Global Vision and Future on Health Economics for Regenerative Medicine: Perspective from Europe Bengt Jönsson Professor emeritus Stockholm School of Economics Vice chair, Expert Panel on Effective Ways of Investing in Health, European Commission
Transcript
Global Vision and Future on Health Economics for Regenerative Medicine: Perspective from EuropeBengt JönssonProfessor emeritus Stockholm School of EconomicsVice chair, Expert Panel on Effective Ways of Investing in Health, European Commission
The European Union: 500 million people – 28 countries
Member states of the European Union
Candidate and potential candidate countries
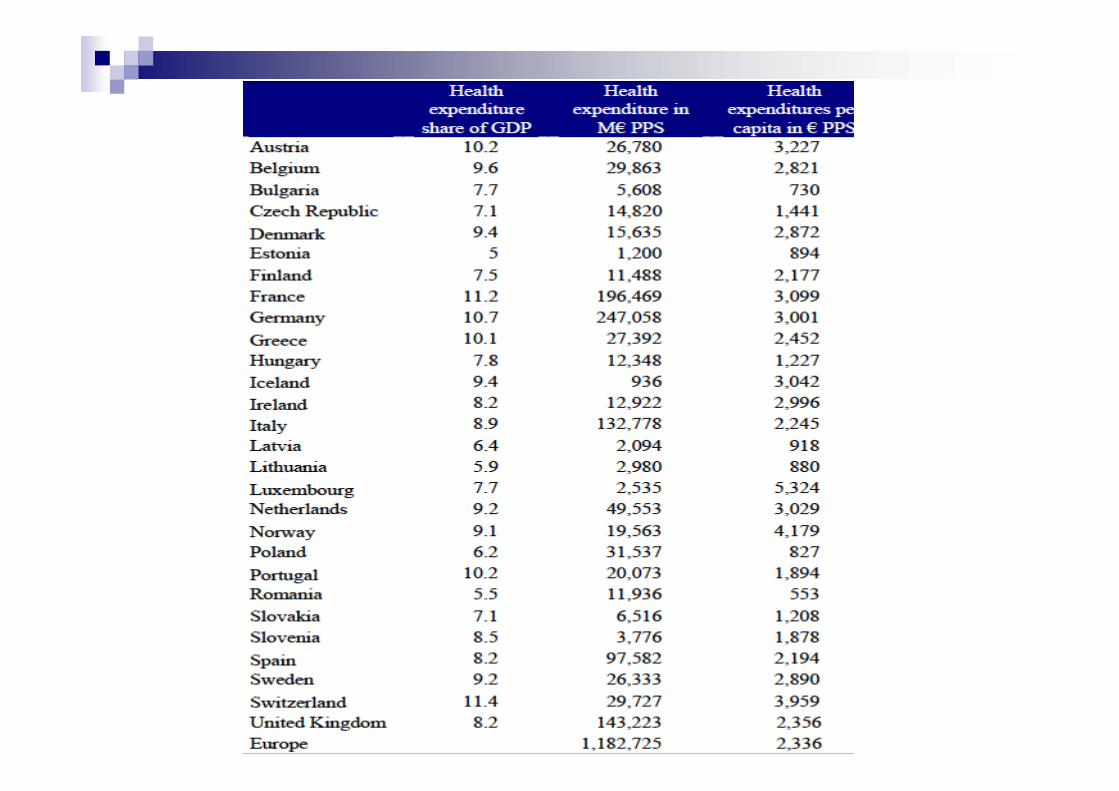
GDP per inhabitant: the spread of wealth
Lith
uani
a
2012 GDP per inhabitant
Index where the average of the 28 EU-countries is 100Lu
Significant reductions in the price of many products and services, including airfares and phone calls
More choice for consumers
2.8 million new jobs
Managing introduction of new innovative health care technologies Decision making under uncertainty Uncertainty can only be reduced at a cost Two alternativesDoing more studies before introduction
May reduce risks But delay potential benefits
Follow up studies after introduction For risk assessment For effectiveness assessment
Lack of effectiveness – Loss of money and health Loss of moneyBecause money spent on ineffective usage
does not contribute to improved outcome Loss of health Because resources has alternative uses
within the health care budget
Increased risk of loss of money?
