Changes in FIGO 2014 Staging of Ovarian Cancer SUJOY DASGUPTA MBBS (Gold Medalist) MS (OBGY-Gold Medalist) DNB (OBGY) Senior Resident, Deptt of Gynaecological Oncology, Chittaranjan National Cancer Institute (CNCI)
Transcript
Changes in FIGO 2014 Staging of Ovarian Cancer
SUJOY DASGUPTA
MBBS (Gold Medalist) MS (OBGY-Gold Medalist)DNB (OBGY)
Senior Resident,Deptt of Gynaecological Oncology,Chittaranjan National Cancer Institute (CNCI)
Prof J Heyman, Stockholm
Characteristics of Staging
Objectives of Staging
• To plan treatment
• To explain prognosis
• To evaluate the results of treatment
• To facilitate the exchange of information between treatment centers
Ovarian Cancer Staging
• FIGO, 1973
• FIGO, 1988
October 7-12, 2012; Rome, Italy
Professor Lynette Denny,
The Chair of FIGO Committee on Gynecologic Oncology
• Gynecology Cancer Intergroup
• International Gynecologic Cancer Society
• European Organization for Research and Treatment of Cancer
• American Society of Gynecologic Oncology; the European Society of Gynecologic Oncology
• National Cancer Research Network, UK
• Australian Society of Gynaecological Oncology
• Korean Society of Gynecologic Oncology
• Japanese Society of Obstetrics and Gynecology
May, 2013
• FIGO Executive Board
• AJCC
• UICC
January 1, 2014
FIGO, 2014
• Staging
• Histologic type and grading must be mentioned
• Primary site- Ovarian, Fallopian tube and Peritoneal Cancer
New Staging
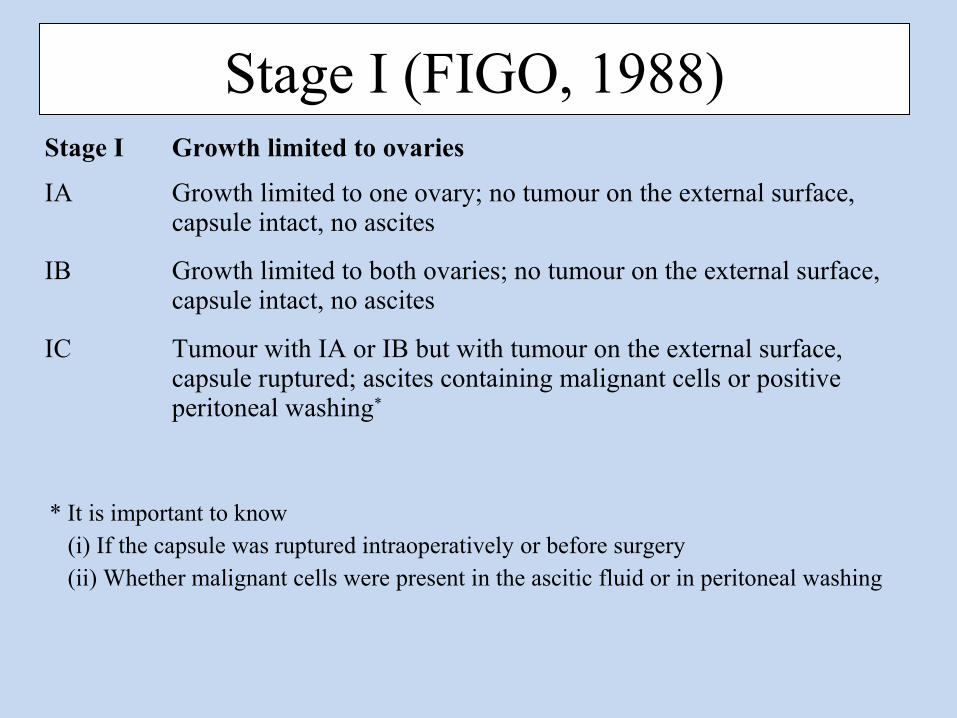
Stage I (FIGO, 1988)Stage I Growth limited to ovaries
IA Growth limited to one ovary; no tumour on the external surface, capsule intact, no ascites
IB Growth limited to both ovaries; no tumour on the external surface, capsule intact, no ascites
IC Tumour with IA or IB but with tumour on the external surface, capsule ruptured; ascites containing malignant cells or positive peritoneal washing*
* It is important to know (i) If the capsule was ruptured intraoperatively or before surgery (ii) Whether malignant cells were present in the ascitic fluid or in peritoneal washing
Controversies
Surgical SpillCan affect prognosis???
