38
1 Government of Samoa 2010-2015 National Health Promotion Policy

1
Government of Samoa
2010-2015
National Health Promotion Policy

2
FOREWORD
I am pleased to introduce this policy regarding health promotion in Samoa.
As stipulated in the Health Sector Plan 2008-2018, the Ministry of Health (MOH) is devoted to promoting good health for the whole nation as a major strategic action in achieving the common vision of A Healthy Samoa. This vision dates back to Samoa’s response to the ‘Health for All’ goal of
the Alma Ata Declaration on Primary Health Care (1978); followed by the Ottawa Charter on Health Promotion (1986); the New Horizons in Health (1995) for the WHO Western Pacific Region; and the Pacific Health Ministers Yanuca Islands Declaration on Health in the Pacific in the 21st Century, (1995), which adopted the vision of Healthy Islands. The MOH contributes through the promotion of healthy lifestyles for all Samoans and ensures that the onus is on people’s health and wellbeing before the incidence of ill health. The Healthy Islands concept articulated within the Yanuca Islands Declaration is premised on the principles of “Health Promotion” and “Health Protection” the coordination of which are practically realized in Samoa by the MOH according to its mandated duties. The MOH launched and leads implementation of health promotion activities since 1996 within settings such as Healthy Hospitals, Healthy Markets, Health Promoting Schools and the National Church Health Promotion Programme, additionally, the Parliamentary Advocacy Group for Healthy Living. The idea of healthy living is promoted and backed by Samoa’s political leaders, so as to ensure that we keep people healthy and away from hospitals for as long as it is possible due to our limited facilities, limited workforce and capacity. When people fall sick, they are given quality health care within the context of our health system. This policy document seeks to guide a nation-wide collaborative effort in achieving a common goal by encouraging all Samoans to have control over their health and to take necessary steps in reversing the increasing trends of noncommunicable diseases. It identifies issues and outlines an achievable set of strategies to guide all agencies in Samoa who are involved in any form of health promotion activity to adopt the proven, effective approaches of community mobilization and the creation of enabling and supportive environments. The Health Promotion Policy is a major step in achieving the objective of “strengthening health promotion and primordial prevention” as articulated in the Health Sector Plan 2008-2018. I would like to acknowledge all those who contributed to the development of this document and commend the health sector partnership which has resulted in this Health Promotion Policy. Faafetai,
Palanitina Tupuimatagi Toelupe Director General & CEO - MOH
3
ACKNOWLEDGEMENTS This National Health Promotion Policy has been commissioned and supported by the Ministry of Health, through development and coordination from the Policy Unit, Strategic Development and Planning Division. A technical consultant, Mr Chris Hagarty of the Burnet Institute, Australia, was recruited through the Health Sector Wide Approach Programme (SWAp) to facilitate consultation for, and drafting of the Policy.

4
TABLE OF CONTENTS
FOREWORD ..................................................................................................................... 2
ACKNOWLEDGEMENTS ................................................................................................... 3
ABBREVIATIONS.............................................................................................................. 5
INTRODUCTION .............................................................................................................. 6
VISION ............................................................................................................................ 9
AIM ................................................................................................................................. 9
SITUATIONAL ANALYSIS ................................................................................................ 10
LEGISLATIVE AND POLICY FRAMEWORK ....................................................................... 14
KEY STRATEGIC AREAS .................................................................................................. 17
KSA 1: STRENGTHEN AND BUILD HEALTHY PUBLIC POLICIES. ................................................... 17
KSA 2: CREATE ENABLING AND SUPPORTIVE ENVIRONMENTS. ................................................. 18
KSA 3: STRENGTHEN COMMUNITY ACTION. ........................................................................ 19
KSA 4: BUILD AND DEVELOP PERSONAL LIFE SKILLS FOR INDIVIDUALS. ....................................... 19
KSA 5: CONTINUE TO STRENGTHEN REORIENTATION OF HEALTH SERVICES. ................................. 21
IMPLEMENTING THE NATIONAL HEALTH PROMOTION POLICY .................................... 23
STRATEGIC PLAN OF ACTION ........................................................................................ 27
REFERENCES .................................................................................................................. 34
COMMUNITY SUMMARY .............................................................................................. 35
5
ABBREVIATIONS AusAID Australian Agency for International Development
AIDS Acquired Immuno-Deficiency Syndrome
HIV Human Immunodeficiency Virus
KSA Key Strategic Area
MDGs Millennium Development Goals
MOH Ministry of Health
NCC National Council of Churches
SPC Secretariat for the Pacific Community
TTM Tupua Tamasese Meaole National Hospital, Apia
UN-OHCHR United Nations Office of the High Commissioner for Human Rights
WHO World Health Organization
WHO-WPRO WHO Regional Office for the Western Pacific
6
INTRODUCTION The Samoa Ministry of Health, as is clearly articulated in its Health Sector Plan, 2008-2018, is committed to supporting nation-wide health promotion as a major strategic action towards achieving its common vision of “A Healthy Samoa”1. In recognising that many of the major threats to the health of the people of Samoa are preventable through healthy lifestyle choices, the health sector in Samoa finds itself at a cross-roads; either it continues to commit its resources to curative services which attempt to treat an individual after they experience the effects of ill health, or it redistributes a portion of its resources and expertise to the promotion of healthy lifestyles for all Samoans before the onset of ill-health and suffering. It is understood that by focusing its attention on promoting healthy lifestyles, and thereby preventing the onset of many of the sources of ill health in Samoa (such as non-communicable diseases; stroke, heart disease, diabetes, and other diseases such as typhoid and dengue fever), the health sector could succeed in easing the financial and human resource burden on the hospitals and clinics of the country. This financial burden is evident through the recent National Health Accounts 2006/2007 which shows that 26.4% of Total Health Expenditures is currently being spent on Inpatient Curative Care (local 17%, overseas 9.4%). This National Health Promotion Policy has been developed by the Samoa Ministry of Health, through consultation with partner government ministries, non-government organisations and community stakeholders. Rather than being a document which guides the actions of the Ministry of Health alone, the National Health Promotion Policy belongs to all Samoans, and seeks to guide a nation-wide collaboration which uses Samoa’s proven, traditional capacity to work together towards a common goal; to encourage and enable its citizens to assume control over their health, and to take the necessary steps to reverse the rising tide of preventable ill-health. The development and endorsement of this Policy is a major step toward the Ministry of Health enacting one of its key strategies under its Health Sector Plan, 2008-2018, and achieving its objective “to strengthen health promotion and primordial prevention”2.
1 Samoa Ministry of Health (2008). Health Sector Plan, 2008-2018. Apia, Samoa Ministry of Health. 2 Ibid.

