HRQoL), but also so as not to restrain discussion of their experience and
issues of importance to them. Interviews were chosen to explore individual patient
experience, acknowledging that this could be different due to specific disease and
treatment factors, personal beliefs or social influences. For this reason, individual
interviews were chosen as the data collection method of choice over other qualitative
data collection approaches, for example, focus group.
A thematic content analysis approach was applied to the data generated (following
Braun and Clarke) allowing for identification of unique and shared experiences across
the participant interviews, and details of the processes undertaken are described
below.
The context of the qualitative patient interviews within the Phase 1 study is
demonstrated in Figure 5.1.
108
Dietitian intervention
Structured survey
HRQoL data
EORTC questionnaires, HADS, COST-FACIT
Nutrition data
Objective assessment of weight, FFM,
nutritional status, vitamin status
Dietary habits (structured survey)
Quantitative data Qualitative data
Patient interviews
Data extracted:
Prevalence of nutritional complications
(mean/SD, proportions)
HRQoL status (mean/SD scores)
Data extracted:
Coding and themes
Quotes
Theoretical thematic content analysis
Exploration of the nutritional complications and HRQoL among patients with GEP NET
Outcome:
Description of HRQoL and presence of
nutritional complications
Occurance of intervention during study period
Outcome:
In-depth description of patient experience and
how it relates to nutritional complications and
their impact
Exploration of nutrition information and
intervention sought and received by GEP NET
patients
Phase 1 study
Figure 5.1 Mixed-methods approach to Phase 1 study
109
5.4 Methods
5.4.1 Recruitment and sampling
A purposive sample of participants who had consented to take part in the Phase 1
study were invited, at time of recruitment, to take part in two semi-structured, audio-
recorded interviews - one at recruitment and another six-months later. A purposive
sampling method was used for two reasons: to ensure a diverse representation of
participant experiences as part of the interview data, and to focus on inclusion of
participants from the Phase 1 study that had reported making a dietary change as a
result of their NET diagnosis. Where possible, it was intended to achieve diversity with
regard to participant demographics, diagnosis, and treatment type; which enabled a
heterogeneous sample representative of the NET population. A benefit of purposive
sampling in qualitative research is identification of individuals or groups that have
experience with or are knowledgeable about an aspect of interest to the research
question (Patton, 2015). In the case of these interviews, the focus was to explore
patient experience in regard to nutritional issues and dietary change, therefore it was
considered important to ensure sampling of participants that reported making a
dietary change during the Phase 1 quantitative questionnaires. Therefore, participants
who reported making a dietary change due to their NET diagnosis in the Phase 1
questionnaire, 1.0 Section 2.0 (details in Chapter 2, Section 2.5.11), were approached
to consider taking part in the interviews. A maximum of 15 interviews were intended
to be completed based on evidence that data saturation (where no new themes
emerge from interviews) commonly occurs after 10-12 interviews (Creswell, 2007).
Interviews were undertaken six months apart, to explore whether participants
described different experiences over time, after medical management and treatment
at a specialist NET referral hospital.
Eligible patients were approached to participate in an interview by the lead researcher
(PhD student) after completion of baseline data collection for the Phase 1 study.
Responses to Questionnaire 1.0 Section 2.0 was checked prior to determine the
patient’s eligibility for an interview. It was explained that consent to the interview at
110
baseline would also mean consent to participate in a repeat interview in six-months
(although this was verbally re-checked at the six month interview timepoint). Eligible
participants were told interviews were optional and they could continue to participate
in data collection the Phase 1 study if they chose to decline the interview. Verbal
consent was obtained from those willing to participate in an interview at time of
baseline data collection, and a time to complete the baseline interview by phone
within the following two-weeks was scheduled with the participant. Interviews were
audio-recorded.
Interviews were conducted via phone, or in-person at the request of the participant,
within two weeks of initial recruitment to the Phase 1 study for the baseline interview,
and within 2 weeks of the six-month (T6) data collection point for the six-month
interview. All interviews were conducted by the same researcher (PhD student). Verbal
consent was audio-recorded prior to the start of each interview. Ethics approval for
patient interviews was obtained from the Peter MacCallum Cancer Centre Human
Research Ethics Committee (HREC/17/PMCC/7) in April 2017.
5.4.2 Interview questions
A semi-structured interview schedule was developed by the lead researcher (PhD
student) and reviewed by supervisors, one of whom is experienced in qualitative
research methodology. Questions were informed by the teams’ clinical expertise as
well as published evidence available. A total of 12 key questions (with corresponding
prompts) were designed for the first interview, and 11 questions (again with prompts)
for the six-month interview. Questions were structured to prompt discussion of
patients’ experiences in regard to the aims described above in Section 5.2. Interview
questions at six-months were aligned with those at baseline, with language modified
to reflect the period of time that had passed since the previous interview. The
interview schedule is included in Appendix 4. Four questions addressed participant
experience of dietary and nutritional changes and impact on quality of life before and
after their diagnosis, with a focus on symptoms and access to information; two
111
questions addressed emotional health and coping with the diagnosis; and six questions
addressed the impact of the NET diagnosis on nutrition including weight change,
eating, and the extent of nutrition advice and intervention received. Questions were
piloted with two consumers from NeuroEndocrine Cancer Australia (formerly the
Unicorn Foundation), who had a diagnosis of a NET to test clarity and flow of
questioning.
5.4.3 Thematic content analysis
Interviews were audio-recorded and transcribed verbatim by a party external to the
research team. Thematic content analysis as described by Braun and Clarke informed
the approach to data analysis (Braun and Clarke, 2006). The transcripts were read and
re-read to ensure familiarity with the content and to begin to identify recurring themes
or issues raised by participants. Content from individual interviews were initially coded
against interview questions (theoretical approach at semantic level analysis) to identify
recurrent themes common to or unique to individuals across the data sets (at baseline
and at six months). Interview data were coded into data extracts (quotes or lines of
text) by the lead researcher (PhD student) and extracts grouped into emergent
themes. Themes did not necessarily reflect content most commonly talked about, but
rather represented areas of particular relevance to the topic areas of interest for the
research. That is, things were not regarded as important by virtue of how often they
were referred to, but rather by how meaningful they were to participants in response
to questions answered. Interview data were coded against the 12 key interview
questions to enable initial description of content, then further exploration of coded
responses and overall content was conducted to generate themes from the baseline
and six months-interviews. As the same questions were asked at both the interview
time points, themes identified at the first interview were used to guide the six months-
interview questions, but this did not exclude opportunity for new themes to emerge,
or for participants’ changing experiences over time.
112
A cross-section of interviews was independently coded by a supervisor to check inter-
rater reliability across common themes identified. There was minimal inter-researcher
variation in theme recognition at both time points, and all themes were discussed to
ensure consensus.
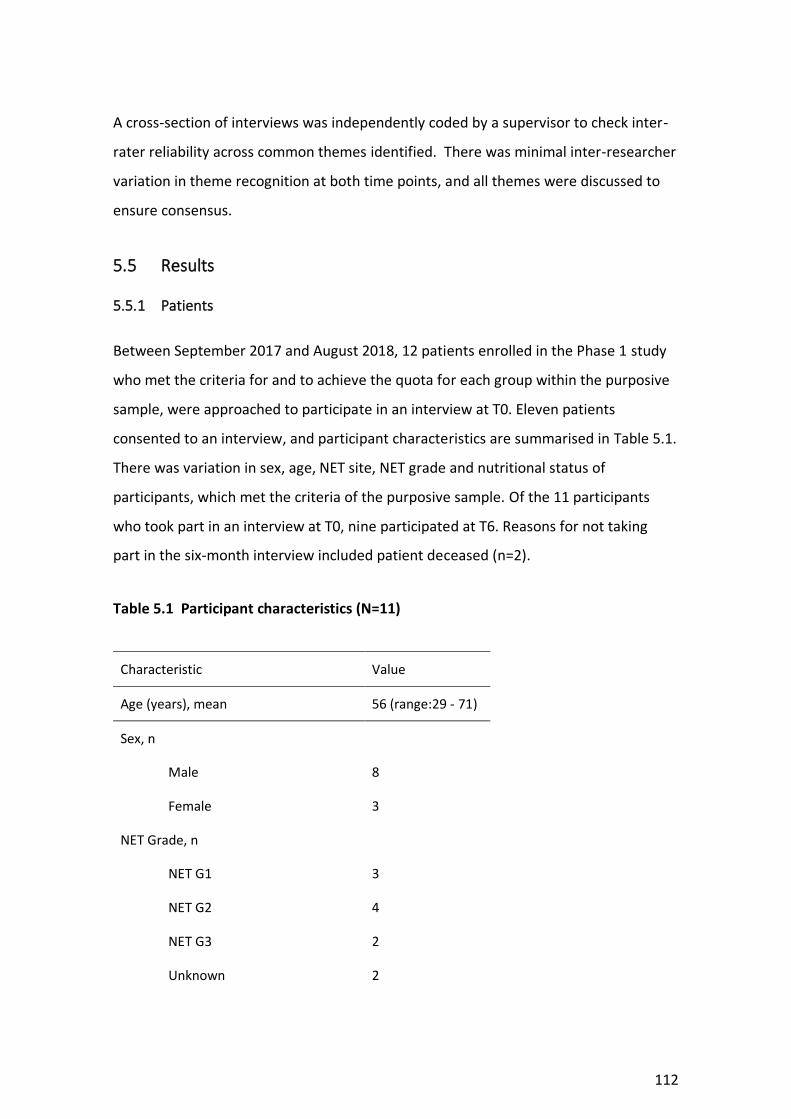
5.5 Results
5.5.1 Patients
Between September 2017 and August 2018, 12 patients enrolled in the Phase 1 study
who met the criteria for and to achieve the quota for each group within the purposive
sample, were approached to participate in an interview at T0. Eleven patients
consented to an interview, and participant characteristics are summarised in Table 5.1.
There was variation in sex, age, NET site, NET grade and nutritional status of
participants, which met the criteria of the purposive sample. Of the 11 participants
who took part in an interview at T0, nine participated at T6. Reasons for not taking
part in the six-month interview included patient deceased (n=2).
