Functional Imaging of the Pharynx Using ElectronBeam Tomography
Franz Lindbichler, MD,1 Johann Raith, MD,1 Martin Uggowitzer, MD,1 and Anita Wuttge-Hannig, MD21University Hospital Graz, Department of Radiology, Graz, Austria and2Privat Radiologist (AW-H), Mu¨nchen, Germany
Abstract. Due to long scan times it was impossible tomake dynamic swallowing imaging using computer to-mography (CT) of the third or fourth generation. Thisstudy evaluates whether electron beam tomography withscan times of 100 ms enables a more detailed dynamicimaging of swallowing disorders. Examination usingelectron beam tomography was done in three planes: (1)Passavant’s cushion (n4 6), (2) thyrohyoid membrane(n 4 9), and (3) upper esophageal sphincter (n4 5). Thetechnique is discussed here in detail and documentedwith figures of the plane before swallowing as well as theintradeglutitive reachend plane. This study shows thatelectron beam tomography enables dynamic imaging ofpharyngeal deglutition in transverse planes and can giveuseful additional information to the videofluorographicor kinematographic swallowing examination, which re-main the gold standard in the functional evaluation ofswallowing disorders.
Imaging of pharyngeal swallowing calls for a functional,dynamic image modality because phases which last lessthan 1 sec have to be documented [1]. Mono- anddouble-contrast pharyngography only allows a morpho-logic analysis of pharyngeal structures [2]. Today, vid-eofluorographic and kinematographic swallowing ex-aminations are the methods of choice for dynamic imag-ing of swallowing, but they also have disadvantages: (1)it is not possible to image swallowing in a third plane, the
transverse plane; and (2) lack of orientating anatomicstructures in the height of the mesopharynx and hypo-pharynx because of the rapid movement of hyoid boneand larynx intradeglutitively, with consecutive poor im-age quality of topographic interrelationships.
Because of long scan times it was impossible toperform dynamic swallowing examinations using CT ofthe third or fourth generation [3]. Electron beam tomo-graphy (EBT), with its technical possibilities [4] such asscan times of 100 ms was promising as a method fordynamic imaging of pharyngeal swallowing. This studyevaluates the ability of EBT in swallowing examinations,as well as its limits. Primarily it was not the aim to studythe pathology, but to show physiologic changes duringdeglutition. To the best of our knowledge, no similarstudy of functional imaging of the pharynx using CT hasbeen undertaken.
Immediately after the videofluorographic exami-nation of pharyngeal deglutition, EBT (Evolution, Ultra-fast CT, Siemens, Germany) was performed on selectedinformed volunteers. The scan technique was a single-slice cine mode with scan times of 100 ms (130 kV, 620mA) and a slice thickness of 3-mm or 6-mm, dependingon the size of the structure imaged. The patient was in asupine position and during swallowing of a 20 ml bolus,a sequence of 20 times per level was scanned. Thismeans that in one and the same level, 20 slices result in2,3 seconds (scan time 100-ms, interscan delay 16 ms).Because there is a difference between speed of the bolusduring deglutition and scanning, it is not possible to im-age the whole pharynx in the intradeglutitive phase ofswallowing. Besides you cannot see the beginning ofswallowing directly, as with videofluorography, CTscanning has to be started when the patient is asked toinitiate swallowing. For these reasons, one way to get tofunctional results using EBT is to image only one levelwith multiple scans (20 for example), in a short time,beginning with the verbal order for deglutition. The im-
Correspondence to:Franz Lindbichler, M.D., Auenbruggerplatz 9,8036 Graz, Austria
ages could be viewed either one by one or in a cinesequence. The latter shows the functional interrelation-ships of the different structures such as hyoid bone andlarynx, which are moving through the imaged plane in-tradeglutitively. The levels were always transversely par-allel to the hard palate. The study was done at threepharyngeal locations, at the height of the Passavant’scushion [5], just above the hyoid bone to focus on thehypopharynx, or at the location of the upper esophagealsphincter (UES). The exact position of the plane wasevaluated by the prior videofluorographic swallowingexamination and adapted on the preview scan.
Region of the Passavant’s Cushion
The plane chosen in these 6 patients was the hard palate(Fig. 1) and the bolus consisted of diluted iodinated con-trast agent (Jopamidol, 1:20). The aim of the study in thisheight was to image the mechanism of closure betweenthe soft palate and the Passavant’s cushion [5]. At restthe well-known structures of the meso-epipharyngealjunction could be clearly discerned [6].
During swallowing, the meso-epipharyngeal seg-
Fig. 1. Level for evaluation of the meso-epipharyngeal junction before swallowing. Hard palate (large star), dens axis (small star).Fig. 2. Closed meso-epipharyngeal junction by the soft palate (star) and Passavant’s cushion (arrows) during swallowing (same patient as inFig. 1).
Fig. 3. Initial level for examination of the thyrohyoid membrane. Epi-glottis (arrow).
102 F. Lindbichler et al.: EBT Imaging of the Pharynx
ment was completely and symmetrically closed by thesoft palate and the Passavant’s cushion (Fig. 2).
Thyrohyoid Membrane
The plane was placed referring to the craniocaudalmovement of the hyoid bone and larynx, evaluated priorto the videofluorographic swallowing examination, 1–2cm cranial to the hyoid bone (Fig. 3), so that the thyro-hyoid membrane was reached intradeglutitively. The bo-lus consisted of water, because in prior examinationsusing diluted contrast agent, marked artefacts (motionartefacts and shading or dishing artefacts) made diagno-sis impossible.