7
Health promotion is a process. Health promotion is the process of enabling people to increase control over, and to improve their health by focusing on the social, environmental and economic conditions which impact on health and well being. It is based on the understanding that health is not merely the absence of disease, but rather a state of complete physical, spiritual and mental well being, which is influenced by a number of social, environmental and economic factors, known as ‘determinants of health’3. The process of health promotion works to encourage individuals and communities to adopt healthier behaviours and to make healthier choices throughout their lives. It does this through two main ways;
i. The mobilisation (bringing together) of communities to work together towards healthier lifestyles, and
ii. The influencing of social conditions to create a suitable environment which enables and supports communities and individuals to make appropriate, healthy choices.
Community mobilisation: The community mobilisation aspect of health promotion recognises that individuals and communities have unique capacities and strengths with which to address problems which affect them, and that they are in the best position to ensure that they do this in a suitable, culturally acceptable way. Health promotion therefore seeks to work with individuals and communities to identify;
i. their own health and social needs, and ii. actions through which to address these.
As a process, health promotion aims to mobilise communities and groups to work together, using their strengths and intimate knowledge of their culture and practices to address the ‘determinants of health’ which affect themselves and their community. The process of communities coming together to identify and address their problems and concerns is as essential to the long-term achievement of health and well being as the implementation of any activities which may arise from the process. Creating enabling and supportive environments: In addition to mobilising communities to take control of the factors which can adversely affect their health and social development, health promotion also recognises that some of the determinants of health which affect individuals and communities are beyond their control, and so seeks to influence the environment in which communities live, so that they are enabled and supported in their efforts to make healthy choices.
3 WHO. (2010). "Ottawa Charter for Health Promotion, 1986." Retrieved 21st April, 2010, from http://www.who.int/healthpromotion/conferences/previous/ottawa/en/.

8
Part of this process utilises the concept of ‘primordial prevention’; the prevention of risk factors which could adversely affect determinants of health before they can be introduced to individuals and communities. The creation of enabling and supportive environments therefore contributes to the Samoa health sector’s objective “to strengthen health promotion and primordial prevention”4. Health Promotion in Action – an example.
A community came together, and through discussion about their health, identified that diabetes and heart disease cause many of their community to spend time in hospital each year. After receiving advice from a community nurse that a high-fat diet contributes to these diseases, they came to recognise that they consume too much harmful fat in their diet, and they decided that they would eat healthier, less-fatty cuts of meat.
This decision would have been a difficult one to achieve before, because their closest stores stocked only imported mutton flaps, turkey tails and high-fat chicken legs, however recent changes to government importation legislation had made it more affordable for stores to stock quality, local beef and chicken products, which are much lower in fat.
In this example, the coming together of the community (community mobilisation) led to the realisation that many in their community were suffering from diabetes and heart disease, and between them, their community was making many trips to the clinics and hospitals each year to seek treatment for these problems. Together, the community was able to arrive at a decision on how to make healthier eating choices, however their intention to eat less-fatty meat was dependant on healthier meat being available to them.
This was made possible by government legislation on imported meat products, which made it less financially attractive for importers, wholesalers and stores to stock fatty meat products. The changing of government legislation contributed to creating an enabling and supportive environment in which the community was able to pursue healthier eating choices.
4 Samoa Ministry of Health (2008). Health Sector Plan, 2008-2018. Apia, Samoa Ministry of Health.

9
VISION All individuals and communities in Samoa are enabled and supported to lead healthier lives through having control over their health and well being, throughout their life-cycle. The vision for this National Health Promotion Policy will contribute to the achievement of the health sector’s common vision of “A Healthy Samoa”, as stipulated in the Health Sector Plan, 2008-20185. The vision is based on the philosophy of achieving long-term, sustainable improvements to the health and well being of individuals and communities through empowering and supporting them to utilise their collective strengths, capacities and resources towards the achievement of their own, identified health and social goals.
AIM The aim of this National Health Promotion Policy is; To guide all agencies, organisations and groups in Samoa who are involved in the delivery of health promotion activities to engage in empowering partnerships which enable and support individuals and communities to have control over their health and well being.
5 Samoa Ministry of Health (2008). op. cit.
10
SITUATIONAL ANALYSIS: DEVELOPING A COMMUNITY-DRIVEN HEALTH PROMOTION MODEL FOR SAMOA The concept of health promotion being a process which addresses the determinants of health was first developed and articulated throughout the world with the signing of the Ottawa Charter for Health Promotion in 19866. This event triggered an international movement which sought ‘health’ as the goal (rather than the prevention of disease), and sought to achieve healthy lifestyles through the core concepts of individual and community mobilisation, and the creation of enabling and supportive environments. In 1995, the World Health Organization’s Regional Office for the Western Pacific (WHO-WPRO) launched its policy document, New Horizons in Health, which presented the Ottawa Charter’s concepts in an appropriate framework for the region (WHO, 1995a)7. Shortly afterwards, at a meeting of Health Ministers from Pacific Island nations on Yanuca Island, Fiji, this was further adapted into a concept specifically targeting the geographical, environmental and cultural uniqueness of the Pacific. The Yanuca Island Declaration clearly articulated the way forward for Pacific Island countries to implement health promotion activities which utilised the concepts of community mobilisation and creation of enabling and supportive environments8. Following this, many of these newly named, ‘Healthy Islands’ initiatives commenced throughout the Pacific, achieving varying levels of success through a number of health promotion initiatives, such as;
Community malaria prevention and control, and improved household sanitation and waste management in Solomon Islands.
Village-identified and driven environmental health activities through the development of a village environmental health workforce in Fiji.
National, multi-sectoral strategic plans driven by community-identified environmental health priorities in Fiji.
Convening of Health Promotion Councils to coordinate community-identified initiatives for prevention and control of both communicable and non-communicable diseases in Kiribati and Tuvalu.
Establishment of local committees to identify and enact initiatives for prevention and control of non-communicable diseases in Cook Islands and Niue9.
6 WHO. (2010). op. cit. 7 WHO (1995a). New Horizons in Health. Manila, WHO Regional Office for the Western Pacific. 8 WHO (1995b). Yanuca Island Declaration. Manila, WHO regional Office for the Western Pacific. 9 Galea, G., B. Powis, et al. (2000). "Healthy Islands in the Western Pacific: international settings development." Health Promotion International 15(2): 169-78.
11
Samoa launched its inaugural Healthy Islands initiative in 1998, in the form of the Aiga ma Nu’u Manuia (Healthy Homes, Healthy Villages) programme, which saw village women’s committees come together to identify their community health and social needs, particularly in regards to their physical environment, and to mobilise their communities to work together to address these10. Led by a multi-sectoral steering committee and coordinated by the Ministry of Women, Community and Social Development, the programme has been implemented in 183 villages across the country, and has facilitated entry from different ministries on a range of activities which have succeeded in increasing the self-reliance and empowerment of communities to identify, manage and seek appropriate support for community development initiatives11. Utilising the Healthy Islands concepts articulated within the Yanuca Island Declaration, the Ministry of Health also led the implementation of health promotion activities within other settings, including;
Healthy Hospital: The Hospital Management Committee at the TTM National Hospital, Apia, is tasked with ensuring the hospital environment is a safe and healthy place in which to work, visit or stay as a patient or carer. The Committee undertakes periodic needs assessment and monitoring for the identification of factors which contribute to the promotion or inhibition of healthy lifestyles within the hospital, which in turn leads to planning and implementation of health-improvement and behaviour change promotion activities. Teams of staff are mobilised for grounds clean-up and maintenance, and to both coordinate and participate in group activities to promote physical exercise. Another successful initiative of the Committee has been to provide participative, patient-oriented group, and one-to-one health information sessions.
Healthy Markets: Committees of market managers, vendors and patrons were mobilised in each of Apia’s two main markets, and supported by personnel from the Ministry of Health’s Environmental Health Section to undertake periodic needs assessments for the identification of issues, practices and behaviours which have the potential to impact upon the health and well being of the communities which work in, and access the markets. Initiatives have led to the market communities taking responsibility for food safety and environmental sanitation, and have led market vendors in group physical activity. The Ministry of Health has also been invited to deliver health promotion messages and to conduct health assessment activities in the markets.
Health Promoting Schools: This country-wide programme was developed for implementation in government primary schools, in order to address the environmental and behavioural factors which could impact on the determinants
10 Samoa Ministry of Health (2008). op. cit. 11 Galea, G. et al. (2000). op. cit.