Table 5.1 Participant characteristics (N=11)
Characteristic Value
Age (years), mean 56 (range:29 - 71)
Sex, n
Male 8
Female 3
NET Grade, n
NET G1 3
NET G2 4
NET G3 2
Unknown 2
113
Characteristic Value
NET site, n
Small intestine 6
Pancreas 3
Gastric 1
Unknown 1
Nutritional statusa
A (well nourished) 5
B (suspected/moderate malnutrition)
5
C (severely malnourished) 1
Notes.
aAs calculated by PG-SGA global status score
5.5.2 Insights from the baseline interviews
Four key themes were identified from the baseline interviews. The themes were
uncertainty, complexity, conflicting advice from health professionals, and self-
management/seeking information. For each theme, a number of sub-themes were also
identified. These are presented in Table 5.2, along with quotes to help illustrate each
theme.
Participants reported a variety of symptoms related to their NET, including diarrhoea,
fatigue, pain, flushing, bloating and wind, bowel obstruction and difficulty swallowing,
and altered blood sugar levels. Diarrhoea was a symptom frequently described by
participants to be a significant burden on their day-to-day activities and quality of life.
When asked about how they were coping with their diagnosis, common responses
from participants included ‘fear’, ‘poor quality of life’, ‘draining’, and ‘feel depressed’
and general concern for the impact of their diagnosis on their lives and their family.
114
The impact of a NET on quality of life was frequently reported by participants, partially
in relation to work and the inability to perform their work to the same degree as prior
to diagnosis, which had negative financial impacts as well. The impact of a NET
diagnosis on family and social relationships and activities was reported by some
participants. They reported that family members were burdened by the uncertainty of
a NET diagnosis and observing the patient be unwell or experience symptoms. As a
result, family members often attempted to help by providing nutrition advice or
suggesting dietary modification to help them feel better. Due to various symptoms
experienced by participants; in particular gastrointestinal symptoms such as diarrhoea,
bloating and abdominal cramps/wind; social activities and eating out were restricted
due to fear of experiencing symptoms in public and the limitations of restricted eating
habits.
115
Table 5.2 Themes identified
Theme Sub-themes Quotes
Uncertainty ● Diagnosis and prognosis
● Treatment planning and outcome
● Information
“It’s just uncertainty. I’m still pretty uncertain about the diagnosis…uncertain about how the treatment is going to work and just uncertain about time”
“At this stage I don’t know whether I’m going to live for two years or whether I’ll see ten”
“A lot of those physical activities I did or used to do I’m unable to do now…we’ll see over the next four treatments how well I respond and whether I can get back to where I was”
“I sort of wanted something [information] that would say for NET patients…I just wanted it more specific for a NET cancer”
“I haven’t had the answers [to my questions]”
Complexity ● Symptoms
● Long-term disease burden
● Nutritional impacts and behaviours
“NETs appear quite fickle so everybody gets slightly different symptoms, the symptoms aren’t consistent, symptoms can often be marked by something else”
“They [treatments] may or may not work for me so what’s an estimated timeline of 5-10 years could be anywhere from 2 years with lots of complications, or you know beyond 10 years with very few complications”
“I’ve kind of had to put my life on hold because I really don’t know what we were exactly dealing with”
“I’ts all too hard [referring to eating]”
“I was sent to a dietitian and they put me on an extreme low carb diet but I’d still have something to eat and it still goes through me”
116
Theme Sub-themes Quotes
“Just [avoid] fruit, meats and low carb potatoes and things like that. Green veggies and not to eat anything that, you know sweet things like that”
“I’ve eliminated stone fruits and dried fruit and onions and garlic, and all the things I used to love eating”
Conflicting advice ● Limited confidence in health professionals
● Confusion with nutrition messages
“Most GPs never see a NET in their careers”
“I’m not quite sure where I should be going with all of this, you know nutrition wise, what I should and shouldn’t eat”
“I was sent to a dietitian and after a little while they put me on a low carb diet…extreme low carb diet [but] I’d still have something to eat and it still goes through me”
“Nutrition-wise, what I should and shouldn’t eat or what’s best that I do or don’t do. That’s why I’m feeling a bit you know in the air about it at the moment”
“I went to some dietitian who was basically sitting there googling possibilities while we were in the room”
“She just said she didn’t know what advice to offer me and she just gave me a printout on the FODMAP diet”
Self-management and seeking information
● Responsibility to manage own care and information
● Nutrition important to patient
“The more I learnt about NET the more I learned it can have effects on absorption of vitamins and minerals, things like that then yeah they should [offer advice about]”
“I’ve just sort of been self-helping and looked up these discussion boards and they’ll talk about what sets them off worse and then I sort of take that on board and I’ll stop having that in my diet”
117
Theme Sub-themes Quotes
“I would’ve loved to have had a brochure sit up there amongst all the other cancers just giving all those basic advice…that was the biggest thing missing in my first six months of diagnosis”
“I think it would be brilliant to have an information sheet on nutrition [for NETs], because as I say the oncologists a) they don’t understand NET, b) if the do understand NET they focus on treating the cancer. They don’t focus on looking at side-effects”
118
5.5.3 Uncertainty
One of the key themes identified was uncertainty. This related to a NET diagnosis and
prognosis, which underpinned and contributed to patients’ experiences and
behaviours with regard to their well-being and relationships with friends and family.
People described the uncertainty of a living with a NET diagnosis on their quality of life,
with some describing the uncertainty as causing a feeling of lack of control over their
situation. Several patients experienced a prolonged time to diagnosis and prolonged
treatment planning, which added to their uncertainty of what illness they had and how
serious or impacting on their life it would be. Two participants emphasised their
uncertainty regarding prognosis and the impact of their NET on their length of life,
after being told by medical professionals that they were unable to provide a clear
prognosis. This had an emotional impact on these participants, causing distress, and a
lack of control. One participant said:
“It’s just uncertainty. I’m still pretty uncertain about the
diagnosis…uncertain about how the treatment is going to work and just
uncertain about time”- Patient 3
Another participant said:
“At this stage I don’t know whether I’m going to live for two years or
whether I’ll see ten” – Patient 7
There was uncertainty regarding expectations of treatment, how it would impact their
current symptoms (i.e. would they improve or worsen), and the impact on their length
and quality of life. One participant said:
“A lot of those physical activities I did or used to do I’m unable to do
now…we’ll see over the next four treatments how well I respond and
whether I can get back to where I was” – Patient 1
119
Uncertainty regarding symptoms and their impact on quality of life over time was
particularly pronounced for some participants, specifically those who reported
experiencing diarrhoea. Diarrhoea was reported to have a considerable impact on
quality of life, particularly if severe (more than 6-10 times per day), as it inhibited their
ability to leave the house. As many participants had only commenced treatment or
were still in the treatment planning phase, they were unsure as to how long they
would be burdened with severe diarrhoea and how it would impact their life longer-
term. One participant described the severity of their diarrhoea:
“I could be going [to the toilet] up to 20 to 30 times a day” – Patient 6
The same participant described the impact of their diarrhoea on their ability to leave
home:
“It’s like you’d go to the toilet and then 10 minutes later you need to go
again and it was just fluids you know, coming out, it was just terrible…I
couldn’t go anywhere because I needed to near a toilet” – Patient 6
Participants spoke about the emotional burden of their diagnosis on themselves and
their families, particularly because they felt uncertain and fearful about the impact on
their length of life (risk of death) and how their diagnosis and treatment might impact
how they live their life and their ability to physically and financially support their
family. Those with partners and children described the impact of this uncertainty on
those close to them. One participant said:
“The cancer is affecting my family, my wife and my children because you
know it’s something hard to get your head around but as I say you can’t do
much about it you just gotta keep on going on” – Patient 4
Most participants were aware that their disease was rare and learnt, often through
their own research, that information and guidance about their disease management
120
was not readily available to them. Some participants reported being unsure where to
access timely and accurate information about NETs but were also unsure regarding
what information would be helpful for them. This was particularly heightened for
participants who had received care or treatment at a health service that did not have a
specialist NET referral centre, unlike the centre where this PhD project was
undertaken. These participants spoke about having initial contact with health
professionals that had limited experience in the management of NETs. In these cases,
they felt unable to access sufficient information or support for their disease, and
experienced uncertainty regarding their prognosis and expectations of treatment.
Participants who’s first contact with medical professionals after a NET diagnosis was at
the study site, reported good receipt of information, and improved clarity regarding
treatment planning, in comparison with participants who had initial contact with
medical professionals at non-NET specialist health services.
5.5.4 Complexity
The theme of complexity was evident throughout all of the interviews and related to
several factors including pathway to diagnosis, morbidity and symptom burden,
nutritional impacts of a NET and nutrition-related behaviours. The path to NET
diagnosis and treatment was reported as complex, with some participants recalling
multiple conversations with different doctors before having a clear diagnosis, and
some participants undergoing tests and treatment at other centres with limited clarity
on their diagnosis, before being referred to the study site. One participant said:
“Nobody seemed to know anything about it [NET] and even recently well
certainly in Wellington um the first oncologist I was under there had no
understanding of NET and he just assumed you’d be dead.” – Patient 1
Another participant spoke about his experience over-time since his NET diagnosis:
121
“I feel as though I’ve been neglected um quite a bit over my journey with
not having treatment, not getting the right scans done. I’ve had to it wasn’t
until I went to a support group of my own volition that I found out about
the PRRT um treatment” – Patient 6
People described experiencing various symptoms related to their NET including
diarrhoea, fatigue, pain, flushing, bloating, wind, difficulty swallowing and altered
blood sugar levels. Complexity surrounding symptom burden was observed due to the
variation in symptom type and severity reported by participants, and the range of
impacts symptoms had on quality of life and daily function. Examples of symptom
burden impacting quality of life included reducing their confidence to leave their
home, reducing their ability to socialise with friends or family (particularly over food),
and persistent symptoms causing mental distress. One participant described the
impact of their diarrhoea on their ability to leave the house:
“I have to probably go to the toilet three times before I can leave the
house…safely leave the house”- Patient 1
Another participant also described their trouble with diarrhoea:
“worry about you know that you’re gonna get diarrhea or not or have to
leave early because of it or you know you got to cancel before you even
went out because it was um a bit rife so yeah it’s had had a big negative on
my life actually” – Patient 6
Another participant spoke about the impact of their NET diagnosis on their social life:
“Apart from not being out go out socially um on a weekend or an evening I
lost my social circle” – Patient 8
Participants reported continuously monitoring their symptoms and searching for
strategies to manage or improve them, which often involved attempts at dietary
122
change, including food avoidance and altered meal patterns. Some participants
described the ongoing impact of symptom burden on their quality of life, whereas
others reported finding a way to live with their symptoms, by mentally accepting them
as part of the disease process and through developing strategies to enable
continuation of daily activities.
