Invited Article—General Otolaryngology Evidence-Based Medicine in Otolaryngology, Part 5: Patient Decision Aids Otolaryngology– Head and Neck Surgery 2015, Vol. 153(3) 357–363 Ó American Academy of Otolaryngology—Head and Neck Surgery Foundation 2015 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/0194599815592366 http://otojournal.org Melissa A. Pynnonen, MD, MSc 1 , Gregory W. Randolph, MD 2 , and Jennifer J. Shin, MD, SM 2 Sponsorships or competing interests that may be relevant to content are dis- closed at the end of this article. Abstract Modern medical decision making is a complex task requiring collaboration between patients and physicians. Related clini- cal evidence may delineate a clearly favorable path, but in other instances, uncertainty remains. Even in these circum- stances, however, there are techniques that optimize deci- sion making by blending existing evidence with individual patient values in the context of physician counseling. This installment of ‘‘Evidence-Based Medicine in Otolaryngology’’ focuses on the crucial issue of how practitioners may approach clinical situations where the data do not delineate a single irrefutable path. We describe decision aids—tools that can educate patients about data related to complex clinical decisions. We review their definition, quality stan- dards, patient interface, benefits, and limitations. We also discuss the related concept of option grids and the role of decision aids in evidence-based practice. Keywords decision aid, physician-patient relations, decision making Received April 11, 2015; revised May 27, 2015; accepted June 1, 2015. I n this series entitled ‘‘Evidence-Based Medicine in Otolaryngology,’’ we consider what constitutes evidence- based practice, the state of the literature in our field, and specific numeric analyses that may help facilitate everyday deci- sions. 1-4 As we continue to focus on the application of clinical evidence in daily practice, we recognize that there are often inherent limitations (and sometimes contradictions) in published studies. With that in mind, this installment focuses on the cru- cial issue of how practitioners may handle clinical situations where the data do not delineate a single irrefutable path. Even in these circumstances, there are techniques that optimize deci- sion making and blend existing evidence with individual patient values in the context of physician counseling. Much of medical practice centers on decisions: decisions regarding diagnostic testing, medications, and surgery. Making such decisions involves 2 steps: (1) understanding the possible choices, including the risks and benefits of each, and (2) asses- sing each choice relative to the patients’ intrinsic preferences. Some decisions are straightforward to the point of being reflexive, while others may lead to near equipoise, with more than 1 viable option. Decision aids are tools that have been developed to facil- itate this process, and they can be utilized to educate patients regarding the data related to complex clinical deci- sions. While they are in the incipient phase in otolaryngol- ogy, they have been utilized in other medical venues, and they are expected to facilitate evolution of data-centered and guideline-recommended practice in modern medical practice. This fifth installment of ‘‘Evidence-Based Medicine in Otolaryngology’’ describes decision aids, the types of health care decisions that they can best facilitate, related quality standards, and their benefits and limitations. What Is a Decision Aid? A decision aid is a tool designed to help patients make an evidence-based health care decision when multiple choices exist. This tool can help patients make testing or treatment decisions. 5 A decision aid displays information on choices and potential outcomes, based on the strongest, most rele- vant published data. 6,7 They have been developed as book- lets and brochures, as well as electronic and Internet-based media. They complement the physician’s role and are used in conjunction with physician counseling. There is high- quality evidence indicating that decision aids improve patient knowledge and reduce patient decision conflict. 5 A decision aid consists of 3 basic components. First, it describes the nature of the health care condition and describes clearly the different options available for manage- ment of that condition. Second, a decision aid provides 1 Department of Otolaryngology, University of Michigan Health System, Ann Arbor, Michigan, USA 2 Department of Otolaryngology, Harvard Medical School, Boston, Massachusetts, USA Corresponding Author: Jennifer J. Shin, MD, SM, Department of Otolaryngology, Harvard Medical School, 45 Francis Street, Boston, MA 02115, USA. Email: [email protected]at SOCIEDADE BRASILEIRA DE CIRUR on September 2, 2015 oto.sagepub.com Downloaded from
Transcript
Invited Article—General Otolaryngology
Evidence-Based Medicine inOtolaryngology, Part 5: PatientDecision Aids
Otolaryngology–Head and Neck Surgery2015, Vol. 153(3) 357–363� American Academy ofOtolaryngology—Head and NeckSurgery Foundation 2015Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/0194599815592366http://otojournal.org
Melissa A. Pynnonen, MD, MSc1, Gregory W. Randolph, MD2, andJennifer J. Shin, MD, SM2
Sponsorships or competing interests that may be relevant to content are dis-
closed at the end of this article.
Abstract
Modern medical decision making is a complex task requiringcollaboration between patients and physicians. Related clini-cal evidence may delineate a clearly favorable path, but inother instances, uncertainty remains. Even in these circum-stances, however, there are techniques that optimize deci-sion making by blending existing evidence with individualpatient values in the context of physician counseling. Thisinstallment of ‘‘Evidence-Based Medicine in Otolaryngology’’focuses on the crucial issue of how practitioners mayapproach clinical situations where the data do not delineatea single irrefutable path. We describe decision aids—toolsthat can educate patients about data related to complexclinical decisions. We review their definition, quality stan-dards, patient interface, benefits, and limitations. We alsodiscuss the related concept of option grids and the role ofdecision aids in evidence-based practice.