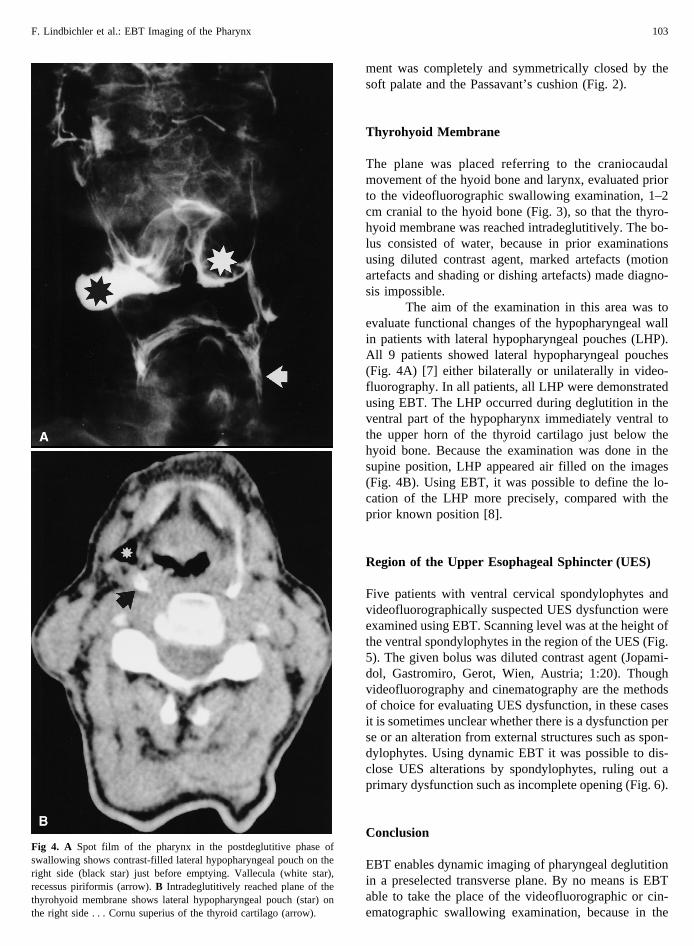
The aim of the examination in this area was toevaluate functional changes of the hypopharyngeal wallin patients with lateral hypopharyngeal pouches (LHP).All 9 patients showed lateral hypopharyngeal pouches(Fig. 4A) [7] either bilaterally or unilaterally in video-fluorography. In all patients, all LHP were demonstratedusing EBT. The LHP occurred during deglutition in theventral part of the hypopharynx immediately ventral tothe upper horn of the thyroid cartilago just below thehyoid bone. Because the examination was done in thesupine position, LHP appeared air filled on the images(Fig. 4B). Using EBT, it was possible to define the lo-cation of the LHP more precisely, compared with theprior known position [8].
Region of the Upper Esophageal Sphincter (UES)
Five patients with ventral cervical spondylophytes andvideofluorographically suspected UES dysfunction wereexamined using EBT. Scanning level was at the height ofthe ventral spondylophytes in the region of the UES (Fig.5). The given bolus was diluted contrast agent (Jopami-dol, Gastromiro, Gerot, Wien, Austria; 1:20). Thoughvideofluorography and cinematography are the methodsof choice for evaluating UES dysfunction, in these casesit is sometimes unclear whether there is a dysfunction perse or an alteration from external structures such as spon-dylophytes. Using dynamic EBT it was possible to dis-close UES alterations by spondylophytes, ruling out aprimary dysfunction such as incomplete opening (Fig. 6).
Conclusion
EBT enables dynamic imaging of pharyngeal deglutitionin a preselected transverse plane. By no means is EBTable to take the place of the videofluorographic or cin-ematographic swallowing examination, because in the
Fig 4. A Spot film of the pharynx in the postdeglutitive phase ofswallowing shows contrast-filled lateral hypopharyngeal pouch on theright side (black star) just before emptying. Vallecula (white star),recessus piriformis (arrow).B Intradeglutitively reached plane of thethyrohyoid membrane shows lateral hypopharyngeal pouch (star) onthe right side . . . Cornu superius of the thyroid cartilago (arrow).
F. Lindbichler et al.: EBT Imaging of the Pharynx 103
latter, all parts of the pharynx and esophagus can beexamined, whereas with EBT only the dynamic changesand the morphology of one level can be imaged. There-fore videofluorography and cinematography still remainthe methods of choice for the diagnosis of functionalswallowing disorders. However, EBT can add useful,additional information to equivocal or indistinct video-fluorographic findings in a specific part of the pharynx.
References
1. Neumann S: Physiologie des Schluckvorganges. In: BartolomeG, Bucholz-DW, Hannig C, et al (eds):Diagnostik und Therapieneurologisch bedingter Schlucksto¨rungen.Stuttgart, Jena, NewYork: Gustav Fischer, 1993
2. Hannig C:Radiologische Funktionsdiagnostik des Pharynx und
des Osophagus.Berlin, Heidelberg, New York, London, Paris,Tokyo, Hong Kong, Barcelona, Budapest: Springer-Verlag,1995
Fig. 5. Initial level for evaluation of the UES in the height of a ventral cervical spondylophyte (arrow).Fig. 6. Impression of the UES (white arrow) due to ventral cervical spondylophyte (black arrow).
104 F. Lindbichler et al.: EBT Imaging of the Pharynx