Complex nutritional impacts and nutrition-related behaviours
Participants reported various changes to their diet and nutrition as a result of their NET
symptoms and diagnosis. Table 5.3 outlines the type of dietary changes reported in the
interviews and the frequency in which it was reported.
Table 5.3 Reported dietary changes
Food/drinks avoided (n) Other changes (n)
Milk/dairy (4) Smaller meals/eats less (5)
Alcohol (2) Healthy food (4)
Spicy (2) Avoids sweets (2)
Egg (2) FODMAP diet (2)
Bread (2) Vegan diet (1)
Meat (1) Low carb (1)
Stone fruit (1) Avoid preservatives (1)
Dried fruit (1)
Onion/garlic (1)
Tomato (1)
Cauliflower (1)
123
There was considerable variation in the types of dietary changes reported by
participants (Table 5.3). The majority of dietary changes were in response to a degree
of symptom burden, but dietary change was also reported by people who were
asymptomatic. People who were asymptomatic described attempts to change their
diet to be more healthy (commonly increasing fruit and vegetables, reducing fat), as
they felt it would improve their treatment and recovery from their NET.
There were numerous symptoms reported by participants to impact their diet,
including early satiety/feeling full, bloating, wind/gas, nausea, diarrhoea, pain,
dysgeusia, vomiting, flushing and high/low blood sugar levels. Participants were most
likely to reduce their meal size and eat less overall if experiencing symptoms of early
satiety, bloating, diarrhoea, and vomiting. Participants who reported experiencing
regular diarrhoea, would generally eat less overall or modify the foods they ate for fear
of worsening diarrhoea and needing to use the toilet. One person said:
“It doesn’t matter what I eat. Whatever I ate came out” – Patient 2,
another stated,
“I realized certain foods like milk so dairy products that used to bring on
bouts of diarrhoea” – Patient 6
Dietary changes initiated due to diarrhoea included reduced meal size or eating less,
less spicy food, less dairy or milk, less meat, less bread, less fruit, and less onion and
garlic. Participants reporting dairy and spicy food contributing to their diarrhoea, but
the dietary changes were based upon individual experience. Participants experiencing
symptoms of bloating, wind/gas and abdominal pain reported these being worsened
by some food types including dairy, garlic, meat, tomato or acidic products, and spicy
foods, but there was observed variation in individual experiences and attitudes
towards the types of food that were worsening their symptoms. Weight loss was
reported more often than weight gain by participants at baseline. Despite their weight
history or status, it was evident that many were continuously monitoring their weight
124
and used it as a measure of their overall health status. One participant described their
experience with weight loss and managing their changing body shape:
“just trying to um maintain my weight at least rather than lose any more
but you know and just to put some back – all the weight that I had put
back’s gone straight to me stomach. Nothing in my arms or legs or anything
like that but yeah....it’s not exactly where I want it but at least I’ve turned
the corner of losing weight so....I’ll just try and manage my shape now” –
Patient 6
Impact of diet and weight change on quality of life
The impact of dietary change on quality of life was described by many participants.
People talked about the impact on social activities and relationships, with several
describing difficulty in eating out and socialising with friends during a meal due to
restrictions on their diet and tolerance of food. One participant said:
“I can’t eat this and I can’t eat that and it’s becoming harder and harder
because you can’t go to all places or have all different sorts of food…It
affects you socially because everyone has to change what they want
because you can’t have what’s [food] on offer” – Patient 8
Another said in reference to meeting friends out for dinner:
“I went out but I just couldn’t eat anything” – Patient 9
One participant described the impact of their diet and symptoms on his/her ability to
travel outside the house and on holiday, citing a need to pack their own food:
“I often take food with me you know if I go on a plane trip I’ve always got a
packet of rice biscuits and boiled eggs, things like that”. – Patient 5
125
The impact of weight change on quality of life was described but less pronounced than
dietary change. Participants who had experienced weight loss were regularly
monitoring their weight and conscious of their weight status. They reported that
weight loss contributed to the symptom of fatigue and limited their function in regard
to physical activity. One participant who had experienced weight gain reported
medicine physician, allied health (psychologist, psychiatrist, physiotherapist, social
worker, dietitian).
A Participant Information and Consent Form was sent to eligible health professionals
via email, with details regarding the study and the proposed focus groups. Health
professionals were asked to return an email to the lead researcher (PhD student), with
the signed consent form attached, if they agreed to participate. Focus groups were
then scheduled once consent was obtained from a minimum of ten health
professionals (to ensure adequate numbers for a meaningful focus group). An attempt
was made to include a minimum of three participants in each focus group (in addition
to the facilitators). Attempts were made to ensure a multidisciplinary sample of health
professionals in each focus group where possible. If a health professional provided
consent but was unable to participate in a scheduled focus group, they were offered
an individual phone interview with the lead researcher that addressed the same
questions as those addressed in the focus groups.
7.3.3 Focus group facilitation
Focus groups were facilitated by the lead researcher (PhD student) and one additional
facilitator who was external to the research team, for the purpose of monitoring and
addressing potential bias, as the lead researcher was known to some of the
participants. The lead researcher was responsible for asking participants the schedule
of questions (Appendix 5), whilst both facilitators asked follow-up or probing questions
as appropriate/required. At the end of the focus group, both facilitators reflected
together on the session to ensure that the lead researcher had not influenced the flow
or content of responses, and to check that the key aims of the focus group had been
achieved.
7.3.4 Focus group questions
Proposed questions for focus groups were established after completion of a
comprehensive review of relevant literature (literature review published in Chapter 1).
188
Further revision of questions occurred after review of results of the health professional
online survey described in Chapter 6. The focus group questions and schedule is
included in Appendix 5. Based on the literature review and survey responses,
questions were designed to address three key themes: the importance of nutrition
within the overall context of a NET patients care, screening and management of
malnutrition and vitamin deficiencies in NET patients, provision of nutrition advice. De-
identified demographic information was collected from each participant at the
commencement of a focus group or interview, including discipline (area of speciality),
length of time working with NET patients, and average number of NET patients they
manage per year.
During the focus groups, the lead facilitator proposed each question to participants as
outlined in the schedule (Appendix 5). As appropriate during the focus groups, further
probing questions were asked of participants to seek clarity or elaboration about
issues or concepts they were speaking about. An example of this probing is provided
below:
“There’s been a couple of points about diet changing or patients wanting to change
their diet to manage diarrhoea. In what way have they reported making changes in
that regard? Do you have any examples?”
7.3.5 Data management and Content analysis
Focus groups were audio recorded and audio data were stored electronically, and
password protected. Audio data were transcribed verbatim by a party external to the
research team. Analysis of transcriptions was undertaken by the lead researcher (PhD
student) and another researcher with qualitative research experience, who was
external to the research team.
A process of content analysis was applied to the focus group data as the intent was to
use a deductive approach, where analysis of focus group data was guided by evidence
from existing literature (as presented in Chapter 1), and results from the quantitative
189
health professional survey discussed in Chapter 6. Initial content analysis was
undertaken based upon a question-by-question format (Krueger, 2002), using the eight
key questions proposed to participants. The main purpose of focus groups was to
generate additional in-depth data relating to key topics of interest proposed in the
health professional survey. Therefore, initial content analysis of question responses
was performed to summarise and explore health professional practices in relation to
key topics, that were also explored in the Health professional survey (Chapter 6), that
is: health professional perceived occurrence and importance of nutritional
complications among NET patients (Questions 1, 2 and 3), malnutrition screening and
management practices (Question 4), vitamin deficiency screening and management
practices (Question 5), provision of nutrition advice (Question 6), and the use and
availability of evidence-based guidelines (Question 7). Data from transcripts were
coded against these questions using manifest content analysis, in order to summarise
responses based upon topics of interest and to identify commonality in responses to
questions.
Both researchers then re-visited the transcriptions and undertook further content
analysis, using a latent analytical approach, to identify emerging themes across all
health professional focus groups and interviews. A latent analytical approach seeks to
examine underlying ideas, assumptions and concepts that inform the content of the
data (Braun and Clarke, 2006). The intent of latent content analysis in this study was to
generate themes relating to the experiences of health professionals that influence
their practice and decisions regarding nutrition-related complications in NETs. This
approach enabled in-depth exploration and interpretation of the reasoning and
barriers behind nutrition-related practices, thereby contributing to the aim of
generating data that can inform future NET-specific nutrition guidelines. The content
analytical approach is summarised in Figure 7.1.
190
Figure 7.1 Focus group content analysis
Manifest content analysis
Coding against topics:
1) Health professional perceived occurrence and
importance of nutritional complications among NET
patients
2) Malnutrition screening and management practices
3) Vitamin deficiency screening and management
practices
4) Provision of nutrition advice
5) Use and availability of evidence-based guidelines
Related question:
Questions 1, 2, and 3
Question 4
Question 5
Question 6
Question 7
Latent content analysis
Health professional experience
and influential factors of their
nutrition-related knowledge and
practices
Themes
191
Descriptive statistics were used to report participant demographic data.
7.4 Results
7.4.1 Participant characteristics
Thirteen of 18 health professionals working in the NET unit at Peter Mac took part in
either a focus group or phone interview in July 2018. Three focus groups were
conducted, with a range of two to five participants in each group. All focus groups
were scheduled with a minimum of three participants, however, one participant had to
reschedule their attendance at last minute and therefore one group was conducted
with only two participants. Participant characteristics are described in Table 7.1. There
was a range of different professions represented in the focus groups and interviews.
Nine of thirteen participants reported working with NET patients for at least five years,
and nine reported managing over 50 NET patients per year on average (Table 7.1).
