Page 1
INFECTION CONTROL
&PREVENTION
A PEDIATRICIAN’S GUIDE
PEER-REVIEWED FEATURE
Deciphering bacterialmeningitis
“When can my childreturn to school?”
HOSPITAL ZONE
Children’s HospitalLos Angeles’ novel facial cleft care
ContemporaryPediatrics.comExpert Clinical Advice for Today’s Pediatrician ContemporaryPediatrics.comExpert Clinical Advice for Today’s Pediatrician
JULY 2016VOL. 33 | NO. 07Contemporary
PEDIATRICS
CO
NT
EM
PO
RA
RY
PE
DIA
TR
ICS
JU
LY 2
01
6 V
OL. 3
3 N
O. 0
7
IN
FECTIO
N C
ON
TRO
L & PR
EVEN
TION
D
ECIPH
ERIN
G B
AC
TERIA
L MEN
ING
ITIS
CH
ILDR
EN'S
HO
SPITA
L LOS
AN
GELES
' NO
VEL FA
CIA
L CLEFT C
AR
E
EYE ON
WASHINGTON
FDA Seeks to
Defi ne “Healthy”
Page 2
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 64
editorial advisory boardContemporaryPEDIATRICS
physician contributing editors
founding editor
Frank A Oski, MD
OUR MISSION Office- and hospital-based pediatricians and nurse practitioners use Contemporary Pediatrics’ timely, trusted, and
practical information to enhance their day-to-day care of children. We advance pediatric providers’ professional development through
in-depth, peer-reviewed clinical and practice management articles, case studies, and news and trends coverage.
contentSARA MICHAELVP, Content & Strategy
TERESA MCNULTYGroup Content Director
CATHERINE M. RADWAN Content Managing Editor440-891-2636 / [email protected]
MIRANDA HESTERContent Specialist
KATHRYN FOXHALL & MARIAN FREEDMANContributing Editors
NANCY BITTEKERDirector, Design and Digital Production
NICOLE DAVIS-SLOCUMArt Director
publishing & salesGEORGIANN DECENZOEVP, Managing Director
AVIVA BELSKYGroup Publisher732-346-3044 / [email protected]
DIANE CARPENTERIAssociate Publisher732-346-3092 / [email protected]
JOANNA SHIPPOLIAcct Manager, Recruitment440-891-2615 / [email protected]
RENEE SCHUSTERList Acct Executive440-891-2613 / [email protected]
MAUREEN CANNONPermissions440-891-2642/ [email protected]
REPRINTS [email protected]
877-652-5295 ext 121
Outside US, UK, direct dial:
281-419-5725 ext 121
CUSTOMER SERVICE888.527.7008
Scott A Shipman, MD, MPH Director of Primary Care Initiatives
and Workforce Analysis,
Association of American Medical
Colleges, Washington, DC, and
Assistant Professor of Pediatrics,
Dartmouth Institute for Health
Policy and Clinical Practice, Geisel
School of Medicine at Dartmouth,
Lebanon, New Hampshire
Michael G Burke, MDSection Editor for Journal
Club, Chairman, Department of
Pediatrics, Saint Agnes Hospital,
Baltimore, Maryland
Bernard A Cohen, MDSection Editor for Dermcase,
Professor of Pediatrics and
Dermatology, Johns Hopkins
University School of Medicine,
Baltimore, Maryland
Michael S Jellinek, MD Professor of Psychiatry and of
Pediatrics, Harvard Medical School,
Boston, and Chief Executive
Officer, Community Network,
Lahey Health System, Burlington,
Massachusetts
Jane A Oski, MD, MPH Department of Pediatrics, Tuba City
Regional Health Care Corporation,
Tuba City, Arizona
W Christopher Golden, MDAssistant Professor of Pediatrics
(Neonatology), Johns Hopkins
University School of Medicine, and
Medical Director, Full Term Nursery,
Johns Hopkins Hospital, Baltimore,
Maryland
Steven M Selbst, MD Professor of Pediatrics, Vice Chair
for Education, Director, Pediatric
Residency Program, Sidney Kimmel
Medical College at Thomas
Jefferson University, Philadelphia,
Pennsylvania, and Attending
Physician, Pediatric Emergency
Medicine, Nemours/Alfred I duPont
Hospital for Children, Wilmington,
Delaware
Harlan R Gephart, MD Clinical Professor of Pediatrics,
University of Washington School of
Medicine, Seattle, Washington
Andrew J Schuman, MDSection Editor for Peds v2.0,
Clinical Assistant Professor
of Pediatrics, Geisel School of
Medicine at Dartmouth, Lebanon,
New Hampshire
Gary L Freed, MD, MPH Director, Division of General
Pediatrics, Professor of Pediatrics
and Health Management and
Policy, and Director, Child Health
Evaluation and Research (CHEAR)
Unit, University of Michigan Health
Systems, Ann Arbor, Michigan
Donna Hallas, PhD, CPNP, PNP-BC, PMHS, FAANPClinical Professor, New York
University (NYU) College of
Nursing, and Coordinator, Pediatric
Nurse Practitioner Program, New
York, New York
Page 3
Trust Eucerin. Over 100 years committed
to skin science.Reference: 1. Weber TM, Samarin F, Babcock MJ, Filbry A, Rippke F. Steroid-free over-the-counter eczema skin care formulations reduce risk of flare, prolong time to flare, and reduce eczema symptoms in pediatric subjects with atopic dermatitis. J Drugs Dermatol. 2015;14(5):478-485.
Eucerin Eczema Relief Body Creme relieves dry,
itchy skin and provides hydration for patients
with eczema-prone skin1—in a light, fast-absorbing
daily formula
FLARE FREE AND LOVING ITEUCERIN® ECZEMA RELIEF BODY CREME HELPED
4 OUT OF 5 CHILDREN STAY FLARE FREE FOR 6 MONTHS1*
*Subjects applying daily Eucerin® Eczema Relief Body Creme demonstrated a statistically significant difference (P =0.006) in the prevention of eczema flares compared with control group subjects.1
©2016 Beiersdorf Inc.
SKIN PROTECTANT
Page 4
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 66
ContemporaryPEDIATRICS
13 puzzlerBOY WITH FEVER, COUGH, AND ORAL LESIONS
J David Sterns, MD; Riva Kamat, MD, FAAP
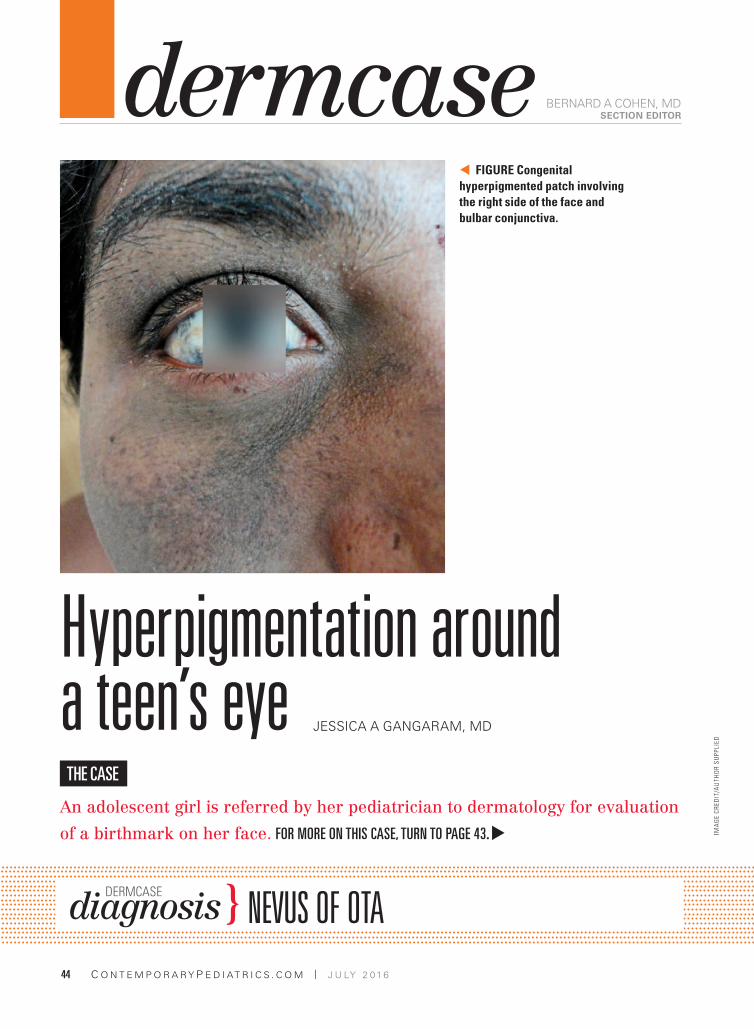
44 dermcaseHYPERPIGMENTATION AROUND A TEEN’S EYE
Jessica A Gangaram, MD
July 2016
VOL. 33 NO. 7
GE
TT
Y I
MA
GE
S/L
AR
S K
LOV
E
Contemporary Pediatrics (Print ISSN: 8750-0507, Digital ISSN: 2150-6345) is published monthly by UBM Medica, 131 W. 1st Street, Duluth, MN 55802. Subscription rates: one year $89, two years $150 in the United States & Possessions, $105 for one year, $189 for two years in Canada and Mexico; all other countries $105 for one year, $189 for two years. Single copies (prepaid only) $18 in the United States; $22 in Canada and Mexico, and $24 in all other countries. Include $6.50 per order plus $2.00 per additional copy for U.S. postage and handling. Periodicals postage paid at Duluth, MN 55806 and additional mailing offices. POSTMASTER: Please send address changes to Contemporary Pediatrics, PO Box 6083, Duluth, MN 55806-6083. Canadian GST number: R-124213133RT001. Publications Mail Agreement Number 40612608. Return Undeliverable Canadian Addresses to: IMEX Global Solutions, P. O. Box 25542, London, ON N6C 6B2, CANADA . Printed in the U.S.A.© 2016 UBM. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission
in writing from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or personal use of specific clients is granted by UBM for libraries and other users registered with the Copyright Clearance Center, 222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: [email protected] Medica provides certain customer contact data (such as customers’ names, addresses, phone numbers, and e-mail addresses) to third parties who wish to promote relevant products, services, and other opportunities that may be of interest to you. If you do not want UBM Medica to make your contact information available to third parties for marketing purposes, simply call toll-free 866-529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you in removing your name from UBM Medica’s lists. Outside the U.S., please phone 218-740-6477.Contemporary Pediatrics does not verify any claims or other information
appearing in any of the advertisements contained in the publication, and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.Contemporary Pediatrics welcomes unsolicited manuscripts for consideration. To assist the Editor in the safekeeping and return of submitted materials, authors must transmit manuscripts and their accessory parts (photographs, computer diskettes, permissions, etc.) to Contemporary Pediatrics by reputable overnight courier, certified or registered US Postal Service mail (including “return receipt requested” service), or messenger. Library Access Libraries offer online access to current and back issues of Contemporary Pediatrics through the EBSCO host databases. To subscribe, call toll-free 888-527-7008. Outside the U.S. call 218-740-6477.
Do you have a manuscript to submit
to Contemporary Pediatrics?
E-mail [email protected] for submission guidelines.
NEW VIDEOS AT CONTEMPORARYPEDIATRICS.COM
NEW to Contemporary Pediatrics! Check out our latest evidence-based Medical Minute videos from Bobby Lazzara, MD. This month? A nationally representative survey asks parents what they want to know about vaccines. PLUS! Dr. Lazzara explains the latest recommendations for pediatric dermatology conditions.
peer-reviewed feature14 Deciphering bacterial meningitisPediatricians need to understand not only how bacterial meningitis can be prevented in
children through vaccination, but also its risks, symptoms, workup, and treatment.
Pat F Bass III, MD, MS, MPH
clinical feature21 Infection control and prevention:
“When can my child return to school?”Teaching parents and educators about infection control practices can improve
prevention and decrease risk of disease transmission to help keep kids in school.
Pat F Bass III, MD, MS, MPH
the hospital zone32 CLEFT LIP AND
PALATE: TEAM APPROACH
TO TREATMENTA multidisciplinary center for children
with facial clefts ensures that patients
treated by its team of specialty
providers emerge with little or no
evidence of their cleft deformities.
Lisette Hilton
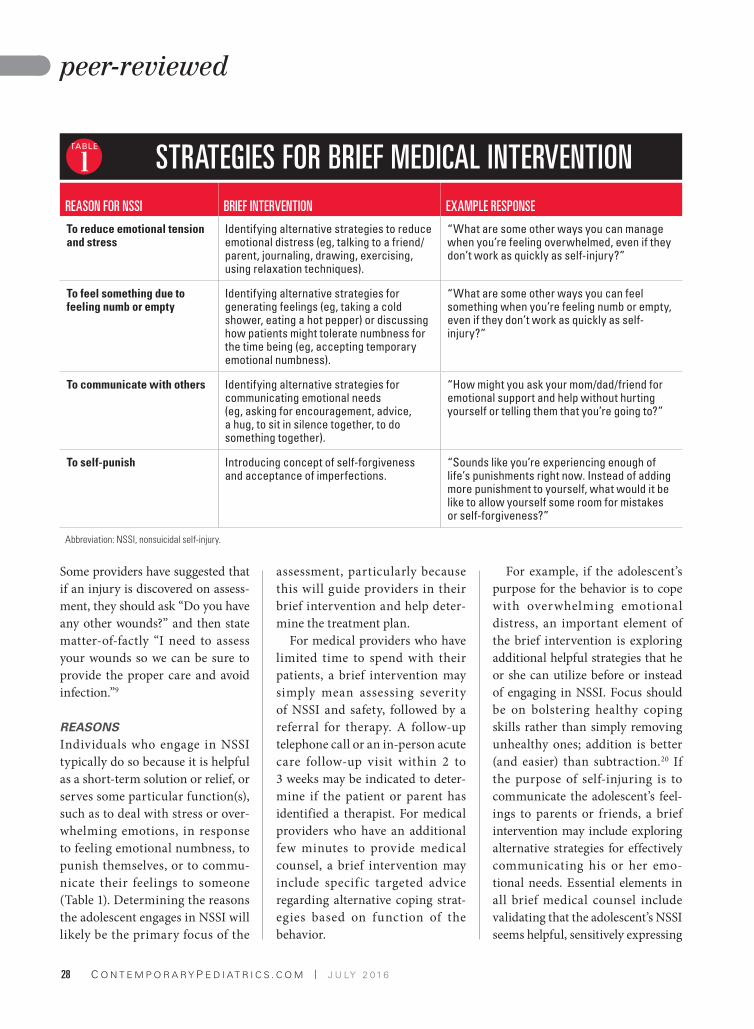
peer-reviewed feature25 SOARS model: Risk assessment of nonsuicidal self injury A new asssessment tool helps physicians screen adolescents for self-harming
behaviors, then develop a treatment plan or referral to therapy for these patients.
Nicholas J Westers, PSYD; Jennifer J Muehlenkamp, PHD, May Lau, MD, MPH
departments9 INTER@CTIVE
Readers react.
10 EYE ON WASHINGTON
FDA revamps nutrition facts labels.
11 JOURNAL CLUB
in addition4 EDITORIAL ADVISORY BOARD
45 ADVERTISING INDEX
Page 5
© 2016 Impax Laboratories, Inc.
All rights reserved. Printed in USA 04/2016 PP-ADP-MEB-US-0005
NOW AVAILABLEReferences: 1. EMVERM [prescribing information]. Horsham, PA: Amedra Pharmaceuticals LLC; 2015. 2. Committee on Infectious Diseases, American
Academy of Pediatrics. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics;
2012:566-567,851. 3. Friedman AJ, Ali SM, Albonico M. [published online December 24, 2012]. J Trop Med. 2012;2012:590463. doi:10.1155/2012/590463.
4. Treatment. Centers for Disease Control and Prevention website. http://www.cdc.gov/parasites/pinworm/treatment.html. Updated July 19, 2013.
Accessed January 22, 2016.
INDICATION
EMVERM (mebendazole) 100 mg chewable tablet is indicated in adults and children over 2 years of age for the treatment of Enterobius vermicularis (pinworm), Trichuris trichiura (whipworm), Ascaris lumbricoides (common roundworm), Ancylostoma duodenale (common hookworm), and Necator americanus (American hookworm) in single or mixed infections.
IMPORTANT SAFETY INFORMATION
Mebendazole is contraindicated in persons who have shown hypersensitivity to the drug.
Warnings: There is no evidence that mebendazole, even at high doses, is effective for hydatid disease. There have been rare reports of neutropenia and agranulocytosis when mebendazole was taken for prolonged periods and at dosages substantially above those recommended.
Precautions: Periodic assessment of organ system functions, including hematopoietic and hepatic, is advisable during prolonged therapy.
Adverse reactions include: Transient symptoms of abdominal pain and diarrhea with expulsion of worms in cases of massive infection; liver function test elevations [AST (SGOT), ALT (SGPT), and GGT]; and on rare occasions hypersensitivity (rash, urticaria and angioedema); rare reports of neutropenia, agranulocytosis (see WARNINGS) and hepatitis when mebendazole was taken for prolonged periods and at dosages substantially above those recommended; and very rare cases of convulsions.
Drug Interactions: Preliminary evidence suggests that cimetidine inhibits mebendazole metabolism and may result in an increase in plasma concentrations of mebendazole.
Pregnancy Category C: Mebendazole has shown embryotoxic and teratogenic activity in pregnant rats at single oral doses as low as 10 mg/kg (approximately equal to the human dose, based on mg/m2). In view of these fi ndings the use of mebendazole is not recommended in pregnant women.
Nursing Mothers: It is not known whether mebendazole is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when mebendazole is administered to a nursing woman.
Pediatric Use: The drug has not been extensively studied in children under two years; therefore, in the treatment of children under two years the relative benefi t/risk should be considered.
Overdosage: In the event of accidental overdosage, gastrointestinal complaints lasting up to a few hours may occur. Vomiting and purging should be induced. Activated charcoal may be given.
Information for Patients:
% Patients should be informed of the potential risk to the fetus in women taking mebendazole during pregnancy, especially during the fi rst trimester (See Pregnancy Category C).
% Patients should also be informed that cleanliness is important to prevent reinfection and transmission of the infection.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1-800-FDA-1088. To report SUSPECTED ADVERSE REACTIONS contact Impax Laboratories, Inc. at 1-877-994-6729.