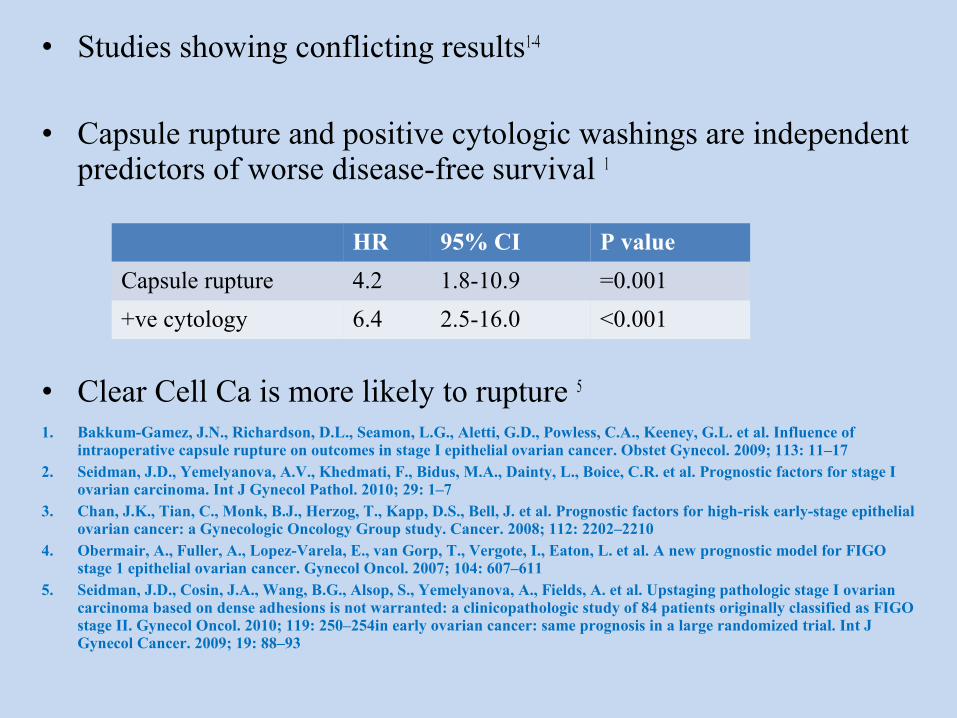
• Studies showing conflicting results1-4
• Capsule rupture and positive cytologic washings are independent predictors of worse disease-free survival 1
• Clear Cell Ca is more likely to rupture 5
1. Bakkum-Gamez, J.N., Richardson, D.L., Seamon, L.G., Aletti, G.D., Powless, C.A., Keeney, G.L. et al. Influence of intraoperative capsule rupture on outcomes in stage I epithelial ovarian cancer. Obstet Gynecol. 2009; 113: 11–17
2. Seidman, J.D., Yemelyanova, A.V., Khedmati, F., Bidus, M.A., Dainty, L., Boice, C.R. et al. Prognostic factors for stage I ovarian carcinoma. Int J Gynecol Pathol. 2010; 29: 1–7
3. Chan, J.K., Tian, C., Monk, B.J., Herzog, T., Kapp, D.S., Bell, J. et al. Prognostic factors for high-risk early-stage epithelial ovarian cancer: a Gynecologic Oncology Group study. Cancer. 2008; 112: 2202–2210
4. Obermair, A., Fuller, A., Lopez-Varela, E., van Gorp, T., Vergote, I., Eaton, L. et al. A new prognostic model for FIGO stage 1 epithelial ovarian cancer. Gynecol Oncol. 2007; 104: 607–611
5. Seidman, J.D., Cosin, J.A., Wang, B.G., Alsop, S., Yemelyanova, A., Fields, A. et al. Upstaging pathologic stage I ovarian carcinoma based on dense adhesions is not warranted: a clinicopathologic study of 84 patients originally classified as FIGO stage II. Gynecol Oncol. 2010; 119: 250–254in early ovarian cancer: same prognosis in a large randomized trial. Int J Gynecol Cancer. 2009; 19: 88–93
HR 95% CI P value
Capsule rupture 4.2 1.8-10.9 =0.001
+ve cytology 6.4 2.5-16.0 <0.001
Prat J, FIGO Committee on Gynecologic Oncology (2014). Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int J Gynaecol Obstet. 124:1 5.‐
• Meta-analysis of 9 studies included 2382 patients
• Progression free survival (PFS)
Pre-op rupture << Intra-op rupture << No rupture
• “Intra-op rupture” vs “No rupture”-
in patients who underwent a complete surgical staging with or without adjuvant platinum based ‐chemotherapy
• Rupture should be avoided during primary surgery of malignant ovarian tumors confined to the ovaries
Bilateral tumoursIndependent contralateral primary tumor vs
implants or metastases ???
• Primary bilateral tumour- Relatively uncommon, occurring in only 1%–5% of stage I cases 1, 2
• Implants/ metastasis- seen in 30% of stage I tumours 3
1. Heintz, A.P., Odicino, F., Maisonneuve, P., Quinn, M.A., Benedet, J.L., Creasman, W.T. et al. Carcinoma of the ovary. FIGO 26th Annual Report on the Results of Treatment in Gynecological Cancer. Int J Gynecol Obstet. 2006; : S161–S192
2. Yemelyanova, A.V., Cosin, J.A., Bidus, M.A., Boice, C.R., and Seidman, J.D. Pathology of stage I versus stage III ovarian carcinoma with implications for pathogenesis and screening. Int J Gynecol Cancer. 2008; 18: 465–469
