41
Gender differences in the NICU: the disadvantaged ‘Y’ Vedang A. Londhe, M.D. Assistant Professor of Pediatrics Division of Neonatology and Developmental Biology

Gender differences in the NICU: the disadvantaged ‘Y’
Vedang A. Londhe, M.D. Assistant Professor of Pediatrics
Division of Neonatology and Developmental Biology
Outline • Y chromosome
– Ontogeny – Implications in the newborn – Implications in NICU
• Prematurity/survival • Respiratory • Neurologic • Metabolic • Neuro-behavioral
• Review questions

“Over the course of time, the Y chromosome has degenerated and now contains only 50 genes compared to almost 3000 in the X chromosome. Therefore, the Y chromosome is highly repetitive and mostly non-functional (probably no surprise to half of the population without one).”
Ingemarsson, Gender aspects of preterm birth, BJOG: an International Journal of Obstetrics and Gynecology, April 2003, Vol 110 (Suppl 20), pp. 34-38
Outline • Y chromosome
– Ontogeny – Implications in the newborn – Implications in NICU
• Prematurity/survival • Respiratory • Neurologic • Metabolic • Neuro-behavioral
• Review questions

• Reduced by one third from original size and lost 97 % genes (~45/1438 remaining)
• High mutation rate due to highly oxidative sperm/testis environment
• SRY (Sex-determining Region Y) gene – Primary sex determination gene – ‘Testis determining factor’ – Found in all male mammals—130 million years old
Y chromosome



www.kcampbell.bio.umb.edu/November01/Sryproof.gif

• SRY transcribed as early as two-cell stage embryo
• Y chromosome results in accelerated early growth secondary to higher metabolic rate – Provides XY embryo with advantage for faster growth and
development – XY embryos have better chance to develop testes before
accumulation of estrogenic hormones
• Some researchers speculate that the Y chromosome might disappear completely in 100 million years—future male characteristics may only be special attribute found in women‡
‡Ingemarsson, Gender aspects of preterm birth, BJOG: an International Journal of Obstetrics and Gynecology, April 2003, Vol 110 (Suppl 20), pp. 34-38

Outline • Y chromosome
– Ontogeny – Implications in the newborn – Implications in NICU
• Prematurity/survival • Respiratory • Neurologic • Metabolic • Neuro-behavioral
• Review questions

Implications in the newborn
• Sex ratio: dependent variables? – Birth order? – Parental age? – Social class? – Paternal occupation? – Season of birth? – Calendar period of delivery?

Implications in the newborn
• Sex ratio: dependent variables? – Birth order? – Parental age? – Social class? – Paternal occupation? – Season of birth? – Calendar period of delivery?
• NO evidence that gender determination is anything other than a chance process†
– Sex ratio male vs female was 1.06 in population of 549,048 births
†Maconochie et al., Sex ratios: are there natural variations within the human population?, Br J Obtet Gynaecol 1997, 104: 1050-1053

• Cesarean delivery – Overall Cesarean rates
• 13.2% in women carrying male fetuses • 9.2% in women carrying female fetuses
– Male fetuses • Cesarean rate increased by 30% for FTP (vs. females) • Cesarean rate increased by 70% for fetal distress (vs. females) • When adjusted for GA and fetal size:
– Male fetal sex DID NOT continue to predict risk of Cesarean delivery for FTP
– Male fetal sex DID continue to predict risk of Cesarean delivery for fetal distress
– Emergency Cesarean rates • 8.3% in women carrying male fetuses • 7.1% in women carrying female fetuses • May be due to increased bradycardia in males during last hour of
labor as compared to females = different response to hypoxia?
Lieberman et al., The association of fetal sex with the rate of Cesarean section, Am J Obstet Gynecol 1997, 176:667-671

Outline • Y chromosome
– Ontogeny – Implications in the newborn – Implications in NICU
• Prematurity/survival • Respiratory • Neurologic • Metabolic • Neuro-behavioral
• Review questions

Implications in the NICU
• Prematurity
Ingemarsson, Gender aspects of preterm birth, BJOG: an International Journal of Obstetrics and Gynecology, April 2003, Vol 110 (Suppl 20), pp. 34-38