See full Prescribing Information at www.EMVERMHCP.com and Brief Summary on following page.
AAP, American Academy of Pediatrics; CDC, Centers for Disease Control and Prevention; FDA, US Food and Drug Administration.
THE EMVERM SAVINGS CARD IS AVAILABLE ONLINE AT
WWW.EMVERMHCP.COM/SAVINGS
>��The ONLY FDA-APPROVED prescription treatment indicated for pinworm2
>� Mebendazole—prescribed by physicians for MORE THAN 40 YEARS3
>��The AAP Red Book recommends mebendazole as a DRUG OF CHOICE for highly contagious pinworm infections2
>��The AAP Red Book and CDC recommend TREATING THE ENTIRE HOUSEHOLD since family members are frequently infected2,4
>� ONE 100-MG CHEWABLE TABLET, for ONE DAY is the same dosage schedule for children and adults1
WITH ITS 95% CURE RATE1
IS BACKMEBENDAZOLE
NOW AVAILABLE FOR PINWORM
Page 6
!"#!$"
%&
'()*)+,-./0)1
&
233&(4&56)7-*0)&8-*0)9:
&
;$<!=&>?""@$AB&!""#$%&'%("#)*+",-#./,#.011#$,"+&,232*(#
)*./,4%-2/*#
<CD<5@8<EC>&@CD&?>@F!&
5"3"*6%7/1"#-%31"-+#%,"#2*62&%-"6#./,#-8"#-,"%-4"*-#/.#
!"#$%&'()*+,$%-(.)/0%(*#9:2*;/,4<=#1%(.2)%(*+#%(.2()%0#
9;82:;/,4<=#3*.0%(*+/)-'%(.&(4$*#9&/44/*#,/0*6;/,4<=#
3".5/&*#&-0+4)&4$"0/$#9&/44/*#8//';/,4<=#6$.0#&%+
0-$%(.0")*#9>4",2&%*#8//';/,4<#2*#+2*(1"#/,#42?"6#2*."&-2/*+@#
A..2&%&B#C%,2"+#%+#%#.0*&-2/*#/.#+0&8#.%&-/,+#%+#:,""?2+-2*(#62%,,8"%#
%*6#(%+-,/2*-"+-2*%1#-,%*+2-#-24"=#6"(,""#/.#2*."&-2/*=#%*6#
8"142*-8#+-,%2*+@#A..2&%&B#,%-"+#6",2C"6#.,/4#C%,2/0+#+-062"+#%,"#
+8/;*#2*#-8"#-%31"#3"1/;@#
&
GH+7/I(&
')+9)I/*H-:H:1&
J6HK7/I(&
'9IHL6MIH-:H:1&
5/((/+&
$/M+,7/I(&
'-:L-IH-:H:1&
N//O7/I(&
5MI)&I-9):&
4"%*&DEF# GHF# DHF# DGF#
&!44&
I),ML9H/+&
4"%*&
I# DJF# DDF# DDF#
5EC8$@<CD<5@8<EC>&
5"3"*6%7/1"#2+#&/*-,%2*62&%-"6#2*#:",+/*+#;8/#8%C"#+8/;*#
8B:",+"*+2-2C2-B#-/#-8"#6,0(@#
J@$C<CF>&
K8","#2+#*/#"C26"*&"#-8%-#4"3"*6%7/1"=#"C"*#%-#82(8#6/+"+=#2+#
".."&-2C"#./,#8B6%-26#62+"%+"@#K8","#8%C"#3""*#,%,"#,":/,-+#/.#
*"0-,/:"*2%#%*6#%(,%*01/&B-/+2+#;8"*#4"3"*6%7/1"#;%+#-%'"*#
./,#:,/1/*("6#:",2/6+#%*6#%-#6/+%("+#+03+-%*-2%11B#%3/C"#-8/+"#
,"&/44"*6"6@#
G$!5@?8<EC>&
F)+)I-0&
G)IH/,HL&-::)::()+9&/P&/I4-+&:Q:9)(&PM+L9H/+:R&H+L0M,H+4&
6)(-9/K/H)9HL&-+,&6)K-9HLR&H:&-,SH:-*0)&,MIH+4&KI/0/+4),&
96)I-KQT&
<+P/I(-9H/+&P/I&G-9H)+9:&
$%-2"*-+#+8/016#3"#2*./,4"6#/.#-8"#:/-"*-2%1#,2+'#-/#-8"#."-0+#2*#
;/4"*#-%'2*(#4"3"*6%7/1"#60,2*(#:,"(*%*&B=#"+:"&2%11B#60,2*(#
-8"#.2,+-#-,24"+-",#9!""#GI)4+-+LQ&5-9)4/IQ&5<@#
$%-2"*-+#+8/016#%1+/#3"#2*./,4"6#-8%-#&1"%*12*"++#2+#24:/,-%*-#-/#
:,"C"*-#,"2*."&-2/*#%*6#-,%*+42++2/*#/.#-8"#2*."&-2/*@#
DIM4&<+9)I-L9H/+:&
$,"1242*%,B#"C26"*&"#+0(("+-+#-8%-#&24"-262*"#2*8232-+#
4"3"*6%7/1"#4"-%3/12+4#%*6#4%B#,"+01-#2*#%*#2*&,"%+"#2*#:1%+4%#
&/*&"*-,%-2/*+#/.#4"3"*6%7/1"@#
5-ILH+/4)+):H:R&"M9-4)+):H:R&<(K-HI()+9&/P&=)I9H0H9Q&
)*#&%,&2*/("*2&2-B#-"+-+#/.#4"3"*6%7/1"#2*#42&"#%*6#,%-+=#*/#
&%,&2*/("*2&#".."&-+#;","#+""*#%-#6/+"+#%+#82(8#%+#LM#4(N'(#9/*"#
-/#-;/#-24"+#-8"#804%*#6/+"=#3%+"6#/*#4(N4O<#(2C"*#6%21B#/C",#
-;/#B"%,+@#P/42*%*-#1"-8%1#40-%-2/*#-"+-+#2*#42&"#+8/;"6#*/#
40-%("*2&2-B#%-#+2*(1"#6/+"+#%+#82(8#%+#GLM#4(N'(#9QH#-24"+#-8"#
804%*#6/+"=#3%+"6#/*#4(N4O<@#R"2-8",#-8"#+:",4%-/&B-"#-"+-=#
-8"#SQ#-,%*+1/&%-2/*#-"+-=#*/,#-8"#>4"+#-"+-#2*62&%-"6#40-%("*2&#
:,/:",-2"+@#P/+"+#0:#-/#LM#4(N'(#2*#42&"#9"T0%1#-/#-8"#804%*#
6/+"=#3%+"6#/*#4(N4O<=#(2C"*#-/#4%1"+#./,#GM#6%B+#%*6#-/#."4%1"+#
./,#QL#6%B+#:,2/,#-/#("+-%-2/*=#8%6#*/#".."&-#0:/*#."-0+"+#%*6#
/..+:,2*(=#-8/0(8#-8","#;%+#+12(8-#4%-",*%1#-/?2&2-B@#
GI)4+-+LQ&
8)I-9/4)+HL&!PP)L9:&
$,"(*%*&B#U%-"(/,B#U#
5"3"*6%7/1"#8%+#+8/;*#"43,B/-/?2&#%*6#-",%-/("*2&#%&-2C2-B#2*#
:,"(*%*-#,%-+#%-#+2*(1"#/,%1#6/+"+#%+#1/;#%+#QM#4(N'(#
9%::,/?24%-"1B#"T0%1#-/#-8"#804%*#6/+"=#3%+"6#/*#4(N4O<@#)*#
C2";#/.#-8"+"#.2*62*(+#-8"#0+"#/.#4"3"*6%7/1"#2+#*/-#
,"&/44"*6"6#2*#:,"(*%*-#;/4"*@#>1-8/0(8#-8","#%,"#*/#
%6"T0%-"#%*6#;"11V&/*-,/11"6#+-062"+#2*#:,"(*%*-#;/4"*=#%#:/+-V
4%,'"-2*(#+0,C"B#8%+#3""*#6/*"#/.#%#1242-"6#*043",#/.#;/4"*#
;8/#2*%6C",-"*-1B#8%6#&/*+04"6#4"3"*6%7/1"#60,2*(#-8"#.2,+-#
-,24"+-",#/.#:,"(*%*&B@#K8"#2*&26"*&"#/.#+:/*-%*"/0+#%3/,-2/*#
%*6#4%1./,4%-2/*#626#*/-#"?&""6#-8%-#2*#-8"#("*",%1#:/:01%-2/*7#
)*#QWM#6"12C",2"+#/*#-",4=#*/#-",%-/("*2&#,2+'#/.#4"3"*6%7/1"#;%+#
26"*-2.2"6@#
CMI:H+4&"/96)I:&
)-#2+#*/-#'*/;*#;8"-8",#4"3"*6%7/1"#2+#"?&,"-"6#2*#804%*#421'@#
X"&%0+"#4%*B#6,0(+#%,"#"?&,"-"6#2*#804%*#421'=#&%0-2/*#+8/016#
3"#"?",&2+"6#;8"*#4"3"*6%7/1"#2+#%642*2+-","6#-/#%#*0,+2*(#
;/4%*@#
G),H-9IHL&?:)&
K8"#6,0(#8%+#*/-#3""*#"?-"*+2C"1B#+-062"6#2*#&8216,"*#0*6",#-;/#
B"%,+Y#-8","./,"=#2*#-8"#-,"%-4"*-#/.#&8216,"*#0*6",#-;/#B"%,+#-8"#
,"1%-2C"#3"*".2-N,2+'#+8/016#3"#&/*+26","6@#
@D#!$>!&$!@58<EC>&
F-:9I/H+9):9H+-0&
K,%*+2"*-#+B4:-/4+#/.#%36/42*%1#:%2*#%*6#62%,,8"%#2*#&%+"+#/.#
4%++2C"#2*."&-2/*#%*6#"?:01+2/*#/.#;/,4+@#
NQK)I:)+:H9HSH9Q&
Z%+8=#0,-2&%,2%#%*6#%*(2/"6"4%#8%C"#3""*#/3+",C"6#/*#,%,"#
/&&%+2/*+@#
5)+9I-0&C)IS/M:&>Q:9)(&
[",B#,%,"#&%+"+#/.#&/*C01+2/*+#8%C"#3""*#,":/,-"6@#
UHS)I&
K8","#8%C"#3""*#12C",#.0*&-2/*#-"+-#"1"C%-2/*+#\>!K#9!]^K<=#>_K#
9!]$K<=#%*6#]]K`#%*6#,%,"#,":/,-+#/.#8":%-2-2+#;8"*#4"3"*6%7/1"#
;%+#-%'"*#./,#:,/1/*("6#:",2/6+#%*6#%-#6/+%("+#+03+-%*-2%11B#
%3/C"#-8/+"#,"&/44"*6"6@#
N)(-9/0/4HL&
R"0-,/:"*2%#%*6#%(,%*01/&B-/+2+@#9!""#J@$C<CF><@#
E#!$DE>@F!&
)*#-8"#"C"*-#/.#%&&26"*-%1#/C",6/+%("=#(%+-,/2*-"+-2*%1#&/4:1%2*-+#
1%+-2*(#0:#-/#%#.";#8/0,+#4%B#/&&0,@#[/42-2*(#%*6#:0,(2*(#+8/016#
3"#2*60&"6@#>&-2C%-"6#&8%,&/%1#4%B#3"#(2C"*@#
DE>@F!&@CD&@D"<C<>8$@8<EC&
K8"#+%4"#6/+%("#+&8"601"#%::12"+#-/#&8216,"*#%*6#%601-+@#K8"#
-%31"-#4%B#3"#&8";"6=#+;%11/;"6=#/,#&,0+8"6#%*6#42?"6#;2-8#
.//6@#
&
GH+7/I(&
')+9)I/*H-:H:1&
J6HK7/I(&
'9IHL6MIH-:H:1&
5/((/+&
$/M+,7/I(&
'-:L-IH-:H:1&
N//O7/I(&
D/:)# Q#-%31"-=#/*&"#
Q#-%31"-#
4/,*2*(#%*6#
"C"*2*(#./,####
J#&/*+"&0-2C"#
6%B+#
Q#-%31"-#
4/,*2*(#%*6#
"C"*2*(#./,####
J#&/*+"&0-2C"#
6%B+#
Q#-%31"-#
4/,*2*(#%*6#
"C"*2*(#./,####
J#&/*+"&0-2C"#
6%B+#
).#-8"#:%-2"*-#2+#*/-#&0,"6#-8,""#;""'+#%.-",#-,"%-4"*-=#%#+"&/*6#
&/0,+"#/.#-,"%-4"*-#2+#%6C2+"6@#R/#+:"&2%1#:,/&"60,"+=#+0&8#%+#
.%+-2*(#/,#:0,(2*(=#%,"#,"T02,"6@#
#
A/M&-I)&)+L/MI-4),&9/&I)K/I9&+)4-9HS)&:H,)&)PP)L9:&/P&
KI):LIHK9H/+&,IM4:&9/&96)&=D@T&#H:H9&777TP,-T4/SV(),7-9L6R&/I&
L-00&2WX33W=D@W23XXT&8/&I)K/I9&>?>G!58!D&@D#!$>!&$!@58<EC>&
L/+9-L9&<(K-Y&U-*/I-9/IH):R&<+LT&-9&2WXZZW[[\W]Z^[T#
&
G0)-:)&>))&PM00&GI):LIH*H+4&<+P/I(-9H/+&-9&
777T)(S)I(6LKTL/(T&&
&
P2+-,230-"6#XBa#>4"6,%#$8%,4%&"0-2&%1+#__U#
b/,+8%4=#$>#QDMLL#
#
cOMQG#)4:%?#_%3/,%-/,2"+=#)*&@#
>11#,2(8-+#,"+",C"6@#$,2*-"6#2*#d!>@#
MQNOMQG##$$Ve$)V5AXVd!VMMMO#
#
Page 7
9J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
inter ctive JOIN US AND JOIN IN WITH YOUR PEDIATRIC PEERS AT CONTEMPORARYPEDIATRICS.COM
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 6
40
ANDREW J SCHUMAN, MD SECTION EDITOR
peds v2.0
Every few years I like to speculate about the future of medical technol-ogy as well as the future of pediat-ric practice. Both, you see, are very much intertwined, and in my view the future of pediatric practice looks very good indeed.One needs to consider that we practice medicine at a time when innovation is progressing at an amazing pace. In the tech sector, experts speak frequently of “dis-ruptive technologies” that create entirely new ways of doing things, or shake up an industry entirely. For example, personal computers replaced the typewriter decades ago, and downloadable media is replac-ing compact disc media, just as compact discs replaced videocas-sette tapes and vinyl records. Let’s take a look at some current medical technologies that are “begging” for disruption, and other technologies that may prove to be “game chang-ers” over the next few years.
To help improve pediatric prac-tice, physicians must remain nim-ble, optimistic, and ever willing to try new things. We also must be innovators ourselves, to challenge the status quo and to aggressively confront government or insurance reforms when they are not in our patients’ best interest or ours. It is important to remember that inno-vation is not limited to keeping an open mind toward new office tech-nologies. It also involves being cre-ative when it means implementing new models of care or new work-flows, and utilizing improved meth-ods of educating parents to keep our patients healthy.
Curing MDSDYep, I have just identified a new medical condition—one that is not yet listed in the Diagnostic and Statistical Manual of Mental Dis-orders, Fifth Edition! Medical docu-mentation stress disorder (MDSD)
unfortunately affects many physi-cians who have been forced by the government to prematurely adopt expensive and inefficient electronic health record (EHR) systems. I dis-cussed improving medical docu-mentation (ie, avoiding “note bloat”) in the January 2016 issue of Contem-porary Pediatrics.If you are unfamiliar with this condition, let me enlighten you. Medical documentation stress dis-order is a “click”-related disorder, caused by the inability of provid-ers to expedite completion of office notes, therefore requiring taking an hour or more of one’s personal time to complete notes at home. Symptoms include staring into space or yelling at one’s computer screen, as well as a compulsion to frequently check one’s retirement funds, and chronic pain in one’s dominant hand.
Fortunately, MDSD is a treatable condition. Management modali-ties include scribes, virtual scribes (see Contemporary Pediatrics , November 2015), and my favor-ite, voice recognition software (see Contemporary Pediatrics, June
Disruptive technology and pediatric practiceHere is a closer look at several innovative medical technologies that are poised to become “game changers” in pediatric practice.
Part of the
Contemporary Pediatrics is part of the ModernMedicine Network, a Web-based portal for health professionals offering best-in-class content and tools in a rewarding and easy-to-use environment for knowledge sharing among members of our community.
Hearing You on Deafness
our digital guru, Dr. Andrew
Schuman, considers game-changing tech for your
pediatric practice. Don’t miss his latest Peds v2.0 article at
ContemporaryPediatrics.com/Schuman-0716
We heard from you about Dr. Andrew
Schuman’s latest article “MOC reform:
One year later,” June 2016, and
also regarding Dr. Rachel St. John’s
commentary “Pathologizing deafness,”
May 2016. Here are just a few of your
thoughts on these articles.
Thank you for the excellent article
regarding the update on MOC. Here
is a very brief summary of my opinion
regarding MOC. I did research before
going to medical school and became a
doctor because I did not want to continue
doing research. The very small amount
of knowledge gleaned from the large
amount of time utilized to complete MOC
part 4 is not acceptable to me. I hardly
have enough time in the day just to see
my patients. I have no problem with
examinations to assess my competency,
but the rest of MOC is a huge waste of
time designed by and for academicians.
—Ron Beckel, MD
****
I just fi nished reading the Contemporary
Pediatrics article about MOC reform.
I love what the ABA has done with
weekly/monthly questions. I’m in for
piloting that with ABP!
— Thomas D. Miller, MD
I enjoyed your recent article on the
latest in MOC. There are at least 2 other
things wrong with MOC, besides what
you point out:
1. There is no distinction between
academics and those in private practice.
If one is actively engaged in teaching
and research, there should be some
sort of a waiver for the educational
part —eg, if I publish articles and give
talks, that should be proof enough that
I am keeping up (at least in my area of
specialization).
2. The fee schedule borders on extortion.
After passing my last exam in 2012 and
completing all of my MOC requirements,
the ABP would not list me as board
certifi ed until I paid for the next 10 years!