3. Seidman, J.D., Yemelyanova, A.V., Khedmati, F., Bidus, M.A., Dainty, L., Boice, C.R. et al. Prognostic factors for stage I ovarian carcinoma. Int J Gynecol Pathol. 2010; 29: 1–7
Surface involvementGross Excrescences vs
Microscopic Involvement ???
• Exophytic papillary tumor on the surface of the ovary or fallopian tube
• Smooth surfaced tumours rarely have exposed cancer cells on the surface
• Assessment of surface involvement requires careful GROSS examination
Dense AdhesionsShould be considered stage II ???
• Adhesions of an apparent stage I tumor requiring sharp dissection (or when dissection results in tumor rupture)
• Dense adhesions may result in outcomes equivalent to tumors in stage II 1,2
• Upstaging to stage II based on dense adhesion- ????? 3
1. Dembo, A.J., Davy, M., Stenwig, A.E., Berle, E.J., Bush, R.S., and Kjorstad, K. Prognostic factors in patients with stage I epithelial ovarian cancer. Obstet Gynecol. 1990; 75: 263–273
2. Ozols, R.F., Rubin, S.C., and Thomas, G.M. Epithelial Ovarian Cancer. in: W.J. Hoskins, R.C. Young, M. Markman, C.A. Perez, R. Barakat, M. Randall (Eds.) Principles and Practice of Gynecologic Oncology. 4th ed. Lippincott, New York; 2005: 895–987
3. Seidman, J.D., Cosin, J.A., Wang, B.G., Alsop, S., Yemelyanova, A., Fields, A. et al. Upstaging pathologic stage I ovarian carcinoma based on dense adhesions is not warranted: a clinicopathologic study of 84 patients originally classified as FIGO stage II. Gynecol Oncol. 2010; 119: 250–254
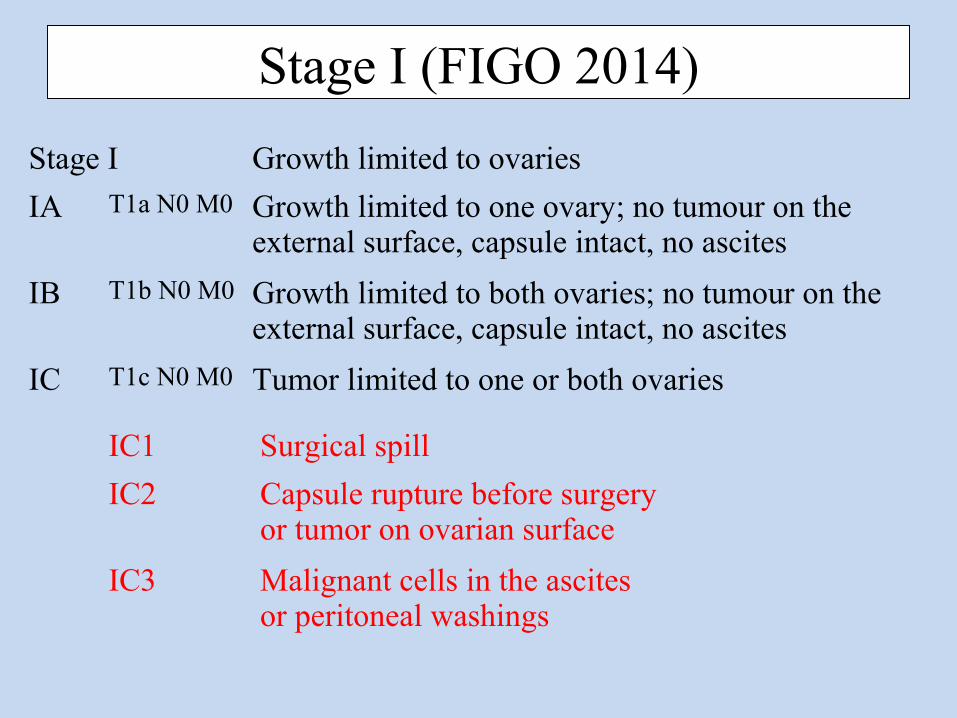
Stage I (FIGO 2014)
Stage I Growth limited to ovaries
IA T1a N0 M0 Growth limited to one ovary; no tumour on the external surface, capsule intact, no ascites
IB T1b N0 M0 Growth limited to both ovaries; no tumour on the external surface, capsule intact, no ascites
IC T1c N0 M0 Tumor limited to one or both ovaries
IC1 Surgical spill
IC2 Capsule rupture before surgery or tumor on ovarian surface
IC3 Malignant cells in the ascitesor peritoneal washings
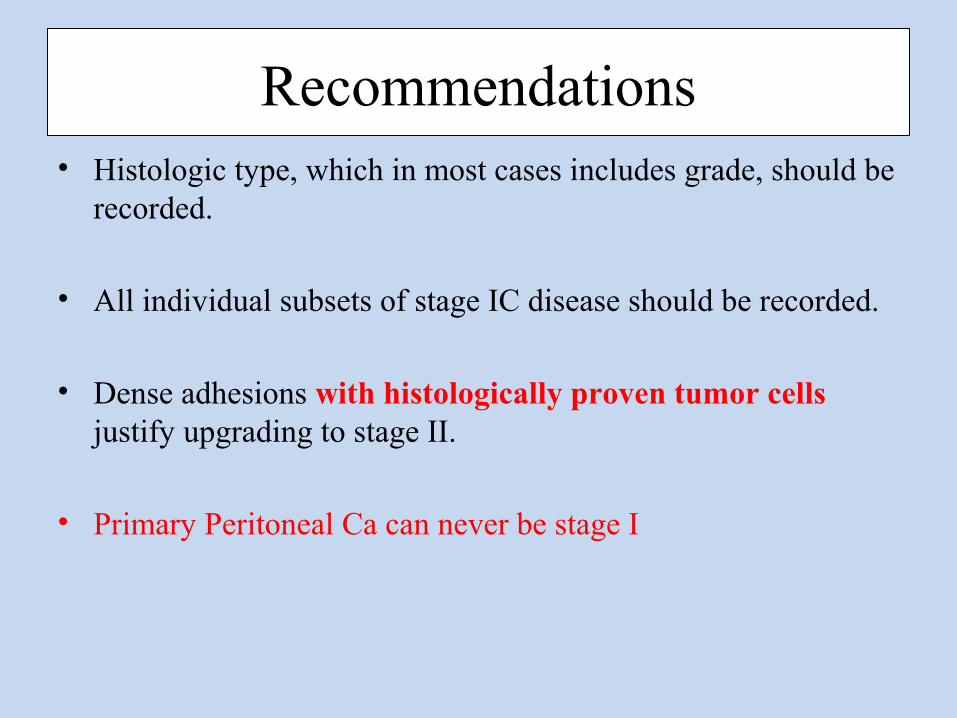
Recommendations• Histologic type, which in most cases includes grade, should be
recorded.
• All individual subsets of stage IC disease should be recorded.
• Dense adhesions with histologically proven tumor cells justify upgrading to stage II.
• Primary Peritoneal Ca can never be stage I
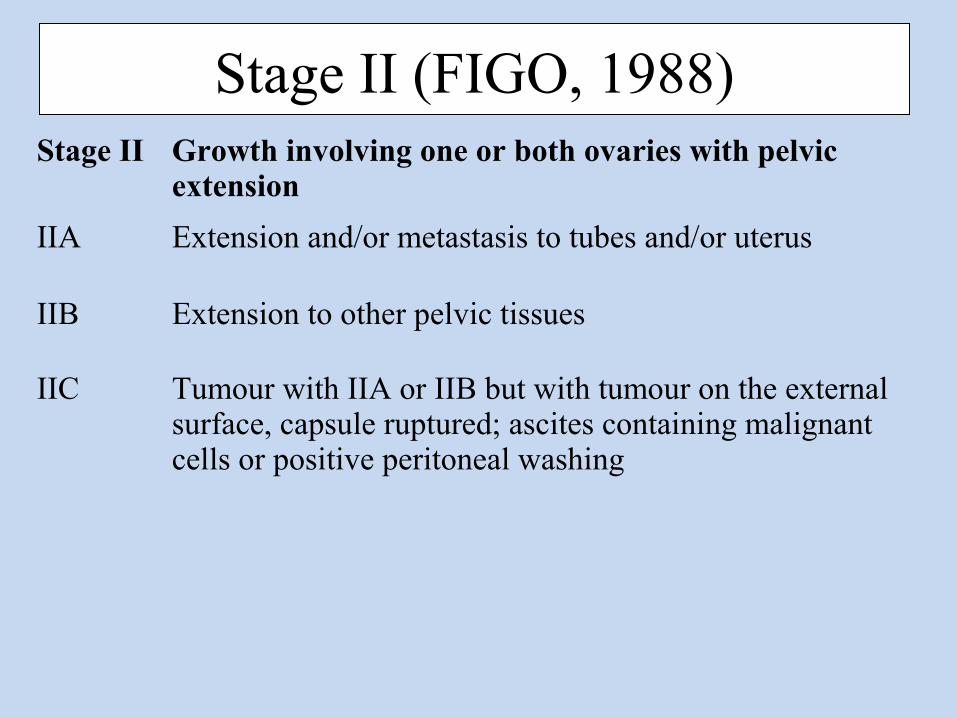
Stage II (FIGO, 1988)Stage II Growth involving one or both ovaries with pelvic
extension
IIA Extension and/or metastasis to tubes and/or uterus
IIB Extension to other pelvic tissues
IIC Tumour with IIA or IIB but with tumour on the external surface, capsule ruptured; ascites containing malignant cells or positive peritoneal washing
Controversies
What is exactly Stage II ???