12
of health and well being of the students, their families and teaching staff. Led and supported by the Ministries of Health and Education, Sport and Culture, school committees of community leaders and school principles were supported to undertake a health and social needs assessment, and to prioritise actions for health and social improvement. School communities have been mobilised to implement action plans, which have included the initiation of tobacco-free school campaigns, improvements to water supply and sanitation systems and healthier nutritional plans for school canteens.
National Church Health Promotion Programme: The National Council of Churches (NCC) and the Ministry of Health have developed a Facilitation Package which will see key representatives of the NCC trained in the community mobilisation approach to health promotion. These trained, NCC Facilitators will be tasked with the role of supporting Church Committees across the country to mobilise their communities for the identification of their health and social needs, and the development and implementation of action plans to address these.
These health promotion activities have proven extremely successful in mobilising and empowering communities and other stakeholders to work together towards the identification of health and social needs, and the development of culturally appropriate and acceptable initiatives with which to address these. These initiatives have facilitated the fruitful engagement of personnel from a number of government ministries with individuals and other stakeholders at the community level, creating valuable two-way transfer of information and learning which will help to ensure that future initiatives utilise community mobilisation for the development of realistic goals and outcomes. Beyond community mobilisation, for Samoa to achieve its full commitment through the endorsement of the Yanuca Island Declaration, it must meet the challenge of initiating systematic approaches which create enabling environments that support the improved healthy behaviours identified by communities. To this end, the Ministry of Health and other interested, influential stakeholders have embarked on building capacity within Samoa to make this happen. A National Health Promotion Council comprising multi-sectoral, senior officials from a number of key ministries was convened some years ago to coordinate health promotion activities in the country. Although this Council is currently inactive, it was successful in sensitising those participating ministries to the concepts identified in the Healthy Islands approach to health promotion. Additionally, a Parliamentary Advocacy Group for Healthy Living, comprising the Parliamentary Speaker, a number of prominent members of both leading political parties and the Director General/Chief Executive Officer for the Ministry of Health was convened to explore options for the coordination of national health promotion activities. The Group has visited Health Promotion Foundations in Australia and Thailand to

13
investigate appropriate methods for implementing community-led approaches to health promotion, and to sensitise the political community to this. These multi-sectoral bodies have, and continue to contribute to a legislative and political environment which is aware and supportive of the community-driven approach to health promotion. With their support, and through endorsement of the Cabinet, this National Health Promotion Policy will guide and assist all agencies in Samoa who are involved in any form of health promotion activity to adopt the proven, effective approaches of community mobilisation and the creation of enabling and supportive environments.
14
LEGISLATIVE AND POLICY FRAMEWORK The development of Samoa’s participatory, community mobilisation approach to health promotion and this Policy’s aim to further develop this concept to encourage multi-sectoral collaboration in the creation of enabling and supportive environments for communities to achieve healthy behaviour change have been informed through a number of international legislations, treaties, conventions, declarations and frameworks. The following list identifies the key, international legislative documents which have led to the conception, development and implementation of the health promotion approach adopted by Samoa under this Policy;
Declaration of Alma Ata, International Conference on Primary Health Care, 1978. The Ottawa Charter for Health Promotion, 198612. The Universal Declaration of Human Rights, 194813. New Horizons in Health, 199514. Yanuca Island Declaration, 199515. Millennium Development Goals (MDGs), 2000-2015 16 , specifically MDG3
(promote gender equality and empower women), MDG4 (reduce child mortality), MDG5 (improve maternal health), MDG6 (combat HIV/AIDS, malaria and other diseases) and MDG7 (ensure environmental sustainability).
Regional Framework for Health Promotion, 2002-200517. Tonga commitment to promote healthy lifestyles and supportive environment,
200318. Samoa commitment: achieving healthy islands, 200519.
Within Samoa, the Ministry of Health Act, 200620, as the overarching Act for the provision and regulation of health services in the country, is the key legislative document which informs this National Health Promotion Policy. The Act specifically instructs the Ministry of Health to prioritise “…policies, programmes and practices which increase the capacity of the people of Samoa to have greater access to and control over and participation in their health and well being”.
12 WHO. (2010). op. cit. 13 UN-OHCHR. (2010). "Universal Declaration of Human Rights." Retrieved 6th May, 2010, from http://www.ohchr.org/en/udhr/pages/introduction.aspx. 14 WHO, (1995a). op. cit. 15 WHO, (1995b). op. cit. 16 AusAID. (2010). "The Millennium Development Goals: the fight against global poverty and inequality." Retrieved 6th May, 2010, from http://www.ausaid.gov.au/keyaid/mdg.cfm 17 WHO-WPRO (2005). Regional Framework for Health Promotion, 2002-2005, Manila, WHO-WPRO. 18 WHO-WPRO (2003). Tonga commitment to promote healthy lifestyles and supportive environment. Manila, WHO-WPRO. 19 WHO-WPRO (2005). Samoa commitment: achieving healthy islands: conclusions and recommendations. Manila, WHO-WPRO. 20 (2006). Ministry of Health Act 2006. 19. Samoa.
15
Under this Act, the Ministry of Health is tasked with the responsibility of periodically reviewing and amending the National Health Promotion Policy, and in accordance with the Policy’s development, this should be conducted through consultation with communities and appropriate, multi-sectoral stakeholders. Other legislative documents in Samoa which have the potential to impact upon the determinants of health of individuals and communities include;
Tobacco Control Act, 2008. Food and Drugs Act, 1967. Mental Health Act, 2007. Occupational Safety and Health Act, 200221.
Other legislative documents which govern the actions and responsibilities of agencies and individuals which may contribute to enacting the National Health Promotion Policy include;
National Kidney Foundation of Samoa Act, 2005. Oceania University of Medicine (Samoa) Act, 2002. Samoa Red Cross Act, 1993.
Within the Ministry of Health’s suite of policies, the following documents relate directly to the effective enactment of the National Health Promotion Policy;
National Child Health Policy. National Food and Nutrition Policy. National HIV/AIDS Policy. Safe Motherhood Policy. TTM Healthy Hospital Policy. Samoa Mental Health Policy. National Non-Communicable Disease Policy. National General Prevention Policy. National Tobacco Control Policy. National Sexual and Reproductive Health Policy. National Primary Health Care Policy.
Under direction from other ministries, the following policies and documents also relate directly to the effective enactment of the National Health Promotion Policy;
Strategy for the Development of Samoa, 2008-2012, Ministry of Finance. National Policy for Women of Samoa, 2007-2017, Ministry of Women,
Community and Social Development. National Policy for Children, 2007-2017 (draft), Ministry of Women, Community
and Social Development. National Sanitation Policy, Ministry for Natural Resources and Environment.
21 (2006). Ministry of Health Act 2006. 19. Samoa.