And the fee is nonrefundable, so if I died
the next day, my widow would be out
$1200.
—Ben Z. Katz, MD
****
This is very useful. I am planning to
approach [my] state legislature about
MOC reform to implement a similar law
as Oklahoma.
—Paul G. Mathew, MD, FAAN, FAHS
MORE TALK ON MOCI respect your opinion, and
I know that there [are] loud
advocates from the “disabilities
movement” that are getting
a lot of media attention. Yet, I
disagree. Would you say the
same about blindness? Would
you say the same about spasticity
with cerebral palsy? Yes, there
are hundreds of individuals that
live meaningful lives despite or
because of the above conditions.
But these are still conditions
that require prevention and
accommodation.
— Francisco Enriquez, MD, FAAP
Dr. St. John’s letter was the
epitomy of political correctness,
unless I am totally naive after forty
years of practice. Is being blind a
pathological situation? We can
teach Braille and getting around
with a cane. Who would not want
their eyesight restored? Lacking 1
of the 5 senses is a defi ciency. It
is fi ne to try to accommodate for
the absence of a sense, but even
better to restore it.
— Irwin H. Berkowitz, MD, FAAP
Congratulations to
our Editorial Advisory
Board Member,
Dr. Donna Hallas,
recipient of the
2016 American
Association of Nurse
Practitioners (AANP) Nurse
Practitioner State Award
for Excellence (New York),
which recognizes outstanding
achievements by NPs and NP
advocates. Brava!
Page 8
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 610
washingtonBY KATHRYN FOXHALL
washingtonEYE ON
FOR MORE NEWS @CONTEMPEDSCONTEMPORARYPEDIATRICS.COM/EOW
In May 2016, the US Food and
Drug Administration (FDA) an-
nounced the revamping of the
rules for the “nutrition facts” la-
bel box on packaged foods, the
fi rst major such overall in 20 years.
With the obesity epidemic con-
tinuing, much of the emphasis in
the announcement was on things
such as the FDA’s new requirement
that manufacturers list “added sug-
ars” and that they use a new for-
mat which, among other things,
will display the calories much more
prominently.
Less talked about was the fact
that in the 2 years since the FDA
proposed the changes, there has
been a massive discussion, via the
agency’s regulatory process, on the
many aspects of nutrition science
and policy.
As 1 example, in a comment to
the FDA last fall, the American
Academy of Pediatrics (AAP) said it
was comfortable with the proposal
of a Daily Reference Value (DRV)
of 25 g “for added sugars based on
a 1000-calorie reference amount for
children 1 through 3 years of age.”
However, the AAP said, it’s a
problem that the rules would, in
effect, extend the added sugar rec-
ommendations for an adult to chil-
dren as young as age 4 years, which
would indicate it would be okay for
them to eat up to 14% of their calo-
ries in added sugar.
The FDA declined to make
a change based on the AAP’s
comment, saying that a separate
DRV for different child age groups
“could clutter the label, cause con-
fusion, and draw attention to the
added sugars declaration because
more space would be required for
2 separate percent DV declarations
on the label.”
In another instance, the AAP,
the March of Dimes, and about
22 other groups said the change in
the way the FDA will require that
folic acid be listed could lead to
public confusion, limit the ability
to monitor intake and safety, and
negatively impact birth outcomes.
The new rule would mandate the
expression of the Recommended
Dietary Allowance (RDA) for folate
in “Dietary Folate Equivalents
(DFEs).” The groups’ comments
said, “Because of the difference
between measuring folate/folic acid
in DFEs versus micrograms, this
means the RDA is lower than the
[US Public Health Service] rec-
ommendation for intake among
women of childbearing age.”
The FDA, however, noted that
the DFE, developed by the Institute
of Medicine, “accounts for the
dif ferences in bioavai labi l ity
between food folate (natural folate)
and folic acid, which is more bio-
available (about 1.7 times more
bioavailable).”
The AAP also urged the FDA
to require that foods be labeled for
caffeine because of its numerous
adverse effects. It noted findings
from the American Association of
Poison Control Centers that “more
than 40% of 5156 calls about energy
drinks to US poison control centers
involved children younger than
6, with some suffering serious car-
diac and neurological symptoms.”
In other rules related to obesity,
the FDA says that because pack-
age size affects what people eat,
packages that are between 1 and
2 servings must be labeled as 1 serv-
ing in terms of calories and other
nutrients because people typically
consume those packages in 1 sitting.
Examples are a 20-ounce soda or a
15-ounce can of soup.
Large food manufacturers have
2 years to comply with all the new
requirements, by July 26, 2018, and
those with less than $10 million in
sales have another year after that.
FDA revamps nutrition facts label box
CME VIDEO FOR PHYSICIANS
The FDA and the American Medical Association have announced a
new continuing medical education (CME) video for physicians about
discussing the nutrition facts labels with patients. For this CME, go to
https://cme.ama-assn.org/Activity/4252182/Detail.aspx
Page 9
11J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
journal clubBY MARIAN FREEDMAN COMMENTARY BY MICHAEL G BURKE, MD
journal club CONTEMPORARYPEDIATRICS
A new clinical decision sup-
port tool prompts clini-
cians to ask parents about
secondhand smoke ex-
posure, provides an elec-
tronic nicotine replacement therapy
(NRT) prescription, and makes
referrals for follow-up and further
guidance. A study found that the
tool is easy to use and has a clinical
impact.
Investigators conducted the study
within the Children’s Hospital of
Philadelphia Pediatric Research
Consortium, which includes 31 prac-
tices in 2 states. The tool, which
interfaces with the electronic health
record (EHR), first prompts the
clinician to ask the parent about
smoking status and whether he or
she wants to quit. An affirmative
response triggers a link to an elec-
tronic NRT prescription (nicotine
patch or gum) with dosing guid-
ance. Finally, the tool prompts cli-
nicians to refer parents to an adult
tobacco treatment program and
additional resources and to update
the EHR.
During a 3-month period, clini-
cians used the tool at about three-
quarters of more than 3000 visits at
which 165 parents expressed inter-
est in quitting smoking and were
offered treatment. Although clini-
cian use of the tool varied substan-
tially, more than 75% of clinicians
used the tool at more than 60% of
visits. Of 24 clinicians (18 pediatri-
cians and 6 nurse practitioners) who
used the tool, 17 completed a follow-
up survey. Of these, 94% reported
that they were satisfied with the tool
and found it helpful.
Among the tool’s advantages,
ease of use, a reminder to screen all
parents about smoking, and access
to an electronic NRT prescription
were cited by respondents. Nearly
90% of parents interested in quitting
who were surveyed reported being
satisfied or very satisfied with their
treatment (64% received an NRT
prescription and 25% had filled a
prescription and were using it), and
28% noted that they were moti-
vated to be treated because quitting
was framed around helping their
child (Jenssen BP, et al. Pediatrics.
2016;137[5]:e20154185).
This smoking cessation intervention works!
An analysis of data on the inci-
dence of pertussis shows that
although acellular pertussis (Tdap)
vaccine had a posit ive impact
among adolescents in the 4 years
after it was introduced in 2005,
in 2010 pertussis incidence in this
age group began to increase more
rapidly than it did in all other age
groups. This abrupt shift in inci-
dence occurred in the same year
that 11-year-olds represented the
f irst group of children to have
received acellular vaccines for all
doses of the childhood series, fol-
lowing the 1997 transition from
Tdap booster in teens less effective after initial acellular vaccine series
We know that we should screen for smoke exposure in the home, offer
counseling and referral to smoking cessation resources, and arrange for NRT,
but, as several studies have shown, we don’t. During a short offi ce encounter,
we face obstacles all along the way. The tool described here is an example of
how the EHR makes it easier to get done what we know needs to be done. It
prompts the physician to screen for smoke exposure, presents information on
smoking cessation, allows arrangements for a recruitment call from a smoking
cessation counselor, and provides a prescription for nicotine replacement with
dosing information included. By removing obstacles, this EHR application could
improve health for both parents and children. —Michael G Burke, MD
commentary
Page 10
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 612
journal club
whole pertussis to acellular vac-
cines. These findings indicate that
a Tdap booster vaccine in ado-
lescence has a diminished effect
among those who were primed
with acellular pertussis vaccine in
early childhood.
The extended analysis of reported
pertussis cases between 1990 and
2014 shows that pertussis incidence
was highest among infants aged
younger than 1 year throughout the
period. Pertussis rates were com-
parable among all other age groups
until the late 2000s when the per-
tussis burden increased among chil-
dren aged 1 to 10 years; between
2007 and 2011, the incidence of
pertussis in children in this age
group was 1 to 2 times higher than
in adolescents aged 11 to 18 years.
However, when trends reversed
in 2010, rates of pertussis among
11- to 18-year-olds increased at a
faster rate than it did in all other
age groups combined, and by 2014
adolescents had overtaken all but
young infants in pertussis incidence
(Skoff TH, et al. JAMA Pediatr.
2016;170[5]:453-458).
This means that pertussis is not going away and, despite Tdap boosters, incidence will continue to rise as more children
initially vaccinated with acellular pertussis vaccine move through adolescence. In the words of the researchers, “[S]usceptible
individuals will continue to accumulate in the population.” Until a new solution is devised, it is up to us to continue to think
about pertussis, recognize it early, and initiate treatment to decrease spread. —Michael G Burke, MD
Among children with mild gastroen-
teritis and minimal dehydration, ini-
tial oral hydration with dilute apple
juice followed by preferred f luids is
more beneficial than electrolyte main-
tenance solution, a large study in a
pediatric emergency department (ED)
found.
The 647 study participants, aged 6 to
60 months, were divided into an inter-
vention group that received half-strength
apple juice and a control group that
was given an apple-flavored electrolyte
maintenance solution. After discharge,
the apple juice group was instructed to
drink whatever fluids they wished, while
the electrolyte maintenance solution
group replaced f luids with electrolyte
maintenance solution.
At fol low-up, fewer ch i ld ren
in the apple juice/preferred f lu-
ids group received intravenous rehy-
dration (Freedman SB, et al. JAMA.
2016;315[18]:1966-1974).
Mild gastroenteritis? Try dilute apple juice!
Dilute apple juice or other liquids were not only as good as electrolyte solution in this
study, they were better. Perhaps IV hydration and admission were more common in
the electrolyte solution group because parents had to purchase the solution after ED
discharge, while those in the dilute apple juice arm of the study could be given any fluid
available at home. It is important to note that this study included only patients aged at
least 6 months and only those with mild dehydration; 81% of the enrolled patients had
dehydration scores of 0 or 1 on an 8-point scale. Diarrhea leading to life-threatening
dehydration and electrolyte disturbances is a real and scary thing, even in developed
countries. Dilute apple juice may be fine for mildly dehydrated children, but in moderate to
severe diarrhea I will stick with electrolyte solution. —Michael G Burke, MD
commentary
commentary
Marijuana use can trigger
recurrent cyclic vomiting
in teenagers. A new report
points out that 1 known
cause of cyclic vomiting
syndrome (CVS) is chronic
use of cannabis. Cyclic
vomiting syndrome is a
constellation of recurrent
vomiting, nausea,
and abdominal pain.
When linked to chronic
marijuana use, CVS has
the unique characteristic
of being temporarily
relieved by frequent hot
showers. The researchers
recommend screening for
marijuana use by history
and a urine drug screen
in adolescents with CVS
who take hot showers for
symptomatic relief (Sawni
A, et al. Clin Pediatr.
2016;55[6]:560-563).
also of note
Page 11
13J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
puzzlerIM
AG
E C
RE
DIT
/AU
TH
OR
SU
PP
LIE
D
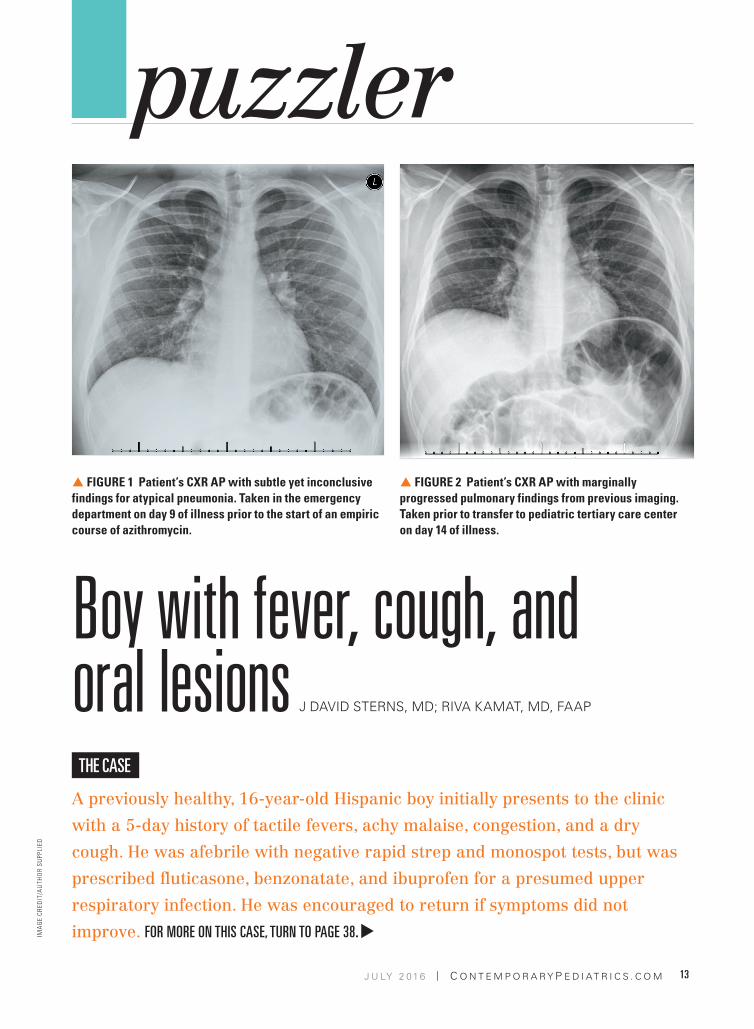
Boy with fever, cough, and oral lesions
A previously healthy, 16-year-old Hispanic boy initially presents to the clinic
with a 5-day history of tactile fevers, achy malaise, congestion, and a dry
cough. He was afebrile with negative rapid strep and monospot tests, but was
prescribed fluticasone, benzonatate, and ibuprofen for a presumed upper
respiratory infection. He was encouraged to return if symptoms did not
improve. FOR MORE ON THIS CASE, TURN TO PAGE 38.
THE CASE
J DAVID STERNS, MD; RIVA KAMAT, MD, FAAP
S FIGURE 1 Patient’s CXR AP with subtle yet inconclusive
findings for atypical pneumonia. Taken in the emergency
department on day 9 of illness prior to the start of an empiric
course of azithromycin.
S FIGURE 2 Patient’s CXR AP with marginally
progressed pulmonary findings from previous imaging.
Taken prior to transfer to pediatric tertiary care center
on day 14 of illness.
Page 12
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 614
PEER-REVIEWED FEATURE
Dr Bass is chief medical
information officer and
associate professor of
medicine and of pediatrics,
Louisiana State University
Health Sciences Center–
Shreveport. The author
has nothing to disclose in
regard to affiliations with
or financial interests in
any organizations that may
have an interest in any part
of this article.
The introduction of conjugated vaccines
has decreased the incidence of bacte-
rial meningitis in children, amounting to
one of the biggest public health successes
in the practicing pediatrician’s career. In
fact, the median age of patients success-
fully treated for bacterial meningitis has
increased from younger than age 5 years
to age 42 years and older. Improvements
have been seen in every age group, except
in those aged younger than 2 months.
Cases of meningitis from strains of bac-
teria not covered by vaccination and
drug-resistant strains, however, remain a
concern for pediatric patients.
Etiology, epidemiology, and risk factorsThe most common causes of bacterial
meningitis are Streptococcus pneumoniae,
Neisseria meningitidis, Haemophilus
influenzae type b (Hib; rarely a cause since
the development of a vaccine), group B
Streptococcus (GBS), and Listeria monocy-
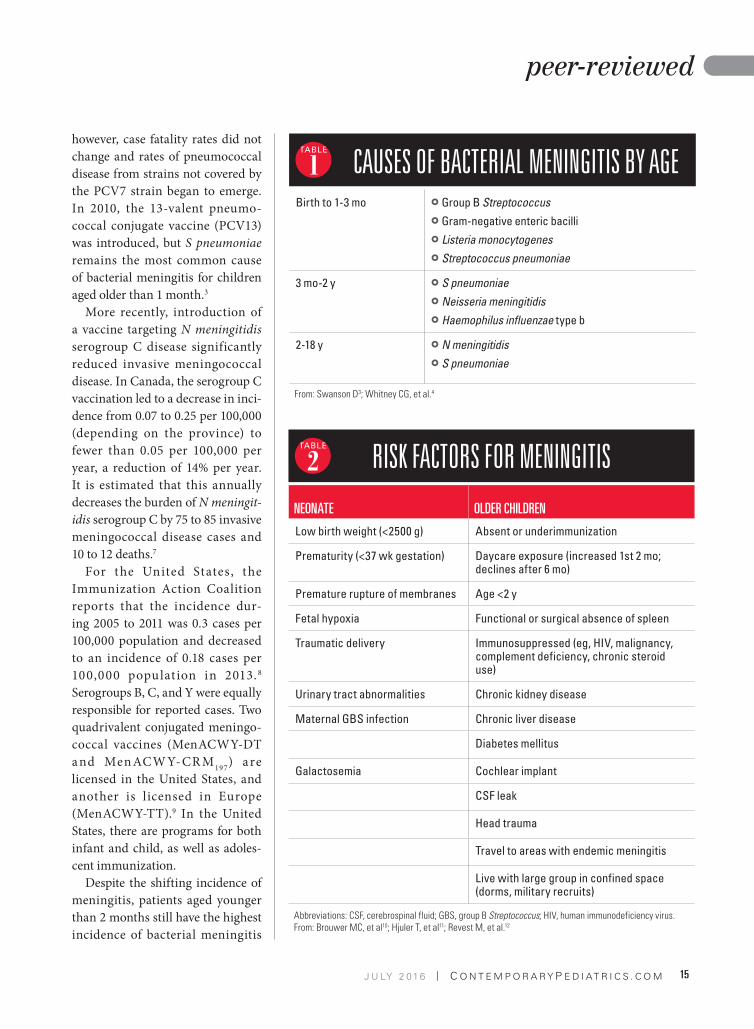
togenes.1-3 Etiology depends on the age of
the patient (Table 1).3,4 Introduction of the
conjugate Hib vaccine in the 1990s almost
eliminated Hib in countries in which it was
introduced and decreased the overall inci-
dence of meningitis by nearly 55%.3 This
was followed by the introduction of the
heptavalent pneumococcal vaccine (PCV7)
in 2000, which reduced pneumococcal
meningitis by nearly 60% in children aged
younger than 2 years.3-5
In the years between 1998 and 2007,
herd immunity continued to drop the rate
of meningitis by more than 30%, from a
rate of 2 cases per 100,000 to 1.38 cases
per 100,000.3,6 Despite these advances,
Deciphering bacterial meningitisPAT F BASS III, MD, MS, MPH
Pediatricians need to understand not only how bacterial meningitis can be prevented through vaccination, but also its risks, symptoms, workup, and treatment.