• Difficult to define
• <10% of ovarian cancers
• A heterogeneous group
1.Potentially curable tumors- direct extension to adjacent organs but have not yet metastasized
2.Tumour seeded the pelvic peritoneum by metastasis (Poor Prognosis)
Pelvic Tissue???
• Sigmoid colon
• Bladder
• Transmural involvement ???
Pelvic peritoneumIs separate from abdominal peritoneum?
• Peritoneum is a continuous anatomic unit
• Pelvic involvement and extrapelvic involvement are prognostically similar (as for stage IIIA endometrial carcinoma)
• Anatomically stage II disease
Committee felt that……….
• Older IIC is redundant
• Prognostic difference exists between stage IIA and IIB
(5 year OS 78% and 73% respectively)
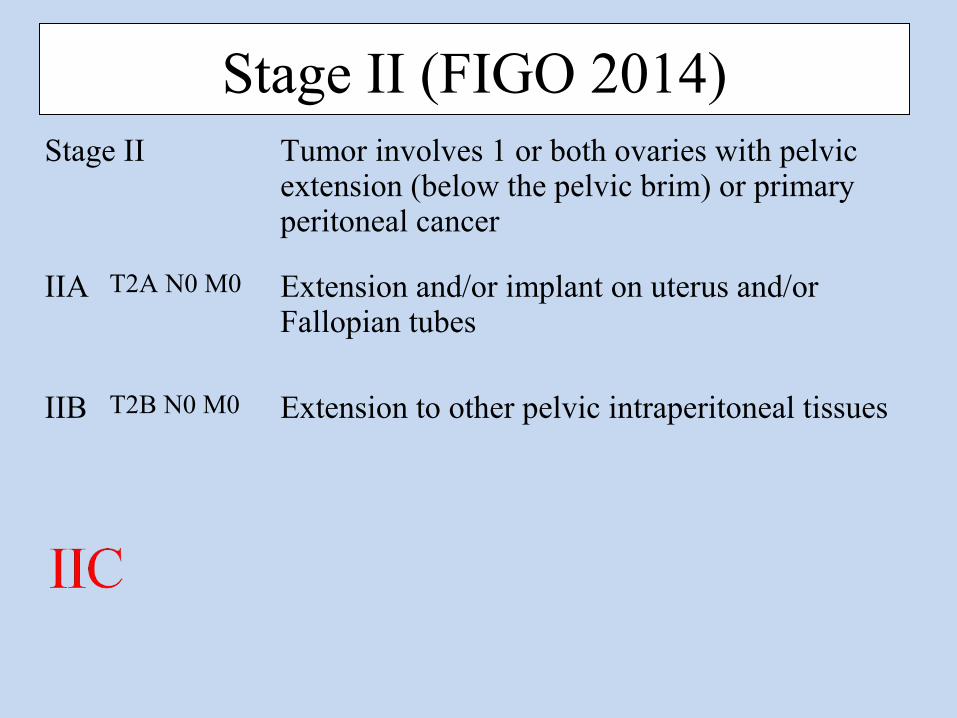
Stage II (FIGO 2014)Stage II Tumor involves 1 or both ovaries with pelvic
extension (below the pelvic brim) or primary peritoneal cancer
IIB T2B N0 M0 Extension to other pelvic intraperitoneal tissues
Stage III (FIGO, 1988)Stage III Growth involving one/ both ovaries with peritoneal implants outside
the pelvis and/ or retroperitoneal and/or inguinal lymph nodes.Superficial liver metastasis equals stage III.Tumour limited to true pelvis but histologically proven malignant extension to small bowel and omentum.
IIIA Tumour grossly limited to true pelvis with negative nodesBut histologically confirmed microscopic seeding of abdominal peritoneal surface
IIIB Tumour of one or bothe ovariesWith histologically confirmed implants on abdominal peritoneal surface, none more than 2 cm in diameter, node negative
IIIC Abdominal implants more than 2 cm diameterAnd/or retroperitoneal or inguinal lymph nodes or both
Controversies
Lymph nodes- in IIIC ???
