Unveiling THE PERSON behind THE PAIN Recovering from MUSCULOSKELETAL PAIN Little Known Evidence-Based for Chronic Back and Neck Pain Exercising: Is it necessarily PAIN GAIN ALL ABOUT PAIN Team-Based Approach to MARCH — MAY 2012 NO ? A PUBLICATION FOR PRIMARY CARE PHYSICIANS A CRYING SHAME Managing Pain Chronic Pelvic Pain Interventional Treatment Non-Surgical MICA (P) 212/03/2010
Transcript
Unveiling THE PERSON behind THE PAIN
Recovering from MUSCULOSKELETAL
PAIN
Little Known Evidence-Based
for Chronic Back and Neck Pain
Exercising: Is it necessarily PAIN GAIN
ALL ABOUT
PAIN Team-Based Approach to
MARCH — MAY 2012
NO ?
A PUBLICATION FOR PRIMARY CARE PHYSICIANS
A CRYING SHAME
Managing Pain
Chronic Pelvic Pain
Interventional Treatment Non-Surgical
GPBUZZ
MICA (P) 212/03/2010
CHRONIC PELVIC PAINA CRYING SHAME
1812Recovering from Muscloskeletal Pain
COVER STORY
IN EVERY ISSUE
6
Cancer Pain An inter-disciplinary,
collaborative approach
20
CONTENTSWe welcome 2012 with a revamped issue of the GP Buzz. As our
readers may recall, GP Buzz has been actively engaging you on latest updates and services of Tan Tock Seng Hospital.
More than just a facelift, we promise more interesting content and line-up of medical stories which will benefit both our GP partners and their patients.
For the first issue of the revamped GP Buzz, we focus on managing pain through a multi-disciplinary and team-based approach. Pain may sound like a simple four-letter word, but it remains one of the most challenging medical conditions to address as the pain experience is unique to each patient.
Our team of specialists will share on various aspects of managing pain from non-surgical intervention treatment for chronic pain to recovering from musculoskeletal pain. Find out more from our Psychologist on understanding the various aspects of living with pain. Let our Principal Physiotherapist shed light on the right approach to exercising.
The exclusive interview with Professor Martyn Partridge, Senior Vice Dean of the Lee Kong Chian School of Medicine, provides insights on Singapore’s newest Medical School.
As part of the revamp, you will be reading regular columns such as Fitness and Healthy Recipes. Look out for our CME Updates and Newsroom as we update you on the latest line-up of events and services.