Bacterial Meningitis
Page 13
15J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
peer-reviewed
however, case fatality rates did not
change and rates of pneumococcal
disease from strains not covered by
the PCV7 strain began to emerge.
In 2010, the 13-valent pneumo-
coccal conjugate vaccine (PCV13)
was introduced, but S pneumoniae
remains the most common cause
of bacterial meningitis for children
aged older than 1 month.3
More recently, introduction of
a vaccine targeting N meningitidis
serogroup C disease significantly
reduced invasive meningococcal
disease. In Canada, the serogroup C
vaccination led to a decrease in inci-
dence from 0.07 to 0.25 per 100,000
(depending on the province) to
fewer than 0.05 per 100,000 per
year, a reduction of 14% per year.
It is estimated that this annually
decreases the burden of N meningit-
idis serogroup C by 75 to 85 invasive
meningococcal disease cases and
10 to 12 deaths.7
For the United States, the
Immunization Action Coalition
reports that the incidence dur-
ing 2005 to 2011 was 0.3 cases per
100,000 population and decreased
to an incidence of 0.18 cases per
100,000 populat ion in 2013.8
Serogroups B, C, and Y were equally
responsible for reported cases. Two
quadrivalent conjugated meningo-
coccal vaccines (MenACWY-DT
a nd Men ACW Y-CR M197
) a re
licensed in the United States, and
another is licensed in Europe
(MenACWY-TT).9 In the United
States, there are programs for both
infant and child, as well as adoles-
cent immunization.
Despite the shifting incidence of
meningitis, patients aged younger
than 2 months still have the highest
incidence of bacterial meningitis
CAUSES OF BACTERIAL MENINGITIS BY AGEBirth to 1-3 mo } Group B Streptococcus
} Gram-negative enteric bacilli
} Listeria monocytogenes
} Streptococcus pneumoniae
3 mo-2 y } S pneumoniae
} Neisseria meningitidis
} Haemophilus influenzae type b
2-18 y } N meningitidis
} S pneumoniae
From: Swanson D3; Whitney CG, et al.4
1
2 RISK FACTORS FOR MENINGITIS
NEONATE OLDER CHILDREN
Low birth weight (<2500 g) Absent or underimmunization
Prematurity (<37 wk gestation) Daycare exposure (increased 1st 2 mo;
declines after 6 mo)
Premature rupture of membranes Age <2 y
Fetal hypoxia Functional or surgical absence of spleen
Traumatic delivery Immunosuppressed (eg, HIV, malignancy,
complement deficiency, chronic steroid
use)
Urinary tract abnormalities Chronic kidney disease
Maternal GBS infection Chronic liver disease
Diabetes mellitus
Galactosemia Cochlear implant
CSF leak
Head trauma
Travel to areas with endemic meningitis
Live with large group in confined space
(dorms, military recruits)
Abbreviations: CSF, cerebrospinal fluid; GBS, group B Streptococcus; HIV, human immunodeficiency virus.From: Brouwer MC, et al10; Hjuler T, et al11; Revest M, et al.12
Page 14
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 616
peer-reviewed
primarily associated with the differ-
ent etiologies (Table 1).3,4 In this age
group, GBS and Escherichia coli are
responsible for 70% to 80% of cases.
Although routine maternal GBS and
intrapartum antibiotic treatment
have decreased early-onset GBS dis-
ease by 86%, the incidence of late-
onset disease has not changed.3
Risk factors for pediatric men-
ingitis, which also vary by age, are
presented in Table 2.10-12
Differential diagnosisA number of different diseases can
mimic meningitis, and not all chil-
dren presenting with signs and
symptoms of meningitis have the
disease. In a review of 650 children
undergoing a lumbar puncture,
there were many diseases found to
mimic meningitis symptoms such
as pneumonia, otitis media, phar-
yngitis, and gastroenteritis. In this
review study, neck stiffness was
twice as likely (50% vs 25%) and a
positive Brudzinski test was 3 times
as likely in patients diagnosed with
meningitis.13,14 Viral illness, sinus-
itis, and migraine were common
causes of headache, with no cases
of bacterial meningitis in 2 stud-
ies of patients presenting to an
emergency department with head-
ache.15,16 Although 30% of patients
presenting to an emergency depart-
ment with signs of meningismus
had meningitis, 8% had pneumonia
and 46% were diagnosed with upper
respiratory tract infection or other
self-limiting illnesses.17
Other causes of meningitis also
can mimic bacterial meningitis
such as viruses, fungi, mycobacte-
ria, and parasites. Retropharyngeal
abscess is a relatively common infec-
tious disease process that mimics
meningitis. Other infectious mim-
ickers include brain abscess, sub-
dural or epidural abscess, and
encephalitis.3
PresentationThe clinical features of bacterial
meningitis are often nonspecific
and can vary by age. The younger
the child, the less likely he or she
will present with classic symptoms
of fever, headache, and meningeal
signs. A neonate or young infant
may only present with apnea, bulg-
ing fontanel, diarrhea, fever, irri-
tability, lethargy, poor feeding,
temperature instability, or vomit-
ing.18 Symptoms are variable, how-
ever, and the patient may have fever,
hypothermia, or euthermia. Parents
may describe their infant as fussy,
jittery, or inconsolable.3 Seizure may
be a presenting sign in 20% to 50%
of cases of Hib meningitis (less in
other etiologies), but neck stiffness
is uncommon.
In older children, changes in
mentation, fever, headaches, nausea,
photophobia, and vomiting may be
present. Symptoms may evolve over
several days or a period of hours.3
Seizure may be the sole presenting
sign in patients with pneumococ-
cal meningitis. A positive Kernig
or Brudzinski sign has low sensi-
tivity for meningitis, and their
absence does not rule out meningi-
tis.18 Rash and petechiae are present
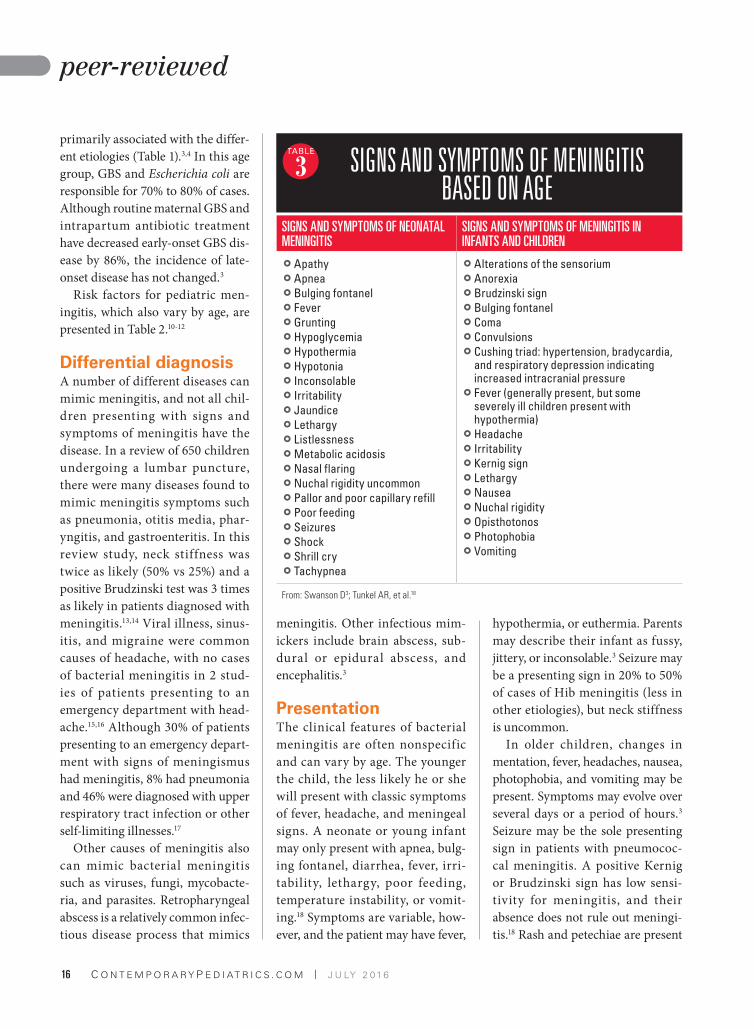
3 SIGNS AND SYMPTOMS OF MENINGITIS BASED ON AGE
SIGNS AND SYMPTOMS OF NEONATAL
MENINGITIS
SIGNS AND SYMPTOMS OF MENINGITIS IN
INFANTS AND CHILDREN
} Apathy
} Apnea
} Bulging fontanel
} Fever
} Grunting
} Hypoglycemia
} Hypothermia
} Hypotonia
} Inconsolable
} Irritability
} Jaundice
} Lethargy
} Listlessness
} Metabolic acidosis
} Nasal flaring
} Nuchal rigidity uncommon
} Pallor and poor capillary refill
} Poor feeding
} Seizures
} Shock
} Shrill cry
} Tachypnea
} Alterations of the sensorium
} Anorexia
} Brudzinski sign
} Bulging fontanel
} Coma
} Convulsions
} Cushing triad: hypertension, bradycardia,
and respiratory depression indicating
increased intracranial pressure
} Fever (generally present, but some
severely ill children present with
hypothermia)
} Headache
} Irritability
} Kernig sign
} Lethargy
} Nausea
} Nuchal rigidity
} Opisthotonos
} Photophobia
} Vomiting
From: Swanson D3; Tunkel AR, et al.18
Page 15
17J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
peer-reviewed
in about 50% of cases of invasive
disease attributed to N meningiti-
dis. Symptoms of bacterial men-
ingitis presenting in neonates and
older children are listed in Table
3.3,18 Table 4 shows how different
signs may display in different age
groups.14,19
DiagnosisBlood cultures, a complete blood
count, and electrolytes should be
obtained. White blood cell (WBC)
counts can be normal, high, and
may be low in neonates. More than
80% of patients (the percentage is
higher for Hib and lower for other
causes) not pretreated with antibiot-
ics will have positive blood cultures
with bacterial meningitis. Procalci-
tonin levels will be elevated in bac-
terial meningitis, but these cannot
distinguish between bacterial and
viral meningitis. If petechiae or low
platelet counts are present, dissem-
inated intravascular coagulation
should be considered and worked
up. Syndrome of inappropriate
antidiuretic hormone (SIADH) is
suggested by a low sodium level and
other testing.3
A lumbar puncture (LP) should
be obtained unless contraindicated
in patients because of:
} Hemodynamic instability,
} Increased intracranial pressure,
} Coagulopathy, or
} Neurologic findings indicating a
mass lesion.
Computed tomography (CT)
is not routinely needed prior to
LP. The CT findings not appar-
ent on physical exam are unlikely
to change clinical management.20
Patients with coma, papilledema,
and focal neurologic f indings
should have a CT prior to LP. The
need for CT, however, should not
delay obtaining blood cultures or
antibiotic administration. Patients
without these findings do not need a
CT prior to LP.21,22 If CT is obtained,
LP should be performed after CT if
there are no contraindications.
Spinal fluid should be sent for:
} WBC count and differential;
} Glucose;
} Total protein; and
} Gram stain and bacterial culture.
In the bacterial meningitis patient
not treated with antibiotics before
presentation, elevated WBCs, low
glucose, and elevated protein in the
spinal fluid are suggestive of bacte-
rial meningitis. Spinal f luid nor-
mals are based on the patient’s age.
Occasionally, cerebrospinal (CSF)
fluid may appear normal when the
spinal tap is performed very early in
a child’s illness.
The spinal tap results can be
altered following a traumatic tap,
making it difficult to diagnose bac-
terial meningitis. Following a trau-
matic tap, cell counts are difficult to
4 SYMPTOMS PRESENT IN MENINGITIS BASED ON AGE
SIGN 0-2 MO (%) 2-24 MO (%) 2-5 Y (%) 5-12 Y (%)
ROTHROCK
≤24 MO (%)
Fever 80 96 82 100 >95
Lethargy 40 57 36 17 87-95
Irritability 40 18 18
Altered mentation
53-78
Seizure 4 22-23
Vomiting 20 57 73 100 54-71
Focal neuro exam
5-6
Bulging fontanel
40 18
Nuchal rigidity
29 55 67 54-59
Kernig sign 7 27 33 9-11
Brudzinski sign
64 69 83 10-13
From: Levy M, et al14 (columns 2-5); Rothrock SG, et al.19
Page 16
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 618
peer-reviewed
interpret. The easiest formula is to
subtract 1 to 2 CSF WBCs for every
1000 CSF red blood cells (RBCs)/
mm3. This formula and the formula
comparing the ratio of CSF WBCs
to CSF RBCs to blood WBCs to
blood RBCs, however, should be
interpreted with caution and likely
empiric antibiotics should be started
pending culture results.3
Pretreatment with antibiotics
decreases likelihood of a positive
CSF culture. Reports demonstrate
a positive culture result in bacte-
rial meningitis with oral and par-
enteral antibiotics of only 71% and
66%, respectively. Parenteral anti-
biotics sterilize the CSF within a
couple of hours, but antimicrobial
pretreatment does not impact the
ability to diagnose bacterial menin-
gitis using cell counts, protein, and
glucose.3,23-25
Although latex agglutination
tests are available to assist in mak-
ing a diagnosis, these rarely alter
the treatment plan and the tests are
not needed in most instances.10 In
fact, such testing is no longer rou-
tinely recommended for antibiotic-
pretreated patients.3
Empiric antibioticsThe goal is to administer anti-
biotics as early as possible once the
diagnosis of bacterial meningitis
is considered. Although adverse
outcomes are not associated with
duration of symptoms prior to
treatment, delay of antibiotic
administration is associated with
poor outcomes.26,27 Empiric anti-
biotic therapy should target likely
pathogens based on the patient’s
age, underlying health conditions,
and local efficacy and susceptibility
patterns. Antibiotic choices should
have good penetration into CSF and
have bactericidal properties.3,28
Empiric antibiotics for bacterial
meningitis in the neonatal period
are primarily ampicillin plus genta-
micin or ampicillin plus cefotaxime.
The latter regimen is more com-
mon when clinicians are concerned
about increasing resistance of E coli
to ampicillin. Once an organism is
identified, the antibiotic coverage
can be tailored for the infant.3,28
Empiric antibiotics for bacte-
rial meningitis outside the neo-
natal period include vancomycin
(because of cephalosporin-resistant
pneumococci) plus either cefotax-
ime or ceftriaxone. Vancomycin
can be discontinued if the etiology
of bacterial meningitis is suscep-
tible to penicillin or cephalosporins.
Rifampin may be added in certain
situations for pneumococcal men-
ingitis, and the pediatrician should
consider consultation with an infec-
tious diseases specialist.3,28
In children with signif icant
allergic reactions to penicillins
and cephalosporins, vancomycin
plus rifampin or vancomycin plus
meropenem are options for initial
therapy.3,28
Antibiotics may be discontinued
when blood and CSF cultures are
negative in patients with an unre-
markable CSF in which bacterial
meningitis is ruled out. Children
with positive blood cultures and an
abnormal CSF, but a negative CSF
culture, are often treated as if the
CSF culture were positive. If both
CSF and blood cultures are nega-
tive but the child had an abnormal
CSF evaluation, consultation with a
pediatric infectious diseases expert
is recommended.3,28
Total duration of antibiotic ther-
apy will depend on the patient’s
age and bacterial etiology. For
uncomplicated neonatal meningi-
tis with GBS or S pneumoniae, a
14- to 21-day course of treatment is
usually sufficient. Outside the neo-
natal period, the usual course of
treatment for uncomplicated bac-
terial meningitis is 10 to 14 days
for S pneumoniae and 7 days for
N meningitidis.3,28
Dexamethasone therapySteroids are believed to decrease
neurologic complications in bac-
terial meningitis by decreasing
inflammatory response and mod-
ulating mediators that are released
when initial antibiotics result in the
lysis of cell walls.29 However, dexa-
methasone therapy outside of treat-
ment for H influenzae (for which it
is clearly indicated) remains con-
troversial. There is also a potential
concern that steroids may decrease
the effectiveness of vancomycin by
decreasing inflammation and fur-
ther reduce its already suboptimal
Empiric antibiotic therapy should target likely pathogens based on the patient’s age, underlying health conditions, and
local efficacy and susceptibility patterns.
Page 17
GERMS. VOMIT. OVER ANXIOUS
PARENTS.
REMEMBER WHEN THAT WAS ALL YOU HAD TO WORRY ABOUT?
LET DOCTORSBE DOCTORS™
NETWORK-ENABLED EHR, PRACTICE MANAGEMENT, CARE COORDINATION, AND PATIENT ENGAGEMENT SERVICES
Page 18
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 620
peer-reviewed
CSF penetration.3,28
The American Academy of
Pediatrics (AAP) Committee on
Infectious Diseases recognizes the
benefit of dexamethasone therapy
in H influenzae type b meningitis.
The AAP says clinicians can con-
sider its use in bacterial meningitis
in patients aged older than 6 weeks
after considering the risks and ben-
efits. If used, dexamethasone should
be administered with the first dose
of antibiotics because it has no bene-
fit if administered more than 1 hour
after the antibiotic.3,28
ComplicationsAmong survivors of bacterial men-
ingitis, 50% are reported to have
at least 1 complication at 5 years.