Table 7.1 Focus group participant characteristics
Characteristic n
Discipline
NET nurse 3
Medical oncologist 3
Surgeon 2
Nuclear medicine physician 2
Endocrinologist 1
Dietitian 2
Number of years working with NET patients, n (%)
< 1 year 1
1-2 Years 3
2-5 years 0
192
5-10 years 7
Number of years working with NET patients, n (%)
>10 years 2
Number of NET patients managed per year, n (%)
<10 1
10-20 3
20-50 0
50-100 6
>100 3
7.4.2 Results of initial content analysis
Responses to the each of the key questions proposed during the focus group were
summarised (manifest content analysis) and then reviewed by two researchers to
undertake latent content analysis to identify strong and recurring themes in the data
set.
Through a process of manifest content analysis there was considerable similarity in the
majority of responses to each question posed to focus group participants. A summary
of initial coding per topic area/question is provided in Table 7.2.
193
Table 7.2 Results of initial coding per topic area
Topic area Related question(s)
Summary of responses
Health professional
perceived occurrence and
importance of nutritional
complications among NET
patients
1, 2 and 3 - Responses varied when discussing if
nutrition was considered important
to patients, some believed it was
very important, others believed it
was less important that other issues
such as prognosis, treatment and
symptoms
- Symptom management was
considered by the majority to be
very important to address in NET
patients, and health professionals
said that symptoms (e.g. diarrhoea,
abdominal pain, bloating, weight
loss) often contributed to nutrition
issues
- The majority discussed that dietary
restriction and food intolerances
were common among NET patients
- The majority discussed that nutrition
issues, e.g. weight loss, malnutrition,
dietary restriction, impacted
negatively on patient quality of life
- The majority discussed that
malnutrition and weight loss is less
common in NETs than other
gastrointestinal cancers, but did
exist
194
Topic area Related question(s)
Summary of responses
- Malnutrition and weight loss were
considered issues mostly for patients
at end of life, with high-grade (grade
3) NET, and progressive disease
- Weight loss was considered less of
an issue for patients who were
undergoing PRRT, and who had
improved symptoms from their
treatment
Malnutrition screening and
management practices
4 - The majority said they did not
regularly or systematically screen for
malnutrition in their practice
- General questions to patients about
weight change or symptoms were
more common than routine
malnutrition screening, or use of a
validated nutrition screening tool
- Some health professionals said that
routine nutrition screening processes
in NETs could be improved, and
should form part of usual care
Vitamin deficiency screening
and management practices
5 - The majority of health professionals
did not screen for vitamin deficiency
in NET patients
- Some health professionals said it
was the responsibility of the dietitian
to prompt or perform screening for
vitamin deficiency
195
Topic area Related question(s)
Summary of responses
- Health professionals were more
likely to consider screening for
vitamin deficiency if the patient
reported weight loss to them
- The majority of health professionals
said that if they identified a vitamin
deficiency, they would be unsure
how best to treat it
Provision of nutrition advice 6 - The majority of health professionals
relied on the dietitian to provide
comprehensive advice to NET
patients, and would refer to the
dietitian for this purpose
- Non-dietitian health professionals
may provide general advice to
patients such as keeping a stable
weight, following a healthy diet and
symptom management
Use and availability of
evidence-based guidelines
7 - The majority of health professionals
identified a lack of evidence as a
barrier to their nutrition-related
practices, including provision of
nutrition advice and nutrition risk
screening
- The majority of health professionals
used general cancer or general
nutrition guidelines to aid their
practice with NET patients
196
Topic area Related question(s)
Summary of responses
- Some health professionals identified
a need for NET-specific nutrition
guidelines
- In the absence of NET-specific
nutrition guidelines, health
professionals discussed relying on
referral to a dietitian in their health
centre to aid in nutrition
management of patients
7.4.3 Results of latent content analysis
Latent content analysis was conducted after initial manifest content analysis, to
identify recurring themes in the data set, and provide in-depth exploration of health
professional experience and factors that influence their nutrition-related knowledge
and practices. Identified themes in some instances aligned closely with the key topics
of interest presented in Table 7.2, and some additional themes outside of those topics
of interest were identified.
Analysis generated seven key themes – symptoms are precursors of nutrition issues,
provision of nutrition information to patients, patient beliefs about food intolerances
and alternative diets, impact of nutrition issues on the quality of life of NET patients,
adequacy of malnutrition screening and barriers, adequacy of vitamin screening and
barriers, provision of specialised nutrition advice - along with one sub-theme (weight
change is dependent on treatment and symptom type), which are presented in Table
7.3 and described in detail below.
197
Table 7.3 Identification of themes
Theme Related topic Quotes
Symptoms are precursors of
nutrition issues
Health professional perceived occurrence
and importance of nutritional
complications among NET patients
“they will often describe things that make them [symptoms] worse if
we question them and ah there’s spicy foods typically and fatty foods
tend to upset them”
“we’ve all head I don’t wanna eat because it gives me diarrhoea”
“the most distressing weight loss is for patients who have had a
whipples by somebody and they get a lot of weight loss around the
time of surgery”
“the ones who have those sort of abdominal issues and the people
with high grade neuroendocrine tumours [lose weight]”
“PRRT from my perspective, we get these quite cachectic patient that
have been losing weight slowly for a long period of time and they can
put on quite a bit of weight if they have a good [treatment] response”
Provision of nutrition
information to patients Provision of nutrition advice
Use and availability of evidence-based
guidelines
“I think in this neuroendocrine space it’s suboptimal just because it’s a really complex area”
“there’s a lack of confidence [in providing information], maybe just from experience or knowledge with seeing these patients because they are you know more complicated”
198
Theme Related topic Quotes
Patient beliefs about food
intolerances and alternative
diets
Perceived occurrence and importance of
nutritional complications among NET
patients
“I’ve had lot of GI patients who’ve had gut symptoms and they think
that food is causing the issue, but yeah it’s hard to prove”
“there’s quite a bit of perception of food avoidances because they
think it could be contributing or someone told me it could be
contributing [to symptoms] which leads to avoidance”
Impact of nutrition issues on
the quality of life of NET
patients
Perceived occurrence and importance of
nutritional complications among NET
patients
“lots of people who have the well-meaning family or friends and
they’ve got this very restrictive diet and you wonder whether their
food enjoyments gone down as a consequence and that has
implications for overall quality of life”
“I think it’s very hard to live with really restrictive diets…in all sorts of
ways that’s really difficult”
“I think that there are people who are not eating well enough
probably [and] have reduced exercise tolerance and energy levels
because they’re constantly malnourished”
Adequacy of malnutrition
screening and barriers
Malnutrition screening and management
practices
“I don’t know if it’s as high and as obvious as oesophageal or gastric
cancer patients, I wouldn’t say as high as those patients but there’s
still a risk [of malnutrition]”
“I probably feel like we do it badly…it’s more reactive”
“I’m not familiar with the screening tool and if it’s a general screening
tool it may need to be tweaked for neuroendocrine patients”
199
Theme Related topic Quotes
“probably need some evidence base in terms of what screen, what
test, how often”
Adequacy of vitamin screening
and barriers
Vitamin deficiency screening and
management practices
“if we have someone with true carcinoid syndrome, flushing and
diarrhoea for example, perhaps at time point zero all those patients
should have niacin checked and at the moment they’re not”
“If I test them and they’re deficient what do I give them that they’ll
absorb so I just feel at the moment, I feel poorly guided in terms of if I
test, what are the concequences”
I guess we would need some sort of education about looking for
symptoms from deficiencies and also looking at special diets that we
need to look at”
Provision of specialised NET
nutrition advice
Provision of nutrition advice
Use and availability of evidence-based
guidelines
“Nutrition wise with NETs I am not the most knowledgeable person [in
nutrition] so I know where my limits are and yeah I will refer on if I
think there is a reason to do so”
“[I provide] very general advice. If I think they’re the kind of patient
who needs a lot of advice on that [nutrition] then I’d refer [to the
dietitian].”
“it’s a bit of a green field because we’re so focused on the cancer
perspective rather than the nutritional aspect”
200
Symptoms are precursors of nutrition issues
Some health professional participants mentioned nutrition as of interest to patients
with NETs in general, whilst others disagreed and said patients often wouldn’t initiate
questions about nutrition during their consultations, and therefore they believed it
was less important than other aspects such as prognosis and treatment planning.
Those that spoke about nutrition being of interest to patients, explained that it was
often dependent on the symptoms a patient was experiencing. Nutrition was
considered by participants to be important in the context of treatment or symptoms,
rather than its own consideration. The symptoms described by participants to impact
on the nutrition needs of patients varied and included diarrhoea, malabsorption,
bloating, flushing, cramping, nausea, abdominal pain, loss of appetite, carcinoid
syndrome, pancreatic insufficiency, poor blood sugar control and diabetes, and weight
loss. Diarrhoea was frequently reported and discussed by participants to potentially
lead to nutrition issues such as weight loss and dietary change, as well as reduced
quality of life. The diagnosis of an insulinoma was described as relevant to nutrition.
Health professionals discussed the need for patients diagnosed with an insulinoma to
control their blood glucose through modified carbohydrate intake. Some health
professionals described observing the challenge patients face when constantly
monitoring what they eat due to fear of food-related symptoms. One participant said:
“they often will describe things that might make them worse if we question
them and ah there’s spicy foods typically and fatty foods tend to upset
[them]” – Nuclear Medicine Physician
Another said:
“I think people really get to understand the vibe of their diarrhoea and this
particular food makes it worse and this makes it better”- Medical
Oncologist
201
When discussing patient symptoms and their impact on nutrition, health professional
participants related this to the impact that symptoms can have on patient’s quality of
life. The observed impact of treatment and its side-effects on patients’ quality of life
was described by participants, specifically the medical and nursing professionals, as a
problem that often prompted patients to analyse their nutrition and dietary intake in
order to manage symptoms.
Examples of dietary changes made by patients that were observed by health
professional participants, included avoiding spicy foods, fatty foods, reducing fibre and
dairy. Focus group participants explained that patients would attempt to identify foods
that would help control their symptoms. One focus group participant said:
“we’ve all heard ‘I don’t wanna eat because it gives me diarrhoea’” –
Medical Oncologist
Another said:
“so then they don’t eat when they go out” - Dietitian
Health professional observations of patient dietary changes in response to symptoms
is discussed further below in relation to the theme - ‘Patient beliefs about food
intolerances and alternative diets’.
