Evidence-Based Commentary I. INTRODUCTION Adverse drug reactions cause major health problems in the United States. There are about 106,000 fatalities due to adverse drug reactions in the United States per year. 1 The overall incidence of serious adverse drug reactions of hospital patients is 6.7% (95% CI, 5.2% to 8.2%). Approximately 25% of both serious and non-serious adverse drug reactions are caused by idiosyncra- sy/intolerance, pseudoallergic and/or al- lergic adverse drug reactions. Drug idio- syncratic and/or intolerant reactions, as defined in the glossary, are non-im- mune, unpredictable occurrences. Such reactions occur in only a small percent- age of patients and precise mecha- nisms have not been established. Ad- verse drug reactions constitute either the fourth or the sixth leading cause of death in the United States depending on whether one uses the lower (76,000 patients) or the upper (137,000 pa- tients) confidence limit. Physicians should become fully ac- quainted with the proper ways of recog- nizing and preventing such reactions. Further, since 51% of all approved drugs have serious adverse effects not detected prior to approval by the FDA, there have been an increasing number of appeals for more comprehensive monitoring of mar- keted drugs. 2,3 II. DEFINITIONS Drug allergy/hypersensitivity reactions are immunologically mediated re- sponses to pharmacologic agents and pharmaceutical excipients. Such reac- tions may occur after exposure to a wide variety of chemicals (oral, paren- teral, or topical), biologics (derived from natural or recombinant technol- ogy sources) and “inert substances” (excipients) used in the formulation of active drug products. These reactions must be distinguished from pseudoallergic or anaphylactoid re- actions induced by substances such as radiocontrast media, colloid volume ex- panders, basic polypeptides, opiates, ASA/NSAIDS and “inert” excipients. Pseudoallergic or anaphylactoid reac- tions are caused by direct release of me- diators from mast cells and basophils, resulting in the classic end-organ effects that these mediators exert. 4 Direct medi- ator release occurs without evidence of a prior sensitization period, specific IgE antibodies or antigen-antibody bridging on mast cells/basophil cell membranes. This non-immune reaction is immediate, often severe and therefore referred to as anaphylactoid. Because it is not immu- nologic, it may occur the first time that the host is exposed to a particular agent. Some drugs induce both allergic and pseudoallergic reactions. An example of this type of drug is vancomycin which may elicit the pseudoallergic “red man syndrome” as well as true IgE-mediated anaphylaxis. Anaphylactoid reactions have also been reported after the first treatment with quinolones. Drug idiosyncrasy/intolerance re- sponses may mimic immunologically mediated drug reactions. Three major classes of drugs have been shown to induce such reactions: aspirin (ASA), non-steroidal anti-inflammatory drugs (NSAIDs), angiotensin converting en- zyme (ACE) inhibitors, as well as sev- eral preservatives. As cited above, some immediate cardiorespiratory re- actions to ASAs and NSAIDs occur within minutes and strongly resemble anaphylactoid reactions. III. CLASSIFICATION OF IMMUNOLOGICALLY MEDIATED DRUG HYPERSENSITIVITY REACTIONS Clinical presentations of drug allergy are often diverse, depending on type(s) of immune responses and target organ specificity(ies). If immunopathogen- esis is mixed, some drug reactions may be difficult to classify by criteria pre- viously established for naturally occur- ring human hypersensitivity. On the other hand, the characteristics and mechanisms of many allergic drug re- actions are consistent with the chief categories of human hypersensitivity defined by the Gell-Coombs classifica- tion of human hypersensitivity [imme- diate hypersensitivity (Type 1), cyto- toxic (Type 2), immune complex (Type 3), and cell mediated (Type 4)]. 5 Immediate hypersensitivity Type 1 reactions are IgE mediated and result in immediate reactions such as anaphy- laxis. These are exemplified by symp- toms of urticaria, laryngeal edema, wheezing, and cardiorespiratory col- lapse. Common causes are large mo- lecular mass biologicals and many drugs (eg, penicillin). Cytotoxic reac- tions are induced by complement-me- diated cytotoxic IgM or IgG antibodies which are formed in response to drug altered cell surface membranes. Clas- sic examples of this phenomenon are acquired hemolytic anemia induced by methyldopa and penicillin or throm- bocytopenia caused by quinidine. Type 3 reactions are mediated by immune complexes formed in slight antigen ex- cess. The chief manifestations of these reactions include fever, rash, urticaria, lymphadenopathy and arthralgias, which typically appear 1 to 3 weeks after the last dose of an offending drug and subside when the drug and/or its metabolites are completely eliminated from the body. Drugs that are likely to cause these reactions include penicil- lin, sulfonamides, thiouracil, and phe- nytoin. Delayed hypersensitivity Type 4 reactions are mediated by cellular immune mechanisms which include CD4cells, CD8cells, or both. Re- actions in this category include contact dermatitis, a condition in which the topical induction and elicitation of sen- sitization by a drug is entirely limited to the skin. Delayed hypersensitivity responses may also be systemic, in- volving lymphoid organs and other tis- sues throughout the body. Sensitized T-cells produce a wide array of pro- VOLUME 83, DECEMBER, 1999 677
Transcript
Evidence-Based Commentary
I. INTRODUCTIONAdverse drug reactions cause majorhealth problems in the United States.There are about 106,000 fatalities dueto adverse drug reactions in the UnitedStates per year.1 The overall incidenceof serious adverse drug reactions ofhospital patients is 6.7% (95% CI,5.2% to 8.2%). Approximately 25% ofboth serious and non-serious adversedrug reactions are caused by idiosyncra-sy/intolerance, pseudoallergic and/or al-lergic adverse drug reactions. Drug idio-syncratic and/or intolerant reactions, asdefined in the glossary, are non-im-mune, unpredictable occurrences. Suchreactions occur in only a small percent-age of patients and precise mecha-nisms have not been established. Ad-verse drug reactions constitute eitherthe fourth or the sixth leading cause ofdeath in the United States dependingon whether one uses the lower (76,000patients) or the upper (137,000 pa-tients) confidence limit.Physicians should become fully ac-
quainted with the proper ways of recog-nizing and preventing such reactions.Further, since 51% of all approved drugshave serious adverse effects not detectedprior to approval by the FDA, there havebeen an increasing number of appeals formore comprehensive monitoring of mar-keted drugs.2,3
II. DEFINITIONSDrug allergy/hypersensitivity reactionsare immunologically mediated re-sponses to pharmacologic agents andpharmaceutical excipients. Such reac-tions may occur after exposure to awide variety of chemicals (oral, paren-teral, or topical), biologics (derivedfrom natural or recombinant technol-ogy sources) and “inert substances”(excipients) used in the formulation ofactive drug products.These reactions must be distinguished
from pseudoallergic or anaphylactoid re-actions induced by substances such asradiocontrast media, colloid volume ex-
panders, basic polypeptides, opiates,ASA/NSAIDS and “inert” excipients.Pseudoallergic or anaphylactoid reac-tions are caused by direct release of me-diators from mast cells and basophils,resulting in the classic end-organ effectsthat these mediators exert.4 Direct medi-ator release occurs without evidence of aprior sensitization period, specific IgEantibodies or antigen-antibody bridgingon mast cells/basophil cell membranes.This non-immune reaction is immediate,often severe and therefore referred to asanaphylactoid. Because it is not immu-nologic, it may occur the first time thatthe host is exposed to a particular agent.Some drugs induce both allergic andpseudoallergic reactions. An example ofthis type of drug is vancomycin whichmay elicit the pseudoallergic “red mansyndrome” as well as true IgE-mediatedanaphylaxis. Anaphylactoid reactionshave also been reported after the firsttreatment with quinolones.Drug idiosyncrasy/intolerance re-
sponses may mimic immunologicallymediated drug reactions. Three majorclasses of drugs have been shown toinduce such reactions: aspirin (ASA),non-steroidal anti-inflammatory drugs(NSAIDs), angiotensin converting en-zyme (ACE) inhibitors, as well as sev-eral preservatives. As cited above,some immediate cardiorespiratory re-actions to ASAs and NSAIDs occurwithin minutes and strongly resembleanaphylactoid reactions.
III. CLASSIFICATION OFIMMUNOLOGICALLYMEDIATED DRUGHYPERSENSITIVITYREACTIONS
Clinical presentations of drug allergyare often diverse, depending on type(s)of immune responses and target organspecificity(ies). If immunopathogen-esis is mixed, some drug reactions maybe difficult to classify by criteria pre-viously established for naturally occur-ring human hypersensitivity. On the
other hand, the characteristics andmechanisms of many allergic drug re-actions are consistent with the chiefcategories of human hypersensitivitydefined by the Gell-Coombs classifica-tion of human hypersensitivity [imme-diate hypersensitivity (Type 1), cyto-toxic (Type 2), immune complex(Type 3), and cell mediated (Type 4)].5Immediate hypersensitivity Type 1
reactions are IgE mediated and resultin immediate reactions such as anaphy-laxis. These are exemplified by symp-toms of urticaria, laryngeal edema,wheezing, and cardiorespiratory col-lapse. Common causes are large mo-lecular mass biologicals and manydrugs (eg, penicillin). Cytotoxic reac-tions are induced by complement-me-diated cytotoxic IgM or IgG antibodieswhich are formed in response to drugaltered cell surface membranes. Clas-sic examples of this phenomenon areacquired hemolytic anemia induced by� methyldopa and penicillin or throm-bocytopenia caused by quinidine. Type3 reactions are mediated by immunecomplexes formed in slight antigen ex-cess. The chief manifestations of thesereactions include fever, rash, urticaria,lymphadenopathy and arthralgias,which typically appear 1 to 3 weeksafter the last dose of an offending drugand subside when the drug and/or itsmetabolites are completely eliminatedfrom the body. Drugs that are likely tocause these reactions include penicil-lin, sulfonamides, thiouracil, and phe-nytoin. Delayed hypersensitivity Type4 reactions are mediated by cellularimmune mechanisms which includeCD4� cells, CD8� cells, or both. Re-actions in this category include contactdermatitis, a condition in which thetopical induction and elicitation of sen-sitization by a drug is entirely limitedto the skin. Delayed hypersensitivityresponses may also be systemic, in-volving lymphoid organs and other tis-sues throughout the body. SensitizedT-cells produce a wide array of pro-
VOLUME 83, DECEMBER, 1999 677
inflammatory cytokines that ultimatelylead to lymphocytic infiltrates, dissem-inated granulomata, and fibrosis. It hasbeen suggested that there is a markedclinicopathologic similarity betweensome late onset drug reactions andgraft versus host reactions which areinitiated and maintained by T cells.6In addition to the Gell and Coombs
human hypersensitivity classification,there are a number of drug reactionsassociated with specific T cell activa-tion, for which immunopathogenesishas not been fully established. Theseinclude maculopapular rashes, erythro-derma, eczematous rashes, exfoliativedermatitis, drug fever, and fixed drugreactions. The latter are caused by suchdrugs as barbiturates and sulfon-amides. The term “fixed” is applied tothis lesion because reexposure to thedrug usually produces recurrence ofthe lesion at the original site. The pres-ence of CD8� T lymphocytes has beendemonstrated in the peripheral bloodand involved skin of patients withdrug-induced delayed cutaneous hy-persensitivity reactions characterizedby morbilliform and bullous exan-thematous lesions.7 Allergen-specificT cell clones from some of these pa-tients displayed a TH 1-like cytokinepattern, as contrasted to CD4� positiveT cell clones from patients with peni-cillin-induced urticarial exanthemata,which demonstrated a TH2-like cyto-kine pattern.7From the clinical standpoint, the
most practical method of classifyingdrug reactions is by predilection forvarious tissue and organ systems. Cu-taneous drug reactivity represents themost common form of restricted tissueresponsiveness to drugs.8 The pulmo-nary system is also recognized as afavorite site for certain drug hypersen-sitivity reactions. Other individual tis-sue responses to drugs include cyto-toxic effects upon blood componentsand hypersensitivity sequelae in liver,kidneys, and blood vessels. Somedrugs, however, induce heterogeneousimmune responses and tissue manifes-tations. Thus, sensitization to penicillinor its degradation products may even-tuate in anaphylaxis, morbilliform
rashes, serum sickness, drug fever, cy-totoxic effects (eg, hemolytic anemia),hypersensitivity vasculitis, interstitialnephritis, or severe contact dermatitisif applied topically. Finally, the tem-poral relationship to onset of symp-toms after administration of a specificdrug may constitute another type ofclassification, ranging from immediate(minutes to an hour), accelerated (1 to3 days) or delayed beyond 3 days.9To some extent, the structural char-
acteristics of drugs and biologicalproducts permit predictions about whattype of hypersensitivity reactions toexpect from certain classes of thera-peutic substances.6 Allergic reactionsto peptides and proteins are most oftenmediated by either IgE antibodies orimmune complex responses. Such re-actions may also be mixed. In specificsituations, the process may culminatein a multisystem, vasculitic disease ofsmall and medium sized blood vessels.Although immune responses inducedby carbohydrate agents are infrequent,anaphylaxis has been described aftertopical exposure to carboxymethycel-lulose.10 Contact dermatitis is the typ-ical immune response observed aftertopical exposure to a number of fattyvehicles and essential oils in therapeu-tic products (lanolin, clove oil, cam-phor oil, and beeswax).11-13 Any singleor mixed variety of immune responsesmay occur after exposure to low mo-lecular mass (�1,000 daltons) inor-ganic or organic medicinal chemicals.The immunogenic potential of suchdrugs is often determined by one ormore reactive end products or metab-olites which haptenate with variousbody proteins. Often, the parent com-pound itself is not immunogenic be-cause it lacks the ability to conjugatewith proteins in a stable covalent link-age. Metabolism of drugs by cyto-chrome oxidase pathways may occurin the liver, skin, and phagocytic cells.In addition, patients with certain ge-netic polymorphisms are at higher riskfor allergic and autoimmune disordersinduced by drugs. Thus the risks ofprocainamide-induced lupus erythem-atosus and severe mucocutaneous dis-eases after sulfonamide treatment are
higher in patients having the slow-acetylator phenotype.6,14 As a generalrule, increases in molecular mass andstructural complexity are often associ-ated with increased immunogenicity,at least as far as humoral mediatedhypersensitivity is concerned. On theother hand, some proteins (eg, latex)also may induce contact urticariaand/or contact dermatitis in addition toanaphylaxis.
IV. RISK FACTORSThe chemical properties, amount/dura-tion of exposure to the drug and hostfactors may all interact in the develop-ment of drug allergy. Large molecularmass agents such as proteins and somepolysaccharides may be immunogenicand therefore are much more likely toinduce antibody-mediated drug hyper-sensitivity reactions, especially inatopic individuals. On the other hand,specific structural moieties in non-pro-tein medicinal chemicals are often crit-ical determinants in inducing drug hy-persensitivity. How these particularstructures (eg, beta lactam rings ofpenicillins and cepholosporins) are de-graded is of crucial importance. Pro-longed drug and metabolite(s) clear-ance may occur because of geneticpolymorphisms of metabolic enzymepathways (eg, hydralazine, azathio-prine).15,16 Specific chemical structureis responsible for cross-sensitivitywhich may be based either on commoncore elements (eg, beta lactam rings)or side chains. In some cases, sidechain specificity alone may determinedrug hypersensitivity.17–19Parenteral and topical administra-
tions of a drug enhance the possibilityof sensitization while the oral route ofadministration may be safer.20 Topicalapplication of a medicinal chemicalmay induce contact dermatitis. Singledoses of a prophylactic antibiotic aremuch less likely to sensitize comparedwith high dose prolonged parenteraladministration of the same drug. In thecase of penicillin, the latter type of ex-posure may cause an immune-mediatedhemolytic anemia or interstitial nephri-tis.9,21 Frequent repetitive courses oftherapy are also more likely to sensitize.
678 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
Host factors and concurrent medicalillnesses are significant risk factors.Drug reactions appear to occur lessfrequently in infants and in the elderly.Immaturity of the immunologic appa-ratus is given as an explanation for theformer, and involution of the immuno-logic apparatus may account for thelatter.22 In the prospective study byBigby et al women were shown to havea 35% higher incidence of adverse cu-taneous reactions to drugs than men.23In one study, the odds ratio for womendeveloping reactions to RCM was 20-fold greater than for men.24 Allergicreactions to multiple, structurally unre-lated antibiotics tend to occur moreoften in women.25 One recent survey ofpossible familial drug allergy reportedthat children of parents who are aller-gic to at least one antibiotic may havea 15-fold greater risk for subsequentreactions to antibiotics than childrenwithout such histories.26 A genetic re-lationship to histocompatibility anti-genic determinants (HLA-DR3) existsin patients with rheumatoid arthritiswho are treated with gold or penicilla-mine and subsequently develop drug-induced nephropathy.27 Patients withsystemic lupus erythematous appear tohave an increased prevalence of drugreactions although it is not clear thatthis predilection is causally related tothe underlying immunologic abnor-malities or the fact that such patientsare exposed more often to drugs. Thepresence of an atopic diathesis (aller-gic rhinitis, allergic asthma, and/oratopic dermatitis) predisposes to ahigher rate of allergic reactions to pro-teins (eg, chymopapain) but not to lowmolecular agents.28–30 Paradoxically,atopic patients appear to have a greaterrisk of non-IgE-mediated, pseudoaller-gic reactions induced by RCM.31Atopy appears to be associated with asubstantially increased risk of seriousallergic reactions (including anaphy-laxis) once an IgE antibody response toany drug has developed.20,32 Therefore,an atopic background increases the riskthat an immediate hypersensitivity re-action may be severe, but it does notincrease the probability that an IgE-mediated antibody response will de-
velop in response to small molecularmass drugs.
