1
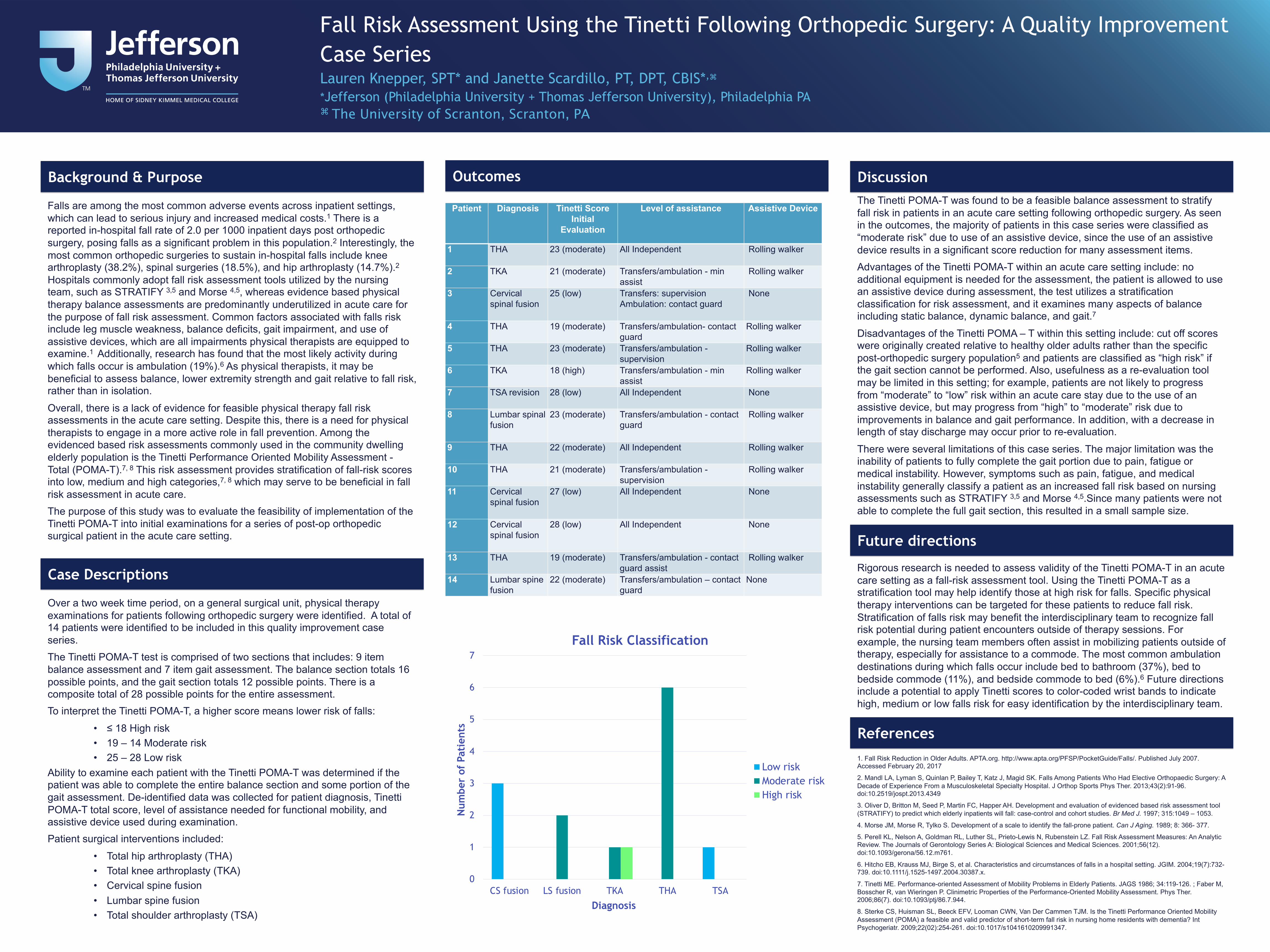
Background & Purpose Falls are among the most common adverse events across inpatient settings, which can lead to serious injury and increased medical costs. 1 There is a reported in-hospital fall rate of 2.0 per 1000 inpatient days post orthopedic surgery, posing falls as a significant problem in this population. 2 Interestingly, the most common orthopedic surgeries to sustain in-hospital falls include knee arthroplasty (38.2%), spinal surgeries (18.5%), and hip arthroplasty (14.7%). 2 Hospitals commonly adopt fall risk assessment tools utilized by the nursing team, such as STRATIFY 3,5 and Morse 4,5 , whereas evidence based physical therapy balance assessments are predominantly underutilized in acute care for the purpose of fall risk assessment. Common factors associated with falls risk include leg muscle weakness, balance deficits, gait impairment, and use of assistive devices, which are all impairments physical therapists are equipped to examine. 1 Additionally, research has found that the most likely activity during which falls occur is ambulation (19%). 6 As physical therapists, it may be beneficial to assess balance, lower extremity strength and gait relative to fall risk, rather than in isolation. Overall, there is a lack of evidence for feasible physical therapy fall risk assessments in the acute care setting. Despite this, there is a need for physical therapists to engage in a more active role in fall prevention. Among the evidenced based risk assessments commonly used in the community dwelling elderly population is the Tinetti Performance Oriented Mobility Assessment - Total (POMA-T). 7, 8 This risk assessment provides stratification of fall-risk scores into low, medium and high categories, 7, 8 which may serve to be beneficial in fall risk assessment in acute care. The purpose of this study was to evaluate the feasibility of implementation of the Tinetti POMA-T into initial examinations for a series of post-op orthopedic surgical patient in the acute care setting. Case Descriptions Over a two week time period, on a general surgical unit, physical therapy examinations for patients following orthopedic surgery were identified. A total of 14 patients were identified to be included in this quality improvement case series. The Tinetti POMA-T test is comprised of two sections that includes: 9 item balance assessment and 7 item gait assessment. The balance section totals 16 possible points, and the gait section totals 12 possible points. There is a composite total of 28 possible points for the entire assessment. To interpret the Tinetti POMA-T, a higher score means lower risk of falls: • ≤ 18 High risk • 19 – 14 Moderate risk • 25 – 28 Low risk Ability to examine each patient with the Tinetti POMA-T was determined if the patient was able to complete the entire balance section and some portion of the gait assessment. De-identified data was collected for patient diagnosis, Tinetti POMA-T total score, level of assistance needed for functional mobility, and assistive device used during examination. Patient surgical interventions included: • Total hip arthroplasty (THA) • Total knee arthroplasty (TKA) • Cervical spine fusion • Lumbar spine fusion • Total shoulder arthroplasty (TSA) Outcomes Discussion The Tinetti POMA-T was found to be a feasible balance assessment to stratify fall risk in patients in an acute care setting following orthopedic surgery. As seen in the outcomes, the majority of patients in this case series were classified as “moderate risk” due to use of an assistive device, since the use of an assistive device results in a significant score reduction for many assessment items. Advantages of the Tinetti POMA-T within an acute care setting include: no additional equipment is needed for the assessment, the patient is allowed to use an assistive device during assessment, the test utilizes a stratification classification for risk assessment, and it examines many aspects of balance including static balance, dynamic balance, and gait. 7 Disadvantages of the Tinetti POMA – T within this setting include: cut off scores were originally created relative to healthy older adults rather than the specific post-orthopedic surgery population 5 and patients are classified as “high risk” if the gait section cannot be performed. Also, usefulness as a re-evaluation tool may be limited in this setting; for example, patients are not likely to progress from “moderate” to “low” risk within an acute care stay due to the use of an assistive device, but may progress from “high” to “moderate” risk due to improvements in balance and gait performance. In addition, with a decrease in length of stay discharge may occur prior to re-evaluation. There were several limitations of this case series. The major limitation was the inability of patients to fully complete the gait portion due to pain, fatigue or medical instability. However, symptoms such as pain, fatigue, and medical instability generally classify a patient as an increased fall risk based on nursing assessments such as STRATIFY 3,5 and Morse 4,5 .Since many patients were not able to complete the full gait section, this resulted in a small sample size. Future directions Rigorous research is needed to assess validity of the Tinetti POMA-T in an acute care setting as a fall-risk assessment tool. Using the Tinetti POMA-T as a stratification tool may help identify those at high risk for falls. Specific physical therapy interventions can be targeted for these patients to reduce fall risk. Stratification of falls risk may benefit the interdisciplinary team to recognize fall risk potential during patient encounters outside of therapy sessions. For example, the nursing team members often assist in mobilizing patients outside of therapy, especially for assistance to a commode. The most common ambulation destinations during which falls occur include bed to bathroom (37%), bed to bedside commode (11%), and bedside commode to bed (6%). 