Annual costs for treatment with new drugs TNF alfa (RA); approx 15 000 Euro Tysabri (MS); approx 25 000 Euro Avastin (Cancer); approx 50 000 Euro (in colon
cancer) Eculizimab (orphan drug), approx 300 000 Euro
Drugs used in small populations with severe disease carry relatively small health risks But the economic risk from incorrect ineffective use
can be substantial And must be balanced against patient benefits
What are the implications? Without third party payment (reimbursement) very few
patients can afford to use the new opportunties Challenge for health care systems based on the principle of
equity Co-payments have no meaning
Small economic incentives for innovation without reimbursement Inefficient allocation of resources since price < cost
Reimbursement decisions must take both costs and effectiveness into account For an efficient and just allocation of resources To create correct incentives for innovation
Problems assessing cost-effectiveness before market authorization
Reimbursement agencies and payers are interested in how the new drug can improve clinical practice and patient outcomeClinical trial data and other scientific
information is helpful but not conclusive Cost-effectiveness is based estimations,
often with help of modelsNeed for follow up and verification of
assumptions
Requests for follow up studies are commonTLV in Sweden as example
Follow up to secure that the drug is used for the right patients (reimbursed indication) Xenical, Reductil (weight loss) Champis (smoke cessation)
Follow up to verify predicted effectiveness and/or cost-effectiveness Fosteo (osteoporosis) Elidel (excema)
Opportunities for developing of new models for payment Coverage by evidence developmentData is collected which are used for
reassessment of the reimbursement decision Risk sharing If predicted goals are not met, payment will be
adjusted Pay for performancePayment per patient treated adjusted for
outcome or other “quality” indicators
Experiences so far
About 60 schemes so farNumbers increasing over timeMajority in EU
Most are coverage by evidence developmentTLV and CMS (US) most active
Some successesBut problems with data collection
Experiences with patient registersFrom a health economic perspective
Data collection too costly and complicated Lack of variables related to patient
outcome and resource allocation Limited access for “outsiders” Not used to their full potential as an
instrument to improve health care and health outcomes
Data is like children…
You like your own best, and do not like strangers to play with them
Why European collaboration?
Information is a public good The value is not reduced if many share it
But costs of producing it are reduced if shared Time is essentialCollaboration gives information faster
Variations in use between countriesGives opportunities to learn from each other
..in particular from early adopters
Key European initiatives
Adaptive licencing Joint regulatory and HTA advice PAES – Post Authorization Efficacy
Studies (in addition to PASS) Assessment of relative effectiveness at the
European levelHTA and reimbursement
What is special with regenerative medicine?
“Regenerative medicine is an emerging interdisciplinary field of research and clinical applications focused on the repair, replacement, or regeneration of cells, tissues or organs to restore impaired function resulting from any cause, including congenital defects, disease, trauma and aging. It uses a combination of several technological approaches that moves it beyond traditional transplantation and replacement therapies. These approaches may include, but are not limited to, the use of soluble molecules, gene therapy, stem cell transplantation, tissue engineering, and the reprogramming of cell and tissue types” (Greenwood et al., 2006).
What is special with regenerative medicine?
”Making goods measureable and comparable is a driver of new market creation, but in the regenerative medicine field there is considerable uncertainty regarding data and product classifications, both in the UK and internationally. This means there is a very strong need for soft interactions between the regulators and stakeholders, especially with MHRA on the one hand, and NICE and Health Technology Assessment agencies on the other, because their approaches to the central issue of product classification and scientific evaluation are very different.”
conclusions from UK workshop
What is special with regenerative medicine?
”Similarly, a key intermediary agency for the NHS, the NIHR Horizon Scanning Centre, which provides notice of significant new and emerging health technologies up to three years prior to their launch in the NHS, does not have experience of how long it will take for various types of regenerative medicine therapies to diffuse since the product and development models are very different from drugs and devices”
conclusions from UK workshop
Development of a common regulatory framework for all medical technologies
Technological developments in healthcare, such as the use of nanotechnology, regenerative medicine and minimally invasive surgery have drawn the pharmaceuticals and devices closer together in terms of both development and usage.
Payers are looking for treatments, and their outcomes and costs, not products
A tentative conclusion
RM technologies have a lot in common with surgical procedures in terms of assessment of value from a payer perspective
The product is only one part of the cost, but can significantly improve the outcome
Important to include health economics early, before the selection of applications and design of studies
It is about accountability
…… all other show data
It is not all about money, but health economics matter, and should be used to support decisions during the whole development process
Health economics – A summary
Health economics is about improving resource allocation for better health
Follow up data must include variables that allow a broad perspective on value
Data must be available to all stakeholders
Health economics – A conclusion
Follow up data are key to the development of rational and accountable decisions about resource allocation
This may provide not only a more efficient allocation of resources for health in the short run but also incentives for more cost-effective innovations in the long run