Sub-theme: Weight change is dependent on treatment and symptom type
When asked about the presence of weight loss among patients with NETs, participants
discussed that they believed it occurred, but did not consider it a common issue for
patients. Estimations of prevalence were provided by some participants – one said
“approximately 20%”, whilst another said “30 to 40%”. During discussion about weight
loss, participants identified certain types of NETs or treatments that they believed put
patients at increased risk of weight loss. These included those undergoing surgery
(specifically “Whipples procedure”, “major surgery”), those with high grade or
202
progressing NET, and with extensive intra-abdominal disease. The impact of Whipples
surgery on weight loss was described by one participant:
“I think the most distressing weight loss is for patients who have had a
whipples by somebody and they get a lot of weight loss around the time of
surgery and they find it difficult to get the weight back on” - Nuclear
Medicine Physician
Another described the differences in risk of weight loss between high versus low grade
NETs:
“I think the ones who have those sort of abdominal issues and the people
with high grade neuroendocrine tumours as well they have very sort of
nasty aggressive, rapidly progressive disease, they can lose a lot of weight
very quickly but for the lower grade NETs no so much unless they’ve got
those specific circumstances” – Medical Oncologist
When asked about the prevalence of weight gain, focus group participants felt that
patients who were asymptomatic or had low-grade tumours were more likely to
experience weight gain. Certain types of treatment were also mentioned to lead to
weight gain, due an improvement in symptoms and NET disease as a result of
treatment. PRRT was a treatment described as leading to weight gain if patients
experienced a good disease response. One health professional participant referred to
PRRT saying:
“I think we alter the balance of insulin and glucagon in the pancreas and so
people tend to gain weight after our treatment” – Nuclear Medicine
Physician
Another said:
203
“PRRT from my perspective, we get these quite cachectic patients that have
been losing weight slowly for a long period of time and they can put on
quite a bit of weight if they have a good [treatment] response” – Nuclear
Medicine Physician
Patients receiving SSA treatment and those with insulinoma were also mentioned by
some participants to be prone to weight gain. One focus group participant commented
on how patients feel about treatment-induced weight gain:
“some patients with effective treatments gain weight and don’t like it. They
have a good response and they put on weight”- Nuclear Medicine Physician
Provision of nutrition information to patients
During the focus groups, participants were not formally asked about how NET patients
access information related to their disease, but through analysis it became evident
that ‘getting NET and nutrition information’ was a strong theme among participants’
discussion. Participants spoke about how they observed patients having difficulty
finding information about their NET, and that information about NETs and their
treatment is hard to access. Participants said they knew patients were often searching
for information outside their treating health service, i.e. the internet, the media or
family and friends. One participant said:
“I think in this neuroendocrine space it’s suboptimal [information available]
just because it is a really complex area. There’s terminology, patients don’t
know whether they have carcinoid syndrome or not so the advice they get
may not be specific or good for them. It’s just sort of general advice. It’s
quite hard for them to tease out truths and myths” – Nuclear Medicine
Physician
204
Participants spoke about the information provided to patients by health professionals
being influenced by their experience with other patients with a NET. As a result, the
information provided by health professionals inexperienced in NETs was not always
optimal or appropriate. Some participants spoke about health professionals being
unaware of the information available to patients, and therefore do not direct patients
to it. One participant said:
“there is a lack of confidence [in providing information], maybe just from
experience and knowledge with seeing these patients because they are you
know more complicated than just some of the other tumour streams” -
Dietitian
Another participant said:
“also they’re seeing specialists outside who don’t have much exposure with
NET patients and limited exposure and therefore the information is very
poor as well. We see this all the time” – Medical Oncologist
When talking about information patients sought from internet and media sources,
participants commented that this information is not reliable and may be mis-directing
patients. One participant described this:
“the site that most links show up on the top is not necessarily the one that’s
the most truest form” – Medical Oncologist
Participants discussed the patient information booklets available from NeuroEndocrine
Cancer Australia (formerly the Unicorn Foundation Australia) as a good source of
information for patients, but were unsure how many patients were accessing these
when receiving or searching for information. Some focus group participants reported
providing the NeuroEndocrine Cancer Australia information booklets to patients during
their consultation, whereas others did not do this routinely.
205
Patient beliefs about food intolerances and alternative diets
When talking about patients seeking information, health professionals spoke about
observing patients seek information regarding their diet and how this contributed to
patient beliefs about food intolerances and diet requirements in the context of a NET.
Health professionals spoke about patients investigating food intolerances due to the
symptoms they experience, including diarrhoea, carcinoid syndrome, flushing and
bloating. Patients with small bowel NETs were also identified by health professionals as
at a higher risk of experiencing of, or believing they suffer from food intolerances. One
participant mentioned that they felt patients with NETs were looking for a “quick fix”
to symptoms and their NET disease, when searching for diet information. Whilst
participants said patients reported food intolerances, they described being unsure
whether food intolerances actually existed to the extent patients believed that they
did. One participant described this:
“I’ve had a lot of GI patients who’ve had gut symptoms and they think that
food is causing the issue, but yeah it’s hard to prove” - Dietitian
Another said:
“there’s quite a bit of perception of food avoidances because they think it
could be contributing or someone told me it could be contributing which
can lead to avoidance, whereas whether there is an intolerance is different”
– Medical Oncologist
The food intolerances reported to health professionals by patients with NETs, included
caffeine, lactose, alcohol, fatty foods, spicy foods, dairy and high fibre foods.
Participants discussed that the changes to diet and suspected food intolerances were
often patient-initiated and rarely identified or suggested by health professionals. It was
also discussed that patients often set out to seek and find their own information
206
regarding recommended dietary changes and food intolerances, rather than obtaining
advice from health professionals. One participant said:
“people [in reference to those with irritable bowel syndrome] just kind of
make it up as they go and I suspect that some of the NET patients do that
too” – Medical Oncologist
Another participant said:
“people are quite keen to read stuff and [be] quite proactive with trying to
find out whatever they can about nutrition related to their disease” -
Dietitian
Participants also spoke about how interest in information on anti-cancer diets are
common among patients with NETs and they are for cancer patients in general. In
combination with dietary change for symptom management, this led to particularly
complex diet behaviours among patients with NETs, as described by participants:
“there would be a bit of an overlap with diets that are supposed to improve
cancer …so the people who are making dietary modification because I’ve
been told that if I avoid you, all meat, all dairy, all sugar, then my cancer
will get better. So there will be an overlap with general altered diets to try
and improve outcomes for people with cancer, overlapping with what I’m
doing to try and help diarrhoea” – Medical Oncologist
When talking about dietary changes and patients seeking information on ways to
improve their cancer and NET symptoms, participants spoke about observing NET
patients seeking vitamin supplements and alternative/herbal remedies. The intent of
patients to improve their cancer outcomes with vitamins/herbal remedies was
described by one participant:
207
“some of them out of desperation because if a medical professional tells
them look we are not going to cure you, they feel they can do better” -
Endocrinologist
Another participant spoke about how vitamin and herbal remedies were considered by
patients to be a natural alternative:
“it’s considered a natural treatment as opposed to like a chemical type of
medical treatment” - Dietitian
Impact of nutrition issues on the quality of life of NET patients
When asked about the quality of life of patients, participants spoke about the negative
impact of NET symptoms, dietary change and weight loss on a patient’s quality of life.
One participant described the impact of poor diet and weight loss:
“I think that there are people who are not eating well enough probably
[and] have reduced exercise tolerance and energy levels because they’re
constantly malnourished” – Nuclear Medicine Physician
Participants spoke about and agreed that diarrhoea was a symptom that commonly
reduced quality of life among patients. One participant said:
“inability to be able to move a certain distance from a bathroom when they
get diarrhoea it’s explosive to urgent...people are essentially housebound”
– Nuclear Medicine Physician
Another said:
“there’s definitely the social implications of diarrhoea. So I’m not going out
because I could have diarrhoea, or I’m not going to go because I don’t know
where the toilets are” – Medical Oncologist
208
Participants said diarrhoea was often difficult for health professionals to manage due
to the many potential causes (pancreatic insufficiency, treatment with SSA, small
intestinal bacterial overgrowth, bile salt malabsorption). When talking about patients
suffering diarrhoea, participants also talked about dietary changes they made to help
reduce their diarrhoea and that these changes subsequently impacted further on their
quality of life. The negative impact of diet changes for symptom management was
discussed in relation to social eating and food enjoyment. Participants spoke about
how diarrhoea and other symptoms lead to restricted diets and therefore further
impact on quality of life by restricting enjoyment of food and ability to eat comfortably
with family and friends. One participant described reduced food enjoyment among
NET patients:
“lots of people who have the well-meaning family or friends and they’ve got
this very restricted diet you wonder whether their food enjoyment’s gone
down as a consequence and that has implications for overall quality of life”
- Nurse
Another said:
“I think it’s very hard to live with really restrictive diets…in all sorts of ways
that’s really difficult” - Nurse
The same health professional spoke about the importance of diet in the context of
patients living with NET disease over a prolonged period:
“We’ve got patients who are living many, many years with NETs as a
chronic condition…and we want them to be able to know and feel free to
make choices with food…so that they can eat with their families and
interact socially and have a really great range of flavours and textures with
the minimal impact on their symptoms” - Nurse
209
Nutrition issues leading to reduced quality of life discussed by participants included;
not being able to eat as expected or comfortably among family and friends, financial
expense of special diets and supplements, and the impact of reduced dietary intake on
weight loss and malnutrition leading to fatigue and less ability to perform and enjoy
daily tasks.
Adequacy of malnutrition screening and barriers
When asked about the presence of malnutrition among patients with NETs,
participants mostly spoke about and agreed that malnutrition was a greater problem
among other patients with gastrointestinal cancers (gastric cancer, oesophageal
cancer, pancreatic adenocarcinoma) than among NET patients. When comparing
presence of malnutrition in patients with NETs compared with other cancers, one
participant said:
“I haven’t seen that many, I don’t know if it’s as high and as obvious as
oesophageal or gastric cancer patients, I wouldn’t say as high as those
patients but still there’s a risk” - Surgeon
There were particular types of NET disease and treatment characteristics that focus
group participants said were likely to lead to increased weight loss and malnutrition
risk, including patients at end of life, with malabsorption issues, severe diarrhoea,
high-grade NETs, presence of mesenteric fibrosis or bowel obstruction. Participants
also discussed and agreed that malnutrition is less likely to be a problem at the time of
NET diagnosis, as patients may not have had time to develop nutritional deficiencies.