V. CLINICAL EVALUATIONAND DIAGNOSIS OF DRUGHYPERSENSITIVITY
The first question facing the physicianin the evaluation of a patient with asuspected adverse drug reaction iswhether the clinical problem is drug-related. The subsequent clinical evalu-ation and diagnosis of drug hypersen-sitivity reactions is based upon anumber of clinical criteria:(1) The symptoms and physical find-
ings are compatible with an im-mune drug reaction;
(2) There is (or was) a definite tempo-ral relationship between adminis-tration of the drug and an adverseevent;
(3) The class and chemical structureof the drug have been associatedwith immune reactions;
(4) The patient previously receivedthe drug on one or more occasions(with the possible exception of ac-celerated serum-sickness-like re-actions);
(5) There is no other clear cause forthe presenting manifestations in apatient who is receiving medica-tions known to cause hypersensi-tivity reactions; and
(6) Skin tests and/or laboratory find-ings (if available) are compatiblewith drug hypersensitivity.
Currently, for most drugs, these ques-tions are answered on the basis of in-formation derived solely from a clini-cally derived data base.
A. HistoryA careful history of previous and cur-rent drug usage, focusing particularlyon the temporal sequence of eventsbetween initiation of therapy and onsetof symptoms is probably the most use-ful factor in the diagnosis of an allergicdrug reaction. In this regard, specificknowledge about the toxicology andallergenicity of the involved drugs of-ten is valuable in trying to delineate thecausal factor. This is particularly im-portant when a patient is receivingmultiple drugs. As previously dis-
cussed, general and specific host riskfactors should also be noted in themedical history.
B. Physical ExaminationSince drug reactions may involve vir-tually any organ system, a carefulphysical examination is recommended.Cutaneous lesions should be describedaccurately with regard to gross appear-ance and distribution. A distinction be-tween maculopapular skin eruptionsand urticaria is very important sincethe latter is more likely to be mediatedby specific IgE antibodies. The pres-ence of purpura and petechiae are oftencutaneous stigmata of vasculitis.33 Un-usual maculopapular lesions of thesides of the fingers and toes or a ser-piginous distribution of such lesionsalong lateral aspects of both soles maysuggest serum sickness.34 Erythemamultiforme minor is a polymorphousmaculopapular lesion that spreads pe-ripherally and clears centrally to forman annular pattern known as a “target”lesion. This consists of three zones: anerythematous central papule that mayblister, an edematous middle ring, andan erythematous outer ring. In an ex-aggerated form, these lesions may de-velop blisters and progressively in-volve mucous membranes.35 Althoughthis symptom complex is termed ery-thema multiforme major and is oftenused synonymously with the Stevens-Johnson syndrome, some cliniciansspecify that the two conditions havedistinguishing features. Target lesions,particularly on the extremities, are stillpresent in erythema multiforme majorwhile widespread blistering purpuricmacules of the face, trunk, and proxi-mal extremities are characteristic ofthe Stevens-Johnson syndrome.33 Atthis stage, more than one mucosal siteis involved and there are progressiveconstitutional symptoms. The clinicalpresentation of Stevens-Johnson syn-drome may evolve into toxic epidermalnecrolysis, a severe drug-induced skindisease in which apoptotic, epidermalcell death results in the separation oflarge areas of skin at the dermo-epider-mal junction, producing the appear-ance of scalded skin.33 Fixed drug
VOLUME 83, DECEMBER, 1999 679
eruptions are pleomorphic, rangingfrom sharply defined erythematouspapules or pigmented areas to edema-tous, bullous, papulovesicular, or urticar-ial lesions. Contact dermatitis is a papu-lovesicular, scaly lesion which appearsat cutaneous sites previously exposed totopical medications. Photoallergic der-matitis often has a similar appearance tocontact dermatitis. Exfoliative dermatitisis a severe, end stage dermatosis thatusually progresses from other types oflate onset cutaneous drug reactions andconsists of large confluent areas of shed-ding scaly epidermis. The entire skin isscaly and erythematous; chills and feverare common. Erythema nodosum lesionsof the extensor surfaces of the extremi-ties may also be associated with cell-mediated responses induced by drugs.Acute life-threatening drug reac-
tions can involve the upper and lowerrespiratory tracts and the cardiovascu-lar system. Vital signs are profoundlyaffected in the course of anaphylaxisand in some cases expiratory wheezingmay be heard (for more detailed dis-cussion of signs and symptoms of ana-phylaxis, see “Practice Parameters onDiagnosis and Treatment of Anaphy-laxis” J Allergy Clin Immunol 1998;101:S482). Drug reactions may presentas an isolated fever, occasionally inexcess of 104°F.36 They may cause awide array of physical abnormalitiesincluding mucous membrane lesions,lymphadenopathy, hepatosplenomeg-aly, pleuropneumonopathic abnormal-ities, and joint tenderness/swelling.
C. General Clinical TestsWhen pulmonary and cardiovascularmanifestations appear days or weeksafter the initiation of the drug, a chestx-ray and electrocardiogram should beobtained. If liver or kidney involve-ment is suspected, liver function testsand a renal profile should be obtained.Other laboratory tests may be indicatedfor late hypersensitivity drug reactions.These include a complete blood countwith a differential cell count and a totalplatelet count to exclude the possibilityof cytotoxic reactions. Eosinophiliamay be observed as an accompanimentof drug fever, immune complex syn-
dromes, eosinophilic pneumonias andthe Churg-Strauss Syndrome. A urinal-ysis should be checked for the pres-ence of proteinuria, casts, and eosino-phils. Proteinuria and/or casts maydenote nephropathy induced by im-mune complex disease or other formsof drug-induced vasculitides. The pres-ence of urine eosinophils combinedwith an increase in total IgE is diag-nostic of interstitial nephritis.21 Otheruseful tests might include a sedimen-tation rate (or C-reactive protein), totalcomplement or complement compo-nents, and several autoantibody tests[antinuclear antibody (ANA), antinu-clear cytoplasmic antibody (c-ANCA)and peri-antinuclear cytoplasmic anti-body (p-ANCA)]. A positive ANAmay point to the diagnosis of the drug-induced lupus syndrome induced bydrugs such as procainamide and hy-dralazine.37 Abnormalities in c-ANCAor p-ANCA frequently occur in drug-induced systemic vasculitides and theChurg-Strauss Syndrome.38 A retro-spective diagnosis of anaphylaxis maybe made by a rise in serum �-tryptase,which peaks at 1 to 2 hours and re-mains elevated in the serum for 2 to 4hours (or more) after the reaction,39 ora 24-hour urine for histamine and/orN-methylhistamine.40 In serum sick-ness-like reactions, several nonspecifictechniques may at times be helpful incertain situations. The most commonscreening test for detection of immunecomplexes is a test for cryoglobulins orcold precipitable serum protein. C1qbinding and Raji cell assays are alsoavailable for detection of immunecomplexes but these are rarely neces-sary in the routine evaluation of drug-induced serum sickness-like reactions.Positive tests are helpful but negativetests do not exclude the possibility ofimmune complex disease.
D. Specific TestsTwo criteria are used to demonstratethe immunologic basis of an adversedrug reaction: (1) detection of an im-mune response to the drug or its me-tabolite(s); and (2) demonstration thatthe immune response is causally re-lated to the immunopathologic se-
quelae in an affected individual. Al-though an immune response to a drugis an essential component of all immu-nologic drug reactions, it does notprove that the patient’s symptoms aredue to a drug allergy. The second cri-terion concerning the drug’s immuno-pathologic role in the reaction is moredifficult to document. In the case ofimmediate hypersensitivity reactionsmediated by IgE antibodies, demon-stration of the presence of drug-spe-cific IgE is usually taken as sufficientevidence that the individual is at sig-nificant risk of anaphylaxis or otherimmediate signs if the drug is admin-istered. This is helpful in the case ofhigh molecular weight agents and afew small molecular mass agents suchas penicillin.41,42 However, insufficientknowledge about drug degradationproducts and/or metabolites and howthey are conjugated with body proteinshas been an impediment to developingeither skin or in vitro assays for mostsmall molecular weight drug chemi-cals. The presence of other isotypicantibody classes or cell-mediated im-munity often is poorly correlated withimmunopathologic mechanisms sincemany individuals receiving drugs maydemonstrate drug-specific immune re-sponses but do not react adversely tothe drug, even if challenged. Thus, theutility of specific immunologic tests(apart from IgE-mediated syndromes)is limited in most instances of drughypersensitivity. At best, such testsprovide adjunctive support for the clin-ical diagnosis.Assessment of drug-specific IgE an-
tibodies induced by many large molec-ular weight and several small molecu-lar weight agents is often highly usefulfor confirming the diagnosis and pre-diction of future IgE-mediated reac-tions, such as anaphylaxis and urticar-ia.6,28,41 Immediate type skin tests areusually the most sensitive diagnostictests but in certain cases where skintesting is not possible (ie, a negativehistamine control test, dermatogra-phism or generalized eczema), specificIgE in vitro assays (eg, RAST, ELISA,EAST, CAP) are available but some
680 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
are not adequately standardized. In thecase of small molecular weight drugs,validated and reliable skin test reagentsare only available for penicillin. Theyhave excellent negative predictivevalue in predicting severe reactions topenicillin. Immunoassays for penicil-lin-specific IgE antibodies are less sen-sitive than skin tests and therefore skintesting is preferred. More detailed in-formation about the methods, reliabil-ity, and predictive capability of skintest reagents for the diagnosis of im-mediate drug allergic reactions may befound in “Practice Parameters for theDiagnosis and Management of Ana-phylaxis” (J Allergy Clin Immunol1998;101:S483–S484). It should beemphasized that neither immediateskin nor in vitro tests for IgE antibod-ies are diagnostic of cytotoxic, im-mune complex or cell-mediated drug-induced allergic reactions.Both direct and indirect Coombs’
tests are often positive in drug-inducedhemolytic anemia. This may reflect thepresence of complement and/or peni-cillin on the red cell membrane, or anRh determinant autoantibody (eg, asoccurs with �-methyldopa).43 Sensitivedrug-specific assays for IgG and IgMantibodies have been developed. Al-though these may be useful as diagnos-tic adjuncts, it is important to note thatelevated levels can occur in individualswho receive the drug and do not expe-rience a clinical reaction. Comple-ment-dependent assays to detect drug-specific cytotoxic antibodies have alsobeen reported. By and large, however,these tests are only available in spe-cific research laboratories and there-fore are not clinically applicable formost drugs.The diagnosis of contact dermatitis
usually can be verified by patch test-ing. The details of this technique arediscussed in greater detail in “PracticeParameters for Allergy DiagnosticTests” (Ann Allergy Asthma Immunol1995;75:570–571). In recent yearsthere have been many reports concern-ing the diagnostic utility of patch testsin non-IgE mediated cutaneous drugreactions.44 A positive reaction may beuseful by identifying a specific drug in
a patient receiving multiple drugs,provided that it is properly comparedwith a group of negative controls. Thelymphocyte proliferation test has beenstudied extensively as an in vitro cor-relate of drug-induced cellular reac-tions. This is used primarily as a ret-rospective test and is not clinicallyavailable in most medical centers.There is considerable disagreementamong investigators about the value ofthis assay in evaluating drug allergiesbecause neither its positive nor nega-tive predictive values have been sys-tematically investigated. One potentialadvantage of the test for some patientsis that it is possible to obtain in vitroevidence of lymphocyte transforma-tion by the parent drug itself as well asliver microsomal products of the drug,thereby bypassing the need for preciseknowledge of metabolic determi-nants.45 Although the general clinicalapplicability of these tests has not beenvalidated in any large scale study, anumber of investigators have shownthat drugs may induce both CD4� andCD8� T-cell responses as well asdrug-specific TH-1 and/or TH-2 re-sponses.46,47 For example, certain con-tact sensitizers are more likely to in-duce TH-1 T-cell responses while avariety of systemically administereddrugs may preferentially induce TH-2responses.48
E. Tissue DiagnosisOccasionally biopsies of involved or-gans may define specific histopatho-logic lesions. Skin biopsies are usefulin differentiating vasculitis, vasculopa-thy, bullous diseases, and contact der-matitis.33 However, they are not help-ful in implicating a particular drug. Aliver biopsy helps to differentiate be-tween cholestatic and hepatocellulardrug reactions but does not identify thespecific cause. Membranous glomeru-lonephritis initiated by deposition ofimmune complexes in the kidney canbe readily identified by immunofluo-rescent stains for IgG, IgM, and com-plement in renal biopsy specimens.49Drugs such as methicillin and sulfon-amides are clearly incriminated incases of interstitial nephritis.21 Fluores-
cent antibody studies of renal biopsiesin such cases reveal that these drugsbind to tubular basement membranesand may induce an immune responseto bound antigen or the modified base-ment membrane protein.
VI. MANAGEMENT ANDPREVENTION OF DRUGHYPERSENSITIVITYREACTIONS
The management of drug allergy be-gins with the suspicion that any unex-plained rash, fever, lymphadenopathy,pulmonary, renal, gastrointestinal orother systemic disturbance may repre-sent drug hypersensitivity. For mild re-actions, a simple withdrawal of thedrug may be all that is required fortreatment. Acute anaphylactic reac-tions require the prompt administrationof epinephrine; the patency of the air-way should be insured and oxygenshould be administered as indicated;and an intravenous cannula should beplaced to facilitate administration offluids, pressor agents, antihistamines,and glucocorticosteroids (see “Param-eter for Diagnosis and Management ofAnaphylaxis” J Allergy Clin Immunol1998;101:S483–S484). Immune com-plex reactions usually resolve sponta-neously once the antigen is cleared;however, symptomatic therapy withantihistamines and possibly non-steroi-dal inflammatory drugs (NSAIDS)may be indicated for control of urticar-ia50,51 and joint symptoms, respec-tively. In cases complicated by moresevere symptoms, refractory urticariaor vasculitis, treatment with glucocor-ticosteroids is indicated. Glucocortico-steroids may also be required for thetreatment of drug-induced hemolytic,thrombocytopenic or granulocytic cy-topenias, especially in situations wherethe responsible drug must be continuedas a life saving measure.52Allergic drug reactions or a history
of such reactions are occasionally en-countered in other clinical situationswhere continued use of the drug isimperative. Among the most importantconditions where drug use may be jus-tified are diabetic ketoacidosis, bacte-rial endocarditis, inflammatory bowel
VOLUME 83, DECEMBER, 1999 681
disease, neurosyphilis, AIDS, and pul-monary tuberculosis. When no alterna-tive drug is available for therapy, therisk of continued administration of theoffending drug may be less than therisk to life posed by the underlyingdisease. Where there is a definite med-ical indication for the agent in ques-tion, either desensitization or gradedchallenge procedures may be consid-ered, depending on the history of theprevious reaction. The use of suppres-sive drugs is optional. These protocolsrequire the supervision of an allergy/immunologist having previous experi-ence with these procedures (see “Prac-tice Parameters for the Diagnosis andManagement of Anaphylaxis” J Al-lergy Clin Immunol 1998;101:S465–S528).Specific desensitization is the rapid
progressive administration of an aller-genic substance to render effector cellsless reactive. Such procedures varywith individual drugs and they are suc-cessful chiefly with agents that induceIgE-mediated reactions. For example,in the case of penicillin, the initial de-sensitization dose is usually 100 to1000 times lower than the concentra-tion of the drug which produced a pos-itive skin test. Oral desensitizationmay be less likely to induce anaphy-laxis than parenteral administration.53Further dosage increases are given at15 to 30-minute intervals until thera-peutic levels are achieved. In mostcases this can be accomplished within4 to 5 hours. This regimen should bereserved for hospitalized patients, re-quiring that experienced personnel andresuscitation equipment be available atall times. Desensitization programs areavailable for a variety of drugs includ-ing penicillin, a number of non-betalactam antibiotics and insulin. Even ifformal protocols do not exist, desensi-tization can be attempted with otheragents.A graded challenge regimen (see
glossary for definition) may be at-tempted to confer clinical tolerance todrugs associated with a variety of non-IgE hypersensitivity reactions.