We hope you enjoy reading this issue and find it a useful reference in helping you to help your patients live a pain-free and fulfilling life.
The Editorial Team
GP BUZZ The Editorial Team : Celine Ong, Lee Wei KitAdvisory Panel : Associate Professor Thomas Lew Associate Professor Chia Sing Joo Associate Professor Chin Jing Jih Dr Chong Yew Lam Dr Tan Kok Leong Joe Hau
Living a
16Exercising: Is it necessarily No Pain, No Gain?
10Little Known Evidence-Based
Non-Surgical Interventional Treatment for Chronic Back and Neck Pain
14Unveiling the Person Behind the Pain
Nurturing Tomorrow’s Doctors Today
ALL aboutTeam-based Approach to Managing Pain
PAIN Pain-FreeLife
8
HIGHLIGHT
We value your feedback on how we can enhance the content of GP Buzz. Please send in your comments and queries to [email protected]
3M A R C H – M A Y 2 0 1 22 M A R C H – M A Y 2 0 1 2
GP BUZZ | CONTENTS GP BUZZ | EDITOR’S NOTE
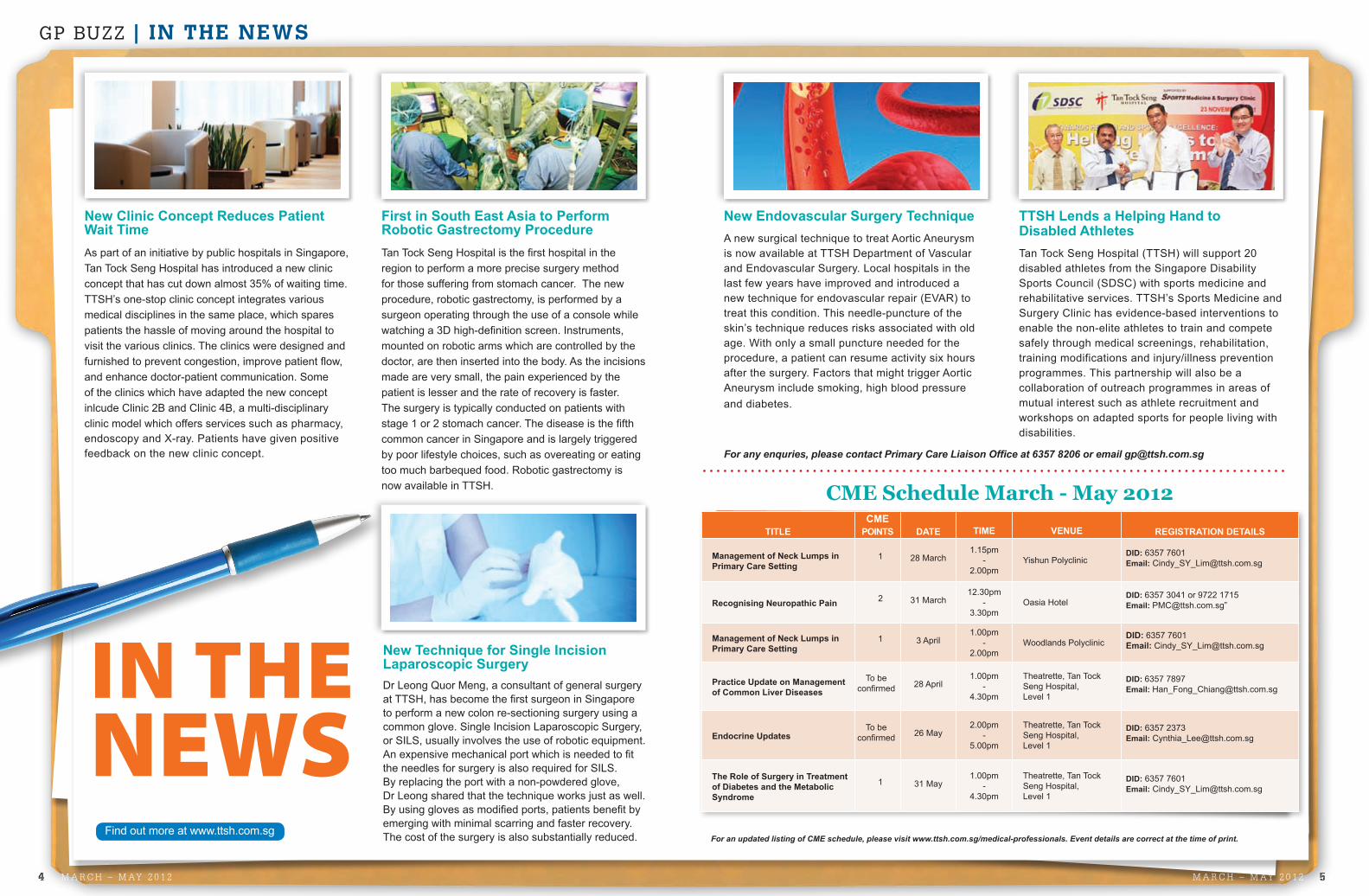
New Technique for Single Incision Laparoscopic SurgeryDr Leong Quor Meng, a consultant of general surgery at TTSH, has become the first surgeon in Singapore to perform a new colon re-sectioning surgery using a common glove. Single Incision Laparoscopic Surgery, or SILS, usually involves the use of robotic equipment. An expensive mechanical port which is needed to fit the needles for surgery is also required for SILS. By replacing the port with a non-powdered glove, Dr Leong shared that the technique works just as well. By using gloves as modified ports, patients benefit by emerging with minimal scarring and faster recovery. The cost of the surgery is also substantially reduced.
New Endovascular Surgery Technique A new surgical technique to treat Aortic Aneurysm is now available at TTSH Department of Vascular and Endovascular Surgery. Local hospitals in the last few years have improved and introduced a new technique for endovascular repair (EVAR) to treat this condition. This needle-puncture of the skin’s technique reduces risks associated with old age. With only a small puncture needed for the procedure, a patient can resume activity six hours after the surgery. Factors that might trigger Aortic Aneurysm include smoking, high blood pressure and diabetes.