1. Diffuse omental and peritoneal disease
2. Only lymph node involvement without any other evidence of intra-abdominal disease (<10% of apparent stage I tumours)
• The 2nd group has better prognosis in terms of DFS and OS1-4
1. Onda, T., Yoshikawa, H., Yasugi, T., Mishima, M., Nakagawa, S., Yamada, M. et al. Patients with ovarian carcinoma upstaged to stage III after systematic lymphadenctomy have similar survival to Stage I/II patients and superior survival to other Stage III patients. Cancer. 1998; 83: 1555–1560
2. Kanazawa, K., Suzuki, T., and Tokashiki, M. The validity and significance of substage IIIC by node involvement in epithelial ovarian cancer: impact of nodal metastasis on patient survival. Gynecol Oncol. 1999; 73: 237–241
3. Cliby, W.A., Aletti, G.D., Wilson, T.O., and Podratz, K.C. Is it justified to classify patients to Stage IIIC epithelial ovarian cancer based on nodal involvement only?. Gynecol Oncol. 2006; 103: 797–801
4. Ferrandina, G., Scambia, G., Legge, F., Petrillo, M., and Salutari, V. Ovarian cancer patients with "node-positive-only" Stage IIIC disease have a more favorable outcome than Stage IIIA/B. Gynecol Oncol. 2007; 107: 154–156
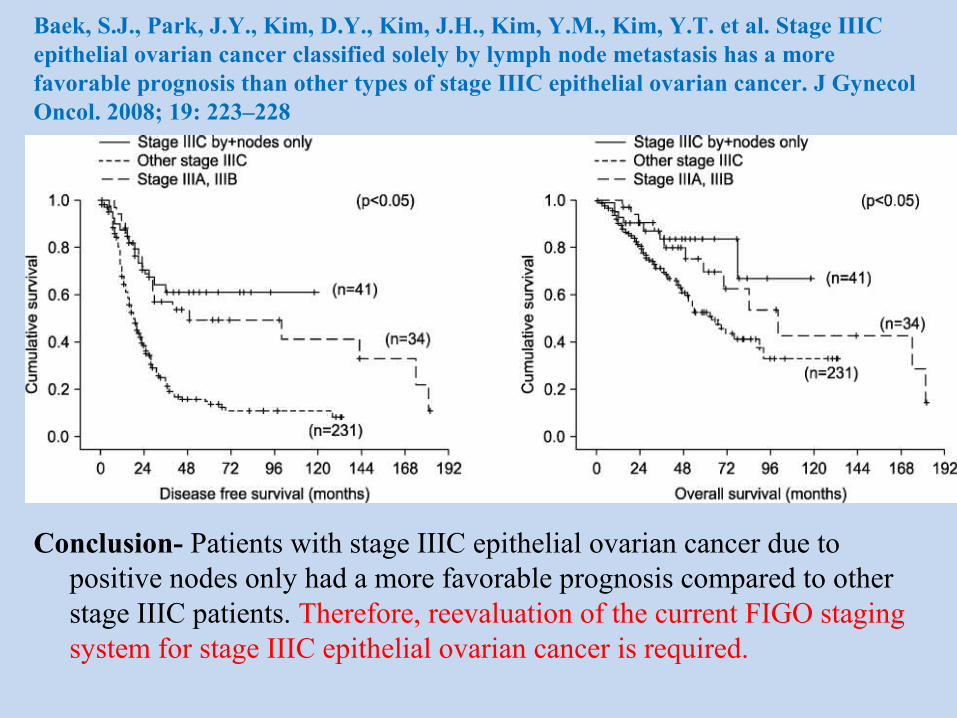
Baek, S.J., Park, J.Y., Kim, D.Y., Kim, J.H., Kim, Y.M., Kim, Y.T. et al. Stage IIIC epithelial ovarian cancer classified solely by lymph node metastasis has a more favorable prognosis than other types of stage IIIC epithelial ovarian cancer. J Gynecol Oncol. 2008; 19: 223–228
Conclusion- Patients with stage IIIC epithelial ovarian cancer due to positive nodes only had a more favorable prognosis compared to other stage IIIC patients. Therefore, reevaluation of the current FIGO staging system for stage IIIC epithelial ovarian cancer is required.
The Committee felt that…………• RPLN involvement only- in IIIA1,
rather than IIIC
• Stage IIIA1 is further subdivided into
• Involvement of retroperitoneal lymph nodes must be proven cytologically or histologically