The principle of a graded challenge isbased on the administration of smalldoses of the drug with incremental pro-gression at regular intervals until atherapeutic dose is achieved.54 Themost common drugs in this categoryare para-aminosalicylic acid, isoniazid,TMP-SMX, pentamidine, dapsone, al-lopurinol, sulfasalazine, diphenylhy-dantoin, and penicillamine. A 6-hourgraded challenge to TMP-SMX inHIV-infected patients has proven to besuccessful without major long termcomplications.55 Graded challengewith aspirin (ASA) or NSAIDS is alsopossible in patients who are intolerantto these drugs, particularly for thosewith respiratory reactions.56 Initialdoses are higher than desensitization(mg versus �g) and the interval be-tween dose increments are variable,ranging from hours, days, or weeks.Modified, more cautious regimens arebased on the fact that slower readmin-istration may be more likely to revealsystemic intolerance, which can berecognized early enough to preventprogression to life-threatening ery-thema multiforme major/Stevens-Johnson syndrome and/or the toxicepidermal necrolysis syndrome in-duced by some of these drugs. Futureuse of drugs which cause these syn-dromes as well as other life-threaten-ing conditions (eg, Churg-Strauss syn-drome and exfoliative dermatitis) isabsolutely contraindicated.Slow graded challenge of a drug in
increasing amounts over days or weeksmay be required for inducing toleranceto drugs causing non-IgE-mediated skinrashes. This technique may offer anotherapproach to a previously unsuccessfulrapid graded challenge regimen (eg,hours to days for drugs such as tri-methoprim-sulfamethoxazole, sulfasala-zine, and allopurinol).57Cautious use of some agents inducing
pseudoallergic reactions (eg, radiocon-trast dyes) is often possible by pretreat-ment of patients with glucocorticoste-roids, H1 (with or without H2)antihistamines and/or albuterol/ephed-rine (see “Practice Parameters On Diag-nosis and Management of Anaphylaxis”
J Allergy Clin Immunol 1998;101:S503–S504).Prevention of allergic drug reactions
is more desirable than treatment of re-actions once they occur. The majorityof serious allergic drug reactions canbe prevented or at least attenuated byalert management. Patients should bequestioned directly concerning previ-ous drug reactions and medical recordsshould be reviewed for previous nota-tions of drug allergy. Cross-reactivitybetween chemically related drugsshould be anticipated. Drugs known toproduce adverse reactions frequently(eg, antibiotics) should be prescribedonly for valid indications and combi-nations of drugs should be used spar-ingly. Orally administered drugs areless likely to produce reactions thandrugs given by the topical or parenteralroute. If injectable drugs are adminis-tered, epinephrine and other emer-gency measures for treatment of acuteanaphylaxis should be available. Med-ic-Alert tags and bracelets represent auseful way of alerting physicians to aprevious severe allergic reaction, al-though it should be kept in mind thathistorical diagnoses of drug allergy of-ten are erroneous or tenuous.Skin tests may be predictive of risk
in certain instances, especially withpenicillin, heterologous sera, and insu-lin.9,14 The frequency with which het-erologous sera are prescribed for hu-mans has declined, resulting in adecrease in the number of anaphylacticor serum sickness reactions to theseagents. Further, homologous sera arenow available for passive immuniza-tion against tetanus, hepatitis B, andrabies.A few states now require that the
names and concentrations of all medi-cations appear on prescription labels.This is a useful advance which helps toassure that the patient is being edu-cated about prescribed medications. Inaddition, the routine establishment ofindividual patient drug profiles bysome hospitals and commercial phar-macies facilitates identification of po-tential allergic reactions.
682 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
VII. PROTOTYPES OFIMMUNOLOGICALLYMEDIATED DRUGHYPERSENSITIVITY
Almost any drug is capable of inducingan allergic reaction and the likelihoodthat this will occur increases in directproportion to the usage pattern of adrug in the general population. Drugsdiffer, however, with their propensitiesto induce either restricted or heteroge-neous immune responses within theGell-Coombs spectrum of human hy-persensitivity. This section will discussseveral of the most common clinicalentities of drug hypersensitivity, someas representative examples of each ofthe four major Gell-Coombs’ catego-ries of human hypersensitivity and oth-ers with heterogeneous and often un-classifiable immune characteristics.
A. IgE-Mediated Reactions (Gell-Coombs Type 1)
IgE-mediated hypersensitivity reac-tions may occur after administration ofa wide variety of drugs, biologicals,and drug formulation agents. The mostimportant drug causes of immediatehypersensitivity reactions are antibiot-ics. Other common drugs that causesuch reactions are insulin, enzymes(streptokinase and chymopapain), het-erologous antisera (equine antitoxinsand, antilymphocyte globulin), murinemonoclonal antibodies, protamine, andheparin.58–64 Detailed discussionsabout these agents may be found in the“Practice Parameters for the Diagnosisand Management of Anaphylaxis” JAllergy Clin Immunol 1998;101:S505–S515). Allergic Type 1 reactionsalso have been reported after exposureto excipients such as eugenol, carmine,vegetable gums, paraben, thiomerosal,sodium metabisulfite, formaldehyde,and sulfonechloramide.13 In the fol-lowing discussion, we will considerboth beta lactam and non-beta lactamantibiotics as the major prototypes inthis category.1. Beta lactam antibioticsAnaphylactic reactions manifested byurticaria, flushing, pruritus, laryngealedema, and cardiovascular collapse
may occur within minutes or, less fre-quently, hours after administration ofbeta lactam antibiotics (ie, drugs thathave a common beta lactam ring struc-ture). Drugs in this category includepenicillin, semi-synthetic penicillins(eg, amoxicillin), cephalosporins, car-bapenems (eg, imipenem), monobac-tams (eg, aztreonam), and carbe-cephems. In addition, non-IgEmediated immunologic reactions mayalso be caused by this class of drugs.These include: cytopenias, immunecomplex disease such as serum sick-ness, vasculitis, glomerulonephritis,fever, and non-urticarial rashes.Penicillin. The prevalence of peni-
cillin hypersensitivity in the generalpopulation is not known. Up to 10% ofhospitalized patients have been re-ported to give a history of allergy topenicillin and, for this reason, many ofthese patients receive alternative anti-microbial drugs.65 The frequency ofanaphylaxis is estimated to be 0.01%to 0.05% with each course of penicil-lin.32 The nature of the past reactioncorrelates somewhat with the chanceof being allergic to penicillin but his-tory alone is not sufficiently reliable tomake a diagnosis of penicillin hyper-sensitivity. Thus, over 80% of patientswith a past history of penicillin hyper-sensitivity do not have penicillin-spe-cific IgE antibodies detected by skintesting.66 Although many patients withdocumented hypersensitivity to peni-cillin lose sensitivity with time, about20% may maintain their hypersensitiv-ity status for long periods of time. Upto 46% of patients with a history ofanaphylaxis and about 15% of thosewith a history of urticaria and angio-edema will exhibit positive immediatehypersensitivity skin tests to penicillinwhen tested at a later date.67 The mostreliable method for evaluating IgE-me-diated penicillin allergy is by skin test-ing to both major and minor determi-nants of penicillin. Positive commercialin vitro tests (RAST or ELISA) maysuggest a diagnosis of penicillin allergy.Negative commercial tests, however, arenot reliable for excluding penicillin hy-persensitivity because they are relativelyinsensitive and do not test for minor de-
terminants.68 Although skin testing pre-dicts only the risk of developing an IgE-mediated reaction, this information is ofcritical clinical importance because mostlife threatening reactions to penicillin arethe result of IgE-mediated anaphylaxis.If possible, it is preferable to treat a
patient with a history of penicillin al-lergy with a non-beta lactam antibioticthat is equally efficacious. Many alter-nate antibiotics, however, may be lesseffective, more expensive, or associ-ated with more side effects than peni-cillin. If there is no effective alterna-tive, an allergist/immunologist shouldbe consulted to determine whether thepatient is allergic to penicillin. Ideally,skin tests should be performed imme-diately prior to planned administrationof penicillin. In penicillin history-pos-itive patients, testing is safe providedthe recommended skin test procedureis followed.42,67,69–71 Penicillin skintesting is not predictive of: (1) IgG orIgM-mediated immune complex dis-ease (eg, serum sickness, glomerulone-phritis, or vasculitis); (2) hemolyticanemia; (3) erythema multiforme mi-nor, erythema multiforme major/Stevens-Johnson syndrome; or (4)toxic epidermal necrolysis. There is noway to adequately predict these non-IgE immune reactions and therefore,patients with a history of these reac-tions should never receive penicillinagain. It appears safe to skin test andrechallenge patients with a history ofisolated drug fever.36,42 Skin testingshould be postponed in anyone cur-rently receiving antihistamines or anti-histamine-like drugs until the respec-tive drug is discontinued and thehistamine wheal and flare responses isre-established.A negative skin test to both major
and minor determinants performedwithin days of a planned therapeuticcourse of penicillin means that a pa-tient may receive penicillin withoutsignificant risk of an IgE-mediated re-action. Although there has been concernthat skin test reagents might stimulatespecific IgE production, resensitizationas a result of skin tests to both major andminor determinants of penicillin has notbeen demonstrated. A negative penicillin
VOLUME 83, DECEMBER, 1999 683
skin test could possibly later convert topositive if the patient has a hidden expo-sure to penicillin between the time of thenegative skin test and later administra-tion of the drug. While this conversioncould occur, especially among medicalpersonnel exposed to penicillin, it ap-pears to be a rare event.Because of the frequent outpatient
need for penicillin treatment in the pe-diatric population and the impractical-ity of testing children when sick, test-ing them when they are well and not inimmediate need of penicillin may beconsidered.70 Although it is preferableto perform skin testing when there isan immediate need for penicillin, theremay be some situations where skintesting of history positive adults not inimmediate need of treatment may alsobe indicated. These include: (1) pa-tients with a history of mitral valveprolapse or other disorders, which re-quire amoxicillin prophylaxis beforedental work, and who are unable to takeerythromycin, azithromycin, or other ap-propriate antibiotics; (2) cancer chemo-therapy-induced neutropenia in patientswho might require penicillin promptlyfor infections that appear suddenly; or(3) patients with a recent possible IgE-mediated penicillin reaction in order toconfirm the cause.A positive skin test identifies pa-
tients who have penicillin-specific IgEantibodies and may be at risk of animmediate life-threatening reaction ifgiven penicillin. This reaction includeshypotension, urticaria, laryngeal an-gioedema, flushing, or pruritus andmay occur within minutes or hours af-ter administration. Skin testing doesnot predict the development of IgE-mediated reactions which may begin24 hours or more after penicillin ad-ministration or reactions due to other“mixed” immune mechanisms (ie,IgM, IgG, or T cell-mediated reac-tions). If skin testing to the major andminor determinants of penicillin isnegative, 97% to 99% of patients (de-pending on reagents used) will toleratepenicillin administration at the time oftesting without risk of an immediatereaction.42 Therefore, the negative pre-dictive value is very high.42 A mixture
of minor determinants is not commer-cially available. If penicilloyl polyly-sine (major determinant) and penicillinG are used for skin testing, 97% ofpatients with a negative skin test willtolerate penicillin.71 Another combinedprospective/retrospective study re-vealed that 99% of these patients tol-erated penicillin.72 Nevertheless, sensi-tivity to one of the minor determinantslacking in penicillin G may not be de-tected if this reagent is used for skintesting. In this regard, 7% to 17% ofskin test positive patients have demon-strated reactivity to a minor determi-nant other than penicillin G.66 Thismay not be clinically important be-cause reaction rates were low in a largenumber of challenged penicillin G skintest negative patients.71,72 If a patienthas both a positive history and a posi-tive skin test for penicillin allergy,there is a 50% or greater chance of animmediate reaction if penicillin isgiven. The precise positive predictivevalue has not been determined becauseof the risk associated with deliberatechallenge in skin test positive patients.In the case of a positive history, skin
test-negative patient who tolerates atherapeutic course of penicillin, thepredictive value of the skin tests forfuture therapeutic courses of penicillinis unknown.67,68 The resensitizationrate appears to be higher in adults thanchildren.73 In the situation where theoriginal history was consistent with asevere IgE-mediated anaphylactic re-action, the patient tolerated a course ofpenicillin and the drug has to be read-ministered, it has been suggested thatretesting should be considered or thepatient could undergo a test dose chal-lenge.74 For history-positive skin testnegative patients who tolerate twocourses of penicillin therapy withoutreaction, the likelihood that a conver-sion to a skin test positive state is ex-tremely low and it is not necessary toperform skin testing or graded chal-lenge prior to additional courses oftherapy.Penicillin skin testing is best per-
formed by personnel skilled in per-forming and in interpreting immediatehypersensitivity skin tests to drugs.