16
A note on Ministry of Health’s monitoring and evaluation responsibilities: As stipulated in its mandate under the Ministry of Health Act 2006, the Ministry is responsible for the regulatory oversight of all health sector activities in the country. As such, the Ministry has been identified in the following monitoring and evaluation framework as having overall responsibility for most of the identified indicators. Should the Ministry decide, at a later time, to task a specific organization, or collection of organizations to coordinate, monitor and evaluate health promotion activities in the country, this will need to be reflected in the framework, and indeed throughout the National Health Promotion Policy.
17
KEY STRATEGIC AREAS The National Health Promotion Policy and its implementation will be guided by the following Key Strategic Areas (KSAs), which are designed to ensure that any agency involved in health promotion activities (or activities of any other name which aim to influence the determinants of health affecting individuals and communities), will do so in accordance with the proven, evidence-based and sustainable approaches adopted under this Policy. It is envisaged that the successful implementation of the Policy relies on genuine partnership and close collaboration amongst multiple partners representing multiple sectors, both within and external to government. Coordination and leadership by the Ministry of Health will be a cornerstone to ensuring all actions implemented under the guidance of the Policy will be done so in accordance with the principles of ava fatafata (fa’a Samoa), respect for others and respect for human rights, as per the Ministry’s mandate values22.
KSA 1: Strengthen and build healthy public policies. KSA 2: Create enabling and supportive environments. KSA 3: Strengthen community action. KSA 4: Build and develop personal life skills for individuals. KSA 5: Continue to strengthen reorientation of health services.
KSA 1: Strengthen and build healthy public policies. The National Health Promotion Policy has been developed for use by all organisations and groups in Samoa, from all sectors, who are engaged in the development of policies, plans and strategies which have the potential to impact upon the population through influencing determinants of health. These could include a variety of sectors, such as transport, public works, trade, agriculture, communications and media, education, law enforcement and of course, health, as decisions made within these sectors have the potential to either limit or expand opportunities for individuals and communities to make healthy choices. The Policy stands as a guide to facilitate decision- and policy-makers from multiple sectors to recognise and consider the health implications of their decisions and actions, and it advocates for multi-sectoral engagement in the policy development process as a means to enabling this. Furthermore, the Policy places equal importance on engaging communities and other stakeholders in the processes of developing and implementing new, guiding policies and plans, so as to ensure these a) reflect and address the
22 Samoa Ministry of Health (2008). op. cit.

18
recognised and identified health and social needs of communities, and b) lead to interventions that are suitable for Samoa’s communities. These processes of multi-sectoral, community and stakeholder engagement aim to foster nation-wide ownership of, engagement in and appropriate implementation of public policy and plans, with a view to achieving more effective, sustainable and positive contributions to the determinants which can impact on the health of all Samoans. Encouraging and guiding the development of healthier public policies is a major contributing factor to the creation of enabling environments which support communities and individuals to make, and achieve healthier choices (see KSA 2).
KSA 2: Create enabling and supportive environments. Health promotion, at its essence, is a process which recognises the unique capacities and strengths within individuals and communities to identify their own health and social needs, and to work together, utilising their skills, available resources and cultural practices to address these needs through the adoption of healthy behaviours or the embracing of health-improving technologies and infrastructure. At the heart of this process is the empowerment of communities; their ownership and control over their own endeavours and destinies. However it is recognised that in the modern environment of local and international trade, media, technology and economics, numerous factors impact on health and well being which are beyond the control of individuals and communities. The challenge for health promotion, therefore, is to engage with multiple sectors to identify and address the barriers which their actions create, and which prevent communities and individuals from being able to action their decisions to make healthier choices or to change their behaviours. The creation of enabling environments which support individuals and communities to address their health and social needs requires action at every level through the guiding principle of mutual respect; for individuals, for communities, for the environment, for property and for human rights. At the community level, respect for the rights of family members, neighbours and others to make healthier decisions in their lives, and to participate in community-driven actions which contribute to a healthier lifestyle is at the core of creating an environment in which everybody, regardless of their gender, religious or political affiliation, socioeconomic status, physical and mental abilities, can benefit from. At the sub-national and national levels, governments have an obligation to respect their citizens’ rights to choose healthier lifestyles, and as part of their duty-of-care to their

19
people, to direct public spending and resourcing towards actions which create opportunities for community-identified, healthier lifestyle choices. Equally, they must be vigilant in identifying and reversing mechanisms and actions both within and outside their countries which threaten to hinder communities from being able to choose healthier lifestyle alternatives. Regional and international bodies, including trade and investment organisations and donors, also have a responsibility to respect the rights of individuals and communities in countries to direct their lives according to their own, identified health and social needs. International organisations must ensure that their own practices and agendas do not prevent or inhibit communities from making healthy lifestyle choices. National and sub-national legislation and policy development which remove barriers to community empowerment, such as discrimination for certain individuals or groups, is essential to respecting the rights of all individuals to determine their own health and social needs. Likewise, processes which act to limit external, harmful influences on the health of communities must remain a focus of decision-making bodies in Samoa.
KSA 3: Strengthen community action. The effectiveness of health promotion lies in its ability to empower individuals and communities to work together and to utilise their collective strengths and resources to identify and enact healthy lifestyle choices. This process of communities coming together is as essential to the long-term achievement of health and well being as the implementation of any activities which may arise from the process. The community-driven nature of the approach ensures both the cultural appropriateness and long-term sustainability of health benefits within communities. Additionally, strengthening community and stakeholder involvement in the development of national and sub-national legislation, policies and plans enriches the policy-making process, and contributes to ensuring government and non-government initiatives benefit, and do not inadvertently obstruct communities from achieving healthy lifestyle choices (see KSA 1).
KSA 4: Build and develop personal life skills for individuals. A key aspect to enabling and supporting communities to identify and address their health and social needs is to facilitate suitable learning and personal development throughout their life cycle. While this learning undoubtedly requires a focus on public health and disease prevention issues, the development of personal life skills which empower communities to enact healthy behaviour change may require a much broader focus.
20
For example, the long-term health benefits for communities as a result of improved and equitable literacy amongst females and males are well established. Likewise, the ability for a community to access and manage donor-supported activities such as the construction of safe water supply systems may be dependant on community members having basic proposal/report-writing and book-keeping skills. These examples demonstrate how non-health specific learning and life-skills development can impact positively on factors which in turn assist communities to enact healthy choices. Building and developing personal life skills requires a multi-faceted approach depending on the audience, and the context. While school students may be receptive to classroom-style delivery of health promoting messages, this is rarely a suitable way of transferring new information to adults, especially if literacy is poor. Similarly, building practical, hands-on skills which will be utilised by community members to enact healthy improvements to their communities requires a much different approach which combines learning with an opportunity to implement that learning immediately. This concept, known as “learning-by-doing”, is a proven, effective method for facilitating long-term retention of information and skills amongst adults2324. Successful “learning-by-doing” can only be achieved through flexible approaches to skills transfer, which take into account the learning capacities of the target audience. For instance, delivering training on developing and managing a sustainable vegetable garden to young village women with poor literacy will utilise a different approach than for a target audience of educated, female primary school teachers who may be looking to develop school vegetable gardens with students. The young village women may require more verbal, hands-on teaching, delivered over a longer period than the school teachers, for whom some of the teaching material may be delivered in writing. Trainers using the “learning-by-doing” approach to build and develop personal life skills need to be flexible; delivering messages in a variety of ways which suit the specific learning requirements of the target audience. This requires trainers to have a suitable understanding of their audience’s strengths and capacities which may facilitate learning, as well as of the barriers and limitations which may inhibit them from being able to grasp concepts or practice the skills being taught. It should be understood that these barriers and limitations, as well as relating to the individuals’ capacities, may be environmental and/or cultural, such as the training being held in a venue that is not accessible for people with disabilities, or it being held too far
23 Baker, E., M. Metzler, et al. (2005). "Addressing Social Determinants of Health Inequities: Learning From Doing." American Journal of Public Health 95(4): 553-5. 24 Ungchusak K, Kanato M, et al. (1998). "Learning by doing: a motivation for public health workers in a Thai-German cooperation project." International Conference on AIDS 12: 951.