First in South East Asia to Perform Robotic Gastrectomy ProcedureTan Tock Seng Hospital is the first hospital in the region to perform a more precise surgery method for those suffering from stomach cancer. The new procedure, robotic gastrectomy, is performed by a surgeon operating through the use of a console while watching a 3D high-definition screen. Instruments, mounted on robotic arms which are controlled by the doctor, are then inserted into the body. As the incisions made are very small, the pain experienced by the patient is lesser and the rate of recovery is faster. The surgery is typically conducted on patients with stage 1 or 2 stomach cancer. The disease is the fifth common cancer in Singapore and is largely triggered by poor lifestyle choices, such as overeating or eating too much barbequed food. Robotic gastrectomy is now available in TTSH. CME Schedule March - May 2012
IN THE NEWS
TTSH Lends a Helping Hand to Disabled AthletesTan Tock Seng Hospital (TTSH) will support 20 disabled athletes from the Singapore Disability Sports Council (SDSC) with sports medicine and rehabilitative services. TTSH’s Sports Medicine and Surgery Clinic has evidence-based interventions to enable the non-elite athletes to train and compete safely through medical screenings, rehabilitation, training modifications and injury/illness prevention programmes. This partnership will also be a collaboration of outreach programmes in areas of mutual interest such as athlete recruitment and workshops on adapted sports for people living with disabilities.
For an updated listing of CME schedule, please visit www.ttsh.com.sg/medical-professionals. Event details are correct at the time of print.
New Clinic Concept Reduces Patient Wait TimeAs part of an initiative by public hospitals in Singapore, Tan Tock Seng Hospital has introduced a new clinic concept that has cut down almost 35% of waiting time. TTSH’s one-stop clinic concept integrates various medical disciplines in the same place, which spares patients the hassle of moving around the hospital to visit the various clinics. The clinics were designed and furnished to prevent congestion, improve patient flow, and enhance doctor-patient communication. Some of the clinics which have adapted the new concept inlcude Clinic 2B and Clinic 4B, a multi-disciplinary clinic model which offers services such as pharmacy, endoscopy and X-ray. Patients have given positive feedback on the new clinic concept. For any enquries, please contact Primary Care Liaison Office at 6357 8206 or email [email protected]
Find out more at www.ttsh.com.sg
To be confirmed
To be confirmed
5M A R C H – M A Y 2 0 1 24 M A R C H – M A Y 2 0 1 2
GP BUZZ | IN THE NEWS
107 Mandalay Road willbe the headquarters ofthe new Novena Campus
Nurturing Tomorrow’s Doctors TodaySenior Vice Dean of the Lee Kong Chian School of Medicine (LKCSoM), Prof Martyn Partridge, shares his insights into the development of Singapore’s newest medical school which opens in 2013.
#1 HOW HAS THE TEACHING OF MEDICINE CHANGED IN THE 21ST CENTURY? I think teaching today is like life - changing rapidly. We have to imbue in our medical students the importance of lifelong learning so they can adapt. They can only do this if they understand the scientific basis of medicine, because no one knows what will be thrown at us in five or 10 years’ time.
Teaching has also changed dramatically. In the old days, medicine was lecture-based and about clinical seminars. But very often, learning was also about apprenticeships — following great men on their ward rounds.
Today, we use new technologies such as e-learning, problem-based learning, and team learning while also relying on traditional clinical seminars and apprenticeships. This concept of blended learning permits us to select the best method for the outcome we wish to achieve.
#2 YOU’VE CONSISTENTLY STRESSED THE IMPORTANCE OF DOCTORS PUTTING THEIR PATIENTS FIRST. HOW CAN SUCH A SCHOOL OF THOUGHT TRANSLATE INTO PRACTICE AT THE NEW SCHOOL? I personally believe that service has dropped out of medicine to some extent, and we need to put it back. To a large extent this involves the selection of medical students with the right qualities, and then providing students with the training and evidence in favour of a
patient-centred system. The evidence is overwhelming that good doctor-patient communication and shared decision-making enhance satisfaction and compliance and dramatically reduce health care costs. Singapore cannot afford not to adopt this approach.
As patients’ expectations change, doctors must deliver the type of care that is necessary for those who receive it. I would like people to say that the doctors we have produced are the type that we would wish to be cared for by ourselves.
#3 GIVEN THE SCHOOL’S LINKS WITH IMPERIAL COLLEGE, WE IMAGINE THAT THE LKCSoM WILL SEE A HIGH-LEVEL OF INTERNATIONAL COLLABORATIONS. CAN YOU TELL US WHAT SOME OF THESE COLLABORATIONS MIGHT BE?
We will undertake some structured electives for final year IC students. Starting from 2013, there will be 30 of them coming to Singapore for a seven-week period to learn more about global health and international health. They will be undertaking seminars both at the Nanyang Technological University (NTU) and Tan Tock Seng Hospital (TTSH). June also sees the first LKCSoM lecture whereby visiting Imperial staff undertake Large Group Interactive Seminars at TTSH, NTU, KK Women’s and Children’s Hospital and elsewhere to share expertise; and that’s an example of the collaborations we wish to see.