The techniques, controls, and interpre-tation are also discussed in “PracticeParameters of Allergy DiagnosticTests” Ann Allergy Asthma Immunol1995;75:586). Skin testing should bedone with (1) benzyl penicilloyl, the ma-jor determinant of penicillin, commer-cially available as PrePen and (2) peni-cillin G diluted to 10,000 units/mL or amixture of minor determinants (MDM;not commercially available) which usu-ally includes a 10�2 M mixture of benzylpenicilloate, benzyl penilloate, and ben-zyl-n-propylamine.75–77 Benzyl penicil-loyl (PrePen) can be used directly fromcommercial vials. Penicillin G is stablefor 1 week refrigerated at a concentra-tion of 100,000 units/mL and for 6months, if frozen. Diluted skin test re-agents should be used within 24 hours.78If full strength prick tests (Pre-Pen 6 �10�5 M, MDM 10�2 M or penicillin G10,000 �/mL) are negative, full strengthintracutaneous tests may be placed.Some practitioners feel that more cau-tious titration with 10-fold to 100-folddilutions of prick and/or intracutaneoustests should be employed.42,79,80 Whealsizes �3 mm and erythema greater thanthe negative control are considered pos-itive for both prick and intracutaneoustests.Using these reagents and proper
technique, serious reactions from pen-icillin skin testing are extremely rare.Anaphylactic reactions and deathsfrom penicillin skin testing have beenreported but all were due to adminis-tration of higher doses initially or in-tracutaneous testing not preceded byprick/puncture testing. Use of penicil-lin skin test reagents does not appear toresensitize the patient. If a systemicreaction to a skin test occurs, patientson concurrent beta-adrenergic block-ing agents or angiotensin convertingenzyme inhibitors at the time of skintesting may not respond to emergencytreatment with epinephrine. For moredetailed information about this issue,refer to “Practice Parameters on Diag-nosis and Management of Anaphy-laxis” J Allergy Clin Immunol 1998;191:S484).If skin testing is positive to any pen-
icillin reagent, the patient should re-
684 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
ceive an alternate antibiotic, unlesspenicillin is essential. In that case, thepatient should undergo desensitization.If the skin test is negative, the patientmay receive penicillin. An oral sub-therapeutic test dose may be given be-fore the full recommended dose. Ifpenicillin G is used as a substitute forthe MDM reagent, there is a small riskthat IgE antibodies to minor determi-nants not present in the penicillin Gmay not have been detected. For theseskin test-negative patients, a test doseof approximately 1⁄100th of the desiredtherapeutic dose of penicillin should beadministered first. If no reaction oc-curs (eg, within 60 minutes), the fulldose may be given safely in mostcases. If such a patient experiences asignificant reaction within 1 hour ofexposure, a formal desensitization pro-tocol may be considered.Ampicillin and amoxicillin. Ad-
ministration of ampicillin and amoxi-cillin is associated with the develop-ment of a maculopapular rash in 5% to10% of patients.81 These patients arenot at risk of a life threatening reactionto penicillin. Most patients will toler-ate future administration of penicillinother than ampicillin and amoxicillinwithout reactions of any kind. If ampi-cillin or amoxicillin is administeredagain, the patient could redevelop arash, but rarely a non-dermatologic re-action. Re-administration of ampicillinor amoxicillin may be better toleratedby children than by adults. If patientswith Epstein-Barr infections are givenampicillin or amoxicillin, almost 100%will develop a non-pruritic rash.82 Theincidence of non-pruritic, cutaneousreactions also may be increased in pa-tients who have an elevated uric acid,are being treated with allopurinol, orhave chronic lymphocytic leuke-mia.83,84 If the rash to ampicillin oramoxicillin is other than maculopapu-lar and non-pruritic in nature (eg, urti-carial), the patient should undergo pen-icillin skin testing before a futurecourse of penicillin is given. If penicil-lin skin testing is negative, the patientshould be approached as outlined inthe prior discussion about penicillin. Ifpenicillin skin testing is positive, the
patient should be given an alternativeantibiotic or undergo desensitization topenicillin.Cross-reactivity between carba-
penems, monobactams, ampicillin andpenicillin. Carbapenem (eg, imipenem)should be considered cross-reactive withpenicillins.85 The monobactam aztreo-nam does not appear to cross-react86,87with penicillins but anecdotal episodesof anaphylaxis have been reported.88There are instances where antibodiesspecific for penicillin side chains mayexist in the absence of beta lactam-spe-cific antibodies.89–91 Patients in this cat-egory probably include those with posi-tive skin tests to ampicillin but negativeto penicillin. Not all these patients havebeen prospectively challenged so theclinical significance of these side chain-specific antibodies is as yet unclear.Cephalosporin allergy (see cepha-
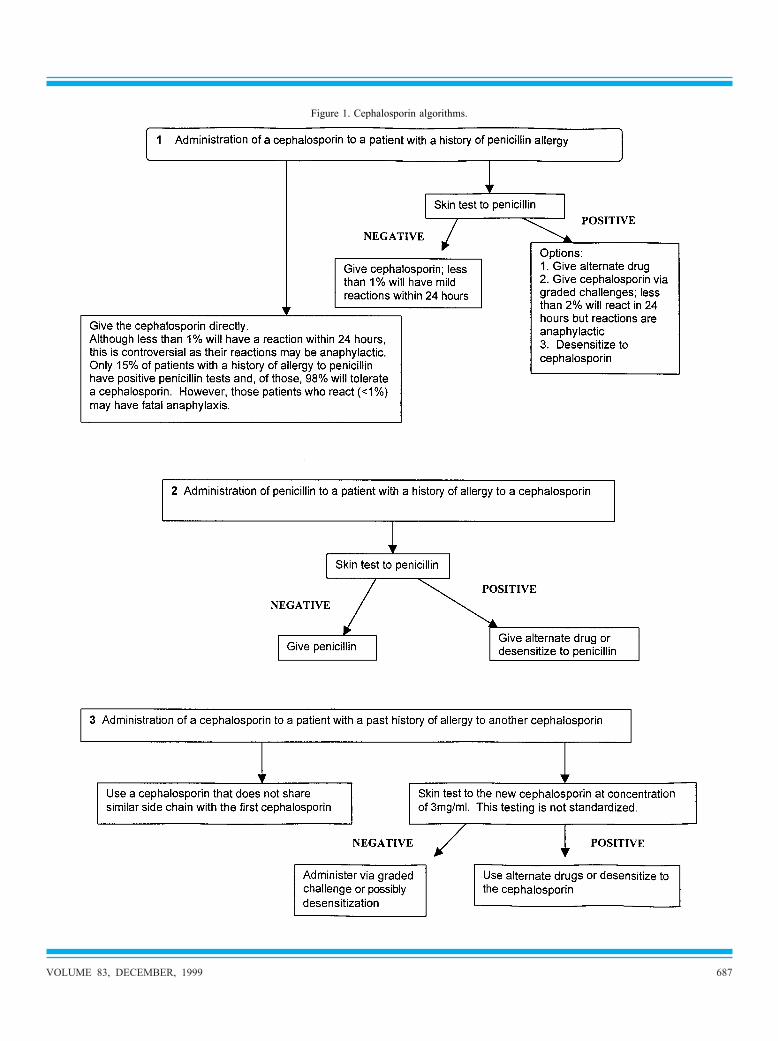
losporin algorithms p 687). Cephalo-sporins and penicillins have a commonbeta-lactam ring structure and moder-ate cross-reactivity has been docu-mented in vitro. Although clinicallysignificant cross-reactivity betweenpenicillin and the cephalosporins is in-frequent, anaphylactic reactions afteradministration of cephalosporin haveoccurred in patients with a positivehistory of penicillin anaphylaxis.92Most of the in vitro cross-reactionsbetween penicillins and cephalosporinshave involved first and second gener-ation cephalosporins.93,94 While IgEantibodies to the beta lactam ring ofpenicillin are of major importance,some reactions to cephalosporins maynot be directed to the beta lactam ringand may be side chain specific.89,93Skin testing with a cephalosporin is notnecessary if the patient has a history ofallergy to penicillin, but has tolerated acephalosporin safely since the originalpenicillin reaction.66 Allergy to cepha-losporins is uncommon compared withpenicillin allergy. If a patient with apast history of allergy to one cephalo-sporin agent requires another cepha-losporin, the following can be consid-ered: (1) after insuring that the newcephalosporin does not share sidechain determinants with the originalone, perform a graded challenge with
the new one; or (2) cephalosporin skintesting can be done although such skintesting is not standardized and the neg-ative predictive value is unknown. Thecephalosporin currently requiredshould be used as the skin test reagent.Concentrations of 3 mg/mL of a par-enteral preparation are usually non-ir-ritating but each cephalosporin re-quires concurrent evaluation for itsirritation potential in non-allergic pa-tients. Skin testing should be done asdescribed in the penicillin section witha prick/puncture test at 3 mg/mL con-centration followed by an intracutane-ous test (if the prick-test reaction isnegative in 10 to 15 minutes). If theprevious clinical reaction was docu-mented as anaphylactic and life-threat-ening, testing should start at 0.3mg/mL or lower. A positive cephalo-sporin skin test implies the presence ofdrug-specific IgE antibodies and thepatient should receive an alternate drugor undergo desensitization. Although anegative skin test at an intracutaneousconcentration of 3 mg/mL may implythat the patient does not have detect-able drug-specific IgE antibodies, itdoes not ensure that drug-specific an-tibodies are absent. IgE antibodies tocephalosporin degraded products notused in the testing may be present butnot detectable. Since the negative pre-dictive value of cephalosporin skintesting is unknown, a cautious gradedchallenge should be done (eg, 1⁄100 ofthe therapeutic dose, increasing tenfoldevery 30 to 60 minutes up to the fulltherapeutic dose). However, if the pre-vious history was consistent with anIgE-mediated reaction, desensitizationshould be undertaken.Administration of cephalosporin
to patients with a history of allergyto penicillin (see algorithm p 687).Prior to 1980, penicillin history-posi-tive, skin test-positive patients whowere given cephalosporin had a reac-tion rate of approximately 10% to20%. Since 1980, reaction rates in pen-icillin history-positive, skin test-posi-tive patients who were given a cepha-losporin have decreased to 2%.66 Priorto 1980, all penicillin-allergic patientswho have reacted to a cephalosporin
VOLUME 83, DECEMBER, 1999 685
had been treated with cephalothin orcephaloridine. Benzyl penicillin andthese first generation agents share asimilar side chain, a finding that couldaccount for increased cross-reactivity.Also, during this time, some early firstgeneration cephalosporins were con-taminated with trace amounts of peni-cillin. Since 1980, contamination ofthis type has not been documented.Nevertheless, because of these dispar-ate observations, there is not a com-mon consensus regarding the manage-ment of a patient with a good history ofan IgE-mediated reaction to penicillinand who subsequently requires admin-istration of cephalosporin. The follow-ing are options that may be considered(1) substitute a non-beta lactam anti-biotic and (2) skin test the patient todetermine whether the patient has IgEantibodies to penicillin. If the skin testis negative, the patient can receive thecephalosporin. If the skin test is posi-tive, there may be an increased risk ofa reaction if the cephalosporin is givenand desensitization with the cephalo-sporin should be performed.If patients with histories of allergy
to penicillin are not skin tested butgiven a second or third generationcephalosporin directly, the chance of areaction is probably less than 1%.94This figure is based on the fact thatonly 15% to 20% of penicillin history-positive patients have positive skintests and, of those, only 2% will reactto a cephalosporin.95 This finding maybe interpreted to mean that skin testingis unnecessary as a 2% reaction ratemay occur even without a prior historyof allergy. It should be emphasized,however, that most of the 2% reactorswere cases of anaphylaxis, some ofwhich were fatal.92 For this reason, it isrecommended that penicillin skin test-positive patients should undergo a for-mal cephalosporin desensitization reg-imen.Administration of penicillin to a
patient with a history of allergy to acephalosporin. Patients with a historyof an immediate-type allergic reactionto a cephalosporin who require peni-cillin should undergo penicillin skintesting. If negative, they can receive
penicillin; if positive, they should re-ceive an alternate drug or undergo pen-icillin desensitization. If the patienthas a history of a non-IgE-mediatedreaction to cephalosporin [other thanerythema multiforme major/Stevens-Johnson syndrome (EMM/SJS) ortoxic epidermal necrolysis (TEN)] andrequires one of the cephalosporins, thepatient can undergo a graded chal-lenge. Skin testing with penicillin isnot appropriate in this setting.Cross-reactivity between carba-
penems, monobactams and cephalo-sporins. Carbapenems (eg, imipenem)should be considered potentially cross-reactive with cephalosporins becauseof the beta lactam ring.85 Cross-reac-tions between monobactams (eg, az-treonam) and cephalosporins have notbeen demonstrated, except for ceftazi-dime which has a side chain identicalto that of aztreonam.87,88
2. Non-Beta Lactam AntibioticsAllergic reactions to non-beta lactamantibiotics can cause morbidity and,rarely, mortality. The overall incidenceof hypersensitivity reactions to theseagents is estimated to be 1% to 3%.Some agents such as TMP-SMX aremore prone to induce such reactions,particularly in HIV-infected individu-als.96–98 Administration of a differentantibiotic may sometimes be necessaryin a patient whose history is consistentwith an allergic reaction to that non-beta lactam antibiotic. If the non-betalactam antibiotic is needed urgentlyand the history is consistent with anIgE-mediated reaction, desensitizationmay be required if an alternative drugis not available. If the drug is notneeded urgently and the history is con-sistent with a non-IgE-mediated mech-anism, cautious graded challengesometimes on an outpatient basis cangenerally be conducted.In the case of some antibiotics, there
are case reports of positive skin testswith the native drug; however, largescale validation of such skin testinghas not been accomplished. It is wellrecognized that most antibiotics havemultiple end products and therefore itis possible that the relevant allergens
may be metabolites and not the parentdrug. While no validated in vivo or invitro diagnostic tests are available fornon-beta lactam antibiotics, skin test-ing with nonirritative concentrations ofthe drug (ie, negative skin test reactiv-ity in a panel of normal, nonexposedvolunteers) may provide useful infor-mation. If the skin test is positive un-der these circumstances, it is likely thatdrug-specific IgE antibodies arepresent. The patient should thereforereceive an alternative antibiotic or un-dergo desensitization. On the otherhand, a negative test does not denotethat drug-specific IgE antibodies areabsent, since it is possible that a drugmetabolite not present in the test re-agent may be the relevant allergen. Ifthis particular antibiotic is required fortreatment, the amount of drug injectedintracutaneously can be used as theinitial starting dose for a desensitiza-tion procedure. Graded test dosingchallenge can also be performed in pa-tients with a history that suggests anon-IgE-mediated reaction other thanEMM/SJS or TEN. In general, for oralagents the starting dose is 0.1 mg. In-cremental doses can be administeredevery 30 to 60 minutes (eg, 1 mg, 10mg, and 50 mg) until a full therapeuticdose has been achieved.A generalized maculopapular reac-
tion is the most common manifestationof drug allergy due to TMP-SMX inpatients with AIDS. Many such pa-tients can tolerate readministration ofthe drug if given slowly over hours ordays. In severely ill patients, particu-larly those with Pneumocytis cariniipneumonia, more rapid administrationmay be necessary. A detailed discus-sion of TMP-SMX is presented in sec-tion X, Adverse Drug Reactions in Pa-tients with HIV Infections/AIDS (p694).Vancomycin has been reported to
cause drug fever, skin rash, or a dis-tinctive cutaneous lesion, the “redman’s syndrome” characterized bypruritus; erythema; and flushing of theface, neck, and upper throat; and some-times hypotension. Prospective studieshave noted that 50% to 90% of treatedpatients experience some of these man-
686 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
Figure 1. Cephalosporin algorithms.
VOLUME 83, DECEMBER, 1999 687
ifestations, although most of them aremild. These symptoms are due to non-specific histamine release that is raterelated, so that slowing the rate of in-fusion will generally prevent furthersymptoms. Addition of an H1 antihis-tamine also helps to alleviate symp-toms.99 IgE-mediated anaphylaxis tovancomycin has also been observedand may be identified by skin tests butit should be noted that skin tests atconcentrations �100 �g may elicit“false positive” wheal and flare reac-tions in normal skin. Anaphylaxisshould be managed in the same mannerdescribed for other non-beta lactam an-tibiotics.100Although aminoglycosides rarely
cause hypersensitivity reactions, thereare individual case reports of IgE-me-diated systemic reactions.101 Desensiti-zation is sometimes indicated when thedrug allergy is thought to involve IgEantibodies and no alternative antibioticis available. Both graded challenge anddesensitization procedures should beperformed by specialists experiencedwith these protocols and the possibleadverse events associated with them.Quinolones (eg, ciprofloxacin) are a
class of antibiotics related to nalidixicacid. Anaphylactoid reactions to thisclass of drug, often following the ini-tial dose, have been reported.102 Cuta-neous lesions appear in about 2% oftreated patients.103 Patients reacting toone quinolone are likely to react torelated drugs of this class.104
B. Cytotoxic Reactions (Gell-Coombs Type 2)
Cytotoxic reactions are very seriousand potentially life-threatening. Immu-nohemolytic anemias due to drugshave clearly been identified after treat-ment with quinidine, �-methyldopaand penicillin. In the case of penicillin,circulating anti-penicillin antibodies ofthe immunoglobulin G isotype havebeen implicated.9 The condition is rarebecause it apparently develops only inthose individuals capable of synthesiz-ing an atypical variety of IgG anti-penicillin antibody. Penicillin bindingby erythrocytes is an essential prelim-inary step in the sensitization process
and is more likely to occur in patientsreceiving very large and prolongeddose regimens of penicillin, as may berequired in the long-term treatment ofsubacute bacterial endocarditis. Aspreviously discussed, positive directand indirect Coombs’ tests in this con-dition also may indicate the presenceof complement on the red cell mem-brane or an autoantibody to an Rh de-terminant.43Thrombocytopenia resulting from
drug-induced immune mechanisms hasbeen well documented. The most thor-oughly evaluated drugs in this categoryare quinine, quinidine, acetaminophen,propylthiouracil, gold salts, and thesulfonamides. Platelet membrane dam-age is mediated chiefly by circulatingdrug-immune serum complexes whichare absorbed onto platelet membranes.Granulocytopenia also may be pro-
duced by cytotoxic antibodies synthe-sized in response to such drugs aspyrazolone derivatives, phenothia-zines, thiouracils, sulfonamides, andanti-convulsives. Immunologicallymediated destruction of peripheralneutrophils occurs within minutes afterreadministration of the drug and theimmunologic specificity of the anti-body has been verified by passivetransfer to nonsensitive volunteers (inthe pre-AIDS era).14
C. Immune Complex Reactions(Gell-Coombs Type 3)
Serum sickness was originally notedwhen heterologous antisera were usedextensively for passive immunizationof infectious diseases. Many small mo-lecular weight drugs are also associ-ated with serum-sickness-like symp-toms. These include penicillin, sulfo-namides, thiouracils, and phenytoin.The chief manifestations of fever, rash,urticaria, lymphadenopathy, and ar-thralgias typically appear 1 to 3 weeksafter the last dose of an offending drugand begin to subside when the drugand/or its metabolites are completelyeliminated from the body.34 Most ofthe clinical symptoms are thought to bemediated by IgG and possibly IgM-drug complexes. The overall immuneresponse in immune complex reactions
is heterogeneous because in somecases, IgE antibodies can also be dem-onstrated and may be associated withurticarial lesions seen early in thecourse of the disease.
D. Cell-Mediated Reactions (Gell-Coombs Type 4)
Allergic contact dermatitis after expo-sure to medications containing activedrugs, additives, or lipid vehicles inointments is the most frequent form ofdrug-mediated delayed hypersensitiv-ity. Morphologically, it usually cannotbe distinguished from contact irritantdermatitis. Almost any drug appliedlocally is a potential sensitizer but lessthan 40 allergens produce most casesof contact dermatitis. Among the drugsinvolved, the most universally ac-cepted offenders are topical formula-tions of penicillin, local anesthetics,and antihistamines. Potent excipienttopical sensitizers include the para-bens, formaldehyde, ethylenediamine,lanolin, and thimerosal.105 Complextopical products may contain many po-tential antigens and additives and inmany instances the major componentof a complex mixture may not neces-sarily be the sensitizer. Photoallergicdermatitis morphologically resemblesallergic contact dermatitis and iscaused by such drugs as sulfonamides,thiazides, quinidine, chlorpromazine,and fluoroquinolones. Once inductionsensitization has occurred, elicitationof dermatitis requires minimal expo-sure to light. Phototoxic, non-allergicreactions (eg, erythrosine) are histo-logically similar to photoallergic in-flammatory responses. As previouslydiscussed, T-cell mediated mecha-nisms (ie, CD8� T cells) have beendemonstrated in patients with late on-set cutaneous reactions such as morbil-liform and bullous eruptions.6,7
E. Miscellaneous SyndromesSpecific drugs or classes of drugs areassociated with characteristic syn-dromes which often do not conformwith specific Gell-Coombs categories.Although various specific immunephenomena can often be demonstratedin these syndromes, their roles in the
688 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
immunopathogenesis of the diseasehave not been clearly established.1. Drug Reactions Associated withSpecific Reactive EndProducts/Metabolites orPharmacogenetic PolymorphismsAlthough reactive metabolites may ex-ert non-immune toxic effects, theymay also haptenate body proteins toinitiate various immunopathogeneticeffects. Immunoreactivity has beenidentified with some drug reactions inthis category, but mixed mechanismsincluding direct toxicity cannot be en-tirely excluded.6Hypersensitivity vasculitis. Many
agents, hematopoietic growth factors,cytokines, and the interferons are sus-pected of causing widespread vascularinflammation of skin and visceral or-gans.38,106 Frequently, the vascularchanges occur during the course of orat the endstage of drug-induced syn-dromes of serum sickness or drug fe-ver. Drugs such as hydralazine, anti-thyroid medications, minocycline, andpenicillamine are often associated withc-ANCA or p-ANCA-positive vasculi-tis-like disease. Antinuclear cytoplas-mic antibody positive vasculitis is alsoassociated with hydralazine-inducedsystemic lupus erythematosus. Similarfindings also apply to propylthiouracil.Procainamide, an anti-arrhythmicagent, is the drug most commonly as-sociated with drug-related lupus.107Lupus-like features occur in 15% to30% of these patients and a large arrayof immune and autoimmune distur-bances has been reported. A Henoch-Schonlein syndrome with cutaneousvasculitis and glomerulonephritis maybe induced by carbidopa/levodopa.108Anti-Convulsant hypersensitivity
syndrome. This life-threatening syn-drome may occur after varying periodsof exposure to anticonvulsant medica-tions. It appears to result from an in-herited deficiency of epoxide hydro-lase, an enzyme required for themetabolism of arene oxide intermedi-ates produced during hepatic metabo-lism of anticonvulsant drugs. It is char-acterized by fever, a maculopapularrash and generalized lymphadenopathy
and resembles the progression ofsymptoms that occur during a serum-sickness-like reaction.109 Physicalsigns tend to persist for some time afterthe drug is discontinued. Biopsies oflymph nodes in this condition aresometimes confused with Hodgkin’sdisease and the entire syndrome hastherefore been called “pseudolym-phoma.” Hepatitis, nephritis, and leu-kocytosis with atypical lymphocytesand eosinophils may be part of thesyndrome. Facial edema occurs in 25%of the patients. These multi-organ re-actions may be induced by phenytoin,carbamazepine, or phenobarbital andcross-reactivity may occur among allanticonvulsants that produce toxicarene oxide metabolites. Valproic acid,gabapentin, and lamatrogine may beacceptable therapeutic alternativessince none of these agents producearene oxide.Pulmonary drug hypersensitivity.