The most commonly cited bacte-
rial cause associated with complica-
tions is H influenzae. Complications
may be categorized as intellectual/
behavioral deficits (78%), neurologic
(14%), hearing loss (7%), and vision
loss (3%).30,31
Examples of intellectual and
behavioral deficits include:
} Cognitive impairment,
} Academic limitations, and
} Attention-deficit/hyperactivity
disorder.
Intellectual disability (intelli-
gence quotient [IQ]<70) is noted in
4% of survivors of bacterial menin-
gitis, and studies have found lower
IQ scores in survivors of bacterial
meningitis compared with their
siblings.30,31 In a report of 130 sur-
vivors evaluated at a single center
(average age, 8 and 6 years following
meningitis episode), children expe-
riencing meningitis did worse than
age-matched controls on assess-
ments of fine motor function, IQ
scores, and tests of school behavior,
neuropsychologic function, and
auditory figure-ground differen-
tiation, even though the children
with meningitis performed in the
average range.32-34 Onset of menin-
gitis before age 12 months is associ-
ated with poor performance on tests
requiring language and executive
skills 12 years after disease onset.33
The complications can extend
well into adulthood. In a British
cohort, survivors of meningitis at
age 16 years were more likely to
have attended special education (at
a rate of 4 times the national aver-
age); more than 3 times as likely to
not pass a General Certificate of
Secondary Education (GCSE; an
internationally recognized certifi-
cate in a particular subject); and
twice as likely to not pass core sub-
jects (eg, basic English, math, foreign
language) on a GCSE.35 Similarly,
a Danish cohort reported lifelong
impairment, with meningitis cases
less likely than controls to complete
high school, attain higher educa-
tion, or achieve economic self-suf-
ficiency.36 Finally, mood problems,
behavioral problems, socialization
problems, thought problems, and
attention problems are reported in
multiple studies years after the ini-
tial treatment of meningitis.30,37
The pediatrician needs to be
aware of the educational issues that
may be facing survivors of bacte-
rial meningitis so that parents
and teachers can be on the look-
out for problems and intervene
as necessary and as early as pos-
sible.38 Commonly reported neu-
rologic complications include
spasticity, motor def icits, and
seizure disorder.
Generalized seizures are more
likely to occur at disease onset,
while partial seizures are more
likely to occur at several days of hos-
pital admission. Seizures occurring
early in the course that are easily
controlled are not likely to lead to
neurologic sequelae. Seizures occur-
ring later in the course of treatment
or that are more difficult to control
are more likely to be associated with
permanent neurologic sequelae.38
Hemiparesis or quadriparesis is
generally associated with some sort
of intracranial pathology (eg, cere-
bral edema), which can generally
resolve over time.39
Hearing loss can be either tran-
sient or permanent. It is important
to screen for hearing loss after men-
ingitis. Risk factors for hearing loss
at presentation include:40
} S pneumoniae infection, 2 to
3 times greater compared with
other etiologies;
} Ataxia;
} Symptoms for several days prior
to admittance; and
} Absence of petechiae.
Interestingly, hemiparesis and
subdural empyema seem to have
increased in frequency after the
introduction of PCV13.41
ConclusionMeningitis remains a significant
burden in the pediatric age
group, and complications may
lead to lifelong impairment. It is
important for the pediatrician not
only to understand how bacterial
meningitis can be prevented
through vaccinations but also to
understand its risks, workup, and
treatment.
For references, go to
ContemporaryPediatrics.com/
bacterial-meningitis
Page 19
21J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
CLINICAL FEATURE
Dr Bass is chief medical
information officer and
associate professor of
medicine and of pediatrics,
Louisiana State University
Health Sciences Center–
Shreveport. The author
has nothing to disclose in
regard to affiliations with
or financial interests in
any organizations that may
have an interest in any part
of this article.
Two common questions asked of pediatri-
cians by parents of children with infections
are “When can my child return to school?”
and “How long will I be staying home with
my child?” Understanding when, how
long, and under what conditions a pediat-
ric patient with an infection is contagious
to others is an important part of disease
prevention and treatment. Similarly, the
pediatrician needs to educate parents and
educators about infection control practices
that improve prevention and decrease risk
of disease transmission.
These practices are particularly impor-
tant in regard to school-aged children
because inappropriate exclusion can lead to
a significant number of school days missed.
At times, the pediatrician may need to con-
tact a school if a child is inappropriately
excluded and provide sound reasoning as
to why exclusion is not appropriate.
This article is not a complete review
of communicable diseases or preven-
tion control measures. Rather, the article
reviews a number of diseases that do not
require exclusion; common diseases and
problems that may require some aspect
of exclusion; and a number of prevention
control measures.
Infections spread via respiratory routesWhen children cough or sneeze, aerosol-
ized droplets can be inhaled by individu-
als who are nearby, placing them at risk for
an infection. A person is more commonly
infected, however, when the droplet comes
to rest on a surface that he or she touches,
and then touches that hand to face, nose,
or mouth. As a result, if a child covers a
cough or sneezes into his/her hands, this
may increase the risk of transmission by
Infection control and prevention“When can my child return to school?”
PAT F BASS III, MD, MS, MPH
Teaching parents and educators about infection control practices can improve prevention and decrease risk of disease transmission to help keep kids in school.
Infection control And prevention
Page 20
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 622
clinical feature
contaminating surfaces with mucus
from his/her nose, eyes, or throat.1
Children should be taught to
sneeze or cough into a tissue or
paper towel. If this is not avail-
able, they should be instructed to
sneeze into the crook of the elbow.
Children should then perform good
hand-washing hygiene.
Preventing infections via direct contactChildren touch everything and
often touch their nose, face, and
mouth. Good hand hygiene pre-
vents the risk of transmission of dis-
eases through direct contact.
The Centers for Disease Control
and Prevention (CDC) recommends
a 5-step hand-washing process to
avoid getting sick and spreading
germs to others:2
Wet. Wet hands first with clean,
running water and apply soap.
Lather. Rub hands together to
lather up, focusing on the backs of
the hands, between the fingers, and
under finger nails.
Scrub. Scrub hands for at least
20 seconds. Asking children to
sing “Happy Birthday” to them-
selves twice will be about the right
amount of time.
R inse. Hold ha nds u nder
running water and not standing
water. Standing water potentially
increases risk of reinfection with
the germ or virus. Tell the child to
think of the germ/virus as circling
the drain away from him.
Dry. Dry hands with a clean
towel or let them air dry.
If access to hand-washing is
not available, hand sanitizer is an
option.
Infections not requiring exclusionIn general, school-aged children
with the conditions presented in the
Table1 do not need to be excluded
from school if they feel well enough
to participate in their regular activ-
ities, and if they do not have fever,
rash, or severe illness symptoms
requiring temporary exclusion.
Specific conditions that may require exclusionBoils, abscesses, cellulitus. Signs
and symptoms include furuncles
and carbuncles (boils) that occur in
hairy areas and contain pus. Skin
abscesses are collections of pus and
may be tender, painful, and fluctu-
ant. With cellulitis, skin is red and
tender. Fever may be present with
boils, abscesses, or cellulitus.
Incubation period depends on the
causative agent. It is spread through
person-to-person contact, with a
smaller risk of indirect spread via a
contaminated surface or object.
Staph and strep are the most
common bacteria causing boils,
abscesses, or cellulitus. These infec-
tions are contagious if the infected
area is open and draining. The child
does not need to be excluded unless
there are other symptoms (eg, fever);
if the draining lesion cannot be
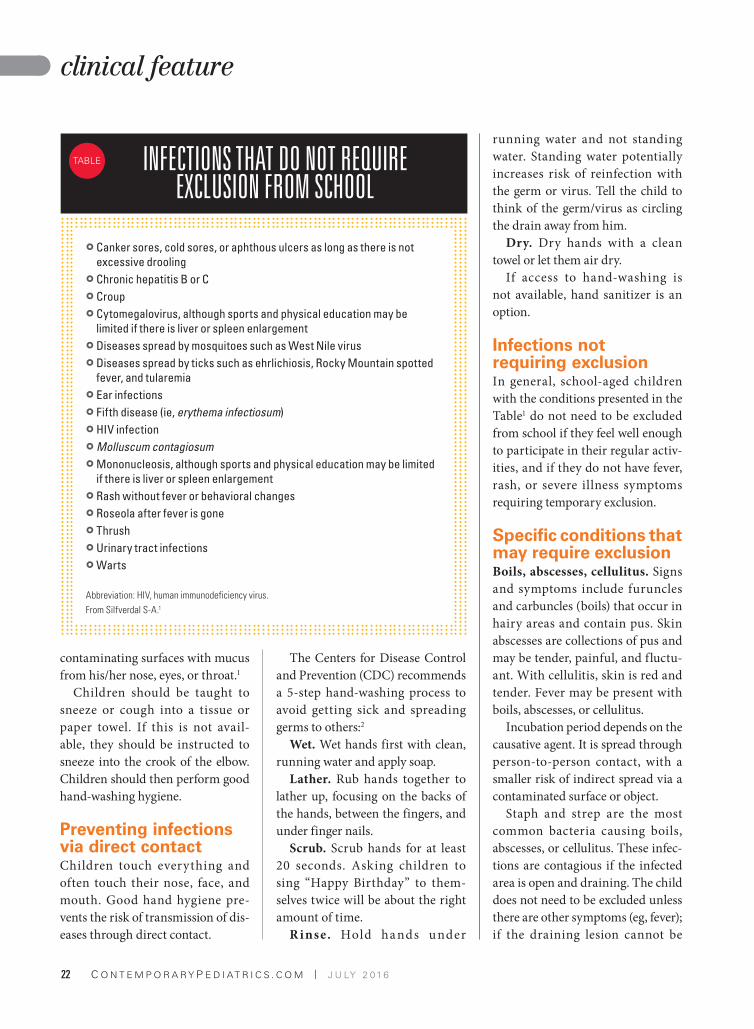
INFECTIONS THAT DO NOT REQUIRE EXCLUSION FROM SCHOOL
} Canker sores, cold sores, or aphthous ulcers as long as there is not
excessive drooling
} Chronic hepatitis B or C
} Croup
} Cytomegalovirus, although sports and physical education may be
limited if there is liver or spleen enlargement
} Diseases spread by mosquitoes such as West Nile virus
} Diseases spread by ticks such as ehrlichiosis, Rocky Mountain spotted
fever, and tularemia
} Ear infections
} Fifth disease (ie, erythema infectiosum)
} HIV infection
} Molluscum contagiosum
} Mononucleosis, although sports and physical education may be limited
if there is liver or spleen enlargement
} Rash without fever or behavioral changes
} Roseola after fever is gone
} Thrush
} Urinary tract infections
} Warts
Abbreviation: HIV, human immunodeficiency virus.
From Silfverdal S-A.1
TABLE
Page 21
23J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
clinical feature
covered; or if drainage is significant
and seeping through the bandage,
contaminating other surfaces.1
Good hand-washing is an impor-
tant way to avoid the spread of infec-
tions from child to child. Infected
children should be instructed not
to share personal items such as tow-
els. Having a methicillin-resistant
Staphylococcus aureus (MRSA)
infection or being a MRSA carrier
is not a reason for exclusion in and
of itself.
C h i c k e n p o x (v a r i c e l l a ) .
Regarding signs and symptoms of
chickenpox, after a prodrome that
may include fever, malaise, phar-
yngitis, or loss of appetite, a mac-
ular rash appears that progresses
to pruritic vesicles and then scabs.
Eruptions occur in crops, so that
a person may have findings in all
3 stages.
The incubation period is usually
from 14 to 16 days. As to how it is
spread, the disease is communicable
from 48 hours before the appear-
ance of the rash until the vesicles
have dried and no new vesicles are
forming. It is spread through aero-
solized droplets or direct contact
with fluid from a skin vesicle.
Although immunization has
made these infections much less
common in the pediatrician’s office
(vaccine is ~70% to 90% effective in
preventing chickenpox), infections
may still be seen in unimmunized
patients, or atypical presentations
seen in immunized or underimmu-
nized populations. School exclusion
is appropriate for active cases, and
school systems also may exclude
at-risk, unimmunized children.
Children with uncomplicated vari-
cella infections may return to school
when the rash has crusted or no new
lesions are present in 24 hours in
an appropriately immunized child
without crusts.3 This often occurs
about 6 days after the start of the
rash.
Conjunctivitis (bacterial and
viral [pinkeye]). Signs and symp-
toms include redness of the eye
and discharge. Discharge may be
mucopurulent or clear. Eyes are
often matted shut in the morning.
Patients also may report itching,
pain, burning, sandy, or gritty feel-
ing in the eye.
The incubation period for bacte-
rial conjunctivitis is 24 to 72 hours,
whereas for adenovirus (the most
common cause of viral conjunctivi-
tis) it is 5 days. As to how it is spread,
both bacterial and viral pathogens
are highly contagious. Spread is via
direct contact with discharge from
the eye or indirect contact from a
contaminated surface or object.
Although the safest preven-
tive measure would be to exclude
children until the discharge has
resolved, this is not feasible. Hand
hygiene is important, especially
when touching the eyes, nose, or
mouth. Infected individuals should
not share towels, cosmetics, or
other personal items. Many schools
require 24 hours of antibiotics for a
child with an eye discharge before
the child can return to school.
This is appropriate to decrease risk
of infecting others with bacterial
conjunctivitis, but it will not impact
risk of spread of viral conjunctivi-
tis. If concerned about school sys-
tems requiring antibiotic treatment,
explaining that pinkeye is like the
common cold and that exclusion
is not appropriate for the common
cold may get the child back in school
without an unneeded treatment.1
D i a r r h e a l i l l n e s s . S i g n s
and symptoms of diarrheal ill-
ness include 3 or more large,
loose (increased water content or
decreased form) stools per day.
Patients often have other symptoms
such as nausea or vomiting.
Incubation period depends on
the causative agent. It is spread by
person-to-person contact via fecal-
oral route.
Good hand-washing and per-
sonal hygiene are paramount in the
prevention and control of diarrheal
illnesses. If good hand-washing
and personal hygiene are not prac-
ticed, there is an increased chance of
spread of illness between children,
particularly if food is contaminated
and shared among students.
Most cases of diarrhea are viral,
and a pathogen is never identified.
An etiology for bloody diarrhea is
more commonly sought and may
identify a pathogen. Younger chil-
dren who are not able to reliably
toilet and practice good personal
hygiene should stay home until
diarrhea has resolved for 24 hours.
Staph and strep are the most common bacteria causing boils, abscesses, or
cellulitus. These infections are contagious if the infected area is open and draining.
Page 22
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 624
clinical feature
Older children who are able to
reliably toilet and practice good
personal hygiene, and who do not
have other symptoms requiring
exclusion (eg, fever), do not need
to stay home unless the diarrhea is
uncontrollable.
Children who have experienced
2 or more episodes of vomiting in
a 24-hour period related to acute
gastroenterit is should remain
excluded from school. Children may
return to school when the child has
no accidents using the toilet and
stool frequency is no more than
2 stools per day more than the
child’s normal stooling frequency.4
The National Institute for Health
and Care Excellence has a more
conservative recommendation and
advises exclusion until 48 hours
after the last episode of diarrhea.5
If an enteric pathogen is identi-
fied as the cause of diarrhea, these
additional exclusions will apply:1
} Shigella: the child should be
excluded until diarrhea resolves
and 1 or more stool cultures are
negative. The requirements will
vary by state.
} S h i g a t o x i n - p r o d u c i n g
Escherichia coli: the child should
be excluded until there are 2 neg-
ative cultures 24 hours apart.
Additionally, state and local
jurisdictions may have differ-
ent laws governing exclusion and
return to school.
Strep throat. Signs and symp-
toms of strep throat include fever;
sore throat; variable throat exam
that may or may not reveal visible
pus spots; or tender and swollen
lymph nodes.
Incubation period is 1 to 3 days.
Strep throat is spread by large
respiratory droplets from a child
with an infection (or a carrier), or
direct contact with nasal/throat
secretions. Indirect transmission is
uncommon.
Strep throat can cause real havoc
in the lives of families with dual
working parents. One parent needs
to leave work early and bring a child
to the pediatrician’s office, and then
current guidelines and many school
systems advise exclusion until the
completion of 24 hours of antibiot-
ics and avoidance of close contact
with other students.4
A 2015 article published in the
Pediatric Infectious Disease Journal,
however, found that a single dose
(50 mg/kg) of amoxicillin led to
91% of children having undetectable
testing the next morning. This led
the investigators to conclude that
children with strep throat treated by
5 pm may return to school the next
day if afebrile and improved.6
Infections are a common reason
for school exclusion. Pediatricians
need to be comfortable discussing
appropriate exclusion and willing
to intervene if children are being
inappropriately excluded from
school or daycare.
R E F E R E N C E S
1. Silfverdal S-A. Book review. Managing Infectious
Diseases in Child Care and Schools: A Quick
Reference Guide. 3rd ed. Aronson SS, Shope TR, eds. Elk Grove Village, IL: American Academy of Pediatrics; 2013. Acta Paediatr. 2015;104(5):535.
2. Centers for Disease Control and Prevention. When and how to wash your hands. Available at: http://www.cdc.gov/handwashing/when-how-handwash-ing.html. Updated September 4, 2015. Accessed June 23, 2016.
3. American Academy of Pediatrics. Summaries of infectious diseases: varicella-zoster virus infections. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee on
Infectious Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2015:846-860.
4. American Academy of Pediatrics. Recommendations for care of children in special circumstances. Children in out-of-home child care: recommendations for inclusion or exclusion. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report
of the Committee on Infectious Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2015:132-151.
5. National Institute for Health and Care Excellence. Diarrhoea and vomiting caused by gastroenteritis in under 5s: diagnosis and management. https://www.nice.org.uk/guidance/cg84. Published: April 22, 2009. Accessed June 1, 2016.
6. Schwartz RH, Kim D, Martin M, Pichichero ME. A reappraisal of the minimum duration of antibiotic treatment before approval of return to school for chil-dren with streptococcal pharyngitis. Pediatr Infect Dis
J. 2015;34(12):1302–1304.
7. Clark RC. ‘No-nit’ policy adopted to battle lice in schools. Star News. February 4, 2014. Available at: http://www.starnewsonline.com/article/20140204/articles/140209863?tc=ar. Accessed June 23, 2016.
