3
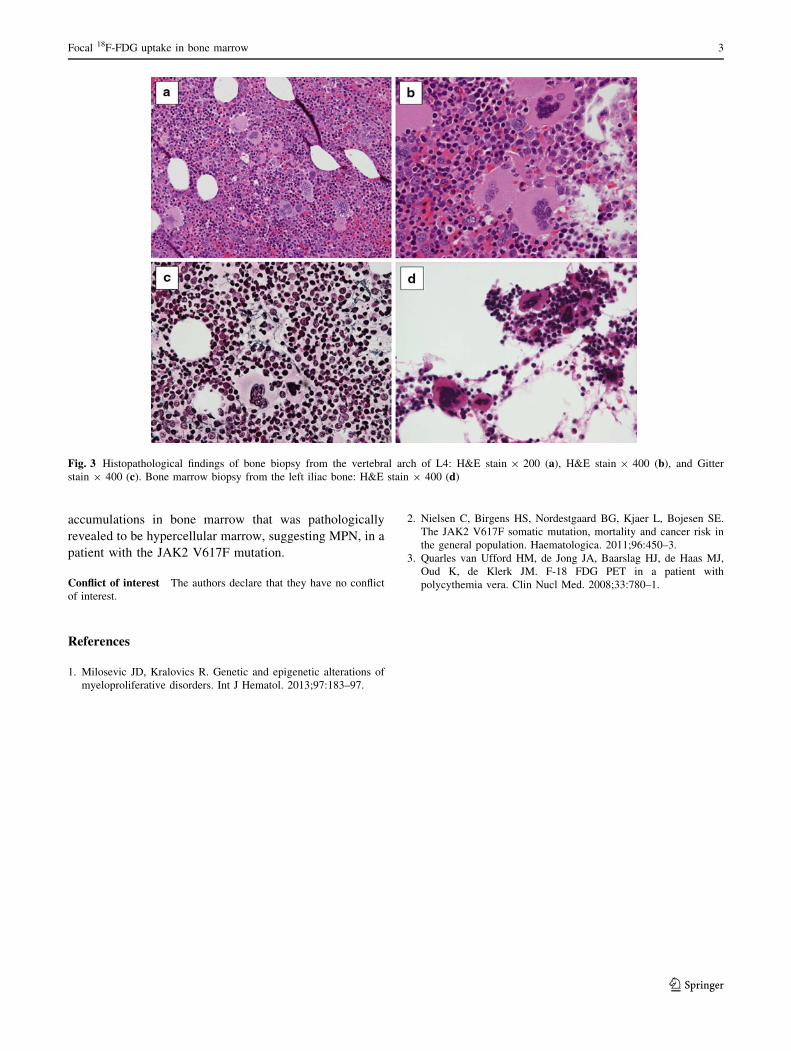
IMAGES IN HEMATOLOGY Focal 18 F-FDG uptake in bone marrow on PET/CT in a patient with JAK2 mutation without overt myeloproliferative neoplasm Akihito Fujimi • Yuji Kanisawa • Shinya Minami • Yusuke Kamihara • Sari Iwasaki Received: 5 September 2013 / Revised: 12 November 2013 / Accepted: 13 November 2013 / Published online: 26 November 2013 Ó The Japanese Society of Hematology 2013 A 58-year-old female diagnosed with early stage esopha- geal carcinoma in our hospital underwent endoscopic resection by endoscopic submucosal dissection (ESD) in April 2013. 18 F-FDG PET/CT performed immediately prior to the ESD showed focal 18 F-FDG accumulations in the vertebral body of Th8, and vertebral body and arch of L4 with SUV max of 3.98–4.42 (Fig. 1a–c). No masses or osteoclastic lesions were observed. MRI findings of the lesions showed low intensity on T1WI and high intensity on STIR image (Fig. 2a–d). To clarify the cause of the 18 F- FDG accumulation in the bone, we performed bone biopsy from the vertebral arch of L4. Histopathological findings revealed hypercellular marrow (80 % cellularity) and increases in number and size of megakaryocytes, most of which were in maturated form with hyperlobulated nuclei, which are usually found in cases with myeloproliferative neoplasm (MPN) (Fig. 3a, b). Reticulin fibrosis of marrow was observed minimally by Gitter staining (Fig. 3c), and collagen fibrosis was not observed. In contrast, laboratory workup for peripheral blood showed no abnormality: WBC 6,920/lL (stab 0.0 %, seg 61.0 %, lymph 30.0 %, mono 6.0 %, eosino 1.5 %, and baso 1.5 %), RBC 452 9 10 4 / lL, Hb 14.1 g/dL, Ht 40.6 %, PLT 33.3 9 10 4 /lL, reti- culocytes 1.2 %, LDH 229 U/L, VB12 351 mg/dL, and NAP score 223. Bone marrow biopsy subsequently per- formed from the left iliac bone showed normocellular marrow, but the number of megakaryocytes was also increased (Fig. 3d). Furthermore, JAK2 V617F mutation was detected in the bone marrow sample by real-time qualitative PCR with a sensitivity of more than 2 % of all alleles. G-banding showed normal diploid karyotype, and BCR–ABL translocation was not detected by FISH ana- lysis. 5 months after the first visit, her laboratory data of peripheral blood was within the normal range, and 18 F- FDG PET/CT also showed similar 18 F-FDG accumulation in the bone, without new lesions. We will continue to follow her progress carefully. The JAK2 V617F mutation is present in patients with Philadelphia-negative MPN, including over 90 % of poly- cythemia vera cases and about half of essential thrombo- cythemia and primary myelofibrosis cases [1]. The JAK2 V617F mutation may also be detected in healthy individ- uals without overt MPN [2]. Nielsen et al. [2] reported that the JAK2 V617F mutation was detected in 18 of 10,507 participants (0.2 %) in the general population, and three of these 18 individuals with the JAK2 V617F mutation developed overt myeloproliferative disorder during up to 17.6 years of follow-up. In the present case, focal 18 F-FDG accumulation in bone marrow and histopathological find- ings, other than the finding of the left iliac bone marrow as positive for JAK2 V617F mutation, suggest that the patient is more likely to develop some form of overt MPN in the A. Fujimi (&) Á Y. Kanisawa Department of Hematology and Oncology, Oji General Hospital, 3-4-8 Wakakusa-cho, Tomakomai 053-8506, Japan e-mail: [email protected] S. Minami Department of Gastroenterology, Oji General Hospital, Tomakomai, Japan Y. Kamihara Department of Medical Oncology and Hematology, Sapporo Medical University, Sapporo, Japan S. Iwasaki Department of Pathology, Hokkaido University Graduate School of Medicine, Sapporo, Japan 123 Int J Hematol (2014) 99:1–3 DOI 10.1007/s12185-013-1473-y













![QUANTIFICATION OF DYNAMIC [18F]FDG PET 10.1007/s11307...QUANTIFICATION OF DYNAMIC [18F]FDG PET STUDIES IN ACUTE LUNG INJURY Journal: Molecular Imaging and Biology Elisabetta Grecchi1,6, Mattia Veronese2,6, Rosa Maria Moresco3, Giacomo Bellani4,5, Antonio Pesenti4 ...](https://static.documents.pub/doc/80x56/5aa9f1017f8b9a6c188d9646/quantification-of-dynamic-18ffdg-pet-101007s11307quantification-of-dynamic.jpg)