21
away from the village for men to allow their wives time away from household duties to attend. Flexibility ensures trainers have a variety of methods through which to transfer information and skills to different audiences, and allows them to adapt their delivery if one method is proving unsuccessful. Understanding the learning capacities and limitations of a target audience is a skill which is developed over time, through training experience and ongoing interaction with communities. In addition to building and developing personal life skills for individuals, the participatory nature of the “learning-by-doing” approach can strengthen the skills of trainers, by exposing them to the differing training needs of communities and individuals, and so assist them to develop a broad repertoire of effective training techniques. The interaction between communities and supportive technical agencies during “learning-by-doing”, and indeed through the activity identification, planning and implementation stages of health promotion offers important opportunities for learning exchange. This exchange benefits the health promotion process in three key ways;
i. It assists communities to receive new knowledge and skills in technical areas of public health (such as village water supply and sanitation systems, or reduction of mosquito breeding reservoirs).
ii. It assists the skills development of technical trainers to deliver learning-by-doing activities according to community requirements.
iii. It assists the development and delivery of more effective, community-driven health promotion activities.
Building and developing personal life skills is an essential step towards empowering communities and individuals to control their health and social determinants. Careful consideration must be devoted to the development of information and skill transfer techniques which yield the greatest, long-term benefit for Samoa’s communities.
KSA 5: Continue to strengthen reorientation of health services. The development of this National Health Promotion Policy stands as a testament to the commitment of the Ministry of Health to move from a purely clinical, curative model of health service delivery, to the provision of health promotion and disease prevention activities. Many gains in the provision of health promotion services have been made to date, however further efforts to reduce preventable disease are essential to ensure the Ministry has sufficient resources to meet the clinical need which will inevitably arise for the treatment of non-preventable diseases.

22
Put simply, the Ministry cannot afford to continue to spend resources on the treatment of preventable diseases at the current rate. An investment in promoting healthy lifestyles (and therefore preventing the onset of many health conditions) is essential for reducing the growing burden on the health sector. This investment will need to be redirected from the resources currently devoted to clinical and curative services, however in the long-term, it is expected that the promotion of health will reduce the number of people presenting to clinics and hospitals for curative treatment. Investment in health promotion goes beyond the supporting of community-identified projects and activities, and efforts to build and develop personal life skills for individuals in communities. For health promotion activities to be effective both in the short and long term, the Ministry of Health must view the implementation of health promotion programmes as an essential technical discipline, and as with all such disciplines, must invest in the ongoing professional development of the practitioners of health promotion. Professional, technical training which contributes to a qualified, technical workforce will facilitate systematic, effective roll-out of health promotion activities across the country. Furthermore, professionally qualified personnel who contribute to the implementation of locally-driven, applied research will help to ensure health promotion activities are planned and implemented based on evidence of what works in the Samoan context, which in turn ensures that investment in health promotion is directed to initiatives with the greatest, proven opportunity for success. Given that health promotion is a multi-sectoral discipline which encompasses health, social, political, economic and environmental components, investment in the development of a professional, technically qualified health promotion workforce will ultimately need to be a joint one, encompassing a range of government ministries, and potentially a whole-of-government approach.

23
IMPLEMENTING THE NATIONAL HEALTH PROMOTION POLICY The National Health Promotion Policy has been developed to guide all agencies, organisations and groups in Samoa who are involved in the delivery of health promotion activities to engage in empowering partnerships which enable and support individuals and communities to have control over their health and well being. The Key Strategic Areas through which to achieve community participatory health promotion demonstrate the multi-faceted interventions required to achieve effective, lasting improvements to the health and well being of communities. The following discussion outlines the roles and responsibilities of various groups and agencies in implementing the National Health Promotion Policy. Individuals and communities: Foremost amongst stakeholders of this Policy are the individuals and communities of Samoa, who not only stand to benefit from its effective implementation, but who are also its guiding informants and implementers. From the development of this guiding, National Health Promotion Policy, to the strengthening and building of healthy public policies, strategies and plans (KSA 1) within a range of government ministries and non-government organisations, the involvement of individuals and communities is essential to ensuring such guiding documents and policies a) support, and do not inadvertently create barriers to achieving healthy lifestyles (KSA 2), and b) deliver benefits to communities in culturally appropriate ways. Encouraging and supporting communities to work together in pursuit of healthy lifestyle changes (KSA 3) is the essential element through which to ensure interventions meet actual health and social needs, and that these are conducted in accordance with cultural customs and practices. The participatory process also requires communities to be prepared to identify and request technical assistance from outside agencies (be they government or non-government), and to be open to both receiving and contributing to development of life skills (KSA 4). Ministry of Health: In accordance with its mandate under the Ministry of Health Act 2006, the Ministry is the overall agency responsible for facilitating the adoption and implementation of this National Health Promotion Policy. It is therefore the Ministry’s responsibility to ensure community engagement and participation (KSA 3) in every stage of the Policy’s implementation, including the strengthening and building of healthy public policies (KSA 1), the creation of supportive and enabling environments (KSA 2), and contributing to, and participating in the building and development of personal life skills (KSA 4).