Most participants said they did not screen for malnutrition on a regular basis or in a
systematic way. They were more likely to ask about weight loss and symptoms
(fatigue, poor appetite) in general rather than perform malnutrition screening. Nurses
and doctors said they would be prompted to consider malnutrition risk in their
consultation if a patient mentioned they had symptoms or had lost weight. Dietitians
210
said they were more likely to perform a comprehensive nutrition assessment than
simple screening. When asked how they manage malnutrition screening, participants
responded:
“I probably feel like we…I do it badly” and “it’s more reactive” – Nuclear
Medicine Physician
When discussing malnutrition screening, some doctors referred to this as checking
blood levels of vitamins and nutrition markers e.g. albumin, others referred to it as
assessing for weight loss.
Most participants agreed that malnutrition screening should be part of standard care
for NET patients and completed on a more systematic basis. Some commented on the
benefit of malnutrition screening in NET patients, due to the impact that weight loss
can have on quality of life. Reported barriers to regular malnutrition screening
included time, lack of evidence and lack of clarity regarding suitable process and tools
to use. One participant commented on the use of screening tools for malnutrition
screening in NET patients, and said they may have specific requirements for a
screening tool:
“I’m not familiar with the screening tool and if it’s a general screening tool
it may need to be tweaked for neuroendocrine patients coz every screening
assumes for every likelihood that there’s a problem that in NETs that’s
probably high particularly. So just…we get some unusual things with NETs”
– Medical Oncologist
Participants spoke about the presence of weight loss and poor dietary intake among
NET patients, which would contribute to their malnutrition risk, but felt that other
issues such as vitamin deficiency and symptoms also contributed to malnutrition risk.
211
One participant commented on barriers to evidence for the best malnutrition
screening process in NETs:
“probably need some evidence base in terms of what screen, what test,
how often, what’s the outcome, what’s the gain” – Medical Oncologist
During the focus groups there was discussion among participants as to which health
professional would be best to screen for malnutrition in NET patients. Some spoke
about the value of a dietitian and that comprehensive nutrition assessment
undertaken by a dietitian would be best for some patients. It was discussed that
identifying patients in need of timely dietitian assessment should be a priority for
screening. Some participants reported referring to the dietitian immediately after a
patient reports weight loss or difficulty with eating. Others discussed that malnutrition
screening should be a simple process and therefore could be done by any member of
the multidisciplinary team.
Adequacy of vitamin screening and barriers
Health professionals described rarely screening for vitamin deficiencies in their
consultation with patients with a NET. Medical and nursing professionals reported
believing it was the dietitian’s role to monitor vitamin deficiencies, prompt testing and
provide guidance on the best approach to this. In response to this, dietitians said they
didn’t routinely consider vitamin screening when consulting with patients. Participants
discussed the types of patients with a NET that may require monitoring of vitamin
deficiency, including those who had lost weight, experienced symptoms such as
diarrhoea, and who had major changes to their diet leading to insufficient nutrient
intake. Identification of these symptoms and factors did not necessarily lead to routine
vitamin screening, as described by one participant:
“If we have someone with true carcinoid syndrome, flushing and diarrhoea
for example, perhaps at time point zero all those patients should have
212
niacin checked and at the moment they’re not” – Nuclear Medicine
Physician
Barriers to vitamin screening included time, lack of evidence for appropriate screening
practices and knowledge of the best approach to screening for vitamin deficiency. One
participant described their uncertainty regarding vitamin testing and supplementation:
“If I test them and they’re deficient what do I give them that they’ll absorb
so I just feel at the moment, I feel poorly guided in terms of if I test, what
are the consequences”- Medical Oncologist
Another participant described the need for further education to guide vitamin
screening practices:
“from a dietitian point of view, if it’s something that we’re going to start
looking at then I guess we would need some sort of education about
looking for symptoms from deficiencies and also looking at special diets
that we need to look at”- Dietitian
When asked about the practice of vitamin supplementation, health professionals
described this only being done if a vitamin deficiency was identified. Some health
professionals supplemented for vitamin D or iron, if deficiency was identified in blood
testing, and others suggested the patient’s GP was the most appropriate person to
manage vitamin supplementation, including vitamin D and B12. After discussion,
participants did not agree on who was best to initiate vitamin screening or
supplementation with patients but did agree that this issue required further
exploration and research to guide best practice.
Lack of evidence was consistently discussed as a barrier to nutrition screening
practices (both malnutrition and vitamin screening) during focus groups. Participants
described a lack of evidence specific to the nutritional management of NETs as a
213
problem impacting their clinical practice. Some participants would use general cancer
guidelines and nutrition guidelines but were unsure on where to access evidence and
clinical guidance for their practice with patients with a NET.
Provision of specialised NET nutrition advice
When asked about provision of nutrition advice to NET patients, medical and nursing
participants reported this as minimal, due to a preference of referral to the dietitian
for nutrition assessment and advice. Participants described easy access and availability
of a dietitian in their hospital, leading to dietitian referral for nutrition assessment and
management if a patient reported issues with their weight or diet. Nutrition advice
from a dietitian was considered by participants as the most reliable source of
information. One participant said:
“Nutrition wise with NETs I am not the most knowledgeable person so I
know where my limits are and yeah I will refer on if I think there is a reason
to do so” - Nurse
Another said:
“[I provide] very general advice. If I think they’re the kind of patient who
needs a lot of advice on that [nutrition] then I’d refer [to the dietitian]. I
don’t have a lot of knowledge in the area, you know medical practitioners
are taught very badly about this, and I don’t have time when you add in all
the other things that you’ve got to discuss in clinic” and “I find it very
valuable having a dietitian in clinic” – Medical Oncologist
Advice provided by dietitians participating in focus groups was comprehensive, but
was as varied as their reports of their focus on assessment and management of
nutrition in practice. Dietitian-based nutrition advice included weight management,
high protein diets, and symptom management through diet. Medical and nursing
214
participants said they provided brief general advice to patients with NETs about
keeping a healthy weight, following a healthy diet, and avoiding severe dietary
restriction. Much of the nutrition advice provided was described as being prompted by
patient symptoms. Focus group participants acknowledged that nutrition and diet play
a role in symptom management in patients with NETs. One dietitian said:
“the advice that we’re giving is symptom based. The initial thing that we’re
looking at is weight, weight changes, and signs of malnutrition” - Dietitian
Barriers to provision of nutrition advice among participants who weren’t dietitians
included time, followed by not knowing what advice to provide. One participant spoke
about how health professionals are less focused on nutrition aspects of NET disease:
“it’s a bit of a green field because we’re so focused on the cancer
perspective rather than the nutritional aspect” – Nuclear Medicine
Physician
7.5 Discussion
Focus groups conducted with multidisciplinary health professionals in Phase 2 resulted
in a thorough description of NET health professional knowledge and practices in regard
to nutritional issues and their management with patients living with a NET. Insights
from the focus groups aligned with results found in the international health
professional survey, confirming survey data and also providing further in-depth
understanding of health professional responses to, and nutrition-related practices with
regard to NETs. Initial manifest content analysis summarised health professional
practices in regard to nutrition screening and management in patients diagnosed with
a NET, and results were similar to those from the Health Professional Survey for
malnutrition screening practices, vitamin screening practices, provision of nutrition
advice, and use of evidence-based guidelines. Latent content analysis led to further in-
depth exploration of health professional experience and opinion regarding nutritional
215
issues among patients diagnosed with a NET and provided rich insights into barriers
and enablers that contribute to nutrition-related practices.
Health professional perceptions of the quality of life and experience of patients
diagnosed with a NET has not been well studied. One small study (n=17), published in
1998, compared patient and staff perceptions of quality of life and found that patient
satisfaction with their quality of life was greater than health professionals perceived it
to be (Larsson, von Essen and Sjoden, 1998). The correlation between patient and
health professional perception of key patient issues and quality of life was a positive
result in that study, potentially indicating good communication and observation of
patient issues and priorities. However, evidence to guide the translation of issue
identification to relevant interventions, for example, malnutrition screening or
investigation and advice regarding dietary change, is lacking and should be the focus
for future health professional education and nutrition guidelines.
During focus groups, health professionals described diarrhoea, abdominal pain, and
weight loss as symptoms most concerning to patients and also most likely to impact on
nutrition. These symptoms were also described by patients in the Phase 1 interviews
(Chapter 5) as impacting on their quality of life, leading to dietary change. During focus
groups, health professionals spoke about their awareness of dietary change and food
restriction made by patients with a NET in an effort to manage their symptoms and to
improve their disease outcomes. They also spoke about how these behaviours are
often initiated by patients themselves rather than in consultation with health
professionals. The issues of dietary change and self-management of dietary restriction
was also highlighted in results of the Phase 1 study and patient interviews (Chapters 4
and 5). These findings indicate that health professionals are aware of dietary change
and restriction among NET patients, however, few health professionals spoke about
how they assisted patients in managing their diet appropriately in response to a NET.
Recommendation to avoid dietary restriction was discussed as part of general advice
provided to patients, but only in brief. Investigation of the occurrence of dietary
216
change and the impact this has on patient’s nutritional status and quality of life was
not mentioned as a consideration during consultation with NET patients.
Comprehensive dietary advice and investigation of food intolerances was presumed by
health professionals to primarily be the role of the dietitian. However, results from
Phase 1 (Chapter 4) indicated that less than 22% of patients with a NET in this study,
had consultation with a dietitian over the study period, whereas up to 56% of patients
with a NET reported making a dietary change to some degree. Despite awareness of
dietary change and restrictions as an issue amongst patients, it is evident that health
professionals are not routinely addressing this or referring patients with NETs to a
dietitian for individualised dietary assessment and management. Of note, the study
site where focus groups were undertaken and where the Phase 1 study was
undertaken, is an accredited European NET Society Centre of Excellence (CoE), and
therefore health professionals have regular access to a NET-specialist dietitian.
Patients diagnosed with a NET at health centres without specialist NET dietitian
support may therefore be less likely to be referred to a dietitian, or the dietary advice
they receive may not be specific to NETs.