IIIA1 (i) Mets ≤10 mm in greatest dimension
IIIA1 (ii) Mets >10 mm in greatest dimension
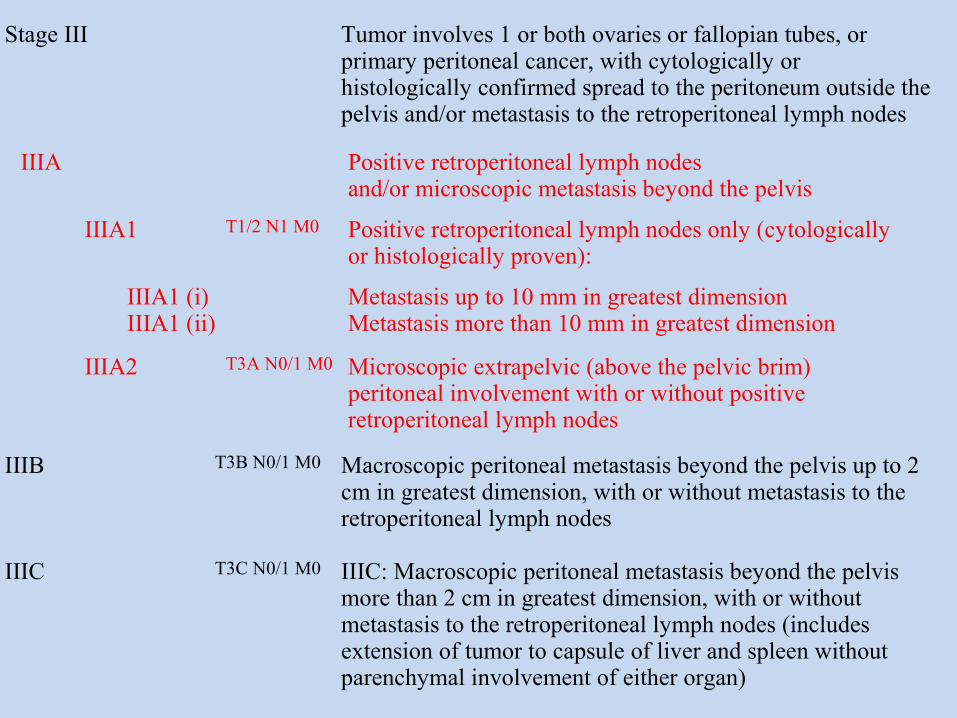
Stage III (FIGO, 2014)
Stage III Tumor involves 1 or both ovaries or fallopian tubes, or primary peritoneal cancer, with cytologically or histologically confirmed spread to the peritoneum outside the pelvis and/or metastasis to the retroperitoneal lymph nodes
IIIB T3B N0/1 M0 Macroscopic peritoneal metastasis beyond the pelvis up to 2 cm in greatest dimension, with or without metastasis to the retroperitoneal lymph nodes
IIIC T3C N0/1 M0 IIIC: Macroscopic peritoneal metastasis beyond the pelvis more than 2 cm in greatest dimension, with or without metastasis to the retroperitoneal lymph nodes (includes extension of tumor to capsule of liver and spleen without parenchymal involvement of either organ)
IIIA1 T1/2 N1 M0 Positive retroperitoneal lymph nodes only (cytologically or histologically proven):
IIIA1 (i) IIIA1 (ii)
Metastasis up to 10 mm in greatest dimension Metastasis more than 10 mm in greatest dimension
IIIA2 T3A N0/1 M0 Microscopic extrapelvic (above the pelvic brim) peritoneal involvement with or without positive retroperitoneal lymph nodes
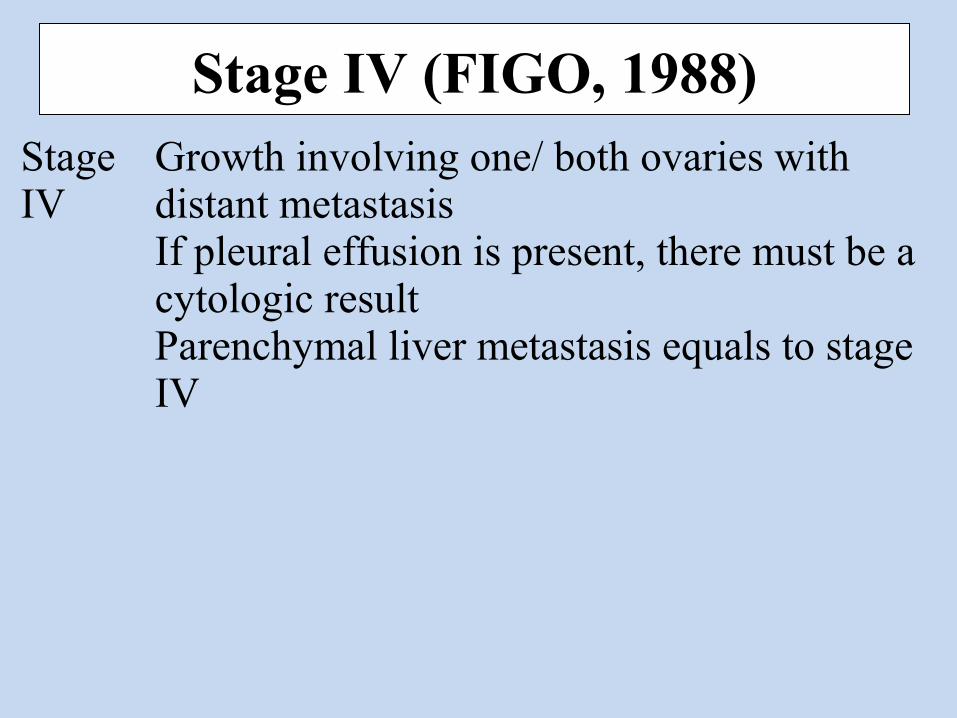
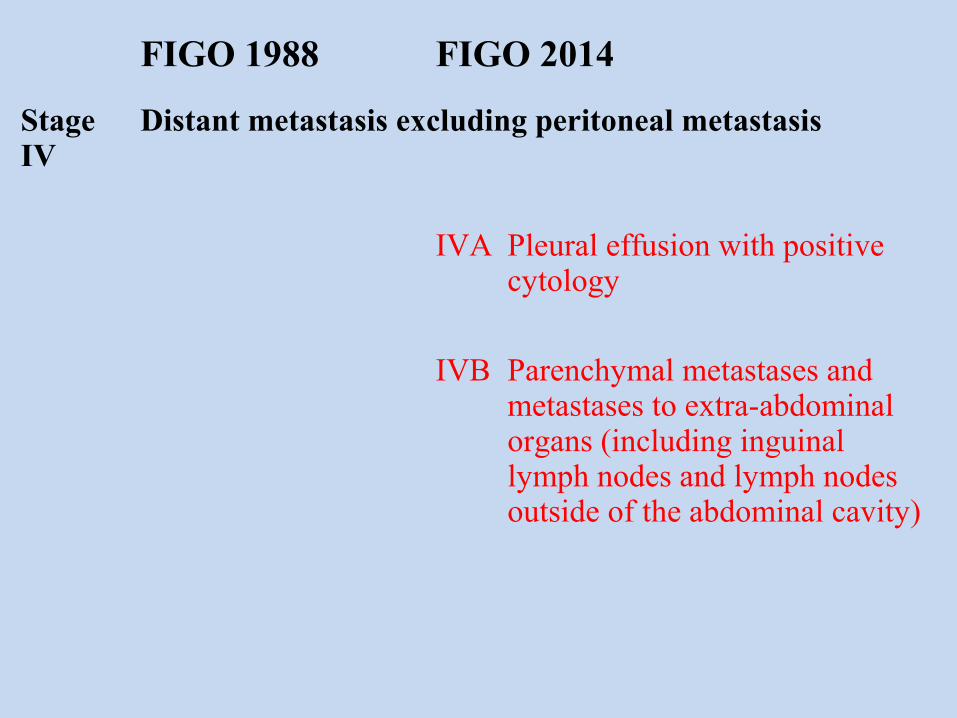
Stage IV (FIGO, 1988)Stage IV
Growth involving one/ both ovaries with distant metastasisIf pleural effusion is present, there must be a cytologic resultParenchymal liver metastasis equals to stage IV
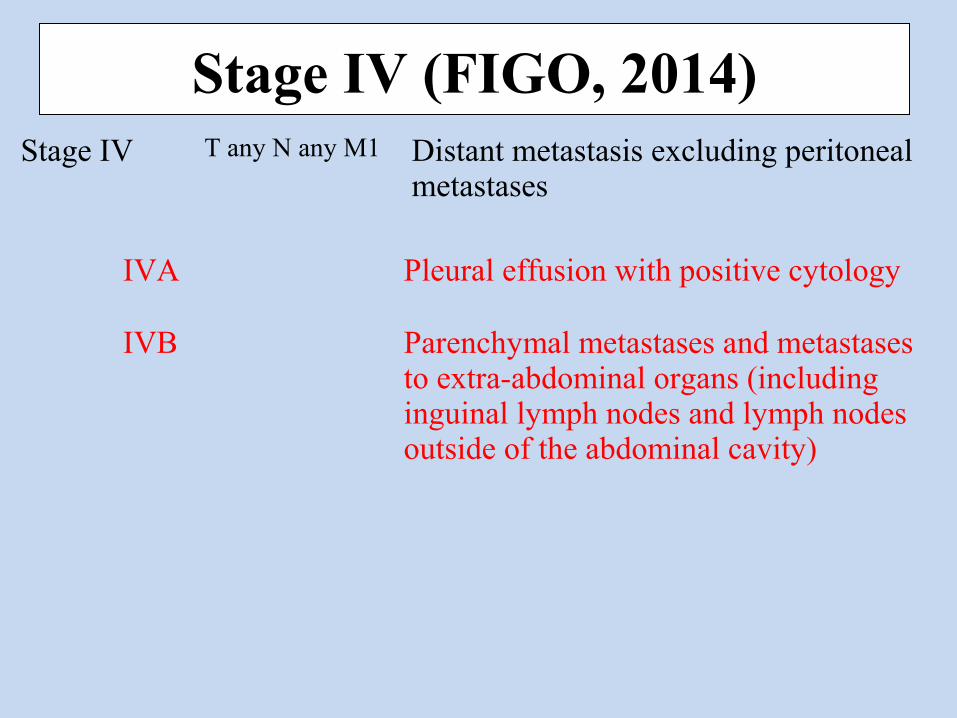
Stage IV (FIGO, 2014)Stage IV T any N any M1 Distant metastasis excluding peritoneal
metastases
IVA Pleural effusion with positive cytology
IVB Parenchymal metastases and metastases to extra-abdominal organs (including inguinal lymph nodes and lymph nodes outside of the abdominal cavity)
Controversies left behind
Abdominal Involvement• Umbilicus
Represents peritoneal extension into the urachal remnant- IIIC or IVB ???