24
The Ministry of Health is also responsible for coordinating and facilitating appropriate multi-sectoral government and non-government participation in the strengthening and building of healthy public policies (KSA 1), the creation of supportive and enabling environments (KSA 2), and contributing to, and participating in the building and development of personal life skills (KSA 4). The continued strengthening of health services reorientation (KSA 5) is predominantly the domain of the Ministry of Health, however this too, should be done in accordance with the identified health and social needs of Samoa’s communities. The Ministry of Health is also responsible for periodically reviewing and amending the National Health Promotion Policy in accordance with its schedule for policy review, or as required by a dynamic health sector. Other Government Ministries: Under the coordination of the Ministry of Health, other government ministries responsible for activities or decisions which either directly or indirectly, positively or negatively influence the determinants of health affecting individuals and communities, have a responsibility to engage in the relevant processes identified in this Policy. In particular, government ministries should be encouraged to contribute to the strengthening and building of healthy public policies (KSA 1), the creation of supportive and enabling environments (KSA 2), and the building and development of personal life skills (KSA 4). Non-government sector: As with government ministries, the non-government sector, comprising both secular and faith-based organisations, have a responsibility to engage in the processes identified in this Policy, particularly if they conduct activities which directly or indirectly, positively or negatively influence the determinants of health affecting individuals and communities. The non-government sector has a key role to play in contributing to the creation of supportive and enabling environments (KSA 2), and in the building and development of personal life skills (KSA 4). It is also recognised that this sector’s close links with community organisations and practices makes it ideal for strengthening and supporting community mobilisation and action (KSA 3), and as some organisations within the sector also provide limited health services, they also have a role to play in strengthening reorientation of health services (KSA 5). Private sector: This sector, comprising marketing, media and communications organisations and private health service providers has a crucial role to play in implementing many aspects of the National Health Promotion Policy. Marketing and media organisations are well positioned to support the Ministry of Health to communicate effective, targeted messages and information which can be essential for contributing to the creation of enabling and supportive environments (KSA
25
2), and in developing resources and strategies for the building and development of personal life skills (KSA 4). Appropriate, targeted communication campaigns can contribute to the nation-wide dissemination of healthy public policies (KSA 1), and can both be strengthened by, and help to promote strengthened community action (KSA 3). Private health service providers are becoming an increasingly important component of the Samoa health sector, and are a crucial element of the Ministry of Health’s commitment to ensuring basic health care is available to all Samoans. The private health sector has considerable experience to offer, and should be engaged in processes for strengthening and building healthy public policies (KSA 1). It is also likely to play a major role in supporting the Ministry of Health’s continued reorientation of health services (KSA 5). Donors and regional technical organisations: Resource acquisition and technical assistance to build health sector capacity are essential elements to ensuring the effective implementation of the National Health Promotion Policy. Long-term improvement in the health of Samoa’s citizens will need to be met with assistance from the international donor community, and from regional technical agencies such as WHO-WPRO and the Secretariat for the Pacific Community (SPC). Existing and potential donors to Samoa’s health sector should be encouraged to engage in the processes of the National Health Promotion Policy, from its development through to its implementation, so as to ensure they are sensitised to the community-driven nature of the Policy’s processes, and therefore ready to both support community action (KSA 3) and direct resources to activities that are identified by communities themselves (rather than activities which are driven by their own agendas). Donors and technical agencies have key roles to play in supporting the strengthening of healthy public policies (KSA 1) across a range of sectors, and in contributing to the creation of supportive and enabling environments (KSA 2). Technical agencies have demonstrated experience in building health sector and community capacity, both professionally (KSA 5) and in terms of life skills development (KSA 4). The potential opportunity for donors to support these initiatives, and the strengthening of health service reorientation (KSA 5), should not be ignored.

26
Stakeholders
KSA
1: S
tren
gthe
n an
d bu
ild
heal
thy
publ
ic p
olic
ies
KSA
2: C
reat
e en
ablin
g an
d su
ppor
tive
env
iron
men
ts
KSA
3: S
tren
gthe
n co
mm
unit
y ac
tion
KSA
4: B
uild
and
dev
elop
pe
rson
al li
fe s
kills
for
indi
vidu
als
KSA
5: C
onti
nue
to
stre
ngth
en r
eori
enta
tion
of
heal
th s
ervi
ces
Individuals and communities Ministry of Health Other government ministries Non-government sector Private sector: general Private sector: health service providers Donors Regional technical organisations Table 1: Summary of stakeholder participation in the Key Strategic Areas of the National Health
Promotion Policy.

27
National Health Promotion Strategic Plan of Action In developing and implementing this National Health Promotion Policy, the Ministry of Health is taking a bold step towards more responsible health sector planning by endeavouring to offset a portion of health care costs towards health promotion activities in an effort to improve the health of all Samoans, and to reduce the long term health care costs of treating preventable diseases. The Ministry of Health is committed to ensuring the resources it allocates to health promotion activities are done so based on actual evidence that they are effective in achieving healthier outcomes for Samoa’s communities. This evidence will be built through the careful development and implementation of key strategic areas prior to, and at appropriate intervals throughout the programme. The strategic plan of action identifies measurable indicators both for programme outputs (short term objectives), as well as for programme outcomes; so that the Ministry of Health will be able to implement and monitor the success of the policy initiatives for improving community health and well being (long term objective). Activity costing has also been identified in effort to effectively budget for policy implementation.

33
National Health Promotion Strategic Plan of Action 2010-2015
Phase Indicator Data Source Responsible stakeholders Comments Costing Sources of Funds
KSA 1: Strengthen and build healthy public policies
Prep
arat
ion
Ministries and other stakeholders identified and invited to participate.
Definitive list developed.
MOH (lead). Identified Ministries and other stakeholders.
Where identified in this Table, the term “community stakeholders” refers to comprehensive inclusion of various groups, including those most marginalised. Programme implementers must commit to facilitating meaningful participation of all genders (including fa’afafines), people living with HIV and AIDS, people with disabilities, sex workers, young people, the elderly, and those living in rural and remote areas.
$5000 per year (over 5 years policy timeframe)
MOH, Donor
Partners Ministries and other identified stakeholders sensitised to Policy’s health promotion approach.
Actions to communicate approach conducted. Evaluation conducted to ensure the approach is understood. Commitment to participate confirmed.
MOH (lead). Identified Ministries and other stakeholders.
Criteria and processes developed for reviewing and assessing health and social impact of public policies.
Criteria developed. Process developed and documented. Pre-test activities conducted (with 2 existing MOH policies).
MOH (lead). Committed participant agencies. Community stakeholders.
Existing and forthcoming public policies identified for review.
List of public policies identified and prioritised and scheduled for review and alteration.
As above.

29
Phase Indicator Data Source Responsible stakeholders Comments Costing Sources of Funds
Impl
emen
t’n
Review and alteration of public policies.
Progress according to review schedule. Regular, ongoing review of altered policies for health impact (2-yearly?)
As above.
KSA 2: Create enabling and supportive environments
Prep
’n Identification of barriers
to improving health and well-being at different levels.
Barriers identified and documented at different levels.
MOH (lead). Committed participant agencies. Community stakeholders.
Nil
Imp’
n
Plan of Action for addressing identified barriers at different levels.
Plan of Action developed; incl. agreed schedules and responsibilities. Ongoing monitoring as per schedule.
As above.
Nil
KSA 3: Strengthen community action
Impl
emen
tati
on
Sensitisation of communities to Policy’s participatory approach.
Community awareness campaign to promote the Policy’s approach; media, community discussions etc.
MOH (lead). Committed participant agencies. Community Leaders.
$15,000 per year (for 5
year period of policy
document)
MOH & Donor & Sector
Partners