Pulmonary manifestations of allergicdrug reactions include anaphylaxis, lu-pus-like reactions, alveolar or intersti-tial pneumonitis, edema, granulomato-sis, and fibrosis.110 Acute pneumonitiswith fever, rash, and eosinophilia oc-curs after treatment with nitrofuran-toin, NSAIDS, and sulfasalazine. If thedrugs are not eliminated promptly,these lesions may progress to a chroniccourse with interstitial fibrosis. Biop-sy-proven eosinophilic pneumoniamay occur after use of sulfonamides,penicillin, and para-aminosalicylicacid. Patchy pneumonitis, pleuritis andpleural effusion may appear during thecourse of various drug-induced lupussyndromes.37,107 Whether or not pleu-ropulmonary fibrosis has an immuno-logic basis is unknown at the presenttime. Characteristic histologic fibroticchanges are caused by certain cyto-toxic drugs such as bisulphan, cyclo-phosphamide, and bleomycin. Acutepulmonary reactions produced by otherfibrogenic drugs, such as methotrexate,procarbazine, and melphalan are simi-lar to those of nitrofurantoin pneumo-nitis and therefore appear to be medi-ated by hypersensitivity mechanisms.These lesions are sometimes confusedwith noncardiac pulmonary edema
which occurs after administration of her-oin, methadone, propoxyphene, or hy-drochlorothiazide. The clinical spectrumof pulmonary hypersensitivity reactionsmay include interstitial pneumonitis(with or without eosinophilia), bronchi-olitis obliterans [with or without orga-nized pneumonia (BOOP)], the pulmo-nary-renal syndrome associated withpenicillamine, and granulomatous le-sions.110,111 The Churg-Strauss syn-drome, a systemic granulomatous andvasculitic process which also involvesthe lung, has been reported in an increas-ing number of patients receiving severaldrugs (glucocorticosteroids, leukotrienereceptor antagonists, and macrolide anti-biotics).112–114 A causal relationship be-tween these drugs and the Churg-Strausssyndrome has not been established. Thislife-threatening disease usually occurs inpatients with a history of asthma, espe-cially after oral glucocorticosteroid with-drawal.Immunologic hepatitis. There is
strong circumstantial evidence that im-munologic hepatitis occurs after sensi-tization to para-amino-salicylic acid,sulfonamides, and phenothiazines.115Cholestatic jaundice is a prominent fea-ture of phenothiazine-induced liver dis-ease. Less well-defined are possible im-munologic aberrations associated withhepatocellular changes occurring afterhalothane, anti-convulsives, erythromy-cin, indomethacin, and isoniazid.Blistering disorders: (1) Erythema
multiforme minor. Erythema multiformeminor appears to be a cell-mediated hy-persensitivity reaction associated withviruses, other infectious agents, anddrugs. It is often referred to as erythemamultiforme “minor” and is manifestedby pleomorphic cutaneous eruptions, attimes bullous.116 Target lesions are alsocharacteristic. If a drug cause is sus-pected, the drug should be stopped im-mediately and the addition of glucocor-ticosteroids may be necessary. Anti-histamines may help pruritus. Earlytreatment of erythema multiforme minor(prednisone 1 mg/kg/qd) may preventprogression to the more serious ery-thema multiforme major/Stevens-John-son syndrome.
VOLUME 83, DECEMBER, 1999 689
(2) Erythema multiforme major/Stevens-Johnson syndrome.Drugs are animportant cause of the erythema multi-forme major/Stevens-Johnson syn-drome (EMM/SJS) as well as toxicepidermal necrolysis (TEN). Thus far,more than a hundred drugs have beenimplicated as causes of these syn-dromes. In a large prospective cohortstudy, drugs associated with a high rel-ative risk of developing SJS or TENwere sulfonamides, cephalosporins,imidazole agents, and oxicam deriva-tives; while drugs in the moderate riskcategory included quinolones, carbam-azepine, phenytoin, valproic acid, andglucocorticosteroids.117 As previouslydescribed under Physical Examination(see p 679), target and bullous lesionsprimarily involving the extremities andmucous membranes are characteristicof EMM while the features of SJS areconfluent purpuric macules on faceand trunk and severe, explosive muco-sal erosions, usually at more than onemucosal surface, that are accompa-nied by high fever and severe consti-tutional symptoms. Ocular involve-ment may be particularly serious.Liver, kidney and lungs may be in-volved singly or in combination. Assoon as the diagnosis is established,the suspected drug should be stoppedimmediately. The use of glucocortico-steroid therapy is controversial.117–119If it is started, it should probably bestarted early in the course of the dis-ease and very large doses (eg, 80 to160 mg) of intravenous methylpred-nisolone (every 4 to 6 hours) should beused. If this treatment is started toolate in the course of the disease (ie, 3to 4 days after onset), it is possible thatTEN could supervene, in which casesystemic glucocorticosteroids are con-traindicated.116,120(3) Toxic epidermal necrolysis.
Stevens-Johnson syndrome and TENare probably part of a single spectrum.If epidermal detachment is less than10%, the disease is probably Stevens-Johnson but when epidermal detach-ment reaches 30% or more, the diag-nosis of toxic epidermal necrolysis isprobable.117 In cases with detachmentof 10% to 30% of the epidermis, the
two syndromes are overlapping. Toxicepidermal necrolysis is almost alwaysdrug-induced and is manifested bywidespread areas of confluent ery-thema followed by epidermal necrosisand detachment with severe mucosalinvolvement. Significant loss of skinequivalent to a third degree burn oc-curs. Glucocorticosteroids are contra-indicated in this condition which mustbe managed in a burn unit.115,116 Thereis a significant risk of infection andmortality is significant. Toxic epider-mal necrolysis should be distinguishedfrom the scalded skin syndrome, a dis-order caused by staphylococcal bacte-rial toxin and characterized by themassive skin cleavage and separationin the uppermost epidermis. Recently,intravenous gamma globulin (0.2 to0.75 g/kg body weight per day for 4days) provided dramatic improvementwith complete recovery in some TENpatients with increased levels of Fasligand.121“Serum sickness-like reactions”
associated with cephalosporins. Ce-faclor and cefprozil are associated with“serum-sickness-like” reactions char-acterized primarily by severe erythemamultiforme and arthralgias. There is noevidence of an antibody-mediated ba-sis for this reaction.122,123 So far, thisreaction has only been reported withthese drugs. Anecdotally, affected pa-tients later have tolerated non-relatedcephalosporins. Such patients shouldavoid the offending drugs and othercephalosporins with similar sidechains. “Serum-sickness-like” reac-tions to cefaclor appear to result fromaltered metabolism of the parent drugresulting in reactive intermediate com-pounds.124 This altered metabolism canoften be documented in a parent of thepatient.2. Immunologic NephropathyThe major example of drug-inducedimmunologic nephropathy is an inter-stitial nephritis induced by large dosesof benzylpenicillin, methicillin, or sul-fonamides. In addition to symptoms oftubular dysfunction, these patientsdemonstrate fever, rash, eosinophilia(especially in the urine), and high lev-
els of total IgE which revert to normalupon discontinuation of the offendingdrug.21 The predominant lesion of thenephrotic syndrome induced by gold,penicillamine, and allopurinol is amembranous glomerulonephritis. Animmunologic basis of this lesion issuggested by deposition of IgG, IgM,and C3 in glomerular lesions.49 In therare pulmonary-renal syndrome in-duced by penicillamine, “lumpy” intra-glomerular deposits of complementand/or immunoglobulins are com-monly observed.111
3. Cancer Chemotherapeutic AgentsCancer chemotherapeutic agents arewell recognized as causes of hypersen-sitivity reactions.125 Some agents, suchas L-asparaginase cause hypersensitiv-ity reactions in more than 10% of pa-tients when given intravenously.126 Thereaction rate is less when it is given bythe intramuscular route. Immediatehypersensitivity Type 1 reactions arethe most common. Doxorubicin, cis-platin, and carboplatin are drugs com-monly associated with IgE-mediatedType 1 reactions.127,128 The latter twodrugs have been reported to cause ane-mia probably mediated by a cytotoxicimmunologic reaction. In addition,some reactions due to these drugs orexcipients in parenteral formulationsappear to be mediated by non-immu-nologic degranulation of basophilsand/or mast cells (eg, Cremophor-El, alipid solvent vehicle in some intrave-nous preparations, particularly pacli-taxel).13 Bleomycin has been reportedto cause arthralgias, pulmonary infil-trates and fever, presumably due toimmune complexes.125,129Methotrexate is the most frequent
cause of non-cytotoxic pulmonary re-actions.130,131 Symptoms of fever,cough, and dyspnea may occur any-where from several days to severalmonths after initiation of therapy. Thechest roentgenogram is characterizedby a diffuse, fine interstitial infiltrate.When the drug is discontinued, symp-toms and pulmonary infiltrates typi-cally clear within a few days. If thedrug is inadvertently continued, inter-stitial fibrosis may ensue. Bleomycin
690 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
and procarbazine are most commonlyassociated with cytotoxic pulmonaryreactions but also have been reportedto cause reactions similar to those as-cribed to methotrexate.110,130
4. Blood and Blood ProductsAcute urticarial reactions occur in 1%to 3% of blood transfusions, while sig-nificant bronchoconstriction/laryngealedema and anaphylactic shock occur in0.1% to 0.2% and 0.002% to 0.005%,respectively.132 Diagnostic in vivo orin vitro tests are not available for suchreactions. Rarely, a patient totally lack-ing serum IgA may develop specificIgE or IgG antibodies against IgA andsubsequently react to IgA in the bloodtransfusion or in trace amounts con-tained in some preparations of intrave-nous gamma globulin.133,134 Activationof complement and other non-IgE-me-diated reactions may also occur afterblood transfusions, presumably as a re-sult of alloantigenic reactivity.132 Re-actions to human serum albumin areextremely rare (0.01%) but occasion-ally allergic patients exhibit positiveprick tests to albumin-containing di-luent solutions.135 Such reactivity hasbeen demonstrated in house dust mite-sensitive patients tested with mite cul-ture medium containing human serumalbumin components.5. ProtamineProtamine sulfate is a low molecularweight (4500 daltons) polycationicprotein isolated from salmon testes. Itis used to reverse the anti-coagulanteffects of heparin after a variety ofprocedures including cardiopulmonarybypass and hemodialysis. It is alsocomplexed to insulin [neutral prota-mine Hagedorn (NPH) insulin] in or-der to delay absorption. Immediategeneralized reactions to protamine in-cluding hypotension, shock, and deathhave been reported.63,136,137 The occur-rence of dose-dependent hypotensionafter rapid intravenous administrationmay be a manifestation of non-specifichistamine release.138 The fact, how-ever, that diabetic patients receivingprotamine-containing insulins appearto be at 40 to 50 times greater risk for
developing anaphylaxis and other ad-verse reactions to intravenous prota-mine suggests that immune mecha-nisms are also involved.136 Detailedinformation about these reactions andrecommended management may befound in “Practice Parameters of theDiagnosis and Management of Ana-phylaxis” (J Allergy Clin Immunol1998;101:S507–S509).6. HeparinAdverse reactions to heparin include lo-calized urticarial reactions at injectionsites, hypereosinophilia and anaphylaxis,all of which are immunologically medi-ated.64,139,140 Heparin-induced thrombo-cytopenia may present in various forms.Mild thrombocytopenia is due to plateletaggregation and is reversible after stop-ping the drug.139 A more severe clinicalproblem is sudden and massive throm-bocytopenia, thrombosis, and necrosiswhich occurs after about 5 days of treat-ment. This is caused by immune com-plexes, a component of which is a hep-arin-dependent IgG specific for plateletfactor 4.139,141 This syndrome has notbeen observed in patients treated withlow molecular weight heparin.142 If thisoccurs, heparin should be discontinuedand the use of warfarin or anti-plateletdrugs should be considered.139
7. Drug Reactions During theOperative and Perioperative PeriodsAnaphylactic/anaphylactoid reactionsare not infrequent during general anes-thesia.143 These reactions may be at-tributed to a number of drugs com-monly used in an operative setting.These include induction agents, mus-cle relaxing agents, opiates, antibiot-ics, and contact with latex allergen.The incidence of life-threatening reac-tions to muscle relaxants has been es-timated at 1 in 4,500 anesthesiaevents.144 Some muscle relaxants, suchas curare, are potent histamine releas-ing agents.145,146 Others such as atra-curium, pancuronium, and vecuroniumare less potent in this regard. Drug-specific IgE antibodies have been dem-onstrated to some of these agents sothat it is apparent that reactions to mus-cle relaxants may involve more than
one mechanism.147 The diagnosis andmanagement of reactions occurringduring and after surgery are discussedin more detail in “Practice Parametersof the Diagnosis and Management ofAnaphylaxis” (J Allergy Clin Immunol1998;101:S512–S515).8. Local AnestheticsPossible systemic allergy to local an-esthetics is often of concern to patientsand their dentists or physicians. Docu-mentation of IgE-mediated reactions israre. Most adverse reactions to localanesthetics are due to nonallergic reac-tions that include vasovagal reactions,toxic or idiosyncratic reactions due toinadvertent intravenous epinephrine oranxiety.148 Of these, anxiety is proba-bly the most difficult to manage; there-fore, the history of a previous reactionmust be carefully evaluated. First, it isnecessary to determine the type of lo-cal anesthetic to be used. Local anes-thetics are either group 1 benzoic acidesters (eg, procaine and benzocaine) orgroup 2 amides (eg, lidocaine andmepivacaine). While the benzoic acidesters often cross-react with eachother, they do not cross-react with thegroup 2 amide drugs. Graded chal-lenge tests may then be performed us-ing incremental concentrations of thelocal anesthetic which the dentist in-tends to use. This test reagent shouldnot contain epinephrine or other addi-tives such as parabens or bisulfites.When there is concern about a previ-ously reported reaction, skin testingand incremental challenge with a non-cross-reacting drug (ie, from anotherclass of local anesthetics) is a reason-able approach in the evaluation of apossible reaction.A simple graded challenge proce-
dure is used to demonstrate whether areaction will occur.149 Prick skin testsare first performed with the undilutedanesthetic. If this is negative, succes-sive injections (subcutaneous or intra-cutaneous) of 0.1 mL of 1:100 dilution,1:10 dilution and the full strength so-lution are given at 15-minute intervals.If reactions are not encountered, 0.5 to1 mL of the anesthetic is injected sub-cutaneously. Using this protocol, there
VOLUME 83, DECEMBER, 1999 691
have been no serious allergic reactionsreported following administration oflocal anesthetics if the skin tests andtest dosing are negative.150Dentists and other health care pro-
fessionals may develop contact derma-titis from local anesthetics. In the eventthat this occurs, patch testing should beperformed to determine the degree ofsensitization to the suspected local an-esthetic and identify the agent(s) whichis least likely to produce a reaction.
VIII. PSEUDOALLERGICREACTIONS
A group of reactions known aspseudoallergic must be differentiatedfrom immune-mediated syndromes.151These are mediated by a diverse groupof agents such as opiates, ASA/NSAIDS, colloid volume expanders,basic polypeptide agents (eg, poly-mixin B, ACTH) RCM, and excipients(eg, Cremophor-EL), among others.Acute reactions to these substances arecaused by direct release of mediatorsfrom mast cells and basophils resultingin the classic end organ effects thatthese mediators exert. Direct mediatorrelease occurs without evidence of aprior sensitization period, specific IgEantibodies, or antigen-antibody bridg-ing on the mast cell/basophil cell mem-brane. The nonimmune reaction is im-mediate and often severe. Because it isnonimmunologic it may occur the firsttime that the host is exposed to theseagents. The reactions are of further in-terest because they can also be elicitedby small doses of the offending sub-stance. It is possible that some of thesereactions could be based in part uponnonimmunologic release of anaphyla-toxins (C3a, C5a) through activation ofthe alternative complement pathway.Neuropeptides (eg, substance P) andendorphins may also activate and in-duce mediator release from mast cells.Osmotic alterations may lead to non-specific mediator release (eg, hyperos-molar mannitol) but such physical ef-fects are more likely to occur at localtissue sites such as the nose or bronchi.