• Isolated parenchymal liver/ spleen metastasis
IIIC or IVB ???
Splenectomy
• Till date, the committee considers them stage IVB
Other Changes
Primary site
Should be designated where possible
• Ovary
• Fallopian tube
• Peritoneum
• “Undesignated”- when not possible to delineate the primary site clearly
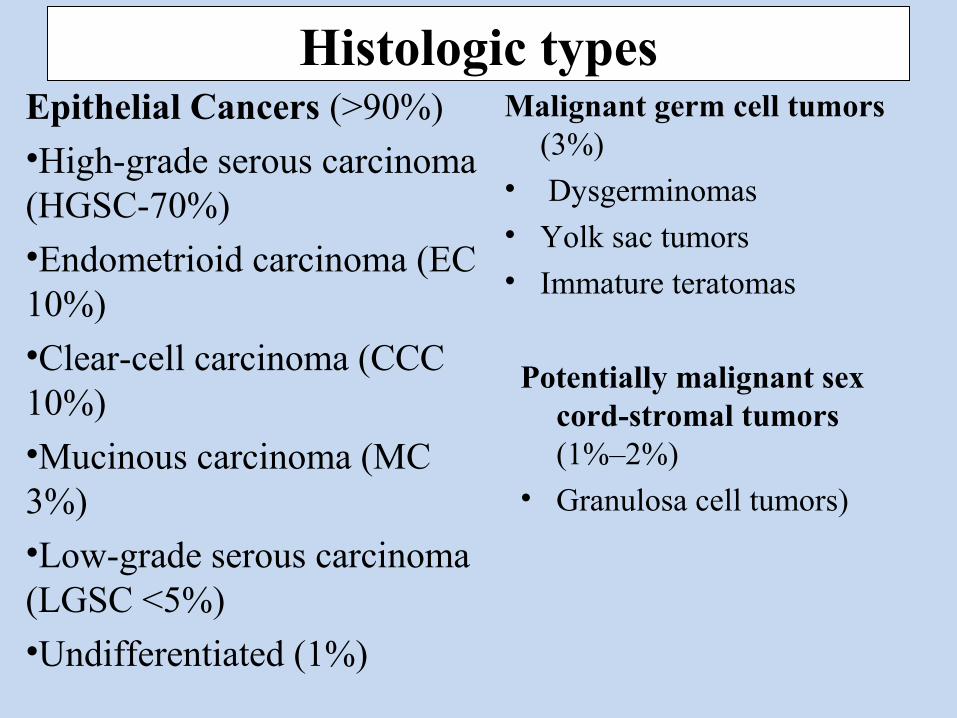
Histologic typesEpithelial Cancers (>90%)
•High-grade serous carcinoma (HGSC-70%)
•Endometrioid carcinoma (EC 10%)
•Clear-cell carcinoma (CCC 10%)
•Mucinous carcinoma (MC 3%)
•Low-grade serous carcinoma (LGSC <5%)
•Undifferentiated (1%)
Malignant germ cell tumors (3%)
• Dysgerminomas
• Yolk sac tumors
• Immature teratomas
Potentially malignant sex cord-stromal tumors (1%–2%)
• Granulosa cell tumors)
To summarize
• Comprehensive surgical staging
• Histological type should be included
• Primary site should be mentioned wherever possible
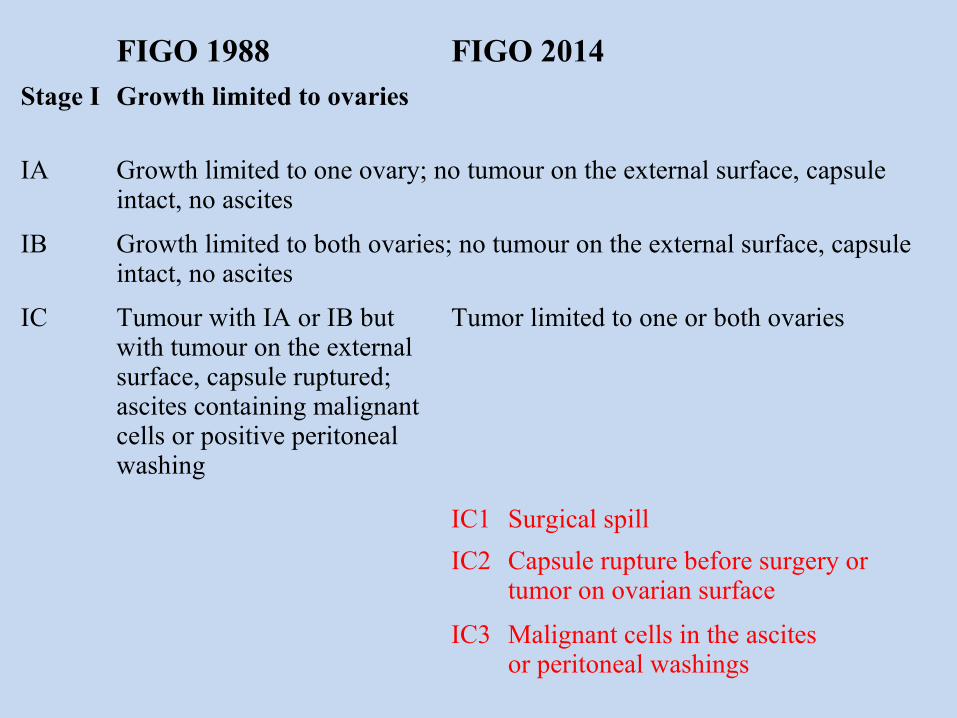
FIGO 1988 FIGO 2014Stage I Growth limited to ovaries
IA Growth limited to one ovary; no tumour on the external surface, capsule intact, no ascites
IB Growth limited to both ovaries; no tumour on the external surface, capsule intact, no ascites
IC Tumour with IA or IB but with tumour on the external surface, capsule ruptured; ascites containing malignant cells or positive peritoneal washing
Tumor limited to one or both ovaries
IC1 Surgical spill
IC2 Capsule rupture before surgery or tumor on ovarian surface
IC3 Malignant cells in the ascitesor peritoneal washings