30
Phase Indicator Data Source Responsible stakeholders Comments Costing Sources of Funds
Development of a community participatory assessment tool to identify issues impacting on health and well-being.
Health and well-being assessment tool developed and pre-tested through community participatory processes.
MOH; technical sections. Committed participant agencies. Community stakeholders.
Nil
Community and stakeholder representatives trained in conducting community assessments using the developed tool.
Representatives trained. Number of completed assessments submitted.
As above. Agreed system for submission of assessments to coordinating body required.
$3000 per year (for 5
year period of policy
document)
MOH, Donor & Sector
Partners
Community assessments conducted; health and social needs identified and prioritised; plans of action developed.
Technical assistance (MOH and others) to review identified community assessments. Plans of action submitted. Periodic progress reviewed as per schedule.
As above.
Nil
MOH, Donor & Sector
Partners
Prep
’n
Resources provided to facilitate community action plans (as required).
Processes for grants developed and documented.
MOH; Health Sector SWAp. Donors. Committed participant agencies.
$5000 per year (for 5
year period of policy
document)
MoH & Donor
Partners
31
Phase Indicator Data Source Responsible stakeholders Comments Costing Sources of Funds
Number of applications received. Acquittal of grants as per agreed terms.
MOH (lead); technical sections. Community stakeholders.
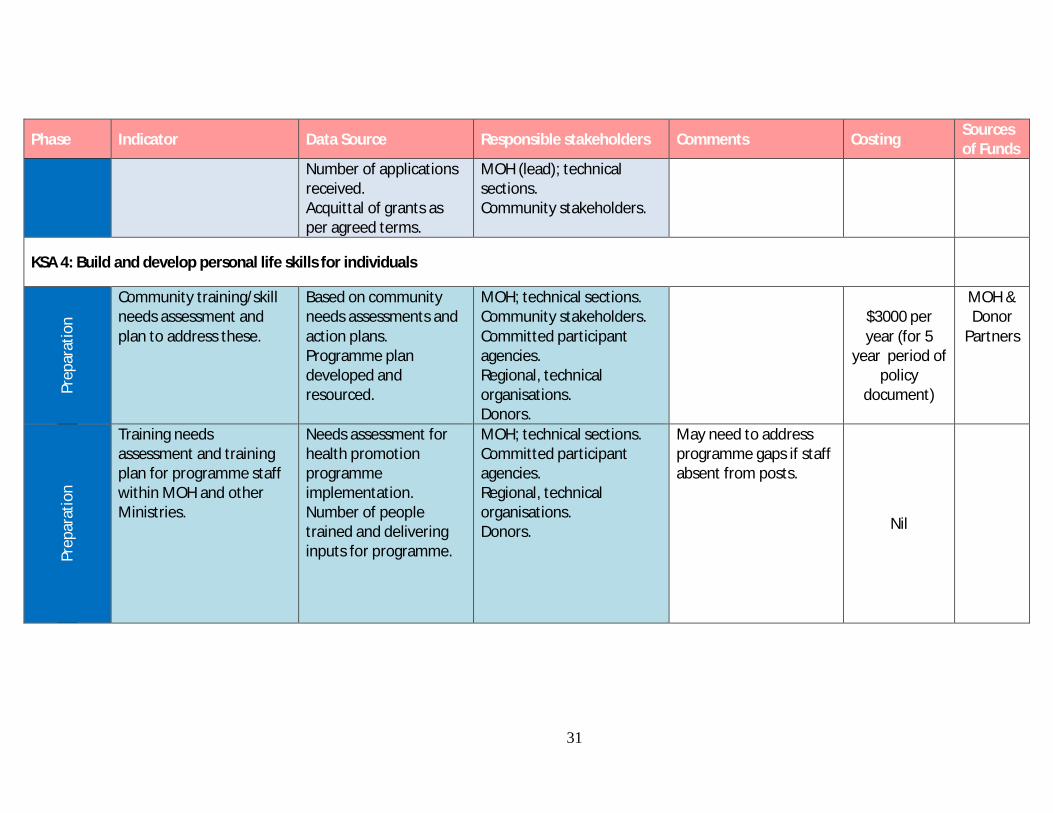
KSA 4: Build and develop personal life skills for individuals
Prep
arat
ion
Community training/skill needs assessment and plan to address these.
Based on community needs assessments and action plans. Programme plan developed and resourced.
MOH; technical sections. Community stakeholders. Committed participant agencies. Regional, technical organisations. Donors.
$3000 per year (for 5
year period of policy
document)
MOH & Donor
Partners
Prep
arat
ion
Training needs assessment and training plan for programme staff within MOH and other Ministries.
Needs assessment for health promotion programme implementation. Number of people trained and delivering inputs for programme.
MOH; technical sections. Committed participant agencies. Regional, technical organisations. Donors.
May need to address programme gaps if staff absent from posts.
Nil

32
Phase Indicator Data Source Responsible stakeholders Comments Costing Sources of Funds
Impl
emen
tatio
n
Community training/skills transfer activities conducted.
Number of people provided with skills development and building. Evaluation of training, immediately post, and after identified follow-up period.
MOH; technical sections. Community stakeholders. Committed participant agencies. Regional, technical organisations. Donors.
$3000 per year (for 5
year period of policy
document)
MOH & Donor
Partners
KSA 5: Continue to strengthen reorientation of health services
Prep
’n Identified targets for
resource allocation to health promotion activities.
Financial allocation of overall health sector expenditure to health promotion.
MOH. Ministry of Finance. Public Service Commission.
Could be a percentage of health sector expenditure, increasing annually.
Nil
Impl
emen
tat’
n
Technical training needs assessment for health promotion programme personnel within MOH and other Ministries.
Number of programme personnel receiving professional development training. Number of programme personnel receiving higher professional qualifications.
MOH; technical sections. Committed participant agencies. Regional, technical organisations. Donors.
May need to address programme gaps if staff absent from posts.
Nil
33
Phase Indicator Data Source Responsible stakeholders Comments Costing Sources of Funds
Research plan developed and implemented to inform programme monitoring.
Research needs identified and prioritised, and research schedule developed. Number of professionally-qualified personnel conducting applied research.
As above.
Nil