A. OpiatesOpiates such as morphine, meperidine,codeine, and narcotic analogs canstimulate mast cell-mediated releasedirectly without an immunologicmechanism. Patients with this problemexhibit generalized pruritus and urti-caria after injection of the respectivenarcotic. Occasional mild wheezingmay be noted. Skin tests to opiates aredifficult to interpret because theseagents cause release of histamine fromskin mast cells in all patients. Verydilute skin test concentrations havebeen recommended if an IgE-mediatedreaction is suspected.152 Some opiatereactions can be attenuated by pread-ministration of antihistamines. Narcot-ic-induced pseudoallergic reactions arerarely life-threatening. If there is a pos-itive history of such a reaction to anagent and analgesia is required, a non-narcotic alternative pain medicationshould be selected. If this does notcontrol pain, graded challenge with analternative opiate up to a dose that willcontrol pain should be tried. A singlecase of a documented IgE-mediated re-action to morphine has been reported.153
B. Radiocontrast MediaRadiocontrast media containing organiciodine may cause adverse reactions suchas generalized urticaria/angioedema,bronchospasm, laryngospasm, shock,and death. A review of 10,000 consecu-tive intravenous urograms reveals thatthe incidence of pseudoallergic reactionsis 1.7%.154 The frequency of fatal reac-tions is 1 in 50,000 intravenous poly-gram procedures.155 These adverse reac-tions are not mediated by specific IgEantibodies. Only 16% of individualswith a previous immediate generalizedreaction after intravenous injection of io-dinated radiographic compound respondwith symptoms on the second chal-lenge.156 If these reactions had been me-diated by specific IgE, it would be ex-pected that a higher percentage of suchpatients would have experienced gener-alized reactions after the second chal-lenge dose. No single pathogenic mech-anism accounts for these unpredictableclinical manifestations but it is likely thatmast cell activation accounts for the ma-
jority of these reactions. Activation ofcomplement components has been de-scribed but not in all cases. Radiocon-trast media can also cause intravascularvolume expansion and precipitate “car-diogenic” pulmonary edema in patientswith ischemic cardiac heart disease.157There is no evidence that sensitivity toseafood or “iodine” predisposes or iscross-reactive with RCM reactions. Al-though predictive tests are not available,patients with documented atopic profilesand those using beta blocking agents ap-pear to be at significant risk for RCManaphylactoid reactions.158,159Management of a patient who re-
quires RCM and has had a prior reac-tion to RCM includes the following(1) determine if the study is essential;(2) determine that the patient under-stands the risks; (3) ensure proper hy-dration; (4) use a non-ionic, lower os-molar RCM, especially in high riskpatients (asthmatic patients, patientson beta blockers and those with cardio-vascular disease)160 and (5) use a pre-treatment regimen which has been doc-umented to be successful in preventingmost reactions.161 One reported regi-men consists of prednisone 50 mg(p.o.) 13, 7, and 1 hours before theprocedure, diphenhydramine 50 mgone hour before the procedure and ei-ther ephedrine 25 mg or albuterol 4mg 1 hour prior to the procedure.Some investigators prefer combiningan H2 antagonist with the H1 antago-nist one hour before the procedure andomitting ephedrine or albuterol.
C. Other AgentsAnaphylactoid reactions have been de-scribed after administration of manycolloid volume expanders (dextran,gelatin, hydroxyethel starch, and hu-man serum albumin).135 An effectivegraded challenge protocol may be usedto prevent severe anaphylactoid reac-tions to dextran contained in iron-dex-tran complexes.162 This may be lifesaving in patients who require paren-teral iron. Life threatening reactions tothe osmotic diuretic, mannitol, is mostlikely due to hyperosmolar-dependenthistamine release. Systemic anaphy-lactoid reactions may occur after par-
692 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
enteral administration of Cremophor-El, a solvent for paclitaxel, teniposide,cyclosporin, and some anesthetics.There are also anecdotal reports of reac-tions to sodium benzoate and chlorobu-tanol that are used as preservatives invarious biologicals. Some drugs mayhave clinical presentations that oftencannot be distinguished from anaphy-laxis. These include ASA, NSAIDs, van-comycin, protamine, and quinolones.
IX. NON-IMMUNE DRUGIDIOSYNCRASY/INTOLERANCE REACTIONS
A. Aspirin and Non-Steroidal Anti-inflammatory Agents
Aspirin and NSAIDs cause a spectrumof adverse reactions which include (1)cardiorespiratory, anaphylactoid reac-tions occurring within minutes after in-gestion of ASA or an NSAID; (2) ur-ticaria and/or angioedema afteringestion of ASA/NSAID; (3) exacer-bation of urticaria in patients withchronic idiopathic urticaria; or (4)asthma with or without rhinoconjunc-tivitis in about 10% of patients withchronic rhinitis, sinusitis, nasal polypsand/or asthma.163 The association ofasthma, nasal polyps, and aspirin sen-sitivity is termed the aspirin triad. Thenomenclature ascribed to this reactionis not standardized and terms such asaspirin idiosyncrasy, aspirin intoler-ance, aspirin sensitivity or simply, as-pirin-induced asthma are commonlyused.164 A few episodes of allergic al-veolitis (hypersensitivity pneumonitis)have been reported after ingestion ofan NSAID.165The role of IgE-mediated mecha-
nisms in patients who experience acuteurticaria/angioedema after ingestionof these drugs is controversial. Al-though several early studies reportedanti-aspiryl antibodies in some pa-tients, they did not correlate eitherwith urticarial or respiratory symp-toms.166,167 Specific antibodies to aspi-rin anhydride, a former contaminant ofcommercial aspirin, were encounteredin a few patients.168 Anaphylactoid re-actions to ASA and NSAIDs associ-ated with vascular collapse are sugges-
tive of anaphylaxis because they occurafter 2 or more exposures to ASA or toa specific NSAID and these patients donot have preexistent histories of urti-caria, nasal polyps, and asthma.169These patients do not experience cross-reactions with other NSAIDS whichinhibit COX-1 and COX-2 enzymes.164The bronchoconstriction that occurs
in asthmatics with nasal polyps is mostlikely due to aspirin-induced blockageof COX-1 and COX-2 specific cyclo-oxygenase metabolic pathways withsubsequent decreased synthesis ofPGE2 which results in accumulation of5-lipoxygenase and increased produc-tion of leukotrienes.164,169 Agents thatinhibit 5-lipoxygenase activity or leu-kotriene (LT) receptors may be bene-ficial in this syndrome.170,171 All pa-tients with the ASA triad and a third ofpatients with chronic idiopathic urti-caria have cross-reactions withNSAIDS. Acetaminophen in doses�1000 mg and pyrazolones that havestronger blocking effects on the cy-cloxygenase pathway induce cross-re-actions in about a third of aspirin-sen-sitive patients. Baseline urinaryleukotriene E4 levels are increased inASA-sensitive patients compared withASA-tolerant asthmatics and increasemarkedly 2 to 4 hours after ASA chal-lenge.The diagnosis of ASA/NSAID intol-
erance can usually be established byhistory and often does not require con-firmation. Skin testing is of no valueand there are no commercially avail-able in vitro tests for detection of ASAand NSAID sensitivity. When the his-tory is unclear or erroneous (about15% of the time) or where more defi-nite diagnosis is required, the only ac-ceptable diagnostic test is a controlledoral challenge test graded test dos-ing).163 When the history is primarilyurticaria or a respiratory reaction, testdosing may be performed in an outpa-tient setting with appropriate emer-gency equipment.172Patients with intolerance reactions
to ASA/NSAID are also at risk fordeveloping similar reactions to otherdrugs or excipients. Several earlierstudies revealed that a small percent-
age of individuals with aspirin intoler-ance develop bronchospasm afterchallenge with tartrazine, a colorantadditive structurally related to pyrazo-lones.173–175 These results were notconfirmed by other investigatorswhose patients were receiving bron-chodilators in order to stabilize air-ways before placebo and tartrazinechallenges.176,177 The symptoms pro-duced by tartrazine in these individu-als are usually similar to those pro-duced by aspirin and a similarpathogenetic mechanism(s) is postu-lated. Adverse reactions to tartrazinecan occur in the absence of ASA/NSAID intolerance.178Management includes selection of
analgesics with minimal or no inhibi-tion of specific COX-1 cyclooxygen-ase activity [eg, acetaminophen(�1,000 mg), nonacetylated salicy-lates, opiates, and dextropropoxy-phene]. It has yet to be determinedwhether COX-2 inhibitors will besafely tolerated by patients with ASA-induced asthma.164 Desensitization ofASA-intolerant asthmatics may be ap-propriate if ASA or an NSAID is ther-apeutically necessary or asthma ispoorly controlled with current medicalmanagement. Aspirin desensitizationis not effective in aspirin-sensitive ur-ticaria and/or angioedema.179 Aspirindesensitization in patients with a his-tory of ASA-induced systemic (ana-phylactoid) reactions should be per-formed in an intensive care facility. Itis not without risk but has been suc-cessful in selected patients.169
B. Angiotensin-Converting Enzyme(ACE) Inhibitors
Two major adverse effects, cough andangioedema, are associated with theuse of ACE inhibitors.180,181 Generallycough and angioedema do not occur inthe same patient. These symptoms arenot associated with immunologic reac-tions. Although plasma bradykinin lev-els are elevated in many of these pa-tients, the etiologic basis of bradykininactivation is not known.182The incidence of cough may range
up to 25% and about 10% of patientsrequire discontinuation of therapy.180
VOLUME 83, DECEMBER, 1999 693
Cough is twice as common in womenthan men. In most cases, cough disap-pears within 1 to 2 weeks after discon-tinuation of the respective drug. Theincidence of cough associated with theuse of enalapril and lisinopril is higherthan that associated with the use ofcaptopril.183 Angiotensin II receptor in-hibitors do not induce cough.Angioedema is a potentially life-
threatening complication of ACE in-hibitors. It appears in 0.1% to 0.2% ofpatients receiving these drugs. Thetemporal relationship between initia-tion of these drugs and occurrence ofangioedema is unpredictable and dif-fers from the temporal pattern of otheradverse drug reactions. In addition thepattern of relapses and remissions isatypical of drug allergy. The majorityof reactions occur more than 1 monthafter the initial dose. About one-thirdof patients experiencing these episodesrequire hospitalization; 10% requireintensive care.181 These statistics in-crease considerably if recurrences oc-cur (ie, hospitalization, 45% and inten-sive care, 28%). Further, intubation ismore likely to be required in the treat-ment of relapsing patients; therefore,physician recognition of this syndromeis essential for prevention of relaps-es.181 As is the case with ACE-inducedcough, patients receiving enalapril andlisinopril are more likely to experiencethese reactions than those on captopril.There have been rare reports of ab-dominal pain and ascites associatedwith angioedema of the abdominal vis-cera due to ACE inhibitors. Angio-edema may persist for several weeksafter the drug is discontinued. Thereare several reports of angioedema as-sociated with use of angiotensin II re-ceptor inhibitors.184
C. PreservativesSome preservatives may evoke coughand bronchoconstriction in susceptibleasthmatic patients after exposure tonebulizer solutions or formulationscontaining benzalkonium chloride orsulfites.185 It has been suggested thatsusceptibility to sulfites in some asth-matic patients may be due to a defi-ciency of sulfite oxidase.186
X. ADVERSE DRUGREACTIONS IN PATIENTSWITH HIV INFECTION/AIDS
Drug reactions are common in patientswith AIDS and, in some cases the in-cidence of reactions may be related tothe degree of immunodeficiency.187–197These reactions cause significant mor-bidity and mortality in this population.Unfortunately, the pathogenesis ofthese reactions is unknown. Adversereactions to sulfonamides (SMDs) maycomplicate both treatment and prophy-laxis of Pneumocystis carinii pneumo-nia in many patients with AIDS.187–195Unlike reactions to amoxicillin196 andanti-mycobacterial agents,197 adversereactions to SMD may decline withHIV disease progression.198 To date,risk factors for the development ofdrug intolerance/reactivity in patientswith AIDS have not been clearly iden-tified. Evidence exists to suggest thatcoexistent cytomegalovirus or Epstein-Barr virus infections, altered drug me-tabolism, slow acetylator phenotype,high-dose TMP-SMX treatment and/orglutathione deficiency may play a rolein the development of reactivity.199–204Adverse cutaneous SMD reactionsmay be tolerated without ceasing ther-apy in some cases. Sulfonamidesshould be discontinued immediatelyhowever, if any of the following de-velop: (1) persistent rash and/or feverfor more than 5 days; (2) absolute neu-trophil count �500/m3; (3) hypoten-sion; (4) dyspnea; or (5) any signs ofblistering, desquamation of the skin ormucous membrane involvement.194There appears to be a relationship
between the development of adverseSMD reactions and the dose adminis-tered, since some patients can continuetreatment after interruption of therapyor lowering of the dosage.188,196,198,200The degree of clinical cross-sensitivitybetween different SMDs is not known.The degree of clinical cross-sensitivitybetween TMP-SMX and dapsone isthought to be low, and it appears thatthe majority of patients who react toTMP-SMX may tolerate dapsone.Dapsone, however, probably shouldnot be used in those patients in whom
TMP-SMX caused the Stevens-John-son syndrome or visceral involvementsuch as hepatitis or pneumonitis.192The most common reaction to
SMDs is a morbilliform, maculopapu-lar eruption often associated with feverthat occurs after 7 to 12 days of ther-apy. Immediate (anaphylaxis, urticaria,and mucosal angioedema) and delayed(erythema multiforme minor, erythemamultiforme major/Stevens-Johnsonsyndrome, toxic epidermal necrolysis)hepatic, hematologic, renal, and im-mune complex reactions may occur.The spectrum of clinical manifesta-tions of SMD reactions in patients withAIDS suggests that most of these reac-tions are not IgE-mediated. In addition,the observation that desensitization pro-tocols beginning with relatively highstarting doses are often successful inSMD-allergic AIDS patients lends fur-ther support to the impression that analternative pathogenic mechanism is op-erative. The possible increased preva-lence of slow acetylation and altered ac-tivity of oxidative metabolic pathways inAIDS patients with acute illnesses maypartly explain the increased incidence ofadverse drug reactions in these pa-tients.195,199,202 Sulfonamide-specific IgGand IgM antibodies have been found inpatients with AIDS, both those with andwithout skin reactions to SMDs. It isunlikely that these antibodies play apathogenic role in SMD hypersensitivityreactions.205 For those individuals whodevelop maculopapular rashes afterSMD administration, several gradedchallenge protocols have been developedand used successfully.53,206–209 Reintro-duction of a SMD by one of these pro-tocols optimally should not take placeany earlier than 1 month following theinitial adverse reaction nor should any ofthese be used in individuals with a his-tory of bullous dermatitis or Stevens-Johnson syndrome. It may be started ear-lier, however, if treatment of a seriousinfection requiring these drugs is neces-sary. Sulfadiazine,210 acyclovir,211zidovudine, dapsone, and pentamidine212“desensitization” protocols have alsobeen developed for patients with AIDS.Ciprofloxacin-induced anaphylactoid re-
694 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
actions may occur more frequently inpatients with AIDS.103,213In addition to SMDs, patients with
AIDS may have an increased fre-quency of adverse reactions to a num-ber of other agents including (1) anti-tuberculous agents, (2) pentamidine,(3) amoxicillin-clavulanic acid, (4)clindamycin-primaquine, (5) carbam-azepine, (6) phenytoin, (7) thalido-mide, (8) foscarnet, and (9) zidovu-dine.195,214 The fact that these reactionsare clinically diverse suggests that theymay be produced by a variety of mech-anisms.It is likely that the pathogenic mech-
anisms responsible for reactions toSMD in patients with AIDS are multi-factorial. While these reactions are of-ten described as “allergic” in nature, itis unlikely that a single mechanismalone is operative. In fact, there aredata to support both toxic and immu-nologic mechanisms. In addition, otherfactors such as high-dose SMD therapyand severe immunodeficiency mayinfluence the development of SMDhypersensitivity in patients withAIDS.191,200,215
REFERENCES1. Lazarou J, Pomeranz BH, Corey PN.Incidence of adverse drug reactionsin hospitalized patients. JAMA 1998;279(15):1200–1205.
2. Classen DC, Pestotnik SL, Evans FS,Burke JP. Computerized surveillanceof adverse drug events in hospital pa-tients. JAMA 1989;266(20):2847–2852.