• Between 38-40 weeks GA, there was an excess of female newborns delivered
• From 41+ weeks there was again an excess of males
• ‘the guys are either too early or too late!’
• Gender + race – Review of > 1.9 million births, 7.2% excess of males among
white singleton preterm births compared to only 2.8% excess of comparable blacks*
* Mechanisms responsible for preterm birth rates in blacks are less dependent on fetal gender
Cooperstock et al., Excess males in preterm birth: interactions with gestational age, race, and multiple birth, Obstet Gynecol 1996;88:189-193
• Generally believed that fetuses are involved in labor and male fetuses may promote onset of preterm birth – One mechanism: action of androgen precursors involved
in estrogen production, increased in males – Second mechanism: induction of labor may be promoted
by IL-1, exacerbated by lower levels of IL-1 receptor antagonist in amniotic fluid of preterm males → preterm labor٭
• Greater incidence of male births between 24-32 weeks GA (55% vs. 45%)
• Neonatal mortality greater in males 24-32 weeks (9.1% vs. 5.6%) and even greater at 23-24 weeks (55% vs. 32%)
,Bry et al., Interleukin-1 receptor antagonist in the fetomaternal compartment٭Acta Paediatrica 1995;84:233-236
• Respiratory – Male excess in neonatal mortality most
prominent during first week of life – Mortality related to RDS is greatest in males with
relative risk of 1.57 – Mechanism may be due to slower lung
maturation in males leading to higher incidence of RDS in male infants‡ (fewer alveolar type II cells and less surfactant)
– Translates into a greater effect of betamethasone prophylaxis in female infants†
• Although GR numbers are equal, male androgens may reduce tissue levels of GR mRNA and protein → inhibitory effect
‡Khoury et al., Factors affecting the sex differential in neonatal mortality: the role of respiratory distress syndrome, Am J Obstet Gynecol 1985;151:777-782
†Weitzel et al., Clinical aspects of antenatal glucocorticoid treatment for prevention on fneonatal respiratory distress syndrome, J Perinat Med 1987;15:441-446

– Pulmonary function • Studies have shown greater incidence in males of
bronchopulmonary dysplasia and worse pulmonary function even after adjustment for birth weight
• Race also predicts pulmonary function with black females performing best and white males performing worst
Stocks et al., Influence of ethnicity and gender on airway function in preterm infants, AM J Respir Crit Care Med 1997;156:1855-1862

• Neurologic – Extremely premature (and ELBW) male infants
have a distinct disadvantage in outcomes for mortality, in-hospital morbidity, and neurodevelopment
– Both physical and mental developmental indices are worse in males than females <28 weeks GA
• Moderate-severe CP (10.7% vs. 7.3%) • Bayley (mental index) < 70 (41.9% vs. 27.1%) • Psychomotor index < 70 (48.1% vs. 34.1%)
– Male gender remains as an independent risk factor for adverse neurodevelopmental outcome even after multivariate analyses accounting for illness severity, etc.
Hintz et al., Gender differences in neurodevelopmental outcomes among extremely preterm, extremely-low-birth weight infants, for NICHD Neonatal Research Network, Acta Paediatrica 2006;95:1239-1248

– Mechanisms of neurologic injury? • 1980s: hypothesis that increased incidence of IVH due
to unstable cerebral blood flow and hemorrhage • Indomethacin introduced to ‘stabilize’ blood flow but
large RCT showed no benefit • Re-analysis of nearly 20-year old data showed
beneficial effect was gender specific (males) • Possibly due to innate gender differences in response
to brain injury – Male and female cells may have divergent cell death
pathways: deficiency in glutathione metabolism in male cells renders preterm oligodendrocytes more prone to death
• Indomethacin protective action may be via anti-inflammatory effect to prevent cell death, leading to improved outcomes in males
Edwards D., Brain protection for girls and boys,
J Pediatrics 2004;145:723-4