33
REFERENCES AusAID. (2010). "The Millennium Development Goals: the fight against global poverty
and inequality." Retrieved 6th May, 2010, from http://www.ausaid.gov.au/keyaid/mdg.cfm
Baker, E., M. Metzler, et al. (2005). "Addressing Social Determinants of Health Inequities: Learning From Doing." American Journal of Public Health 95(4): 553-5.
Galea, G., B. Powis, et al. (2000). "Healthy Islands in the Western Pacific: international settings development." Health Promotion International 15(2): 169-78.
Government of Samoa, (2006). Ministry of Health Act 2006. 19. Samoa.
Samoa Ministry of Health (2008). Health Sector Plan, 2008-2018. Apia, Samoa Ministry of Health.
Samoa Ministry of Health (2008), National Health Accounts 2006/2007. Apia, Samoa Ministry of Health
UN-OHCHR. (2010). "Universal Declaration of Human Rights." Retrieved 6th May, 2010, from http://www.ohchr.org/en/udhr/pages/introduction.aspx.
Ungchusak K, Kanato M, et al. (1998). "Learning by doing: a motivation for public health workers in a Thai-German cooperation project." International Conference on AIDS 12: 951.
WHO-WPRO (2003). Tonga commitment to promote healthy lifestyles and supportive environment. Manila, WHO-WPRO.
WHO-WPRO (2005). Regional Framework for Health Promotion, 2002-2005. Manila, WHO-WPRO.
WHO-WPRO (2005). Samoa commitment: achieving healthy islands: conclusions and recommendations. Manila, WHO-WPRO.
WHO (1995a). New Horizons in Health. Manila, WHO Regional Office for the Western Pacific.
WHO (1995b). Yanuca Island Declaration. Manila, WHO regional Office for the Western Pacific.
WHO. (2010). "Ottawa Charter for Health Promotion, 1986." Retrieved 21st April, 2010, from http://www.who.int/healthpromotion/conferences/previous/ottawa/en/.
35
COMMUNITY SUMMARY25 The Samoa Ministry of Health is committed to supporting health promotion in order to contribute to “A Healthy Samoa”. Many of the major threats to the health of the people of Samoa (such as stroke, heart disease, diabetes, typhoid and dengue fever) are preventable through healthy lifestyle choices. This National Health Promotion Policy is not simply for the Ministry of Health alone. It belongs to all Samoans, and seeks to encourage and enable all Samoans to assume control over their health and well being. Health promotion is a process. Health promotion is the process of enabling people to increase control over, and to improve their health by focusing on the social, environmental and economic conditions which impact on health and well being. The process of health promotion works to encourage individuals and communities to choose healthier behaviours and make healthier choices throughout their lives. It does this through two main ways;
i. The mobilisation (bringing together) of communities to work together towards healthier lifestyles, and
ii. The influencing of social conditions and processes to create an environment which enables and supports communities and individuals to make healthy choices.
Community mobilisation: Individuals and communities have abilities and strengths which help them to address problems. They are in the best position to ensure that they do this in a suitable, culturally acceptable way. Health promotion works with individuals and communities to identify;
i. their own health and social needs, and
25 Under guidance and direction from the Ministry of Health, this National Health Promotion Policy has been designed and presented in a format which complements other national policies. The technical nature of health promotion requires the use of technical language to describe concepts and processes, and this has contributed to an appropriately detailed document with which to guide the Ministry of Health and other partner government ministries.
Central to the successful implementation of this Policy, however, are the communities of Samoa, for whom much of the language and detail within the document is unnecessary and potentially confusing. For this reason, this ‘Community Summary’ has been designed to promote awareness and understanding of the National Health Promotion Policy, and in particular, the community-participatory concepts outlined within. It is anticipated that this ‘Community Summary’ could be used as a tool to assist agents of health promotion to engage with communities and individuals in the development and implementation of effective, participatory health promotion.
36
ii. actions which help them to address these. As a process, health promotion mobilises communities to work together, using their strengths and cultural knowledge to address the factors which influence health and well being of themselves and their community. Creating enabling and supportive environments: Some of these factors are beyond the control of individuals and communities. Health promotion also seeks to influence the environment in which communities live, so that they are enabled and supported to make healthy choices. Policy Vision: All individuals and communities in Samoa are enabled and supported to lead healthier lives through having control over their health and well being, throughout their life-cycle. Policy Aim: To guide all agencies, organisations and groups in Samoa who are involved in the delivery of health promotion activities to engage in empowering partnerships which enable and support individuals and communities to have control over their health and well being. Health Promotion in Samoa. This health promotion approach is not new. It is based on concepts developed between 1986-95, and adapted for the Pacific in 1995. These concepts came to be known as Healthy Islands, and Samoa has implemented a number of activities which have succeeded in bringing communities together to identify and address their health and social needs;
• Aiga ma Nuu Manuia programme. • Healthy Markets (Fugalei and Savalalo). • Health Promoting Schools. • National Council of Churches Health Promotion Programme.
Under this Policy, the next step is to build on these successful examples of community mobilisation, and to create enabling environments that support communities to make healthy choices.
37
Key Strategic Areas (KSAs). Successful implementation of the National Health Promotion Policy will be guided by five (5) Key Strategic Areas (KSAs). Any agency involved in health promotion will do so according to the proven methods of this Policy. KSA 1: Strengthen and build healthy public policies: It is not just the Ministry of Health which influences the health and well being of Samoans. Any policy, plan, strategy, decision or activity, from a whole range of sectors (including transport, public works, trade, agriculture, communications and media, education, law enforcement) can either limit or expand opportunities for individuals and communities to make healthy choices. For communities and individuals to have input into decisions and actions which could affect their health, they must be invited to contribute to the processes of developing and implementing new, guiding policies and plans. This will ensure these;
a) reflect and address the identified health and social needs of communities, and b) lead to activities that are suitable for Samoa’s communities.
Successful implementation of the Policy relies on genuine partnership and commitment to the principles of ava fatafata (fa’a-Samoa); respect for others and respect for human rights. KSA 2: Create enabling and supportive environments: Health promotion recognises the abilities and strengths of individuals and communities to identify their own health and social needs, and to work together to address these. However, in the modern environment of local and international trade, media, technology and economics, factors exist which are beyond the control of individuals and communities, but which impact on their health and well being. Creating enabling environments which support individuals and communities to address their health and social needs requires action at every level (from the community, to the national government, to international organisations and donors) through the guiding principle of mutual respect; for individuals, for communities, for the environment, for property and for human rights. KSA 3: Strengthen community action: The effectiveness of health promotion lies in its ability to empower individuals and communities to work together and to use their collective strengths and resources to make healthy lifestyle choices. The process of communities coming together is as essential to the long-term achievement of health and well being as the implementation of any activities which may arise from the process. KSA 4: Build and develop personal life skills for individuals: Enabling and supporting communities to address their health and social needs requires ongoing learning and personal development.
38
A concept known as “learning-by-doing” is an effective, practical, instructional method for building life skills amongst adults. It is delivered in a flexible way which enables effective communication and learning amongst different target groups, and it allows trainers to learn from the collective skills and knowledge of the communities which participate in the training. KSA 5: Continue to strengthen reorientation of health services: This National Health Promotion Policy aims to alter health sector funding so that a proportion of funds currently being spent almost entirely on treatment and clinical services is directed to promoting healthy lifestyles (and therefore preventing many health conditions). In the long term, it is expected that the promotion of health will reduce the number of people presenting to clinics and hospitals for treatment. The success of this approach relies on the Ministry of Health investing in necessary resources and the ongoing development and of its health promotion workforce. Implementing, monitoring and evaluating health promotion. The Ministry of Health must ensure that the resources it allocates to health promotion are effective in achieving healthier outcomes for Samoa’s communities. Consultation with communities and other stakeholders to develop effective monitoring and evaluation processes prior to commencing health promotion activities is essential to building the evidence required to demonstrate effectiveness. Likewise, plans of action for the Policy’s implementation shall be developed through consultation with stakeholders at both the programme coordination and community levels. This will ensure the plans address actual health and social needs of Samoa’s communities.


![Alliance for Alcohol policy movements€¦ · Health Promotion Policy Research Center, International Health Policy Program (IHPP) Ministry of Public Health ]thaksaphon@ihpp.thaigov.net](https://static.documents.pub/doc/80x56/5f0701cc7e708231d41ad4e4/alliance-for-alcohol-policy-movements-health-promotion-policy-research-center-international.jpg)