Keywords
decision aid, physician-patient relations, decision making
Received April 11, 2015; revised May 27, 2015; accepted June 1, 2015.
In this series entitled ‘‘Evidence-Based Medicine in
Otolaryngology,’’ we consider what constitutes evidence-
based practice, the state of the literature in our field, and
specific numeric analyses that may help facilitate everyday deci-
sions.1-4 As we continue to focus on the application of clinical
evidence in daily practice, we recognize that there are often
inherent limitations (and sometimes contradictions) in published
studies. With that in mind, this installment focuses on the cru-
cial issue of how practitioners may handle clinical situations
where the data do not delineate a single irrefutable path. Even
in these circumstances, there are techniques that optimize deci-
sion making and blend existing evidence with individual patient
values in the context of physician counseling.
Much of medical practice centers on decisions: decisions
regarding diagnostic testing, medications, and surgery. Making
such decisions involves 2 steps: (1) understanding the possible
choices, including the risks and benefits of each, and (2) asses-
sing each choice relative to the patients’ intrinsic preferences.
Some decisions are straightforward to the point of being
reflexive, while others may lead to near equipoise, with more
than 1 viable option.
Decision aids are tools that have been developed to facil-
itate this process, and they can be utilized to educate
patients regarding the data related to complex clinical deci-
sions. While they are in the incipient phase in otolaryngol-
ogy, they have been utilized in other medical venues, and
they are expected to facilitate evolution of data-centered and
guideline-recommended practice in modern medical practice.
This fifth installment of ‘‘Evidence-Based Medicine in
Otolaryngology’’ describes decision aids, the types of health
care decisions that they can best facilitate, related quality
standards, and their benefits and limitations.
What Is a Decision Aid?
A decision aid is a tool designed to help patients make an
evidence-based health care decision when multiple choices
exist. This tool can help patients make testing or treatment
decisions.5 A decision aid displays information on choices
and potential outcomes, based on the strongest, most rele-
vant published data.6,7 They have been developed as book-
lets and brochures, as well as electronic and Internet-based
media. They complement the physician’s role and are used
in conjunction with physician counseling. There is high-
quality evidence indicating that decision aids improve
patient knowledge and reduce patient decision conflict.5
A decision aid consists of 3 basic components. First, it
describes the nature of the health care condition and
describes clearly the different options available for manage-
ment of that condition. Second, a decision aid provides
1Department of Otolaryngology, University of Michigan Health System, Ann
Arbor, Michigan, USA2Department of Otolaryngology, Harvard Medical School, Boston,
Massachusetts, USA
Corresponding Author:
Jennifer J. Shin, MD, SM, Department of Otolaryngology, Harvard Medical
implementation of evidence-based medicine requires that a
physician not only access, interpret, and convey medical evi-
dence to the patient, taking into account the unique clinical
circumstances that may affect the risk/benefit profile, but also
invoke the patient’s personal values related to health care.
Putting all of these components together in a 15-minute visit
can be a lot to ask of a busy physician. Also, understanding
personalized risk statistics can be difficult for physicians and
patients alike. Assessments of mathematical skills among
Americans show average numeracy scores that reflect diffi-
culty in interpreting proportions and graphs.22 Even physi-
cians may have limited understanding of terms such as odds
ratio and 95% confidence interval.2,23-26
A decision aid can facilitate this cognitively challenging
discussion by providing a formal structure to consider each
treatment choice at hand (including the option of no treat-
ment). The tool provides a concrete means to incorporate
patient preferences with medical evidence and physician
recommendations. Finally, the decision aid gives the patient
the opportunity to directly interface with the data, relieving
the clinician of being the sole source of information. A deci-
sion aid or other support tool may allow a patient the extra
time needed for thoughtful deliberation and alleviate some
of the time pressure ubiquitous in today’s practice
environment.7
What Are the Benefits of Decision Aids?