8. American Academy of Pediatrics. Recommendations for care of children in special circumstances. School health: infections spread by direct contact. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book: 2015 Report of the Committee on
Infectious Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2015:156-157.
9. American Academy of Pediatrics. Summaries of infectious diseases: pediculosis capitis. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red
Book: 2015 Report of the Committee on Infectious
Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2015:597-600.
Investigators conclude that children with strep throat treated by 5 pm may return
to school the next day if afebrile and improved.6
For additional resources, go to
ContemporaryPediatrics.com/
infection-control-prevention
Page 23
25J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
PEER-REVIEWED FEATURE
Dr Westers is clinical
psychologist and assistant
professor, Children’s
Health Children’s Medical
Center Dallas, Texas,
and University of Texas
Southwestern Medical
Center, Dallas.
Dr Muehlenkamp is
associate professor of
psychology, University of
Wisconsin–Eau Claire.
Dr Lau is assistant
professor, Children’s
Health Children’s Medical
Center Dallas, Texas,
and University of Texas
Southwestern Medical
Center, Dallas. Drs Westers
and Muehlenkamp have
nothing to disclose in
regard to affiliations with
or financial interests in
any organizations that
may have an interest in
any part of this article.
Dr Lau reports that she
has ownership interest
in Gilead, which does not
affect her ability to be
unbiased in this article.
Medical providers, particularly pediatri-
cians, are often the first to learn that their
patients have been intentionally harming
themselves.1,2 Nonsuicidal self-injury
(NSSI) is defined as directly and
intentionally inflicting damage
to one’s own body tissue with-
out intention of suicide and
not consistent with cultural
expectations or norms.3 Epide-
miologic studies of community
samples indicate an approximately
5.9% lifetime prevalence of NSSI among
adults and 18% among adolescents, with
rates even higher among psychiatric treat-
ment-seeking youth.4-6 Nevertheless, only
1 in 4 clinicians routinely inquires about
and addresses NSSI with his or her adoles-
cent patients.7
Several authors have provided sugges-
tions for how healthcare providers can
respond to patients who self-injure.1,2,8,9 We
developed the SOARS model for medical
providers to use as a brief screening and
assessment of NSSI. Each letter of SOARS
represents an area to assess: Suicidal ide-
ation; Onset, frequency, and methods;
Aftercare; Reasons; and Stage of
change (Figure 1). Using theory,
research, and consideration of
real-world practice, we high-
light the most important ques-
tions to ask, the reasoning for
these questions, and recommen-
dations for how to ask them. Before
screening and assessing NSSI, however,
an important step for medical providers
is to first evaluate their own values and
beliefs about NSSI.8
Being empathic toward individuals who
engage in a behavior typically considered
contrary to protecting one’s health can be
difficult at times. Any negative biases, mis-
conceptions, or judgments about NSSI (eg,
manipulative or done primarily for atten-
tion) may result in a poor response and lack
SOARS modelRisk assessment of nonsuicidal self-injuryNICHOLAS J WESTERS, PSYD; JENNIFER J MUEHLENKAMP, PHD; MAY LAU, MD, MPH
A new assessment tool helps physicians screen adolescents for self-harming behaviors, then develop a treatment plan or referral to therapy for these patients.
SOARS Model
FAST FACT
Approximate lifetime prevalence
of NSSI among adolescents is
18%.7
Page 24
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 626
peer-reviewed
of empathy for patients struggling
with this behavior. Providers who
are aware of their own emotions and
perspectives are better able to moni-
tor them and can help their patients
more effectively.8
Screening for NSSIProviders who use the HEEADSSS
assessment [Home environment,
Education and employment, Eating,
peer-related Activities, Drugs, Sex-
uality, Suicide/depression, Safety
from injury and violence] to obtain
a psychosocial history from ado-
lescents would likely find the most
opportune time to screen for NSSI
prior to screening for suicide.10 It
may seem easiest to simply ask if
they have ever hurt themselves on
purpose without intending suicide.
Asking about NSSI using a broad
question like this, however, typically
results in lower prevalence rates of
the behavior than does asking about
NSSI in a checklist format.5 We rec-
ommend normalizing the behav-
ior (eg, “I know that some people
who experience stressors similar to
yours think about hurting them-
selves on purpose without intend-
ing suicide.”), asking them directly
about it (“Have you ever hurt your-
self on purpose without intending to
end your life or attempt suicide?”),
and finishing the question by list-
ing common forms of NSSI similar
to checklist format (“like cutting,
biting, burning, or hitting?”). If
patients disclose engaging in NSSI,
providers can do a brief assessment
using SOARS. Similar to asking
about suicide, no iatrogenic effects
have been shown from asking about
NSSI.11
Assessing NSSI using the SOARS modelSUICIDAL IDEATION
Because NSSI, by nature, is not sui-
cidal, it should not be confused
with or misinterpreted as a suicide
attempt. Some adolescents fear that
disclosing their NSSI will unneces-
sarily lead to an inpatient psychi-
atric hospitalization. Nevertheless,
immediately after screening for
NSSI, and as part of the HEEADSSS
assessment, it is important to assess
any suicidal ideation concurrent or
in tandem with NSSI.
This is important for at least 2
reasons: For those who engage in
the behavior, using NSSI as a cop-
ing strategy to avoid suicide has
been shown to be among the stron-
gest risk factors for attempting sui-
cide, and a history of NSSI has
been shown to be among the stron-
gest risk factors for future suicide
attempt, and for depressed youth,
even more so than a history of a past
suicide attempt.12-15
How to ask. To obtain the most
honest response from adolescents
who engage in NSSI and to decrease
any anxiety that they may be alone,
it is best to normalize that some
young persons who self-injure think
about suicide when they engage in
NSSI. So, the question can be posed
as: “I know self-injury isn’t usually
about suicide, but some people may
think about suicide when they self-
injure. Do you ever think about pur-
posely ending your life when you
self-injure?
SOARS ASSESSMENT POCKET CARD
Responding to nonsuicidal self-injury (NSSI) using SOARS assessment
Have you ever hurt yourself on purpose without intending to end your life or
attempt suicide, like cutting, biting, burning, hitting?
Suicidal ideation
} I know self-injury isn’t usually about suicide, but some people may think
about suicide when they self-injure. Do you ever think about purposely
ending your life when you self-injure?
Onset, frequency, and methods
} When was the first/most recent time?
} How many times a week/month do you self-injure?
} What do you typically do or use?
Aftercare
} How do you take care of the wounds afterward?
} Have you ever hurt yourself so badly that you needed medical attention,
even if you never got it?
Reasons
} It sounds like this has been helpful for you. What does it do for you?
(In what ways does it help?)
Stage of change
} Is this something you would like to stop?
} Have you ever considered stopping?
1
Page 25
27J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
peer-reviewed
ONSET, FREQUENCY, AND
METHODS
It is important to ask about onset of
NSSI (to determine duration); how
many episodes of NSSI in which
adolescents have engaged (to deter-
mine frequency); and what they typ-
ically use to self-injure (to determine
number of methods). Each of these
characteristics has been shown to
be positively associated with an
increased risk for suicide.
According to the interpersonal-
psychological theory of suicidal
behavior (IPTS), individuals die
by suicide because they have both
the desire to die (based on feelings
of perceived burdensomeness and
perceptions of not belonging or fit-
ting in with anyone, which are often
symptoms of depression) and the
capability to act on that desire.16 The
capability for suicide is acquired
over time, theoretically, as a result
of exposure to painful and provoca-
tive experiences (eg, childhood mal-
treatment, combat exposure, past
suicide attempt, and NSSI) that
cause a decreased fear of death and
an increased tolerance of physical
pain.
According to the IPTS and NSSI
research, individuals may first
engage in NSSI without ever before
having considered suicide. Over
time, individuals who repetitively
engage in NSSI have a greater risk
of suicide because of pain habitua-
tion and decreased fear of death.3,17
Research suggests that risk for a
suicide attempt among those who
self-injure peaks between 20 and
50 lifetime episodes of NSSI and
then declines afterward, likely
because the NSSI has become an
effective coping strategy for those
individuals.12
Using a greater number of meth-
ods for NSSI (eg, cutting, carving,
burning, hitting) is also related to
suicide attempts, especially when
frequency of NSSI is high.3,18,19 Each
type of method may elicit a different
kind of pain (eg, tearing, burning,
bruising) and may independently be
classified as a painful and provoca-
tive experience, thereby increasing
acquired capability for suicide via
both habituation to various forms of
pain and decreased fear of death.19
How to ask. To obtain an idea of
how long an adolescent has engaged
in NSSI, simply ask “When was
the first time you [cut] yourself?”
followed by “When was the most
recent time?” Similar to assessing
other high-risk behaviors using
the HEEADSSS format, providers
should be specific when assessing
frequency and lifetime number of
episodes of NSSI. Rather than ask-
ing vaguely (eg, “How often . . .”),
we recommend that providers be
specific and first ask “How many
times a week do you self-injure?”
or “How many times a month do
you self-injure?” Asking about
increased severity is also impor-
tant, particularly because this may
indicate growing tolerance for pain
and acquired capability for a suicide
attempt: “Have you found that you
have begun to self-injure more often
or more deeply than a year ago (or
when you first started)?” At least
1 study found that an absence of
pain during NSSI is linked to an
elevated risk for suicide attempts.3
To determine the number of dif-
ferent types of methods, providers
can ask “What do you typically do
or use?” If an adolescent responds
that he or she cuts using a blade
from a small pencil sharpener, the
razor from the shower, or a piece
of glass, these are all considered
1 method (ie, cutting), and provid-
ers can then ask about other meth-
ods such as those assessed during
the initial screening question.
AFTERCARE
Medical providers are often in the
best position to screen for NSSI and
to determine severity of injury. Poor
wound care can increase risk for
infection and even scarring. Some
individuals might hurt themselves
more severely than intended and
require medical attention, although
some may not seek it out.
How to ask. As with all assess-
ment questions about NSSI, it is best
to use a low-key and nonjudgmen-
tal demeanor that shows a respect-
ful curiosity.20 Providers can ask
“How do you typically take care of
the wounds afterward?” and “Have
you ever hurt yourself so badly that
you needed medical attention, like
stitches, even if you never got it?”
Over time, individuals who repetitively engage in NSSI have a greater risk of
suicide because of pain habituation and decreased fear of death.3,17
Page 26
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 628
peer-reviewed
Some providers have suggested that
if an injury is discovered on assess-
ment, they should ask “Do you have
any other wounds?” and then state
matter-of-factly “I need to assess
your wounds so we can be sure to
provide the proper care and avoid
infection.”9
REASONS
Individuals who engage in NSSI
typically do so because it is helpful
as a short-term solution or relief, or
serves some particular function(s),
such as to deal with stress or over-
whelming emotions, in response
to feeling emotional numbness, to
punish themselves, or to commu-
nicate their feelings to someone
(Table 1). Determining the reasons
the adolescent engages in NSSI will
likely be the primary focus of the
assessment, particularly because
this will guide providers in their
brief intervention and help deter-
mine the treatment plan.
For medical providers who have
limited time to spend with their
patients, a brief intervention may
simply mean assessing severity
of NSSI and safety, followed by a
referral for therapy. A follow-up
telephone call or an in-person acute
care follow-up visit within 2 to
3 weeks may be indicated to deter-
mine if the patient or parent has
identified a therapist. For medical
providers who have an additional
few minutes to provide medical
counsel, a brief intervention may
include specific targeted advice
regarding alternative coping strat-
egies based on function of the
behavior.
For example, if the adolescent’s
purpose for the behavior is to cope
with overwhelming emotional
distress, an important element of
the brief intervention is exploring
additional helpful strategies that he
or she can utilize before or instead
of engaging in NSSI. Focus should
be on bolstering healthy coping
skills rather than simply removing
unhealthy ones; addition is better
(and easier) than subtraction.20 If
the purpose of self-injuring is to
communicate the adolescent’s feel-
ings to parents or friends, a brief
intervention may include exploring
alternative strategies for effectively
communicating his or her emo-
tional needs. Essential elements in
all brief medical counsel include
validating that the adolescent’s NSSI
seems helpful, sensitively expressing
1 STRATEGIES FOR BRIEF MEDICAL INTERVENTION
REASON FOR NSSI BRIEF INTERVENTION EXAMPLE RESPONSE
To reduce emotional tension and stress
Identifying alternative strategies to reduce
emotional distress (eg, talking to a friend/
parent, journaling, drawing, exercising,
using relaxation techniques).
“What are some other ways you can manage
when you’re feeling overwhelmed, even if they
don’t work as quickly as self-injury?”
To feel something due to feeling numb or empty
Identifying alternative strategies for
generating feelings (eg, taking a cold
shower, eating a hot pepper) or discussing
how patients might tolerate numbness for
the time being (eg, accepting temporary
emotional numbness).
“What are some other ways you can feel
something when you’re feeling numb or empty,
even if they don’t work as quickly as self-
injury?”
To communicate with others Identifying alternative strategies for
communicating emotional needs
(eg, asking for encouragement, advice,
a hug, to sit in silence together, to do
something together).
“How might you ask your mom/dad/friend for
emotional support and help without hurting
yourself or telling them that you’re going to?”
To self-punish Introducing concept of self-forgiveness
and acceptance of imperfections.
“Sounds like you’re experiencing enough of
life’s punishments right now. Instead of adding
more punishment to yourself, what would it be
like to allow yourself some room for mistakes
or self-forgiveness?”
Abbreviation: NSSI, nonsuicidal self-injury.
Page 27
Now available in a 34-oz pump
Show How Much You Care
for Sensitive Skin
*Directly Esterifi ed Fatty Isethionate.
Dove and NutriumMoisture are Registered Trademarks.
© 2016 Unilever
Dove Sensitive Skin
Bar and Body Wash
,���&�%������!#�� �� %$�� ��*!&#���+����
patients
,����"�� �$��$%��#�������.%�����%%*������
�!$%�!�%� ��)%#��%����#!��%���$%#�%&��
�!# �&���&#� ������ $� �.�%���
1-to-1 ratio
,���!#�&��%���(�%���� ����!��� � ��
�������$&#���%� %��!�"��)�(�%��%���
$�� ���� %�������"���$%��#���������%!����"�
"#�$�#'��%���$�� ���##��#
Page 28
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 630
peer-reviewed
concern about the behavior, kindly
advising against it for health rea-
sons, exploring alternative strate-
gies, and offering to make a referral
for therapy.
Unfortunately, many adolescents
who resort to NSSI cannot readily
integrate information on alterna-
tive, healthier coping strategies. In
these situations, listening to them
without judgment, empathizing
with their emotional distress, and
exploring openness to therapy may
be therapeutic and the best way to
respond if an adolescent is over-
whelmed in the moment. Simply
telling an adolescent to stop self-
injuring or reacting negatively may
inadvertently communicate to him
or her that it is not safe to talk about
the behavior, and the adolescent
may choose to continue to engage in
NSSI but no longer talk about it with
his/her provider.
The more reasons behind engag-
ing in NSSI, the greater the risk
for suicide.12 Reasons for NSSI that
are most strongly related to suicide
attempts include: to avoid suicide,
to cope with self-hatred, and to end
dissociation or feel something other
than emptiness or profound anxi-
ety. Many physicians who see ado-
lescents take confidentiality very
seriously and discuss confidentiality
and its limits at the beginning of
the appointment. Each adolescent is
unique, so breaking confidentiality
about NSSI behavior is often based
on the clinical judgment of the med-
ical provider.1 At this point in the
SOARS interview, clinicians will
likely have a good idea of how safe
or at risk an adolescent who self-
injures is for suicidal behavior. If
the purpose of an adolescent’s NSSI
is to avoid suicide, we recommend
that providers break confidentiality
and involve parents. This is impor-
tant because no one may know if
or when the NSSI becomes ineffec-
tive as a strategy to avoid suicide,
and then the adolescent decides to
attempt suicide.
How to ask. It is important to
first acknowledge how NSSI is not
the true problem for those who
engage in the behavior but instead
a solution to feelings coming from a
deeper problem. Validating that it is
a helpful way to cope is not the same
as agreeing with the behavior or
condoning it. Thus, we recommend
that providers ask about the reasons
for engaging in NSSI by stating “It
sounds like this has been helpful
for you. What does it do for you (in
what ways does it help you)?”
However, NSSI does not help all
adolescents. These young persons
typically respond that they heard
about NSSI as an effective coping
2 COMMON APPROACHES FOR ADDRESSING NSSISTRATEGY GENERAL FOCUS SNAPSHOT IN PRACTICE
Motivational interviewing (MI)
Respectfully guiding individuals to engage
in healthy behavioral change by resolving
ambivalence and eliciting motivation for change
Exploring the pros and cons of continuing to
engage in NSSI and the pros and cons of ceasing
NSSI
Cognitive behavioral therapy (CBT)
Modifying thoughts and behaviors to improve
mood and emotions
Differentiating between feelings (eg, anxiety) and
behaviors (eg, NSSI) and modifying the thought
that one must self-injure to improve mood
Dialectical behavior therapy (DBT)
Mindfulness and balancing dialectical (ie,
philosophy of opposing ideas) tension between
acceptance and change by teaching distress
tolerance, emotion regulation, and interpersonal
effectiveness skills
Identifying reason(s) for engaging in NSSI,
nonjudgmentally accepting associated
distressing emotions, and engaging in alternative,
healthier behavior
Emotion-regulation group therapy (ERGT)
Addressing NSSI by learning to regulate
emotions through understanding and acceptance
of emotions, control of behavior, and value-
directed living (ie, identifying meaningful things
in life and making choices consistent with those
values)
Identifying and pursuing meaningful activities in
life and inhibiting impulsive behavior (eg, NSSI),
even if it means experiencing negative emotions
along the way
Abbreviation: NSSI, nonsuicidal self-injury.From: Rollnick S, et al22; Beck AT, et al23; Linehan MM24; Gratz KL, et al.25
Page 29
31J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
peer-reviewed
strategy, tried it once or twice, found
that it was unhelpful, and stopped
engaging in it. Among those who
have already ceased the behavior,
affirming their choice of healthier
coping strategies is sometimes all
that is necessary to prevent future
episodes.