Prof Martyn Partidge
N E W M E D I C A L C A M P U S @ N O V E N A
In the heart of Novena Campus is this wonderful and iconic heritage building along
Mandalay Road which will be our headquarters. The rear of the newly-built education block will be used subsequently for conferences, Master’s courses and post-graduate teaching even when our adjacent 14-storey clinical science building has been built. The intention is for the building to be ready in 2013, a few months before classes start in August. The NTU Novena campus will be immediately adjacent to amazing healthcare facilities, a new national Communicable Diseases Centre, TTSH and the National Skin Centre building. Novena will be a wonderful campus, and a little medical hub in itself.
Republished with permission from LifeWise, National Healthcare Group.
#4 WHAT WOULD BE A TYPICAL SCHOOL DAY IN THE LIFE OF A LKCSoM FIRST YEAR AND THIRD YEAR STUDENT?In the first year, students will spend two days a week at NTU attending seminars, practical sessions, and classes with team-based learning, and problem-solving. The other three days will be spent on a clinical campus either at Novena, a polyclinic or a step-down hospital, attending, clinical seminars and visiting the wards to interview patients and acquire skills in listening to and examining patients.
There will also be special LKCSoM suites of consultation rooms and seminar rooms in up to three polyclinics, where teachers will train students in basic clinical skills. The students will cut their teeth in history-taking and patient examination with simulated patients in communication laboratories, then with paid teachers in a polyclinic, before attending to ill patients in hospitals. We have to help our students realise that health care is delivered in many settings, not just within hospitals.
Increasingly in Years Three, Four and Five, students will be working round the clock in the same way that junior doctors do. We’re talking 24/7 work. Some of the most taxing aspects of clinical care and some of the richest learning opportunities involve acute decision-making that will occur in the emergency departments in the middle of the night.
#5 WHAT, IN YOUR OPINION, WILL SET THE LKCSoM STUDENT APART FROM HIS OR HER PEERS?
We’ve put a lot of thought into how medicine is developing. To produce graduates ready for the challenges and methods of working in 2018 and beyond, our students will have very early exposure to bio-engineering, business school methodologies, and computer sciences. Students will get to learn from the expertise of those at NTU, which we will couple with the clinical strengths of TTSH.
Medical students should understand that regardless of whatever field they practise, they will spend the majority of their time dealing with elderly patients coping with long-term conditions, rather than necessarily making star diagnoses and saving lives of critically-ill patients.
If they don’t understand the value of integrated care and the importance of good care for those with long-term illnesses or the elderly, they will be burnt out by the age of 30 and we will have a generation of doctors who are not professionally satisfied.
#6 WHAT ARE SOME MEANINGFUL WAYS THAT NATIONAL HEALTHCARE GROUP (NHG) CAN SHARE IN LKCSoM’S EXCITING JOURNEY?
NHG staff are shaping the development of this new school in terms of clinical curriculum and in providing clinical teaching staff. I am sure that they will also welcome the scientists necessary to build a successful Medical School. There will be increasing interactions with local experts and, indeed, everyone from assistant deans to module leaders are from NHG. I think local NHG staff will enjoy the pleasure of being part of an active medical school at which new research opportunities will arise, new academic clinical scientists will be appointed, and new facilities will become available.
7M A R C H – M A Y 2 0 1 26 M A R C H – M A Y 2 0 1 2
GP BUZZ | HIGHLIGHT
Chronic pain, which is pain lasting months or years, is much different from acute pain and rarely still serves a purpose. Many medical
conditions or injuries can cause chronic pain. Some people will continue to experience pain long after recovering from an initial injury such as a back or neck injury. Other types of chronic pain are caused by chronic diseases such as arthritis or cancer. Chronic pain can be quite disabling, often preventing people from working and enjoying life. Feelings of isolation, frustration, anger and even guilt are commonly associated with chronic pain. At its worst, chronic pain is accompanied by depression. In a European Study, depression was found to be present in 20% of patients with chronic pain.
In developed countries, reports from a European study by Breivik et al1, an Australian study by Blyth et al2, and Eriksen et al3 in Denmark, showed an incidence of approximately 18%. This incidence is higher in developing countries according to a report by the WHO (5–33%), due most likely to a lack of adequate healthcare and social support networks and cost implications of treatment. In Singapore, the incidence of chronic pain is somewhere in between, estimated at 8.7%4.