3. Moore TJ, Psaty BM, Furberg CD.Time to act on drug safety (Commen-tary). JAMA 1998;279(19):1571–1573.
4. Stanworth DR. The role of non-antigen receptors in mast cell signal-ing processes. Mol Immunol 1984;21:1183–1190.
6. Griem P, Wulferink M, Sachs B, etal. Allergic and autoimmune reac-tions to xenobiotics: how do theyarise? Immunol Today 1998;19:133–141.
7. Hertl M, Mark HF. Lymphocyte ac-
tivation in cutaneous drug reactions.J Invest Dermatol 1995;105:955–985.
8. Arndt K, Jick H. Rates of cutaneousreactions to drugs. A report from theBoston Collaborative Drug Surveil-lance Program. JAMA 1976;225:918–923.
9. Levine BB. Immunologic mecha-nisms of penicillin allergy. Seminarsin Medicine of the Beth Israel Hospi-tal, Boston (Feingold DS, Parris EE,eds), N Engl J Med 1966;275:1115–1125.
10. Patterson DL, Yunginger JW, et al.Anaphylaxis induced by the car-boxymethylcellulose component ofinjectable triamcinolone acetonidesuspension. (Kenalog). Ann Allergy1995;74:163–166.
11. Giorgini S, Melli MC, Sertoli A.Comments on the allergenic activityof lanolin. Contact Dermatitis 1983;9(5):425–426.
12. Hjorth N, Trol’e-Lassen C. Skin re-actions to ointment bases, Trans. St.Johns Hosp; Dermatol Soc 1963;49:127–140.
13. Weiner M, Bernstein IL. Adverse re-actions to drug formulation agents, Ahandbook of excipients. New York:Marcel Dekker, Inc, 1989;209–211;238–241.
14. Parker CW. Drug allergy. N EnglJ Med 1975;292:511–514; 732–736;809–810.
15. Adams LE, Mongey A-B. Role ofgenetic factors in drug-related auto-immunity. Lupus 1994;3:443–447.
16. Black AJ, McLeod HL, Capell HA, etal. Thiopurine methyltransferase ge-notype predicts therapy-limiting se-vere toxicity from azathioprine. AnnIntern Med 1998;129:716–718.
17. Mauri-Hellweg D, Zanni M, Frei E,et al. Cross-reactivity of T-cell linesand clones to beta-lactum antibiotics.Immunology 1996;157:1071–1079.
19. Padovan E, Bauer T, Tongio MM, etal. Penicilloyl peptides are recog-nized as T-cell antigenic determi-nants in penicillin allergy. Eur J Im-munol 1997;27:1303–1307.
21. Ooi BS, Pesce AJ, First MR, et al.IgE levels in interstitial nephritis.Lancet 2: 1974;1:1254–1256.
22. Shulman NR. Immunologic reactionsto drugs. N Engl J Med 1972;286:408–409.
23. Bigby M, Jick S, Jick H, et al. Drug-induced cutaneous reactions: a reportfrom the Boston Collaborative DrugSurveillance Program on 15,438 con-secutive inpatients, 1975–1982.JAMA 1986;256:3358–3363.
24. Lang DM, Alpern MB, VisintainerPF, Smith ST. Gender risk for ana-phylactoid reaction to radiographiccontrast media. J Allergy Clin Immu-nol 1995;95:813–817.
25. Moseley EK, Sullivan TJ. Allergicreactions to antimicrobial drugs inpatients with a history of prior drugallergy [Abstract]. J Allergy Clin Im-munol 1991;87:226.
29. Dolan TP, Meyers A. Bronchialasthma and inhaled rhinitis associatedwith inhalation of pancreatic extracts.Am Rev Respir Dis 1974;110:812–813.
30. Sogn DD. Prevention of allergic re-actions to penicillin. J Allergy ClinImmunol 1987;78:1051–1052.
31. Witten DM. Reactions to urographiccontrast media. JAMA 1975;231:974–977.
32. Idsoe O, Guthe T, Willcox RR, De-Weck AL. Nature and extent of pen-icillin side-reactions, with particularreferences to fatalities from anaphy-lactic shock. Bull Wld Health Org1968;38:159–188.
33. Roujeau JC, Stern RS. Severe ad-verse cutaneous reactions to drugs.N Engl J Med 1994;331:1272–1284.
34. Lawley TJ, Bielory L, Gascon R, etal. A prospective clinical and immu-nologic analysis of patients with se-rum sickness. N Engl J Med 1984;311:1407–1413.
35. Chan HL, Stern RS, Arndt KA, et al.
VOLUME 83, DECEMBER, 1999 695
The incidence of erythema multi-forme, Stevens-Johnson syndrome,and toxic epidermal necrolysis: apopulation-based study with particu-lar reference to reactions caused bydrugs among outpatients. Arch Der-matol 1990;126:43–47.
36. Mackowiak PA, LeMaistre CF. Drugfever: a critical appraisal of conven-tional concepts. Ann Intern Med1987;106:728–733.
37. Adams LE, Hess EV. Drug-relatedlupus. Incidence, mechanisms andclinical implications. Drug Safety1991;6:431–449.
38. Jennette JC, Falk RJ. Small-vesselvasculitis. N Engl J Med 1997;337:1512–1522.
39. Schwartz LB, Yunginger JW, MillerJ, et al. Time course of appearanceand disappearance of human mastcell tryptase in the circulation afteranaphylaxis. J Clin Invest 1989;83:1551–1555.
40. Kaliner M, Dyer J, Merlin S, et al.Increased urine histamine and con-trast media reactions. Invest Radiol1984;19:116–118.
41. Grammer LC, Schafer M, BernsteinDI, et al. Prevention of chymopapainanaphylaxis by screening chemo-nucleolysis candidates with cutane-ous chymopapain testing. Clin Or-thop 1988;234:12–15.
42. Sogn DC, Evans R III, Shepherd GM,et al. Results of the National Instituteof Allergy and Infectious Diseasescollaborative clinical trial to test thepredictive value of skin testing withmajor and minor penicillin deriva-tives in hospitalized adults. Arch In-tern Med 1992;152:1025–1032.
43. Petz LD, Branch DR. Drug inducedimmune hemolytic anemia. In: Meth-ods in hematology. vol. 12, Immunehemolytic anemias. New York:Churchill Livingstone, 1985:47.
44. Barbaud A, Reichert-Penetrat S, Tre-chot P, et al. The use of skin testing inthe investigation of cutaneous ad-verse drug reactions. Br J Dermatol1998;139:49–58.
45. Nyfeler B, Pichler WJ. The lympho-cyte transformation test for the diag-nosis of drug allergy: sensitivity andspecificity. Clin Exp Allergy 1997;27(2):175–181.
46. Mauri-Hellweg D, Bettens F, MauriD, et al. Activation of drug-specificCD4� and CD8� cells in individualsallergic to sulfonamides, phenytoin,
and carbamazepine. J Immunol 1995;155(1):462–472.
47. Zanni MP, von Greyerz S, SchnyderB, et al. T cell reactions in patientsshowing adverse immune reactions todrugs. Inflam Res 1996;45(Suppl. 2):S79–S84.
48. Kimber I, Dearman RJ. Immune re-sponses to contact respiratory aller-gens. In: Immunotoxicology and im-munopharmacology. Dean JH, LusterMI, Munson AE, Kimber I, eds. NewYork: Raven Press, Ltd, 1994:663–679.
49. Sternlieb I, Bennett B, Scheinberg H.D-penicillamine induced Goodpas-ture’s syndrome in Wilson’s disease.Ann Intern Med 1975;82:673–676.
50. Kniker WT, Cochrane CG. The local-ization of circulating immune com-plexes in experimental serum sick-ness. J Exp Med 1968;127(1):119–136.
51. Kniker WT, Guerra FA, RichardsSEM. Prevention of immune complexdisease (serum sickness) by antago-nists of vasoactive amines. PediatrRes 1971;5:381.
52. Wanamacker WM, Wanamaker SJ,Celesta GG, et al. Thrombocytopeniaassociated with long-term levodopatherapy. JAMA 1976;235:2217–2219.
53. Stark BJ, Earl HS, Gross GN, et al.Acute and chronic desensitization ofpenicillin-allergic patients using oralpenicillin. J Allergy Clin Immunol1987;79:523–532.
54. Moreno JN, Poblete RB, Maggio C,et al. Rapid oral desensitization forsulfonamides in patients with the ac-quired immunodeficiency syndrome.Ann Allergy Asthma Immunol 1995;74:140–146.
55. Demoly P, Messaad D, Sahla H, et al.Six-hour trimethoprim-sulfamethoza-zole-graded challenge in HIV-in-fected patients. J Allergy Clin Immu-nol 1999;102:1033–1036.
56. Bush RK, Zoratti E, Taylor SL. Di-agnosis of sulfite and aspirin sensitiv-ity. Clin Rev Allergy 1995;8:159–178.
57. Purdy RH, Phillips DM, SummersRW. Desensitization for sulfasalazineskin rash. Ann Intern Med 1984;100:512–514.
58. Patterson R, Roberts M, GrammerLC. Insulin allergy: reevaluation aftertwo decades. Ann Allergy 1990;64:459–462.
59. Dykewicz MS, McGrath KG, Davi-
son R, et al. Identification of patientsat risk for anaphylaxis due to strep-tokinase. Arch Intern Med 1986;146:305–307.
61. Abramowicz D, Crusiaux A, Gold-man M. Anaphylactic shock after re-treatment with OKT3 monoclonal an-tibody. N Engl J Med 1992;327:736.
62. Dykewicz MS, Rosen ST, O’ConnellMM, et al. Plasma histamine but notanaphylatoxin levels correlate withgeneralized urticaria from infusionsof antilymphocyte monoclonal anti-bodies. J Lab Clin Med 1992;120:290.
63. Weiss ME, Nyhan D, Peng Z, et al.Association of protamine IgE andIgG antibodies with life-threateningreactions to intravenous protamine.N Engl J Med 1989;320:886–892.
64. Bernstein IL. Anaphylaxis to heparinsodium. JAMA 1956;161:1379–1381.
65. Anderson JA. Penicillin allergy. In:Lichtenstein LM, Fauci AS, eds. Cur-rent therapy in allergy, immunologyand rheumatology-3. Toronto: BCDelker, Inc, 1988:68–76.
66. Shepherd G. Allergy to beta-lactamantibiotics. In: Van Arsdel PP, ed.Immunology and Allergy Clinics ofNorth America. Philadelphia: WBSaunders, 1991:611.
67. Green GR, Rosenbloom AH, SweetLG. Evaluation of penicillinhypersensitivity: values of clinicalhistory and skin testing with penicil-lin-polylysine and penicillin G. A co-operative prospective study of thepenicillin study group of the Ameri-can Academy of Allergy. J AllergyClin Immunol 1977;60:339–345.
68. Gruchalla RS, Sullivan TS. In vivoand in vitro diagnosis of drug allergy.In: Van Arsdel PP, ed. Immunologyand Allergy Clinics of North Amer-ica. Philadelphia: WB Saunders,1991:595.
69. Solley GO, Gleich GJ, Van DellenRG. Penicillin allergy: clinical expe-riences with a battery of skin testreagents. J Allergy Clin Immunol1982;69:238–244.
70. Mendelson LM, Ressler C, Rosen JP,Selcow JE. Routine elective penicil-lin allergy skin testing in children andadolescents: study of sensitization. JAllergy Clin Immunol 1984;73:76–81.
696 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
71. Gadde J, Spence M, Wheeler R, et al.Clinical experience with penicillinskin testing in a large inner-city STDclinic [Abstract]. JAMA 1993;270:S134.
72. Shepherd GM. Clinical experienceusing only Pre-Pen and penicillin Gto detect penicillin allergy in hospi-talized adults. J Allergy Clin Immu-nol 1997;99:S134.
76. Ressler C, Neag PM, Mendelson LM.A liquid chromatographic study ofstability of the minor chromato-graphic determinants of penicillinallergy: a stable determinant mixtureskin test preparation. J Pharm Sci1985;74:448–454.
77. Solley GO, Gleich GJ, Van DellenRG. Penicillin allergy a clinical expe-rience with a battery of skin test re-agents. J Allergy Clin Immunol 1982;69:238–244.
79. Van Arsdel PP, Martonick GJ, John-son LE, et al. The value of skin test-ing for penicillin allergy diagnosis.West J Med 1986;144:311–314.
80. Warrington RJ, Simons FEL, HoHW, et al. Diagnosis of penicillin al-lergy by skin testing, the Manitobaexperience. Can Med Assoc J 1978;118:787–791.
81. Shapiro S, Slone D, Siskind D, et al.Drug rash with ampicillin and otherpenicillins. Lancet 1969;2:969–972.
82. Kerns DL, Shira JE, Go S, et al. Am-picillin rash in children: relationshipto penicillin allergy and infectiousmononucleosis. Am J Dis Child1973;125:187–190.
83. Dick H, Stone D, Shapiro S, et al.Excess of ampicillin rashes associ-ated with allopurinol or hyperurice-mia, a report from the Boston Collab-orative Drug Surveillance Program,Boston University Medical Center.N Engl J Med 1972;286:505–507.
84. Cameron SJ, Richmond J. Ampicillinhypersensitivity in lymphatic leuke-mia. Scot Med J 1974;16:425–427.
85. Saxon A, Adelman DC, Patel A, et al.Imipenem cross reactivity with peni-cillin in humans. J Allergy Clin Im-munol 1988;82:213–217.
86. Saxon A, Hassner A, Swabb EA, etal. Lack of cross-reactivity betweenaztreonam, a monobactam antibioticand penicillin in penicillin-allergicsubjects. J Infect Dis 1984;149:16–22.
87. Adkinson NF Jr. Immunogenicity andcross-allergenicity of aztreonam.Am J Med 1990;88:125–155;385–425.
88. Alvarez JS, Sacristan Del Castillo JA,Sampedro Garcia I, Alsar OrtizMJ. Immediate hypersensitivity to az-treonam. Lancet 1990;335:1094.
89. Silva-Dan F, McPhillips S, War-rington RJ. The frequency of skin testreactions to side chain penicillin de-terminants. J Allergy Clin Immunol1993;91:694–702.
90. Miranda A, Blanca M, Vega JM, etal. Cross-reactivity between a penicil-lin and a cephalosporin with the sameside chain. J Allergy Clin Immunol1996;98:671–677.
91. Blanca M, et al. New aspects of al-lergic reactions to beta-lactams:cross-reactions and unique specifici-ties. Clin Exp Allergy 1994;24:407–415.
92. Pumphrey RSH, Davis S. Under-reporting of antibiotic anaphylaxismay put patients at risk. Lancet 1999;353:1157.
93. Blanca M, Fernandez J, Miranada A,et al. Cross-reactivity between peni-cillin and cephalosporins: clinical andimmunological studies. J AllergyClin Immunol 1989;83:381–385.
94. Anne S, Reisman RE. Risk of admin-istering cephalosporin antibiotics topatients with histories of penicillinallergy. Ann Allergy Asthma Immu-nol 1995;74:167–170.
95. Shepherd GM, Burton DA. Adminis-tration of cephalosporin antibiotics topatients with a history to penicillin. JAllergy Clin Immunol 1993;91:262.
96. Carr A, Cooper DA, Penny R. Aller-gic manifestations of human immu-nodeficiency virus (HIV) infection.J Clin Immunol 1991;11:55–64.
97. DeSwarte RD. Drug allergies. In:Patterson R, et al, eds. Allergicdiseases: diagnosis and management,
4th ed. Philadelphia: JB LippincottCo., 1993:395.
98. Finegold I. Oral desensitization to tri-methoprim-sulfamethoxazole in a pa-tient with AIDS. J Allergy Clin Im-munol 1986;78:905–908.
99. Sehai J, Healy DP, Garris R, et al.Influence of antihistamine pretreat-ment on vancomycin-induced redman syndrome. J Infect Dis 1989;160:876–881.
100. Anne S, Middleton E Jr, Reisman RE.Vancomycin anaphylaxis and suc-cessful desensitization. Ann Allergy1994;73:402–404.
101. Earl HS, Sullivan TJ. Acute desensi-tization of a patient with cystic fibro-sis allergic to both beta-lactam andaminoglycoside antibiotics. J AllergyClin Immunol 1987;79:477–483.
102. Landor M, Lashinsky A, Waxman J.Quinolone allergy? Ann AllergyAsthma Immunol 1996;77:273–276.
103. Deamer RL, Prichare JG, LomanGJ. Hypersensitivity and anaphylac-toid reactions to ciprofloxacin. AnnPharmacother 1992;26:1081–1084.
104. Heine H. Cutaneous adverse reactionto ciprofloxacin: demonstration ofspecific lymphocyte proliferation andcross-reactivity to ofloxacin in vitro.Acta Dermato-Venereologica 1997;77(4):285–186.
105. Weiner M, Bernstein IL. In: AdverseReactions to Drug FormulationAgents, A Handbook of Excipients.New York: Marcel Dekker, Inc.,1989:296–312.
116. Olson CL. Blistering disorders. Post-grad Med 1994;96:53–64.
117. Roujeau J-C, Kelly JP, Naldi L, et al.Medication use and the risk ofStevens-Johnson syndrome or toxicepidermal necrolysis. N Engl J Med1995;333:1600–1607.