STATE OF CHANGE
Although many adolescents who
self-injure are not ready to stop
or cannot stop their NSSI, some
desire to stop their self-injury but
are unsure how. Some see no need
to change at all. The transtheoreti-
cal model of behavior change may
be a helpful way of conceptualizing
whether adolescent patients want to
change or are ready to change.21 For
those who are not yet ready to give
up their NSSI, using motivational
interviewing can be a helpful way
of collaborating with these adoles-
cents, guiding them toward moti-
vation for change and exploring the
pros and cons of life without NSSI
(Table 2).22-25 Medical providers do
not need to go into great depth dur-
ing this conversation, but posing a
question about readiness for change
is a good first step for the adoles-
cent to consider how he or she might
stop self-injuring and to determine
if there is a desire to do so.
How to ask. After an adolescent
has disclosed the reasons for his
or her NSSI and the functions it
serves, a provider can ask, “Is this
something you would like to stop?”
or, “Have you ever considered stop-
ping?” If the adolescent responds
that he or she would like to stop
and needs help, then referral to a
mental health professional who has
experience treating adolescents who
self-injure is appropriate. If the ado-
lescent responds that he or she sees
no need to change, then brief medi-
cal counsel could focus on exploring
the pros and cons of the behavior
(eg, perhaps it is harming his/her
relationship with someone impor-
tant, such as parents). The adoles-
cent’s response may also provide a
sense of the likelihood that he or
she will follow up with a referral to a
mental health professional.
SummaryClinicians can choose to spend
much more time discussing and
assessing NSSI, but the purpose
behind the SOARS model for assess-
ing NSSI is to be able to conduct a
brief screening and assessment of
NSSI by recommending what ques-
tions are most important to ask, why
they are important to ask (based on
empirical research and theory), and
how to ask them. Primary focus
should be on the reasons behind
the behavior, which will inform the
brief intervention or counsel medi-
cal providers may give to their ado-
lescent patients. All brief medical
counsel should validate the utility
of NSSI for each patient, sensitively
express concern about the behavior,
kindly advise use of healthier strat-
egies for coping (addition is better
than subtraction), and offer a refer-
ral to therapy.
If using the full SOARS assess-
ment model is not realistic in
a given scenario because of time
constraints, an even shorter ver-
sion (Suicidality, Aftercare, Reasons
[SAR]) can be used that addresses
the 3 most important assessment
questions: Suicidality: “Are you
thinking about suicide when you
self-injure?”; Aftercare: “How do
you take care of your injuries?”;
Reasons: “In what ways is this help-
ing you?” (Figure 2).
Although no empirically sup-
ported treatment targeted spe-
ci f ica l ly for NSSI yet ex ists
(psychotherapeutic or pharmaco-
logic), most treatments that help
patients with NSSI have a tendency
to address the context in which the
behavior occurs (eg, depression,
anxiety, emotion dysregulation).2
As a result, referrals to experts
with a broad background including
empirically supported treatments
such as cognitive behavioral therapy
(CBT), dialectical behavior therapy
(DBT), or emotion-regulation group
therapy (ERGT) will likely be most
helpful (Table 2).23-25
For references, go to
ContemporaryPediatrics.com/
SOARS-for-NSSI
SAR: 3 KEY QUESTIONS
Suicidality Aftercare Reasons
Are you thinking
about suicide when
you self-injure?
How do you
take care of
your injuries?
In what ways
is this helping
you?
2
Page 30
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 632
HOSPITAL ZONE
Ms Hilton is a medical
writer who has covered
health and medicine for
25 years. She resides in
Boca Raton, Florida. She
has nothing to disclose in
regard to affiliations with
or financial interests in
any organizations that may
have an interest in any part
of this article.
The misconception that children born
with cleft lip, cleft palate, or both need
only a single surgery to address their cleft
can leave patients with a lifetime of phys-
ical and emotional challenges. Pedi-
atricians who encounter children
with these facial differences should
encourage parents and caregiv-
ers to pursue a focused, long-
term, multidisciplinary approach
to treating and managing cleft lip
and/or palate because all affected
children benefit.1
Cleft lip and palate is more than a plas-
tic surgery issue, according to Karla A.
Haynes, RN, MPH, MS, CPNP, pediatric
nurse practitioner, at Children’s Hospital
Los Angeles Craniofacial and Cleft Center,
California, one of the country’s largest
multidisciplinary centers for children born
with congenital facial differences, such as
cleft lip, cleft palate, and other craniofacial
conditions.
“The best practice is a multidisciplinary
evaluation, which can be an issue because,
sometimes, people who aren’t very famil-
iar with this patient population might
see craniofacial abnormalities as a plastic
surgery problem. They may not under-
stand that this is a chronic condition, and
that there is a need for ongoing monitor-
ing and care throughout childhood,”
Haynes says.
Cleft lip and palate facts and figuresOccurring in about 1 in 600 live
births in the United States, clefts
involving the lip and/or palate are
among the most common congen-
ital anomalies affecting the craniofacial
region.1,2
Oral facial clefts vary in incidence
according to gender and ethnic back-
ground. Clefting is known to occur more in
males, and Asians and Native Americans
have the highest birth prevalence, with 1
in 500 births. The lowest prevalence is in
people of African descent.2
Cleft palate and cleft lip often occur
together. About two-thirds of those
affected have clefts of the lip and palate.2
Cleft lip alone is more likely to occur
than cleft palate alone, but when it does
Cleft lip and palateTeam approach to treatmentLISETTE HILTON
A multidisciplinary center for children born with cleft lip, cleft palate, or other craniofacial conditions ensures that patients emerge with little evidence of deformity.
Facial Clefts
Karla A. Haynes,
RN, MPH, MS,
CPNP
Page 31
33J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
hospital zone
PH
OT
OS
PR
OV
IDE
D B
Y K
AR
LA
HA
YN
ES
, R
N,
MP
H,
MS
, C
PN
P, C
HIL
DR
EN
’S H
OS
PIT
AL
LOS
AN
GE
LES
.
occur, cleft palate is more common
among females.
Because many of the syndromes
associated with clefting are inher-
ited in an autosomal dominant pat-
tern, each offspring of an affected
person has up to a 50% chance
of inherit ing the syndrome. 2
Recurrence of isolated cleft is low,
however—around 2% to 6%. The
risk increases as the number of
affected persons in a family grows.
What’s meant to happen in utero, doesn’tThe lip normally fuses by 35 days
in utero.3 The lip’s failure to fuse
can impair subsequent closure of
the palatal shelves, which typically
close in the 8th to 9th week.
Although the cause of cleft
l ip sequence typical ly is
a myster y, clef ts occur
in syndromic or isolated
categories.2 Skeletal, cra-
niofacial, eye, and other
anomalies generally occur
with syndromic clef ts .
Cleft-associated syndromes
can originate from intrauterine
exposures to alcohol, isotretinoin,
cigarette smoke, and more, as well
as result from genetic disorders.
Children with clefting are at
higher risk for abnormal tooth
development, as well as mild ocular
hypertelorism, hypernasal speech,
speech delay, recurrent otit is
media, and hearing loss.3
Often detected in utero
Typically, community obstetrics
providers will see a fetal cleft
lip on ultrasound (the cleft
palate generally is not so vis-
ible), according to Haynes.
Cleft lip not detected
before birth should be seen
in the immediate postnatal
period. Cleft palate might
be diagnosed later, during a rou-
tine newborn intraoral examina-
tion, especially if the newborn has a
milder variant, such as bifid uvula or
submucosal clefting. Pediatricians
and others who diagnose cleft palate
should conduct a systemic examina-
tion because every sixth newborn
that has cleft palate is at higher risk
for other malformations, including
S FIGURE 1 Patient with an
unrepaired right unilateral
complete cleft lip and palate. She is
aged 19 days in this photo.
S FIGURE 2 Patient is 5 months
postoperative following cleft lip
repair. She is aged 8 months.
S FIGURE 3 Patient is 3 years postoperative from her palate repair surgery and
2 years postoperative from lip revision surgery.
Alessia Johns,
PhD
Page 32
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 634
hospital zone
congenital heart disease or urinary
tract anomalies.1
To differentiate between an
isolated or syndromic cleft, the
pediatrician should consult with
a craniofacial team and geneticist,
and take a careful family history of
clefts and features of clefting syn-
dromes, including skin disorders
and speech abnormalities.2 The
pediatrician should also ask about
prenatal exposures. In addition,
assessments for vision and hearing
should be done as early as possible.
Immediate concernsBecause cleft palate prevents an
infant from effectively sucking,
these babies have trouble with
breastfeeding. Pediatricians can
recommend that mothers pump
their breast milk and give it to
their babies using a special nip-
ple designed to facilitate feeding
infants with clefting.
The good news is breastfeeding
can be successful in babies with iso-
lated cleft lip only.2 However, par-
ents should know that these babies
tend to take in more air while feed-
ing and might require more frequent
burping. With palatal openings or
dysfunction, nasal regurgitation
also can occur.
Pediatricians should diligently
monitor these children’s growth and
more because children with palatal
clefts are at significantly greater risk
for eustachian tube dysfunction,
recurrent otitis media, and conduc-
tive hearing loss.2
According to Haynes, feeding
and growth can be significantly
impaired and babies can really
struggle to gain weight, with a small
percentage requiring admission for
failure to thrive until families mas-
ter the feeding techniques. This can
be challenging, she says.
Takes a villageChildren’s Hospital Los Angeles
Craniofacial and Cleft Center fea-
tures 13 subspecialty disciplines on
its craniofacial team. The full list
of specialty providers is plastic sur-
gery, nurse practitioners, ears/nose/
throat, audiology, speech pathol-
ogy, genetics, dentistry, ortho-
dontics, psychology, social work,
pediatrics, pulmonology, and a reg-
istered dietician. PH
OT
OS
PR
OV
IDE
D B
Y K
AR
LA
HA
YN
ES
, R
N,
MP
H,
MS
, C
PN
P, C
HIL
DR
EN
’S H
OS
PIT
AL
LOS
AN
GE
LES
.
S FIGURE 5 Patient is 6 weeks postoperative following a sphincter
pharyngoplasty (not visible) to address hypernasal speech. She is aged 7
years 9 months in this photo.
S FIGURE 4 Patient is now 5 years postoperative following cleft lip revision.
She is aged 7 years 3 months in this photo.
Page 33
THE RIGHT BALANCE FOR BARRIER PROTECTION AND SKIN HEALING INGREDIENTSTo learn more or to request samples and coupons for your patients, please visit www.summers-direct.com/samples.
PROFESSIONALLY RECOMMENDEDPROBLEM-SOLVING PRODUCTS
ECZEMA
HEALINGAwarded the Seal of Acceptance
by the National Eczema Association
SOOTHINGRelief from dry skin associated with eczema
MOISTURIZINGRich and long-lasting formula
FOR EVERYONE
DIAPER RASH
TREATMENT8VH�DW�WKH�À�UVW�VLJQ�RI�UHGQHVV
PREVENTIONUse daily to prevent diaper rash
TRUSTEDRecommended by pediatricians, loved by parents
FOR BABY
FUNGAL INFECTIONS
HEALING)RU�WKH�WUHDWPHQW�RI�VXSHUÀ�FLDO�VNLQ�
infections caused by yeast
(Candida albicans)
SOOTHINGRelief from burning, itching and discomfort
PROTECTINGRepels moisture and provides an effective barrier
FOR EVERYONE
Page 34
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 636
hospital zone
PH
OT
OS
PR
OV
IDE
D B
Y K
AR
LA
HA
YN
ES
, R
N,
MP
H,
MS
, C
PN
P, C
HIL
DR
EN
’S H
OS
PIT
AL
LOS
AN
GE
LES
.
Nurse practitioners coordinate
care at the center, and the surgical
care is directed by a plastic surgeon
who relies heavily on the input of
the team members, Haynes says.
“Our patients all have their own
community pediatricians that
do their usual well-child health
surveillance and sick visits,” Haynes
said. “The pediatricians on our cra-
niofacial team monitor patients . . .
looking at signs of obstructive sleep
apnea or gastroesophageal reflux or
some of the things that kids with
cleft lip and cleft palate or other cra-
niofacial diagnoses are more likely
to have.”
The care of these patients often
begins in utero, according to Haynes.
“My nurse practitioner colleagues
and I also do prenatal counseling
in conjunction with a program at
our hospital called the Institute for
Maternal-Fetal Health,” she says.
A nurse practitioner and the
institute’s perinatologist will meet
with pregnant mothers who are
referred to the institute because of
a possible cleft on ultrasound. “[We]
will do another anatomy scan with,
in our case, the craniofacial nurse
practitioner standing right beside
the perinatologist, so we’re looking
at the images together. And based
on what the 2 providers see, the par-
ents are counseled on the diagno-
sis,” Haynes says. “About half, if not
more, of our babies are identified
before birth.”
There are other centers of excel-
lence focused on children with
craniofacial conditions, includ-
ing Seattle Children’s Hospital in
Washington state, Brigham and
Women’s Hospita l /Chi ldren’s
Hospital in Boston, Massachusetts,
a nd Ch i ld ren’s Hospit a l of
Philadelphia, Pensylvania, accord-
ing to Haynes.
At the very least, teams charged
with the care of children with
cleft lip and palate should include
speech-language pathology, surgery,
and orthodontics specialists. The
core team should have ready access
S FIGURE 6 Patient is 12 days postoperative following repair of left
alveolar cleft to stabilize her dental arch and maxilla. She is aged 10 years
3 months in this photo.
S FIGURE 7 Patient is 6 weeks postoperative following repair of left
alveolar cleft (as in Figure 6). She is aged 10 years 4 months in this photo.
Page 35
37J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
hospital zone
to psychology, social work, audiol-
ogy, genetics, general and pediatric
dentistry, otolaryngology, and pedi-
atrics/primary care professionals.
The team should also be able to refer
to a neurosurgeon, an ophthalmolo-
gist, a radiologist, and a geneticist,
according to the American Cleft
Palate-Craniofacial Association.4
Best practicesPediatric patients with cleft lip and
palate require numerous surger-
ies throughout their childhood
and into early adulthood to correct
the aesthetic and functional issues
associated with their diagnoses. In
1 sample of patients, the aver-
age number of surgical procedures
required was 8.6.5
“For all of the facial structures
and sociologic processes that are
affected by craniofacial [condi-
tions], we use different providers
on our team that are looking out for
all of these areas that are at risk,”
Haynes says. “Sometimes, a lack
of continuity of care is a problem.
But definitely pediatricians should
know that if there is a child who is
born with a cleft, they need to be
with ongoing team care.”
There are different stages in the
surgery. When they’re done depends
a lot on the phase of dentition,
according to Haynes. She describes
a potential timeline of treatment for
children with cleft lip and palate:
“The very first surgery that’s done
is usually an initial cleft lip repair,
in which the lip is repaired and the
external nose, as well. That’s usu-
ally done anywhere between 1 and
3 months of age. Sometimes it can
be a little later,” she says. “The sec-
ond surgery is to repair the palate,
which of course is the roof of the
mouth, but it’s also the floor of the
nose. So, it does address that second
nasal component, and that’s usually
done sometime around 1 year of
age, ideally.”
The next surgery that many of
these children need is an alveolar
bone graft, which is done to repair
the dental arch of the maxilla where
the cleft has gone through the gums.
“That can be done in several ways,”
says Haynes, “but the children gen-
erally need to be in mixed dentition
before they can do the orthodontics
that allow them to have that surgery.
That surgery literally can’t be done
before they’re 7, 8, or 9 years of age.”
There are some optional surger-
ies, including scar revisions. “For
many of our kids, once they reach
skeletal maturity, they may need
an orthognathic jaw procedure
because one of the things that hap-
pens with kids with cleft lip and
cleft palate is they often end up
with a pretty significant under-
bite,” Haynes says. “Some of this is
correctable through orthodontics,
but for many kids the only way is
to do a surgery that involves mov-
ing the bones in the face. And that
can’t be done until kids are in their
later teenaged years.”
Care outcomesChildren with cleft lip and palate
have a poor quality of life.6 In addi-
tion, fragmented or uncoordinated
care of these children leads to poor
outcomes in speech and hearing.7
Haynes says the children that get
their care at Children’s Hospital Los
Angeles emerge with little if any
evidence of their cleft deformities.
“When the proper stepwise
approach is taken, children have
surgeries that address each ana-
tomic issue to ultimately result in a
child with good intelligible speech,
normal hearing, a stable maxilla,
proper occlusion of the jaws, and
symmetric facial features,” Haynes
says. “For families and providers
both, one of the biggest, most com-
pelling questions that remains is
‘Why does clefting happen?’ We
may be getting closer to having a
better understanding of the origin
of the ‘isolated’ clefts because of
the relative availability of exome
sequencing. We would also like to
know more about the role environ-
mental factors, such as maternal
diabetes, play.”
Haynes says Children’s Hospital
Los Angeles is conducting research
on the incidence of postpartum
depression in mothers of infants
born with cleft, and investigating
safe infant sleep for infants born
with Pierre Robin sequence.
For additional information to
help pediatricians discuss
facial clefts with families, as well
as references for this article, go to
ContemporaryPediatrics.com/
Hospital-Zone-facial-clefts
Facial clefts involving the lip and/or palate occur in about 1 in 600 live births
in the United States.1,2
Page 36
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 638
IMA
GE
CR
ED
IT/A
UT
HO
R S
UP
PLI
ED
At home, the patient’s cough per-
sisted with the addition of several
episodes of nonbloody, nonbilious
posttussive emesis. On day 9 of ill-
ness, he developed oral vesicular
lesions associated with discom-
fort when swallowing solid foods,
prompting a visit to the local emer-
gency department (ED). There,
his temperature was 102.92°F, but
physical exam and chest imaging
performed at that time were reas-
suring for a safe discharge home
with close follow-up after being
given a 5-day course of azithromy-
cin for bronchitis (Figure 1).
By day 12 of his il lness, the
patient’s course was worsening.
The vesicular oral lesions were fri-
able and beginning to bleed. His
coughing episodes were increas-
ingly f requent and produced
blood-streaked sputum. Severe
odynophagia prevented him from
consuming both solids and liquids.
A complete physical exam by his
pediatrician at follow-up revealed
red, round, ulcerative lesions of the
ventral penile shaft along with skin
peeling and scant mucus discharge
at the urethral opening. Because
of his poor f luid intake and pro-
gressing symptomatology, he was
quickly referred back to the ED and
admitted for continued evaluation
and management (Figure 2).
HistoryThe patient endorsed a history of
acne vulgaris for which he took
minocycline daily. There was, how-
ever, no prior history of surgeries,
abnormal development, or varia-
tions from a regular healthy diet.