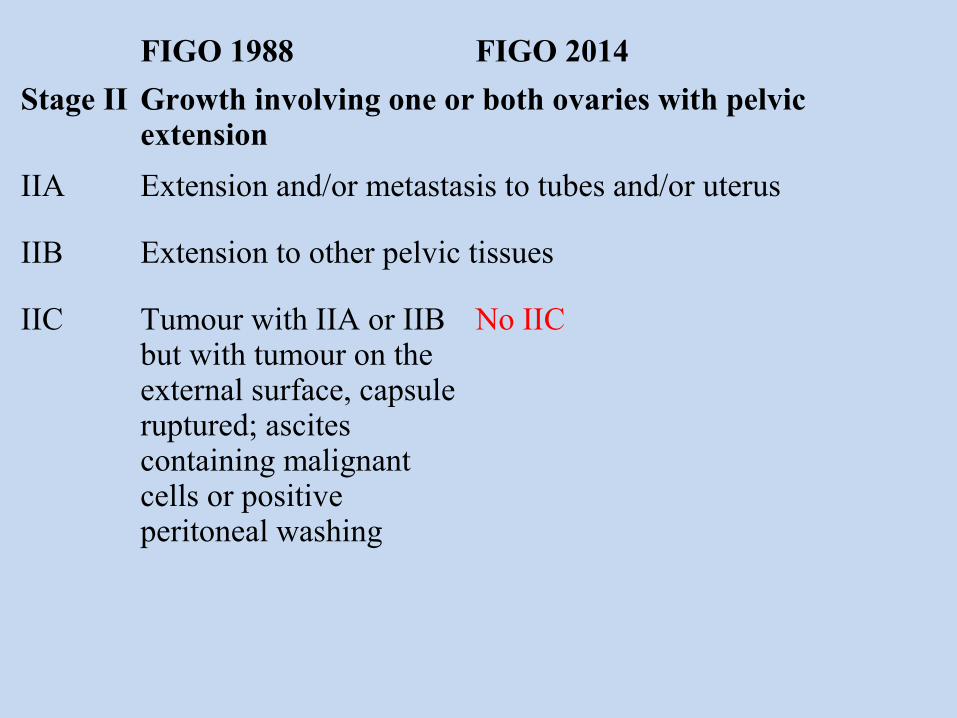
FIGO 1988 FIGO 2014
Stage II Growth involving one or both ovaries with pelvic extension
IIA Extension and/or metastasis to tubes and/or uterus
IIB Extension to other pelvic tissues
IIC Tumour with IIA or IIB but with tumour on the external surface, capsule ruptured; ascites containing malignant cells or positive peritoneal washing
No IIC
FIGO 1988 FIGO 2014
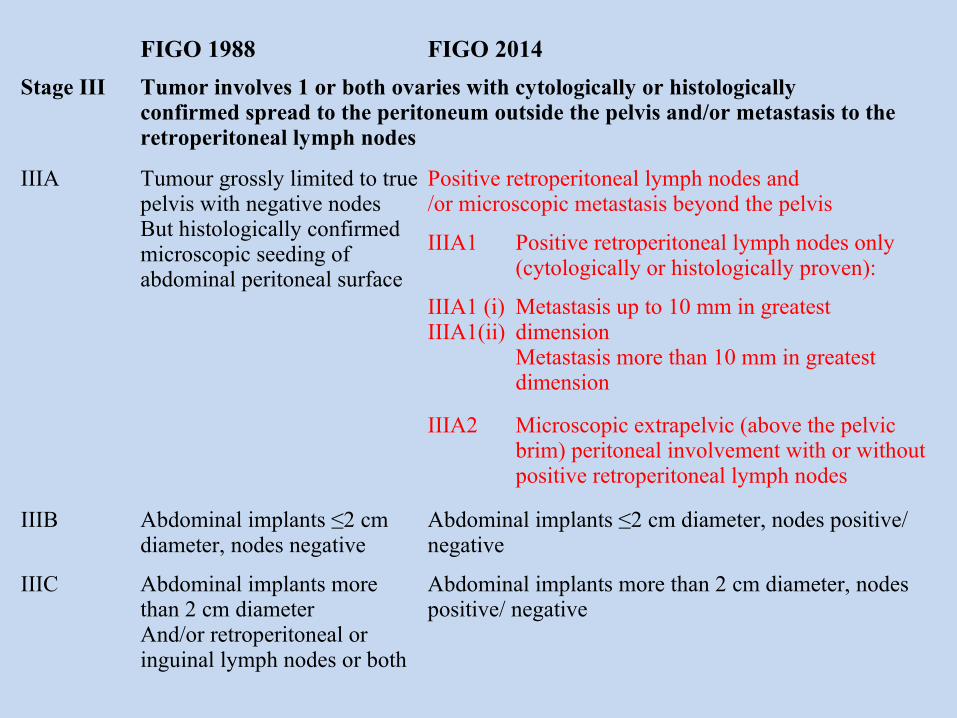
Stage III Tumor involves 1 or both ovaries with cytologically or histologicallyconfirmed spread to the peritoneum outside the pelvis and/or metastasis to theretroperitoneal lymph nodes
IIIA Tumour grossly limited to true pelvis with negative nodesBut histologically confirmed microscopic seeding of abdominal peritoneal surface
Positive retroperitoneal lymph nodes and/or microscopic metastasis beyond the pelvis
IIIA1 Positive retroperitoneal lymph nodes only (cytologically or histologically proven):
IIIA1 (i)IIIA1(ii)
Metastasis up to 10 mm in greatest dimensionMetastasis more than 10 mm in greatest dimension
IIIA2 Microscopic extrapelvic (above the pelvic brim) peritoneal involvement with or without positive retroperitoneal lymph nodes
IIIB Abdominal implants ≤2 cm diameter, nodes negative
Abdominal implants ≤2 cm diameter, nodes positive/ negative
IIIC Abdominal implants more than 2 cm diameterAnd/or retroperitoneal or inguinal lymph nodes or both
Abdominal implants more than 2 cm diameter, nodes positive/ negative