118. Cheriyan S, Patterson R, GreenbergerPA, et al. The outcome of Stevens-Johnson syndrome treated with corti-costeroids. Allergy Proced 1995;16:151–155.
119. Fine JD. Management of acquiredbullous skin diseases. N Engl J Med1995;333:1475–1484.
120. Becker DS. Toxic epidermal necroly-sis. Lancet 1998;351:1417–1420.
121. Viard I, Wehrti P, Bullani R, et al.Inhibition of toxic epidermal necroly-sis by blockage of CD95 with humanintravenous immunoglobulin. Sci-ence 1998;282:490–493.
122. Herbert AA, Syman ES, Levy ML.Serum sickness-like reactions fromcefaclor in children. J Am Acad Der-matol 1991;25:805–808.
123. Hyslop D. Cefaclor safety profile: aten year review. Clin Ther 1988;11:83–94.
124. Kearns GL, Wheeler GJ, ChildressSH, Lefzig LG. Serum sickness reac-tions to cefaclor: Role of hepatic me-tabolism and individual susceptibil-ity. J Pediatr 1994;125:805–811.
125. Weiss RB, Bruno S. Hypersensitivityreactions to cancer chemotherapeuticagents. Ann Intern Med 1981;94:66–72.
130. Cooper JAD, White DA, MatthayRA. Drug-induced pulmonary dis-ease. Part 1. Cytotoxic drugs. AmRev Respir Dis 1986;133:321–340,and Part 2. Noncytotoxic drugs 1986;133:526–534.
131. Alarcon GA, Kremer JM, MacalusoM, et al. Risk factors for methotrex-ate-induced lung injury in patientswith rheumatoid arthritis. Ann InternMed 1997;127:356–364.
132. Greenberger PA. Plasma anaphylaxisand immediate type reactions. In:Rossi EC, Simon TL, Moss GS, eds.Principles of transfusion medicine.Baltimore: Williams & Wilkins,1991:635.
133. Burks AW, Sampson HA, BuckleyRH. Anaphylactic reactions aftergamma globulin administration in pa-tients with hypogammaglobulinemia:detection of IgE antibodies to IgA.N Engl J Med 1986;314:560–564.
134. Lederman HM, Roifman CM, Lavi S,Gelfand EW. Corticosteroids for pre-vention of adverse reaction to intra-venous immune serum globulin infu-sions in hypogammaglobulinemicpatients. Am J Med 1986;81:443–446.
135. Ring J, Messmer K. Incidence andseverity of anaphylactoid reactions tocolloid volume substitutes. Lancet1977;1:466–469.
136. Levy JH, Schwieger IM, Zaidan JR,et al. Evaluation of patients at risk forprotamine reactions. J Thorac Cardio-vasc Surg 1989;98:200–204.
137. Vincent GM, Janowski M, MenloveR. Protamine allergy reactions duringcardiac catheterization and cardiacsurgery: risk in patients taking prota-mine-insulin preparations. CathetCardiovasc Diagn 1991;23:164–168.
138. Tobin MC, Karns K, Anselmino LM,Thomas LL. Potentiation of humanbasophil histamine release byprotamine: a new role for a polyca-tion recognition site. Mol Immunol1986;23:245–253.
142. Warkentin TE, Levine MN, Hirsh J,et al. Heparin-induced thrombocyto-penia in patients treated with low-molecular-weight heparin or unfrac-tionated heparin. N Engl J Med 1995;332:1330–1335.
143. Moscicki RA, Sockin SM, CorselloBF, et al. Anaphylaxis during induc-tion of general anesthesia: subsequentevaluation and management. J Al-lergy Clin Immunol 1990;86:325–332.
144. Vervloet D. Allergy to muscle relax-ants and related compounds. Clin Al-lergy 1985;15:501–508.
145. Moss J. Muscle relaxants and hista-mine release. Acta AnaesthesiolScand 1995;106:7–12.
146. Fisher MM, Munro I. Life-threaten-ing anaphylactoid reactions to musclerelaxants. Anesthesiol Analg 1983;62:559–564.
147. Baldo BA, Fisher MM. Detection ofserum IgE antibodies that react withalcuronium and tubocurarine afterlife-threatening reactions to musclerelaxant drugs. Anaesthesiol Inten-sive Care 1983;11:194–197.
148. Gall H, Kaufmann R, Kalveram CM.Adverse reactions to localanesthetics: analysis of 197 cases. JAllergy Clin Immunol 1996;97:933–937.
149. Schatz M. Skin testing and incremen-tal challenge in the evaluation of ad-verse reactions to local anesthetics. JAllergy Clin Immunol 1984;74:606–616.
150. deShazo RD, Nelson HS. An ap-proach to the patient with a history oflocal anesthetic hypersensitivity: ex-perience with 90 patients. J AllergyClin Immunol 1979;63:387–394.
151. Weiner M, Bernstein IL. Adverse re-actions to drug formulation agents, ahandbook of excipients. New York:Marcel Dekker, Inc, 1989:20–22.
152. Fisher MM. Intradermal testing in thediagnosis of acute anaphylaxis duringanesthesia-results of five years expe-
698 ANNALS OF ALLERGY, ASTHMA, & IMMUNOLOGY
rience. Anaesthesia and IntensiveCare 1979;7:58.
153. Harle DG, Baldo BA, Coroneos NJ,Fisher MM. Anaphylaxis followingadministration of Papaveretum. CaseReport: Implication of IgE antibodiesthat react with morphine and codeine,and identification of an allergenic de-terminant. Anesthesiology 1989;71:489–494.
154. Coleman WP, Ochsner SF, WatsonBE. Allergic reactions in 10,000 con-secutive intravenous urographies.Southern Med J 1964;57:1401–1404.
155. Fischel HW, Doust VL. An evalua-tion of pretesting in the problem ofserious and fatal reactions to excre-tory urography. Radiology 1972;103:497–501.
156. Schatz M, Patterson R, O’Rourke J,et al. The administration of radio-graphic contrast media to patientswith history of a previous reaction. JAllergy Clin Immunol 1975;55:358–366.
157. Lang DM, et al. Elevated risk of ana-phylactoid reactions from radio-graphic contrast media is associatedwith both beta-blocker exposure andcardiovascular disorders. Arch InternMed 1993;153:2033–2040.
158. Enricht T, Chau-Lim A, Duda E, LimDT. The role of a documented aller-gic profile as a risk factor for radio-graphic contrast media reaction. AnnAllergy 1989;62:302–305.
159. Lang DM, Alpern MB, VisintainerPF, Smith ST. Increased risk for ana-phylactoid reaction from contrast me-dia in patients on beta-adrenergicblockers or with asthma. Ann InternMed 1991;115:270–276.
160. Siegle RL, Halvorsen RA, Dillion J,et al. The use of iohexol in patientswith previous reactions to ionic con-trast material, a multicenter clinicaltrial. Invest Radiol 1991;26:411–416.
161. Greenberger PA, Patterson R. Theprevention of immediate generalizedreactions to radiocontrast media inhigh-risk patients. J Allergy Clin Im-munol 1991;87:867–872.
162. Monaghan MS, Glasco G, St. John G,et al. Safe administration of iron dex-tran in a patient who reacted to thetest dose. South Med J 1994;87:1010–1012.
163. Stevenson DD, Simon RA. Sensitiv-ity to aspirin and nonsteroidal anti-inflammatory drugs. In: Middleton EJr, Reed CE, Ellis EF, et al, eds.
Allergy: Principles and Practice, 4thed. St Louis: CV Mosby Co, 1993:1747.
164. Szezeklik A, Stevenson DD. Aspirin-induced asthma: Advances in patho-genesis and management. J AllergyClin Immunol 1999;104:5–13.
166. Minden P, Farr RS. Human antibod-ies against acetylsalicyclic acid-altered human serum albumin. Arthri-tis Rheumatol 1967;10:299–300.
167. Amos HE, Wilson DV, Taussig MJ,Carlton SJ. Hypersensitivity reactionsto acetylsalicylic acid. I. Detection ofantibodies in human sera using ace-tylsalicylic acid attached to proteinsthrough the carboxyl group. Clin ExpImmunol 1971;8:563–572.
168. deWeck AL. Immunological effectsof aspirin anhydride, a contaminantof commercial acetylsalicyclic acidpreparations. Int Arch Allergy ApplImmunol 1971;41:393–418.
169. Stevenson DD. Aspirin and non-steroidal anti-inflammatory drugs.Immunol Allergy Clin North Am1995;15:529–552.
170. Christie PE, Smith SM, Lee TH. Thepotent and selective sulfidopeptideleukotriene antagonist, SK&F104353, inhibits aspirin-inducedasthma. Am Rev Respir Dis 1991;144:957–958.
171. Israel E, Fischer AR, Rosenberg MA,et al. The pivotal role of 5-lipoxygen-ase products in the reaction of aspi-rin-sensitive asthmatics to aspirin.Am Rev Respir Dis 1993;148:1447–1451.
172. Bush RK, Zoratti E, Taylor SL. Di-agnosis of sulfite and aspirin sensitiv-ity. Clin Rev Allergy 1990;8:159–178.
174. Bernstein IL, Gallagher JS, JohnsonH, et al. Immunologic and nonimmu-nologic factors in adverse reactions totartrazine. In: Asher IM, eds. Pro-ceedings, 4th FDA Science Symppo-sium, U.S. Govt. Printing Office,Washington, DC, 1980:258–260.
175. Spector SL, Wangaard CH, Farr RS.Aspirin and concomitant idiosyncra-sies in adult asthmatic patients. J Al-
lergy Clin Immunol 1979;64:500–506.
176. Weber RW, Hoffman M, Raine DAJr, et al. Incidence of bronchocon-striction due to aspirin, azo dyes,non-azo dyes, and preservatives in apopulation of perennial asthmatics. JAllergy Clin Immunol 1979;64:32–37.
177. Stevenson DD, Simon RA, LumryWR, et al. Adverse reactions to tara-trazine. J Allergy Clin Immunol1986;78:182–191.
178. Zlotlow MJ, Settipane GA. Allergicpotential of food additives: A reportof a case of tartrazine sensitivitywithout aspirin intolerance. Am JClin Nutr 1977;30:1023–1025.
179. Mathison DA, Lumry WR, StevensonDD, et al. Aspirin in chronic urticariaand/or angioedema: studies of sensi-tivity and desensitization. J AllergyClin Immunol 1982;69:134.
180. Gibson GR. Enalapril-induced cough.Arch Intern Med 1989;149:2701–2703.
181. Brown NJ, Snowden M, Griffin MR.Recurrent angiotensin-converting en-zyme inhibitor-associated angio-edema. JAMA 1997;278:232–233.
182. Winning AJ, Hamilton RD, Guz A.Cough associated with captopril andenalapril. Br Med J 1987;294:1521–1523.
183. Coulter DM, Edwards IR. Cough as-sociated with captopril and enalapril.Br Med J 1987;296:1521–1523.
184. USP DI. 19th edition. Drug informa-tion for the health care profession.Englewood, CO: Micromedex, 1999:1883.
185. Weiner M, Bernstein IL. Adverse re-actions to drug formulation agents, Ahandbook of excipients. New York:Marcel Dekker, Inc, 1989:292–293;314–320.
186. Gunnison AF, Jaconsen DW. Sulfitesensitivity. A critical review. CritRev Toxicol 1987;17(3):185–214.
187. Jick H. Adverse reactions to tri-methoprim-sulfamethoxazole in hos-pitalized patients. Rev Infect Dis1982;4:426–428.
188. Gordin FM, Simon GL, Wofsy CB,Mills J. Adverse reactions to tri-methoprim-sulfamethoxazole in pa-tients with the acquired immunodefi-ciency syndrome. Ann Intern Med1984;100:495–499.
189. Kovacs JA, Hiementz JW, MacherAM, et al. Pneumocystis carinii
VOLUME 83, DECEMBER, 1999 699
pneumonia: A comparison betweenpatients with the acquired immunode-ficiency syndrome and patients withother immunodeficiencies. Ann In-tern Med 1984;100:663–671.
190. Wharton JM, Coleman DL, WofsyCB, et al. Trimethoprim-sulphame-thoxazole or pentamidine for Pneu-mocystis carinii pneumonia in the ac-quired immunodeficiency syndrome.Ann Intern Med 1986;105:37–44.
191. Greenberger PA, Patterson R. Man-agement of drug allergy in patientswith acquired immunodeficiencysyndrome. J Allergy Clin Immunol1987;79:484–488.
192. Carr A, Cooper DA, Penny R. Aller-gic manifestations of human immu-nodeficiency virus infection. J ClinImmunol 1991;11:55–64.
193. Lee BL, Safrin S. Interactions andtoxicities of drugs used in patientswith AIDS. Clin Infect Dis 1992;14:773–779.
195. Koopmans PP, van der Ven JAM,Vree TB, van der Meer JWM. Patho-genesis of hypersensitivity reactionsto drugs in patients with HIVinfection: allergic or toxic? AIDS1995;9:217–222.
196. Battegay M, Opravil M, Wuthrich B,Luthy R. Rash with amoxicillin cla-vulanate therapy in HIV-infected pa-tients. Lancet 1989;2:1100.
197. Okwera A, Whalen C, Byekwaso F.Randomized trial of thiacetazone andrifampicin-containing regimens forpulmonary tuberculosis in HIV-infected Ugandans. The Makere Uni-versity-Case Western Reserve Uni-versity Research Collaboration.Lancet 1994;344:1323–1328.
198. Carr A, Swanson C, Penny R, Cooper
DA. Clinical and laboratory markersof hypersensitivity to trimethoprim-sulphamethoxazole in patients withPneumocystis carinii pneumonia andAIDS. J Infect Dis 1993;167:180–185.
199. Rieder MJ, Shear NH, Kanee A, et al.Prominence of slow acetylator phe-notype among patients with sulfon-amide hypersensitivity reactions. ClinPharmacol Ther 1991;49:13–17.
200. Carr A, Penny R, Cooper DA. Effi-cacy and safety of rechallenge withlow-dose trimethoprim-sulphame-thoxazole in previously hypersensi-tive HIV-infected patients. AIDS1993;7:65–71.
201. Carr A, Tindall B, Penny R, CooperDA. In vitro cytotoxicity as a markerof hypersensitivity to sulphamethox-azole in patients with HIV. Clin ExpImmunol 1993;94:21–25.
202. Lee BL, Wong D, Benowitz NL, Sul-lam PM. Altered patterns of drug me-tabolism in patients with acquired im-munodeficiency syndrome. ClinPharmacol Ther 1993;53:529–535.
203. Carr A, Gross AS, Hoskins JM, et al.Acetylation phenotype and cutaneoushypersensitivity to trimethoprim-sulphamethoxazole in HIV-infectedpatients. AIDS 1994;8:333–337.
204. Rieder MJ, Krause R, Bird IA, Deka-ban GA. Toxicity of sulfonamide-reactive metabolites in HIV-infected,HTLV-infected, and noninfectedcells. J Acq Imm Def Syn Hum Retro1995;8:134–140.
205. Daftarian MP, Filion LG, CameronW, et al. Immune response to sulfa-methoxazole in patients with AIDS.Clin Diagn Lab Immunol 1995;2:199–204.
206. Finegold I. Oral desensitization toTMP-SMX in a patient with acquiredimmunodeficiency syndrome. J Al-lergy Clin Immunol 1986;78:905–908.
207. White MV, Haddad ZH, Brunner E,Sainz C. Desensitization to tri-methoprim sulfamethoxazole in pa-tients with acquired immune defi-ciency syndrome and Pneumocystispneumonia. Ann Allergy 1989;62:177–179.
208. Absar N, Daneshvar H, Beall G. De-sensitization to TMP-SMX in HIV-infected patients. J Allergy Clin Im-munol 1994;93:1001–1005.
209. Moreno JN, Problete RB, Maggio C,et al. Rapid oral desensitization forsulfonamides in patients with the ac-quired immunodeficiency syndrome.Ann Allergy Asthma Immunol 1995;74:140–146.
210. Tenant-Flowers M, Boyle MJ, CareyD, et al. Sulphadiazine desensitiza-tion in patients with AIDS and cere-bral toxoplasmosis. AIDS 1991;5:311–315.
211. Henry RE, Wegmann JA, Hartle JE,Christopher GW. Successful oral acy-clovir desensitization. Ann Allergy1993;70:386–388.
212. Carr A, Penny R, Cooper DA. Al-lergy and desensitization to zidovu-dine in patients with acquired immu-nodeficiency syndrome (AIDS). JAllergy Clin Immunol 1993;91:683–685.
213. Kennedy CA, Goetz MB, MathisenGE. Ciprofloxacin-induced anaphy-lactoid reactions in patients infectedwith the human immunodeficiencyvirus. West J Med 1990;153:563–564.
214. Havlir D, Torriani F, Dube M. Uve-itis associated with rifabutin prophy-laxis. Ann Intern Med 1994;121:510–512.
215. Gruchalla RS, Pesenko RD, Do TT,Skiest DJ. Sulfonamide-induced reac-tions in desensitized patients withAIDS—role of covalent protein hap-tenation by sulfamethoxazole. J Al-lergy Clin Immunol 1998;101:371–378.