Family history was signif icant
only for maternal allergic reac-
tion of unknown severity to Perco-
cet (oxycodone hydrochloride with
acetaminophen) and Motrin (ibu-
profen). The patient had no known
drug allergy prior to presenta-
tion, and his immunizations were
up-to-date.
Upon HEA DDSSS (Home,
Education, Activities, Drug use
and abuse, Death, Sexual behavior,
Suicidality and depression, Safety)
assessment, the boy stated that
he lives at home with his mother,
father, and 2 younger sisters, the
oldest of which was recently diag-
nosed with pneumonia and suc-
cessfully treated with azithromycin.
He denied having pets in the home.
He was in the 11th grade and doing
well academically. Daily physical
activity was limited because he was
not interested in sports but rather
enthusiastically committed to play-
ing video games. He denied illicit
substance use, depressive symp-
toms, safety concerns, sexual activ-
ity of any kind, or suicidal ideation.
Physical examUpon physical examination, the
patient was afebrile with normal
vital signs. He appeared uncom-
fortable, tired, and in mild distress.
His eyes were without discharge or
conjunctival injection. External ear
canals were normal. Nares revealed
hemorrhagic crusts (Figure 3). Fri-
able, ulcerative lesions and dried
blood were found on his lips (Fig-
ure 4). The superf icia l buccal
mucosa was sloughing and actively
bleeding (Figure 5). The surface of
his tongue was covered by white
ulcerations posteriorly; the pal-
ate and posterior oropharynx were
BOY WITH FEVER, COUGH, AND ORAL LESIONSpuzzlerCONTINUED FROM PAGE 13
S FIGURE 3 Nares with hemorrhagic crusts. Day 16 of illness.
Page 37
39J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
puzzler
IMA
GE
CR
ED
IT/A
UT
HO
R S
UP
PLI
ED
erythematous and edematous; and
tonsillar exudates were appreci-
ated bilaterally. Lung exam was
somewhat limited by dry cough-
ing upon deep inspiration, but rales
were appreciated bilaterally in the
lower lung fields. Mild erythema of
the urethral opening along with a
single ulcerative lesion of the ven-
tral penile shaft was found. The
remainder of his physical exam,
including a thorough skin exami-
nation, was normal.
Differential diagnosisTaking into account the patient’s
presenting history and physical
exam findings, the team proposed
a fairly wide differential (Table).
Included in the list were an atypi-
cal presentation of the autoimmune
mechanisms underlying Crohn dis-
ease, absent of any associated gas-
trointestinal manifestations, and
Behçet disease, without its char-
acteristic ulcerative and erythem-
atous nodules or anterior uveitis.
Ingestion of a corrosive agent that
might precipitate the mucocuta-
neous oral findings also was con-
sidered, although the patient’s age
and absence of any intention for
self-harm made this possibility less
likely.
Infectious etiologies were pos-
tulated as well, including herpan-
gina of an enterovirus infection
or herpes simplex mucositis, most
commonly seen as a reactivation
event of a prior primary infection
in immunocompromised patients.
Even a severe drug reaction to ibu-
profen, such as Stevens-Johnson
syndrome (SJS), was introduced as
a possibility, although the limited
involvement of his pathology to the
nasal-oral and genital areas lessened
the team’s concern (Figure 6).
In narrowing the differential,
patient demographics such as age
and gender, benign past medical
history, absence of high-risk sexual
or self-harm behavior, and context
S FIGURE 4 Friable, ulcerative lesions and dried blood on patient’s lips and
tongue surface. Day 16 of illness.
S FIGURE 5 Sloughing superficial buccal mucosa with mildly active bleeding.
Day 16 of illness.
Page 38
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 640
puzzler
of presentation with corresponding
respiratory symptoms, fever, and
limited cutaneous findings led the
team to favor an infectious etiol-
ogy. What remained to be deter-
mined was the causative organism
and the extent of the pathology it
would instigate in the patient.
Further testingOvernight, ibuprofen was dis-
continued for concerns of SJS and
empiric acyclovir was started for
suspected primary herpes simplex
virus (HSV) infection. A complete
blood count with manual differen-
tial and complete metabolic panel
were normal. A urinalysis showed
scant leukocyte esterase and 5 to
DIFFERENTIAL DIAGNOSIS FOR PEDIATRIC MUCOSITIS
INFECTIOUS ALLERGIC DRUGS POISONING AUTOIMMUNE
Herpangina SJS Chemotherapy Corrosive
agent ingestion
Aphthous
stomatitis
Herpetic mucositis
Erythema
multiforme
NSAIDs and
ASA
Behçet
disease
HIV Crohn
disease
Primary syphilis
SLE
Celiac sprue
Abbreviations: ASA, acetylsalicylic acid; HIV, human immunodeficiency virus; NSAIDs, nonsteroidal anti-inflammatory drugs; SJS, Stevens-Johnson syndrome; SLE, systemic lupus erythematosus.
We’ve made yours “to go”
ContemporaryPediatrics.com/PedsApp
Page 39
puzzler
41J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
1. Corrosive ingestion} Identify specific
agent and time of ingestion
} Assess and protect airway
} CBC, CMP, ABG for baseline; repeat if suspicious for systemic toxicity
} Consult Poison Control, GI, or Surgery if unstable
} Psych eval if suicidal intent
} Supportive care
2. Aphthous stomatitis } HIV status and CBC
for assessment of neutropenia
} Ulcer Severity Score} Vitamin deficiency
assessment and correction
} Negative transglutaminase assay and Tzanck smear (rule out celiac and HSV)
} Supportive care
1. Mycoplasma-induced rash and mucositis} Respiratory infection-
like prodrome and fever} CXR with pneumonia} Findings limited to
oral, nasal, and genital mucosa +/- localized rash
} Mycoplasma PCR for diagnosis confirmation
} Antibiotic (azithromycin)
} Supportive measures with Magic Mouthwash and fluids
} Steroids +/- IVIG if severe
2. Herpangina} Febrile illness with
vesicular and/or ulcerative lesions
} Usually summer months} Constitutional
symptoms such as HA, backache, nausea, or stomach pain
} PCR of nasopharyngeal swab for enterovirus RNA
} Supportive care
1.Herpetic mucositis} Most commonly in the
immunocompromised patient
} Flu-like prodrome} Ulcerative and necrotic
lesions often localized to oral mucosa but can become systemic
} Anti-HSV titers} Acyclovir PO vs IV
along with antibiotics if superimposed bacterial superinfection
2. Erythema multiforme} Infectious vs type IV
hypersensitivity reaction} Flu-like prodrome} Spectrum of presentation
from local cutaneous involvement (target lesions) to widespread pathology of the oral, genital, orbital, and respiratory mucosa
} Clinical diagnosis, although HSV PCR can help confirm diagnosis and CMP can reveal electrolyte abnormalities and renal/hepatic involvement
} Supportive care, wound dressings, and steroids if severe
1. Stevens-Johnson syndrome} Respiratory infection-
like prodrome} Acute development of
targetoid lesions} Minimal to extensive
sloughing of the skin} Commonly idiopathic
but sometimes associated with drugs/infections
} Skin biopsy with full-thickness necrosis diagnostic
} BCx/UCx for superimposed bacterial infection
} Treated like burn patients in ICU
2. Behçet disease} Recurrent aphthous
ulcers, genital ulcers, and uveitis; sometimes with skin involvement and arthritis
} Most commonly affects mid-20s to mid-30s age range
} Extensive workup to rule out disease mimics (SLE, reactive arthritis, HIV)
} Treatment tailored to specific organ involved; multiple consultations may be necessary
Extensive skin findings?
Noninfectious? Infectious? Noninfectious?
Limited skin findings?
DIAGNOSTIC APPROACH
MUCOSITIS?
Abbreviations: ABG, arterial blood gas; BCx, blood culture; CBC, complete blood count; CMP, comprehensive metabolic panel; CXR, chest x-ray; GI, gastrointestinal; HA, headache; HIV, human immunodeficiency virus; HSV, herpes simplex virus; ICU, intensive care unit; IV, intravenous; IVIG, intravenous immunoglobulin; PCR, polymerase chain reaction; PO, per os; RNA, ribonucleic acid; SLE, systemic lupus erythematosus; UCx, urine culture.
6
Page 40
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 642
puzzler
10 white blood cell counts, but no
red blood cells. Serum cultures,
bacterial genital cultures, HSV-1
and HSV-2 polymerase chain reac-
tion tests, culture swabs of the oral
and genital lesions, and Neisseria
gonorrhoeae and Chlamydia tra-
chomatis RNA urine tests all were
sent, none of which returned posi-
tive. Chest x-ray was repeated and
was significant for subtle right
lower lobe infiltrates.
Because initial workup in the
community hospital failed to pro-
vide an identifiable etiology for
the patient’s clinical course, he was
transferred to the nearest pediatric
tertiary care center where he was
found to have Mycoplasma-induced
rash and mucositis, also known as
MIRM.
Treatment and outcomeWith suspicion for MIRM second-
ary to inadequately treated M pneu-
moniae pneumonia, the patient was
started on a second 5-day course of
azithromycin along with intrave-
nous (IV) maintenance f luids and
supportive care for the oral lesions.
Famotidine was begun for prophy-
lactic treatment of presumed gastro-
intestinal mucositis. A telemedicine
dermatology consult was utilized to
help confirm the suspected diag-
nosis, and a 5-day course of pred-
nisone was initiated. Mycoplasma
immunoglobulin (Ig)G and IgM
serology were ordered and returned
positive after hospital discharge on
his 16th day of illness. During a fol-
low-up phone call with the mother,
she noted significant improvement
in his symptoms with normal oral
intake and a successful return to
school 3 days after leaving the hos-
pital (Figure 7).
Dr Sterns is a pediatric intern at Naval
Medical Center, San Diego, California.
Dr Kamat is a pediatric hospitalist, Inova
Children’s Hospital, Falls Church, Virginia.
The authors have nothing to disclose in
regard to affiliations with or financial
interests in any organizations that may have
an interest in any part of this article.
For an in-depth discussion of
MIRM with references, go to
ContemporaryPediatrics.com/puzzler-0716
Symptom onset
} Tactile
fevers
} Malaise
Initial PCP
evaluation
URI diagnosis
} Friable oral
lesions
} Poor oral intake
} PCP follow-up;
genital lesions
found
} Return to ED
and hospital
admission
} Azithromycin
discontinued
} Workup started
} Mucositis stable
} Oral intake much
improved
} Day of discharge
} Congestion
} Dry cough
} Oral lesions
} Productive cough
and posttussive
emesis
} ED visit with
negative CXR
} Azithromycin
started
} Transfer to children’s
hospital
} 2nd course of
azithromycin begun
} Mycoplasma IgM/IgG
serologies drawn
} Dermatology consult
and start of oral
steroid course
} Resolution
of symptoms
and return to
school
Day 2 Day 5 Day 9 Day 12 Day 14 Day 16 Day 19
PATIENT’S DISEASE COURSE
Abbreviations: CXR, chest x-ray; ED, emergency department; IgG, immunoglobulin G, IgM, immunoglobulin M; PCP, primary care physician; URI, upper respiratory infection.
7
Page 41
dermcase
43J U LY 2 01 6 | CON T EMPORARYP ED I AT R I C S . C O M
CONTINUED FROM PAGE 44
Nevus of Ota (also known as “con-
genital melanosis bulbi,” “nevus fus-
coceruleus ophthalmomaxillaris,”
or “oculodermal melanocytosis”)
is a variant of Mongolian spot that
presents with bluish-green to grey-
brown pigmentation on the face.
Approximately half of the cases are
congenital, and the others typically
are acquired in the teenaged years.
Nevus of Ota occurs most fre-
quently in Asians, with an estimated
prevalence of 0.014% to 0.034%, and
it is uncommon among Caucasians.1
It also develops frequently in East
Indians and African Americans,
and is 5 times more common in
females than males.2
Nevus of Ota is caused by the
entrapment of melanocytes in the
upper third of the dermis, involv-
ing the first and/or second (oph-
thalmic and maxillary) branches
of the trigeminal nerve. Although
unconfirmed, investigators suggest
that nevus of Ota may occur when
melanocytes arising from the neural
crest do not migrate to their normal
position in the basal cell layer of
the epidermis during early embryo-
logic development.3 Whereas biopsy
usually is not necessary to establish
the diagnosis, histology shows uni-
formly distributed melanocytes in
the dermis. Differential diagnoses
include blue nevi, café au lait spots,
melasma, and cutaneous melanoma.
Nevus of Ota is usually unilat-
eral (90%), generally involving only
1 side of the face over the cheek,
nose, forehead, temple, and around
the eye; however, it also can be
bilateral, although rarely.4 There
have been a few case reports of
oral mucosal involvement, which is
extremely rare.2 Given the involve-
ment of the trigeminal nerve, it can
cause discoloration of the eyelid,
sclera, cornea, and/or retina. The
sclera is involved in two-thirds of
patients, and scleral involvement is
associated with an increased risk
for glaucoma, which occurs in 10%
of patients.5 For this reason, all
patients with a nevus of Ota that
involves any structure of the eye or
eyelid should be referred to ophthal-
mology for routine screening.
Risk of melanomaThe lesion remains unchanged
throughout life but it may darken
with sun exposure. Because of its
location and high visibility, nevus
of Ota may be associated with
major psychosocial issues for both
children and adults. As a conse-
quence, all patients should be evalu-
ated for possible treatment with the
Q-switched lasers that offer a good
clinical response with little or no
risk of scarring.1
Essentially, nevus of Ota is similar
in pathophysiology and appearance
to the Mongolian spot, but differs
in location. It is a benign condi-
tion that may be managed by the
primary care physician. However,
monitoring should continue given
its rare potential to transform into a
malignant melanoma.
Dr Gangaram is a third-year pediatric
resident, Herman and Walter Samuelson
Children’s Hospital at Sinai, Baltimore,
Maryland. Dr Cohen, section editor for
Dermcase, is professor of pediatrics and
dermatology, Johns Hopkins University
School of Medicine, Baltimore, Maryland.
The author and section editor have nothing
to disclose in regard to affiliations with
or financial interests in any organizations
that may have an interest in any part of this
article. Vignettes are based on real cases
that have been modified to allow the author
and section editor to focus on key teaching
points. Images also may be edited or
substituted for teaching purposes.
R E F E R E N C E S
1. Chan HH, Kono T. Nevus of Ota: clinical aspects and management. Skinmed. 2003;2(2):89-96.
2. Shetty SR, Subhas BG, Rao KA, Castellino R. Nevus of ota with buccal mucosal pigmentation: a rare case. Dent Res J (Isfahan). 2011;8(1):52-55.
3. Hori Y, Takayama O. Circumscribed dermal melano-ses. Classification and histologic features. Dermatol
Clin. 1988;6(2):315-326.
4. Magarasevic L, Abazi Z. Unilateral open-angle glau-coma associated with the ipsilateral nevus of Ota.
Case Rep Ophthalmol Med. 2013; 2013: 924937.
5. Khawly JA, Imami N, Shields MB. Glaucoma associated with the nevus of Ota. Arch Ophthalmol. 1995;113(9):1208-1209.
NEVUS OF OTA
All patients with a nevus of Ota that involves any structure of the eye or eyelid should be referred to ophthalmology for
routine screening.
To read previous
Dermcase articles, go to
ContemporaryPediatrics.com/tag/
Contemporary-Pediatrics-Dermcase
Page 42
BERNARD A COHEN, MD SECTION EDITORdermcase
CON T EMPORARYP ED I AT R I C S . C O M | J U LY 2 01 644
IMA
GE
CR
ED
IT/A
UT
HO
R S
UP
PLI
ED
Hyperpigmentation around a teen’s eyeAn adolescent girl is referred by her pediatrician to dermatology for evaluation
of a birthmark on her face. FOR MORE ON THIS CASE, TURN TO PAGE 43.
W FIGURE Congenital
hyperpigmented patch involving
the right side of the face and
bulbar conjunctiva.
THE CASE
NEVUS OF OTAdiagnosisDERMCASE
JESSICA A GANGARAM, MD
Page 43
45j u ly 2 01 6 | CON T EMPORARYP ED I AT R I C S . c o m
careersArizonA idAho
ARIZONA
Great family and golf community. Full-time Pediatrician BC/BE to join well established Pediatric practice in Tucson, Az. Competitive salary
with excellent benefit package, including bonus compensation.Send CV to [email protected]
Reach your target audience. Our audience.Contact me today to place your ad.Joanna ShippoliAccount [email protected]
Heart of IdaHo!Live in the
If adventure is what you are looking for, this is the right place for you! Idaho’s Treasure Valley offers it all. Hiking, skiing, fishing, whitewater rafting, and more, all within an hour of our multi-specialty group based in Nampa. Boise, Idaho’s capital, and largest city is just minutes away. Saltzer Medical Group, the largest and oldest physician-owned multi-specialty group in the state of Idaho is seeking a pediatric physician. A favorable malpractice climate, shareholder status after three successful years of employment and affordable housing makes this an ideal practice location. Position is in Nampa, call is 1:5. Nurse triage services are available for after hours call. A competitive compensation package with guarantee and incentive is being offered to the right individual. For immediate consideration, Contact Vicki Tyler at (208) 463-3158; or send CV to: [email protected] .
Additional information about our group can be viewedon our website at www.saltzermed.com.
Content Licensing for Every Marketing Strategy
Marketing solutions fi t for:Outdoor | Direct Mail | Print Advertising
Tradeshow/POP Displays Social Media | Radio & TV
Leverage branded content from Contemporary Pediatrics to create a more powerful and sophisticated statement about your product, service,
or company in your next marketing campaign. Contact Wright’s Media to � nd out more about how we can customize your acknowledgements and recognitions to enhance your
marketing strategies.
For information, call Wright’s Media at 877.652.5295
or visit our website at www.wrightsmedia.com
Advertising Index
ATHENA HEALTH corporate ...................................................................... 19www.athenahealth.com
BEIERSDORF Eucerin Eczema .............................................................. 5www.eucerinus.com
IMPAX LABORATORIESEmverm ........................................................................ 7-8www.emvermhcp.com
SUMMERS LABORATORIES Product line .................................................................. 35www.summers-direct.com/samples
UNILEVERDove .............................................................................. 29www.dove.us