Are cool boys better than cool girls?
Stay tuned…
Head Whole body

• Metabolic – It has been suggested that the higher
metabolic rate in males may be sustained throughout life
• Analysis of cord blood glucose at term showed males had higher mean levels compared to females (3.87 vs. 3.71 mmol/L)
• No differences in blood glucose levels seen following planned Cesarean deliveries
• Speculation is that differences in arterial cord blood glucose levels may be due to gender differences in response to labor stress
– Females may be born lighter than boys due to greater insulin resistance٭ (?)
Ingemarsson, Gender aspects of preterm birth, BJOG: an International Journal of Obstetrics and Gynecology, April 2003, Vol 110 (Suppl 20), pp. 34-38
Wilkin et al., The gender insulin hypothesis: why girls are born ligher than boys, and the implications for insulin٭resistance, Internat J of Obesity 2006;30:1056-1061
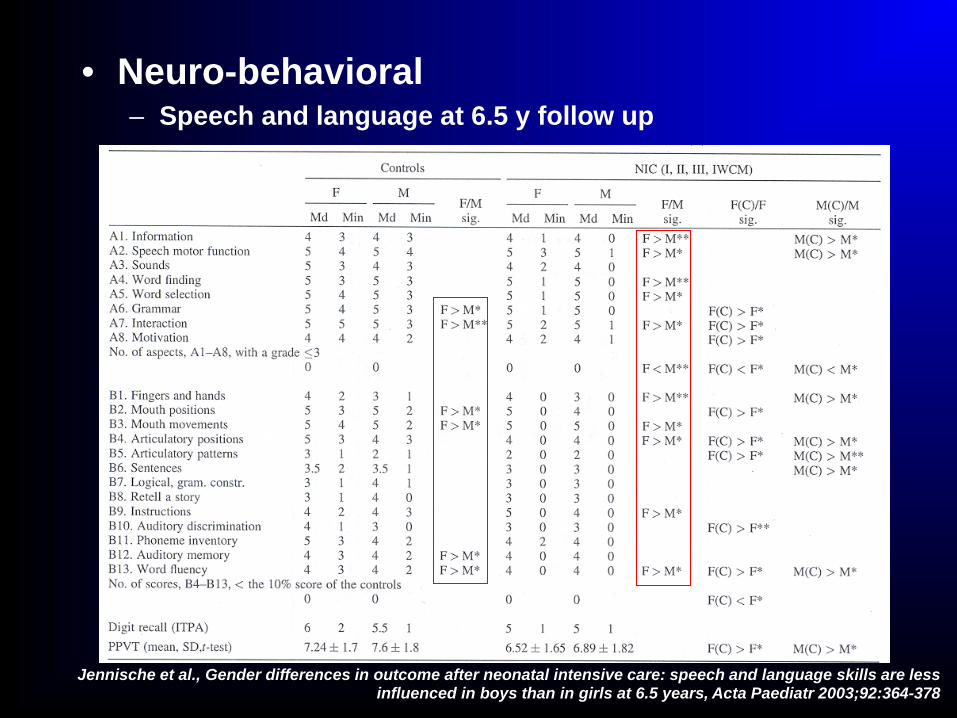
• Neuro-behavioral – Speech and language at 6.5 y follow up
Jennische et al., Gender differences in outcome after neonatal intensive care: speech and language skills are less influenced in boys than in girls at 6.5 years, Acta Paediatr 2003;92:364-378

– Joint attention: an aspect of early communication emerging at 9-12 mos emanating from face-face interaction and interest in objects
– At 1 y follow up, males were outperformed by females in all aspects of social communication even after correction for differences in birthweight
• It is suggested that females have an advantage in facial expression processing from infancy through adolescence
• It is likely that facial expression processing develops in concert with other non-verbal and early communicative skills
Olafsen et al., Joint attention in term and preterm infants at 12 months corrected age, Infant Behavior and Development 2006, 29:554-563

– Pain • Adult males generally believed to have
higher pain threshold and tolerance– based on PET studies of premotor cortex activation
• Male newborns of all gestational ages expressed less facial features of pain compared to females
Guinsburg et al., Differences in pain expression between male and female newborn infants, Pain 2000;85:127-133