Dietary change, if resulting in severe dietary restriction can lead to weight loss and
deterioration of nutritional status. Weight loss and malnutrition can have negative
consequences for patient morbidity and treatment outcomes and lead to increased
health care costs (Nitenberg and Raynard, 2000; Arends et al., 2006). Patients in the
Phase 1 interviews (Chapter 5) discussed the impact that dietary change had on their
social activity, enjoyment of food and overall quality of life, highlighting the
importance of addressing dietary change among NET patients. The best approach for
identifying or screening for patient dietary change by health professionals was not
discussed during focus groups but does require further exploration and consideration.
The risk of dietary restriction among patients with a NET should be considered when
NET-specific nutrition guidelines are developed. Health professionals in this study, and
patients in the Phase 1 study (Chapter 5) identified symptoms of diarrhoea, abdominal
217
cramps, bloating and weight loss as often leading to dietary change and restriction.
Therefore, presence of these symptoms should be considered a risk factor for dietary
change, and a prompt for screening for dietary issues and risk of impaired nutritional
status.
Insights from the focus groups indicate that nutrition-related screening practices,
including screening for dietary change, malnutrition and vitamin deficiencies, are not
routine or systematic among NET health professionals. This was also shown through
results of the health professional survey described in Chapter 6. Several evidence-
based guidelines for cancer management recommend routine screening for
malnutrition for all people with cancer, and at regular intervals (Jann Arends et al.,
2017; Kiss et al., 2020). Results of this research show that these guidelines are not
being incorporated by NET health professionals. Focus groups generated discussion
among health professionals regarding the importance of malnutrition and vitamin
screening in the context of the care of a patient with a NET. Health professionals
identified the need for improved nutrition screening practices with patients and
suggested the development of a systematic process for malnutrition or vitamin
screening was warranted. Limited knowledge of the prevalence of malnutrition and
vitamin deficiencies was identified as a barrier to screening practices, as was evidence
and guidance for the best approach or method to screening. As previously discussed in
Chapter 4, common malnutrition screening tools used with cancer patients include the
Malnutrition Screening Tool (MST), Malnutrition Universal Screening Tool (MUST) and
the Nutrition Risk Screening tool (NRS-2002). These could be appropriate for use with
NET populations, but these screening tools may miss identifying nutritional issues
unique to patients with NETs, for example their unique symptom profile and dietary
restriction. Literature exists identifying malnutrition and vitamin deficiency as
prevalent issues among NET patients (Shah et al., 2005; Fiebrich et al., 2010; Bouma et
al., 2016; Maasberg et al., 2017; Borre et al., 2018). Results presented in this thesis
from Phase 1 and Phase 2 also show that malnutrition, weight loss and dietary change
are prevalent among patients with NETs.
218
Development of nutrition guidelines that summarise evidence for the prevalence of
these nutrition issues among NET patients will assist in the education of health
professionals and prompt initiation of routine nutrition-screening practices. Health
professionals in the focus groups identified the dietitian as responsible for
comprehensive nutrition assessment in NET patients but were unable to agree upon
the most appropriate health professional to perform screening, which would occur
prior to dietitian referral. This is not an issue unique to NETs, with responsibility of
nutrition screening varying within other cancer populations and in hospitalised
patients more broadly. Health professional responsibility for nutrition screening in NET
contexts can therefore be explored using existing literature which focuses on cancer
patients in general. Further qualitative research targeting health professionals on a
broader scale (multiple centres), with a focus on establishment of optimal nutrition
screening practices and responsibilities is important. This process would also
contribute to recommendations for nutrition screening practices in future NET-specific
nutrition guidelines. Groups at greater risk of weight loss and malnutrition identified
by health professionals in these focus groups, included patients undergoing major
gastrointestinal surgery, with progressive NET disease, and with extensive abdominal
disease. Patients identified by health professionals to be the least at risk of weight loss
and prone to weight gain were those undergoing PRRT treatment, with good
treatment response, and those with improving symptoms as a result of treatment.
Existing cancer guidelines recommend all cancer patients are screened for malnutrition
risk, regardless of disease or treatment status (Kiss et al., 2020), but with a focus on
high risk groups in settings with limited resources, which is important to acknowledge
in future NET guidelines. The identification of at-risk NET groups through this research,
is useful to acknowledge the factors most likely to lead to nutrition issues in patients
with a NET, which can be utilised to prioritise and target nutrition resources when
required in practice.
A recurring theme among focus groups participant responses was ‘Provision of
nutrition information to patients’ which was identified by health professionals as
problematic for patients diagnosed with a NET. Health professionals acknowledged
219
that patients were often left to access nutrition information from the internet, family
or other NET patients through blogs or peer groups. They also discussed that health
professionals were themselves often unaware of available, reputable sources of
nutrition information, partially due to the rare nature of a NET diagnosis and the belief
that there was limited nutrition evidence available to support practice. This was
considered a greater issue among health professionals who had limited experience in
managing NETs. These results align with results of the Phase 1 patient interviews,
during which patients discussed the same issue with accessing NET-specific
information on nutrition and therefore confirms the priority of this as a target for
health professional and patient education. Difficulty in accessing NET-specific
information has also been identified in a large published survey of NET patients and
NET health professionals to be a considerable unmet need (Leyden et al., 2020).
Collation and development of NET-specific nutrition information resources would be
beneficial to address this issue, and revision or development of future nutrition
guidelines for NETs could be one way of addressing this gap.
Health professionals identified the role of a dietitian as important in the context of a
NET patients care and treatment, and that nutrition assessment and advice was best
provided by a dietitian who can focus on the individual needs of each patient. This
suggests that a dietitian has an integral role within the multidisciplinary team working
in a NET unit. Participants reported that a specialist NET dietitian was readily available
to receive referrals for patients with NETs within the NET unit of the study site, which
as discussed above was an ENETS CoE. A dietitian in some health centres managing
patients with NETs may not be readily available and given that NETs are rare in
incidence the availability of a dietitian with specialty knowledge and experience in
managing NETs, is likely to be limited to only certain health centres. As health
professionals in this study, and patients in Phase 1, identified expertise in NET
management as important to ensuring patients are managed appropriately and have
access evidence-based information, access to a dietitian with NET expertise would also
be ideal. However, if this is not possible, access to a dietitian with experience in
managing cancer patients during treatment would be appropriate helpful. Promoting
220
the occurrence and importance of nutrition issues in patients diagnosed with a NET
among practicing dietitians, and through professional groups such as the Dietitians
Association of Australia and international dietetic associations, would assist to raise
awareness of nutrition in this rare cancer group. These professional groups can also
provide useful avenues to disseminate appropriate patient education resources and
professional development opportunities specific to NETs, otherwise difficult to access
by dietitians who do not routinely care for patients diagnosed with a NET.
7.6 Conclusion
This qualitative study of multidisciplinary health professionals working with NET
patients, enabled a comprehensive exploration of their knowledge of nutritional
complications among patients and nutrition screening and management practices.
Health professionals perceived symptom burden, inadequate provision of NET-specific
nutrition information, and dietary restriction as key issues impacting patient quality of
life and nutrition, which correlates with results of patient interviews discussed in
Chapter 5. Focus groups identified inconsistencies in nutrition-related practices,
including limited conduct of malnutrition and vitamin screening, and varied provision
of nutrition information. A multidisciplinary approach to management of patients with
NETs was identified as important, as was the role of a dietitian in providing optimal
nutrition assessment and intervention. Health professionals identified barriers to their
NET-related nutrition knowledge and practices as limited evidence or knowledge of
available evidence, and lack of NET-specific nutrition guidelines. Study results provide
additional depth and contextual detail above what was obtained in the health
professional survey discussed in Chapter 6 and will contribute to development of
further NET nutrition research and NET-specific nutrition guidelines, which currently
do not exist. Particular NET types and treatments at greater risk of causing
malnutrition and dietary restriction were identified by health professionals in this
study. Factors leading to deteriorating nutritional status included surgery and presence
of a progressive NET. Factors leading to improvement in nutritional status included
PRRT, treatment response and improving symptoms. These factors are useful
221
considerations for future interventional nutrition research in NETs, and the
development of NET-specific nutrition guidelines. Current cancer guidelines
recommend all cancer patients undergo routine malnutrition screening regardless of
their disease or clinical state, which is not currently occurring with NET patients, as
found through this research. Further research and consultation with NET health
professionals is required to establish robust nutrition screening practices. The high
prevalence of dietary change and food restriction observed in patients should be
considered when establishing suitable nutrition screening processes and tools for use
in a NET population, particularly given the negative impact that dietary restriction can
have on a patient’s quality of life.
223
Chapter 8: Conclusions and implications for research and
practice
8.1 Summary of research findings
The studies presented in this thesis have explored the prevalence of nutritional
complications and their HRQoL impacts among a heterogeneous cohort of GEP NET
patients (Phase 1 research). In parallel they have explored health professional
knowledge and usual management of nutritional complications in GEP NET patients
(Phase 2 research). Results of the Phase 1 study have provided the first comprehensive
longitudinal description of the prevalence of nutritional complications; including
malnutrition, weight change, body composition change (fat-free mass), and dietary
modification; and how this relates to patient’s HRQoL and experience of nutritional
complications. Results of the Phase 2 study have provided the first detailed summary
of NET health professional knowledge and practices in regard to the nutritional
complications in NET patients and has contributed important insights about barriers
and enablers to the nutritional management of these patients. This chapter
summarises the main findings of these studies, the strength and limitations of this
research, and presents a discussion of the implications for clinical practice and
directions for future research.
8.1.1 Quality of life and symptoms in GEP NET patients
Chapter 3 described results for symptoms and quality of life scores among participants
enrolled in the Phase 1 longitudinal embedded mixed methods study. Symptoms were
prevalent among patients with GEP NETs enrolled in the Phase 1 study. The
commonest symptoms at time of recruitment included, in order of prevalence; fatigue
Appendix 2 – Table 2: Comparison of baseline (T0) HRQoL scale and item scores between study data and baseline scores from previously published data of general Australian population and NET populations, values are mean and standard deviation
Gen Pop NET Pop NET Pop NET Pop NET pop
Scale/item
Baseline score (T0)
N = 59
Mercieca-Bebber et al. 2019
N = 1821
Larsson et al. 2001
N = 24
Frojd et al.