There is a host of evidence that patient educational interven-
tions such as decision aids can increase knowledge and pro-
vide more accurate risk perceptions.5,27 Decision aids are
reported to ‘‘increase knowledge, reduce decisional conflict,
cause greater satisfaction with decision-making, support
more realistic expectations, achieve a greater likelihood of
being able to make a decision, result in an increased associ-
ation between patient values and decisions, support patient
participation and enhance communication between physi-
cians, patients, and their relatives.’’6 One meta-analysis
quantified this benefit, demonstrating a significant improve-
ment in knowledge after decision aid use (pooled mean dif-
ference, 13.3%; 95% confidence interval, 11.1-15.5) and a
higher proportion of patients making a decision congruent
with their values (relative risk, 1.51; 95% confidence inter-
val, 1.17-1.96).5
Decision aids purportedly improve patient engagement
because they are designed with the patient in mind. They
are typically written in plain English, with few assumptions
regarding a patient’s underlying health literacy. Decision
aids often present statistics in multiple formats, using con-
sistent language and absolute risk statistics. For example,
‘‘Without treatment, 2 in 100 people will have the cancer
recur. With treatment, 1 in 100 people will have the cancer
recur.’’ This is much easier for patients to understand when
compared with descriptions of relative risk reduction, such
as ‘‘fifty percent lower risk of cancer recurrence.’’ Based on
studies demonstrating the limited mathematical and statisti-
cal sophistication in the average clinical environment, it is
imperative that a decision aid convey numeric risk informa-
tion to patients in a manner that can be clearly and reliably
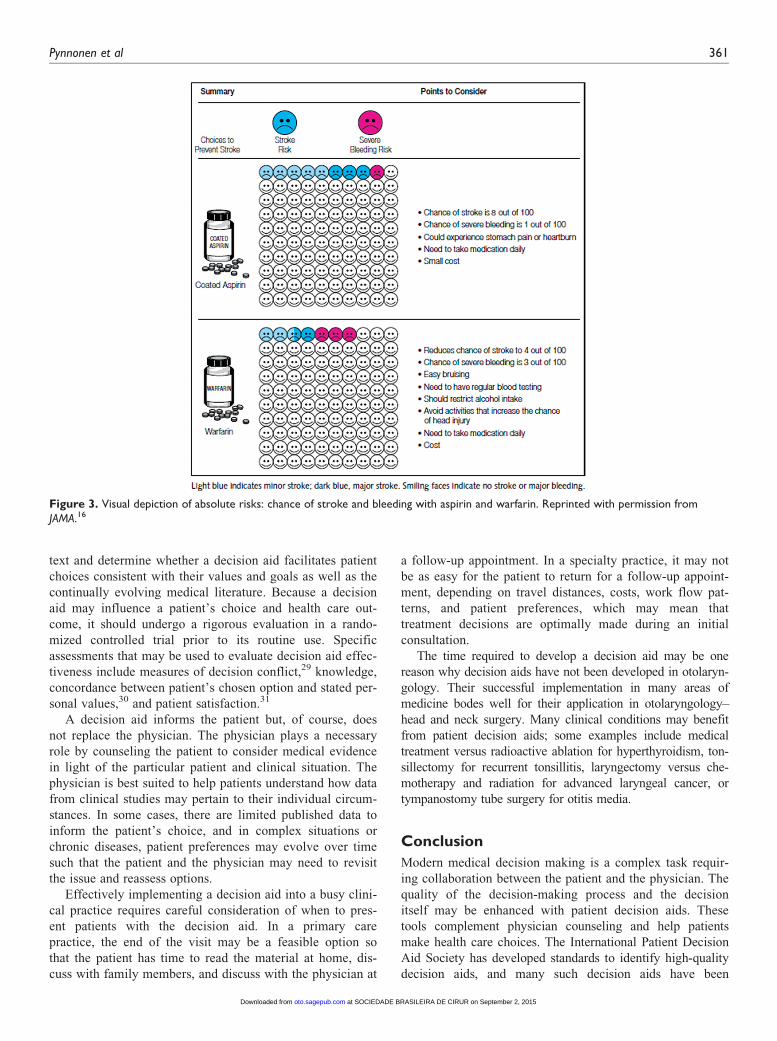
understood.28 A decision aid also often uses figures such as
a pictogram with 99 happy faces and 1 sad face to depict a
1% risk of a bad outcome (Figure 3).
What Are the Limitations of Decision Aids?
Decision aid development is not trivial; it requires a signifi-
cant time and financial investment to create, test, and refine
the content. Although the tool is based on published medical
evidence, the scientific information must be revised and for-
matted to ensure that patients of varying educational and lit-
eracy levels can read and comprehend it and that the
literature represented is selected without bias. This may
often include figures to convey basic health information or
health statistics. Procedures to ensure accuracy of patient
understanding and ease of usability of decision-related
materials are time-consuming. Further contributing to the
burden of development is the need to iteratively revise the
Table 1. Domains of the IPDAS Quality Framework for PatientDecision Aids.12
Development Process Decision Aid Content Evaluation
Systematic development
process
Options
delineated
Establish
effectiveness
Discloses conflict
of interest
Probabilities presented
Evidence-based
information
Values clarified
Patient story usage
Guiding/coaching
Balanced presentation
of options
Uses plain language
Internet access
Abbreviation: IPDAS, International Patient Decision Aid Society.
Figure 2. Implicit and explicit approaches to values clarificationexercises. The example demonstrates these approaches relative tooptions for treatment of otitis media with effusion.
360 Otolaryngology–Head and Neck Surgery 153(3)
at SOCIEDADE BRASILEIRA DE CIRUR on September 2, 2015oto.sagepub.comDownloaded from