– Hearing: ‘Huh? What?’ • Males are less advanced in peripheral
auditory development than females • The human cochlea is fully functional as a
mature sound transducer by 6 mo age • Studies have shown that spontaneous
otoacoustic emissions can be detected as early as 30 weeks GA
• Music stimulation (Brahms’ lullaby) significantly benefited premature females’ days to discharge
Morlet et al., Spontaneous otoacoustic emissions in preterm neonates: prevalence and gender effects, Hearing Research 1995;90:44-54
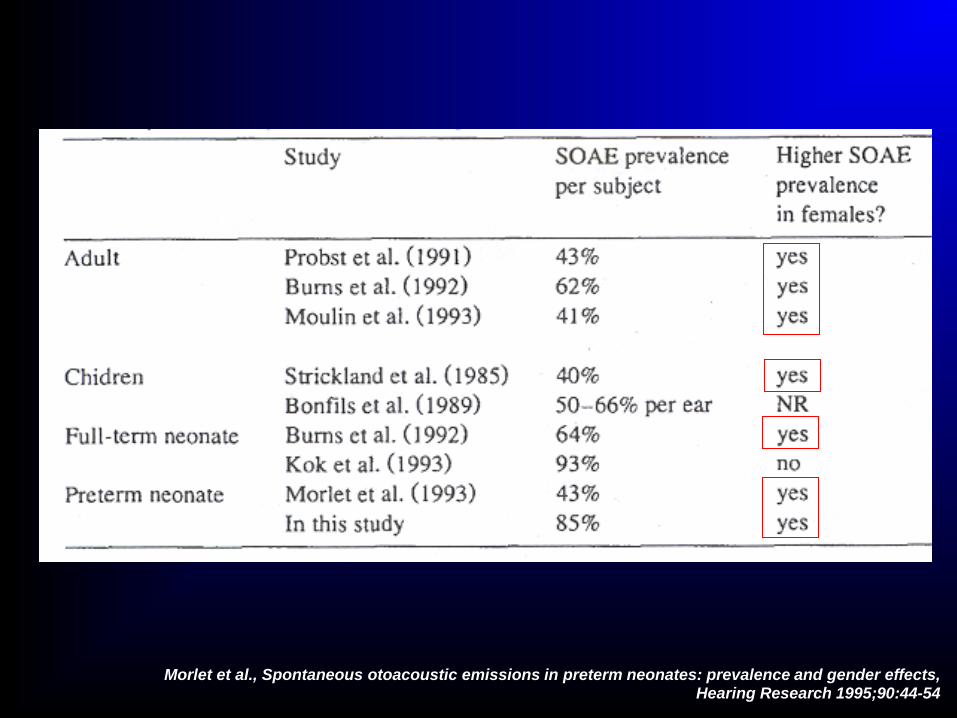
Morlet et al., Spontaneous otoacoustic emissions in preterm neonates: prevalence and gender effects, Hearing Research 1995;90:44-54

– Sleep • Sleep continuity and architecture are
gender related • One study showed preterm males (34 weeks
GA) slept less (~25 min/day) with more wakefulness and active sleep and less quiet sleep than females
Bach et al., Gender-related sleep differences in neonates in the thermoneutral and cool environments, J Sleep Res 2000;9:249-254
“Six hours for a man, seven hours for a woman, and eight for a fool.” --Napoleon Bonaparte

Review questions
1. Which of the following is necessary and sufficient to determine maleness in mammals?
a) Y chromosome b) p arm of Y chromosome c) SRY gene d) Bilateral descended testes

Answer
1. Which of the following is necessary and sufficient to determine maleness in mammals?
a) Y chromosome b) p arm of Y chromosome c) SRY gene d) Bilateral descended testes

Question
2. SRY gene expression is seen at its earliest in which of the following:
a) Sperm cell b) Ovum c) Two cell fertilized embryo d) Ovarian cortex

Answer
2. SRY gene expression is seen at its earliest in which of the following:
a) Sperm cell b) Ovum c) Two cell fertilized embryo d) Ovarian cortex

Question
3. Which of the following scenarios describes an advantage of the Y chromosome?
a) Faster growth of early embryo b) Slower metabolism of early embryo c) Increased facial expression of pain d) There are no advantages of the Y

Answer
3. Which of the following scenarios describes an advantage of the Y chromosome?
a) Faster growth of early embryo b) Slower metabolism of early embryo c) Increased facial expression of pain d) There are no advantages of the Y
Question
4. For which of the following conditions is a male fetus NOT at greater risk for delivery via Cesarean?
a) Fetal distress b) Failure to progress c) Bradycardia d) Hypoxia

Answer
4. For which of the following conditions is a male fetus NOT at greater risk for delivery via Cesarean?
a) Fetal distress b) Failure to progress c) Bradycardia d) Hypoxia

Question
5. Which of the following is TRUE regarding survival at 23-24 weeks GA?
a) Less than ½ of females survive b) Less than ½ of males survive c) Females do not develop BPD d) Females have higher incidence of RDS

Answer
5. Which of the following is TRUE regarding survival at 23-24 weeks GA?
a) Less than ½ of females survive b) Less than ½ of males survive c) Females do not develop BPD d) Females have higher incidence of RDS


THANK YOU!






![NICU Database Appendices - CPQCC NICU Appendices.pdf2020 NICU Appendices| 4 1101 [K. oxytoca, K. pneumoniae and others] including Carbapenem-resistant Klebsiella and Cephalosporin-resistant](https://static.documents.pub/doc/80x56/5f0e96fb7e708231d43ff847/nicu-database-appendices-cpqcc-nicu-2020-nicu-appendices-4-1101-k-oxytoca.jpg)