6 Future directions include a potential to apply Tinetti scores to color-coded wrist bands to indicate high, medium or low falls risk for easy identification by the interdisciplinary team. References 1. Fall Risk Reduction in Older Adults. APTA.org. http://www.apta.org/PFSP/PocketGuide/Falls/. Published July 2007. Accessed February 20, 2017 2. Mandl LA, Lyman S, Quinlan P, Bailey T, Katz J, Magid SK. Falls Among Patients Who Had Elective Orthopaedic Surgery: A Decade of Experience From a Musculoskeletal Specialty Hospital. J Orthop Sports Phys Ther. 2013;43(2):91-96. doi:10.2519/jospt.2013.4349 3. Oliver D, Britton M, Seed P, Martin FC, Happer AH. Development and evaluation of evidenced based risk assessment tool (STRATIFY) to predict which elderly inpatients will fall: case-control and cohort studies. Br Med J. 1997; 315:1049 – 1053. 4. Morse JM, Morse R, Tylko S. Development of a scale to identify the fall-prone patient. Can J Aging. 1989; 8: 366- 377. 5. Perell KL, Nelson A, Goldman RL, Luther SL, Prieto-Lewis N, Rubenstein LZ. Fall Risk Assessment Measures: An Analytic Review. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2001;56(12). doi:10.1093/gerona/56.12.m761. 6. Hitcho EB, Krauss MJ, Birge S, et al. Characteristics and circumstances of falls in a hospital setting. JGIM. 2004;19(7):732- 739. doi:10.1111/j.1525-1497.2004.30387.x. 7. Tinetti ME. Performance-oriented Assessment of Mobility Problems in Elderly Patients. JAGS 1986; 34:119-126. ; Faber M, Bosscher R, van Wieringen P. Clinimetric Properties of the Performance-Oriented Mobility Assessment. Phys Ther. 2006;86(7). doi:10.1093/ptj/86.7.944. 8. Sterke CS, Huisman SL, Beeck EFV, Looman CWN, Van Der Cammen TJM. Is the Tinetti Performance Oriented Mobility Assessment (POMA) a feasible and valid predictor of short-term fall risk in nursing home residents with dementia? Int Psychogeriatr. 2009;22(02):254-261. doi:10.1017/s1041610209991347. Fall Risk Assessment Using the Tinetti Following Orthopedic Surgery: A Quality Improvement Case Series Lauren Knepper, SPT* and Janette Scardillo, PT, DPT, CBIS* , ⌘ *Jefferson (Philadelphia University + Thomas Jefferson University), Philadelphia PA ⌘ The University of Scranton, Scranton, PA Patient Diagnosis Tinetti Score Initial Evaluation Level of assistance Assistive Device 1 THA 23 (moderate) All Independent Rolling walker 2 TKA 21 (moderate) Transfers/ambulation - min assist Rolling walker 3 Cervical spinal fusion 25 (low) Transfers: supervision Ambulation: contact guard None 4 THA 19 (moderate) Transfers/ambulation- contact guard Rolling walker 5 THA 23 (moderate) Transfers/ambulation - supervision Rolling walker 6 TKA 18 (high) Transfers/ambulation - min assist Rolling walker 7 TSA revision 28 (low) All Independent None 8 Lumbar spinal fusion 23 (moderate) Transfers/ambulation - contact guard Rolling walker 9 THA 22 (moderate) All Independent Rolling walker 10 THA 21 (moderate) Transfers/ambulation - supervision Rolling walker 11 Cervical spinal fusion 27 (low) All Independent None 12 Cervical spinal fusion 28 (low) All Independent None 13 THA 19 (moderate) Transfers/ambulation - contact guard assist Rolling walker 14 Lumbar spine fusion 22 (moderate) Transfers/ambulation – contact guard None 0 1 2 3 4 5 6 7 CS fusion LS fusion TKA THA TSA Number of Patients Diagnosis Fall Risk Classification Low risk Moderate risk High risk