2007
N = 59
Strosberg et al. 2018
N = 231
Cella et al. 2018
N = 135
EORTC QLQ-C30
Global health status 63 (22) 69 (22) 68 (23) 58 (19) 67 (22) 55 (19)
Disease-related worries 56 (28) - - - 44 (28) a 40 (27) a
Muscle/bone pain 30 (32) - - - 29 (31) 33 (31)
Sexual function 34 (37) - - - 31 (39) 43 (39)
Information/communication function
15 (27) - - - 5 (14) a 6 (17)
Body image 30 (41) - - - 20 (32) a 31 (36)
Notes.
aDifference in mean score of 10 or greater in comparison to general Australian population, considered clinically significant between-group difference (Cocks et al., 2012)
Larsson study, median 62yo, mid-gut NETs, 75% metastatic, 83% carcinoid syndrome, interferon or SSA treatment (Larsson et al., 2001)
Frojd study, mean 60yo, confirmed carcinoid tumor (NET), 41% SSA treatment, 44% no treatment, all inpatients (Fröjd et al., 2007)
Strosberg study, mean 63-64yo, mid-gut NETs, 100% previous SSA (Strosberg et al., 2018)
Cella study, mean 64yo, 100% metastatic NETs, 100% carcinoid syndrome (Cella et al., 2018)
273
Appendix 3: Complete results for symptom impact on dietary change
Appendix 3 - Table 1 Symptoms reported by participants to impact on dietary change
T0 T2 T4 T6
n N n N n N n N
Loss of appetite 14 15 11 14 9 10 11 15
Nausea 11 13 10 17 5 11 6 9
Vomiting 7 9 5 8 0 4 1 3
Discomfort in abdomen 19 25 13 21 9 14 10 17
Bloating 16 24 12 16 8 13 11 14
Diarrhoea 15 23 10 17 8 15 9 13
Wind or gas 14 24 9 19 7 17 9 15
Pain 14 26 7 19 7 11 6 15
Constipation 7 14 5 10 1 6 4 9
Weight loss 10 21 8 15 6 14 8 11
Feeling tired/less energy 12 18 10 22 9 18 10 18
Indigestion or heartburn 7 19 4 8 2 8 3 11
Weight gain 4 11 3 8 3 6 8 12
Short of breath 5 14 3 12 2 7 1 10
Night sweating 4 16 1 10 1 8 1 9
Feeling flushed or flushing 3 17 3 12 3 7 1 11
Notes.
N = total number of participants reporting to experience that symptom at each time-point
n = total number of participants with the symptom reporting it impacted their diet
275
Appendix 4: Phase 1 patient interview schedule
Phase 1: Patient interviews
Overall research aim:
To describe the experience of people living with gastroenteropancreatic
neuroendocrine tumours, with particular focus on dietary intake, nutritional status and
the prevalence and severity of nutrition-related symptoms.
Focus:
Does a diagnosis and treatment of NET impact QOL?
Do nutrition needs change after a diagnosis of NET?
What extent of intervention has been received from clinicians regarding nutrition?
Baseline Interview
Potential questions:
1. Can you please tell me how things have been for you since you were first
diagnosed with a NET?
2. Had you been unwell or some time before your diagnosis – if so what
symptoms did you have?
3. Have you had any challenging or unexpected things to deal with since your
diagnosis?
4. Had you heard of a NET before you were diagnosed? Where/how did you get
information about the condition? Was it hard to get information?
Emotional health questions:
5. How are you coping/did you cope with your diagnosis?
6. How have you found support/information since your diagnosis?
276
Nutrition questions:
7. Have you noticed any issues with your eating since diagnosis?
8. Have you noticed any issues with your weight since diagnosis?
9. Have changes to your eating or weight impacted on your day to day life? If yes,
in what way?
10. Have you been offered any advice about managing your nutrition, eating or
weight?
If yes, can you please describe the advice you received? Who provided this
advice?
a. Prompt: Would you change the nutrition care you received?
b. Prompt: Has any of the advice been particularly helpful? If so, what?
11. Is there any information about nutrition that you have learnt since your
diagnosis that would have been helpful to know early on? If yes, what?
If they received treatment at another centre prior to referral to Peter Mac/ONJ
Centre:
12. Do you have any symptoms or side-effects from treatment you received prior
to attending Peter Mac/Olivia Newton John Cancer Centre that have affected
your eating or weight?
Six-month Interview
Potential questions:
1. Can you please tell me how you have been managing since you first attended
Peter Mac/Olivia Newton John Cancer Centre?
2. Have you felt unwell over the past few months - if so can you describe how?
What symptoms have you had?
3. Have you had any challenging or unexpected things to deal with since you
started receiving care or treatment at Peter Mac/Olivia Newton John Cancer
Centre?
277
Emotional health questions:
4. How have you been coping with your diagnosis?
5. How have you found support/information since your diagnosis? Is there any
other support or information you wish you had received?
Nutrition questions:
Begin with ‘Since you last interview six-months ago’ or ‘Since you started receiving care
at Peter Mac/Olivia Newton John Cancer Centre’
6. Have you noticed any issues with your eating?
7. Have you noticed any issues with your weight?
8. Do you have any symptoms or side-effects from treatment that have affected
your eating or weight?
9. Have changes to your eating or weight impacted on your day to day life? If yes,
in what way?
10. Have you been offered any advice about managing your nutrition, eating or
weight?
If yes, can you please describe the advice you received? Who provided this
advice?
a. Prompt: Would you change the nutrition care you received?
b. Prompt: Has any of the advice been particularly helpful? If so, what?
11. Is there any information about nutrition that you have learnt since your
diagnosis that would have been helpful to know early on? If yes, what?
279
Appendix 5: Health professional focus group question schedule
Phase 2b: Health professional focus groups
Demographic questionnaire (to be completed prior to focus group)
Please complete the following two questions prior to participation in the focus group:
1. What is your area of specialty (tick)?
☐ Medical oncology
☐ Surgical oncology
☐ Radiation oncology
☐ Nuclear medicine
☐ Gastroenterology
☐ Endocrinology
☐ Other physician (please specify________________)
☐ Nursing (please specify___________________)
☐ Dietitian
☐ Other allied health (please specify_______________________)
2. Please provide an estimate of the number of NET patients that you have contact with or manage each year (tick)?
☐ < 10 per year
☐ 10 – 25 per year
☐ 26 – 50 per year
☐ 51 - 100 per year
☐ > 100 per year
Phase 2b: Focus and questions for discussion during focus group
Overall research aim:
To describe health professional perceptions of nutrition issues amongst patients with NET and summarise current nutrition and management practices.
280
Focus:
Is nutrition considered important within the overall context of a NET patients management/treatment?
What similarities or differences are there amongst health professionals in regards to the screening and management of malnutrition in NET patients?
What similarities of differences are there amongst health professionals in regards to the management of nutrition issues overall (including vitamin deficiencies, change in diet, food intolerances)?
Potential questions:
1. In your experience, what issues are most important to a person newly diagnosed with a NET?
Prompts:
a. What kinds of things to people commonly ask you about or seem most concerned about for example, the disease itself or treatments available to them or prognosis?
2. Do NET patients usually ask you about nutrition issues? Can you describe this in more detail?
Prompts:
a. In regards to nutrition what do NET patients report to be most concerning?
b. What is the most common question you get asked relating to nutrition? c. Do NET patients talk to you about any particular symptoms that impact
on their eating or weight? d. Do you believe nutrition issues (weight loss, change in diet) affect the
quality of life of NET patients? If so, in what way? e. When do nutrition concerns usually arise? At diagnosis, during
treatment, post treatment?
3. In your experience, is malnutrition a concerning problem amongst NET patients? Can you describe why? (Note: describe definition of malnutrition as 5% unintentional weight loss over 3 months, or 10% unintentional weight loss over 6 months)
Prompts:
a. How common is weight loss amongst NET patients? Why? b. How common is weight gain amongst NET patients? Why? c. How common is malnutrition amongst NET patients? Why?
281
d. How common are food intolerances amongst NET patients? Why? e. Do you find that NET patients change their diet due to their NET disease
or treatment? Can you provide some examples?
4. Do you screen for malnutrition when you consult with NET patients? If yes, describe how?
a. Do you believe screening for malnutrition should be a part of standard care for NET patients? If so, by Who? Why?
5. Do you screen for vitamin deficiencies when you consult with NET patients? If you do, describe which ones and why?
a. Do you believe screening for vitamin deficiencies should be a part of standard care for NET patients? If so, by who? Why?
6. Do you routinely give advice about managing nutrition, eating or weight management to NET patients? If so, what kind of advice to you give?
7. Do you believe that there is adequate evidence to inform best practice for management of nutritional issues for patients with NETs?
8. Can you identify any area of research that if prioritised, could make a helpful contribution to the nutritional care of patients with NETs?
283
Glossary
Term Abbreviation Definition
Bioelectrical impedance analysis BIA Method for estimating body
fat and muscle mass, when a
weak electric current flows
through the body to
calculate resistance
(impedance)
Body mass index BMI Calculated by dividing a
person’s weight (kg) by their
height (m2)
Carcinoid syndrome Cluster of symptoms caused
by a neuroendocrine tumour,
usually located in either the
gut or lung, that secretes
hormones
Gastrinoma Tumour located in the
pancreas or duodenum that
produces excessive levels of
the hormone gastrin
Gastroenteropancreatic
neuroendocrine tumour
GEP NET Neurendocrine tumour of
the gastrointestinal tract or
pancreas
Global Leadership Initiative on
Malnutrition
GLIM
284
Glucagonoma Tumour located in the
pancreas that produces
excessive levels of the
hormone glucagon
Fat free mass FFM Encompasses components of
body tissue including internal
organs, muscle, water and
connective tissue
Flushing Symptom of NET
characterised by redness of
the face
Functional tumour A tumour (e.g. NET) that
produces excessive
hormones, often leading to
symptoms
Inflammatory bowel disease IBD Condition causing
inflammation of the digestive
system, including ulcerative
colitis and Chron’s disease
Irritable bowel syndrome IBS Symptoms or condition often
characterised by a
combination of abdominal
pain, bloating, and
alternating constipation and
diarrhoea
285
Insulinoma Tumour located in the
pancreas that produces
excessive levels of insulin
Malnutrition Refers to imbalance (excess
or deficiency) in a person’s
intake of energy and/or
nutrients, associated with
adverse functional and
clinical outcomes
Malnutrition Universal Screening
Tool
MUST Type of malnutrition risk
screening tool
Malnutrition Screening Tool MST Type of malnutrition risk