Chronic pain can promulgate a vicious cycle of anxiety, dependence on other people, and sleep deprivation. Normal daily activities pose a challenge and patients lack the energy to do more for themselves. Good quality sleep becomes a rarity for someone who is in pain, or worried about being in pain. Constant sleep deprivation can lead to depression, with feelings of helplessness. Social activities as well as performance at work get affected. That is why the awareness of chronic pain needs to permeate into the community and its management has to begin in the primary care setting.
In the last three decades, there had been significant advances in knowledge regarding the biological, psychological and social aspects of the experience of pain. The promulgation of multi-disciplinary pain clinics, and the introduction of acute pain management teams into hospitals, together with advances in pharmacological, interventional and psychological management of chronic pain, is now commonplace in most developed countries in the world.
Even in a progressive healthcare environment like Singapore, some fundamental problems do impede the delivery of adequate pain relief to patients who most need it. Some identified factors include a lack of awareness of the impact of chronic pain both to the individual and to the society as a whole, a limited understanding of the conditions that may lead to chronic pain as well as a somatic approach to all conditions.
R E F E R E N C E S :1. Breivik H, Collett V, Ventafridda V. Survey of chronic pain in Europe: prevalence,
impact on daily life and treatment. Eur. J. Pain 10, 287–333 (2006).2. Blyth FM, March LM, Brnabic AJ, Jorm LR, Williamson M, Cousins MJ. Chronic pain in
Australia: a prevalence study. Pain 89, 127–134 (2001).3. Eriksen J, Jensen MK, Sjogren P, Ekholm O, Rasmussen NK. Epidemiology of chronic
non-malignant pain in Denmark. Pain 106, 221–228 (2003).4. Yeo SN, Tay KH. Pain Prevalence in Singapore. Ann Acad Med Singapore 2009;
38: 937-42
ALL aboutTeam-based Approach to Managing Pain
The promulgation of multi-disciplinary pain clinics, and the introduction of acute pain management teams into hospitals, together with advances in pharmacological, interventional and psychological management of chronic pain, are now commonplace in most developed countries in the world.
The same European Study revealed that 61% of individuals with chronic pain were less able or unable to work outside the home and that 19% lost their jobs because of pain.
Some people have pain that do not have an identifiable cause. This is not to say that the pain is not real. Whatever the cause, chronic pain is real and should be treated. A number of organisations in their different ways and with differing objectives helps to fulfill the dictum that ‘pain treatment is a human right’ but there is much more to do.
To conclude, much progress has been made in the education of those responsible for the management of pain and its treatment in our medically-advanced society. Yet, this is far from sufficient and perhaps this brief insight will encourage our readers to find ways of helping to solve the many problems that continue to exist to ensure that the right and timely treatment for all patients in pain.
Dr Nicholas HL Chua is Head of the Acute Pain Service and Consultant Anesthesiologist and Pain Specialist in Tan Tock Seng Hospital Singapore. He specializes in Interventional Pain Management for chronic cancer and non-cancer pain. Dr Chua completed his Medical and Anesthesiology training in the National University of Singapore. He completed his Fellowship of Interventional Pain Physician (FIPP) accreditation in 2007 by the World Institute of Pain (WIP) in Memphis-Tennessee, United States of America.
Dr Nicholas HL Chua
PAIN
9M A R C H – M A Y 2 0 1 28 M A R C H – M A Y 2 0 1 2
GP BUZZ | COVER STORY
The commonly accepted definition for chronic non-cancer pain is pain lasting
longer than three months or beyond the expected period of healing of tissue pathology. In a local survey, the incidence for chronic back pain estimated that 16% of males and 14-20% of females; and for chronic neck pain, 9% of males and 10% of females1. This prevalence is likely to be increased markedly in view of the aging population trend.
PAIN MANAGEMENT TECHNIQUESNon-surgical interventional pain treatment methods had been utilised by numerous pain practitioners for decades. These techniques have gained a definite place in the management of chronic pain syndromes. The challenge of chronic non-cancer pain is not only in the treatment itself but also in establishing an accurate diagnosis. The diagnostic process, which is the cornerstone for establishing a treatment plan, is as important in chronic back and neck pain as with any other medical condition. However, the search for mechanisms underlying chronic spinal pain is made daunting by the frequent lack of significant structural abnormalities as revealed by radiological imaging2. Even if detected, these radiological findings
are usually related to age and bear little correlation with symptoms. Conversely, there is no correlation demonstrated between degenerative changes and pain intensity, whilst radiologically defined cervical spondylosis may be present in significant number of asymptomatic individuals3.
Unfortunately, the utilisation of non-quantitative diagnostic tests such as medial branch blocks, provocative discography or nerve root blocks is still not common in most pain centres today.
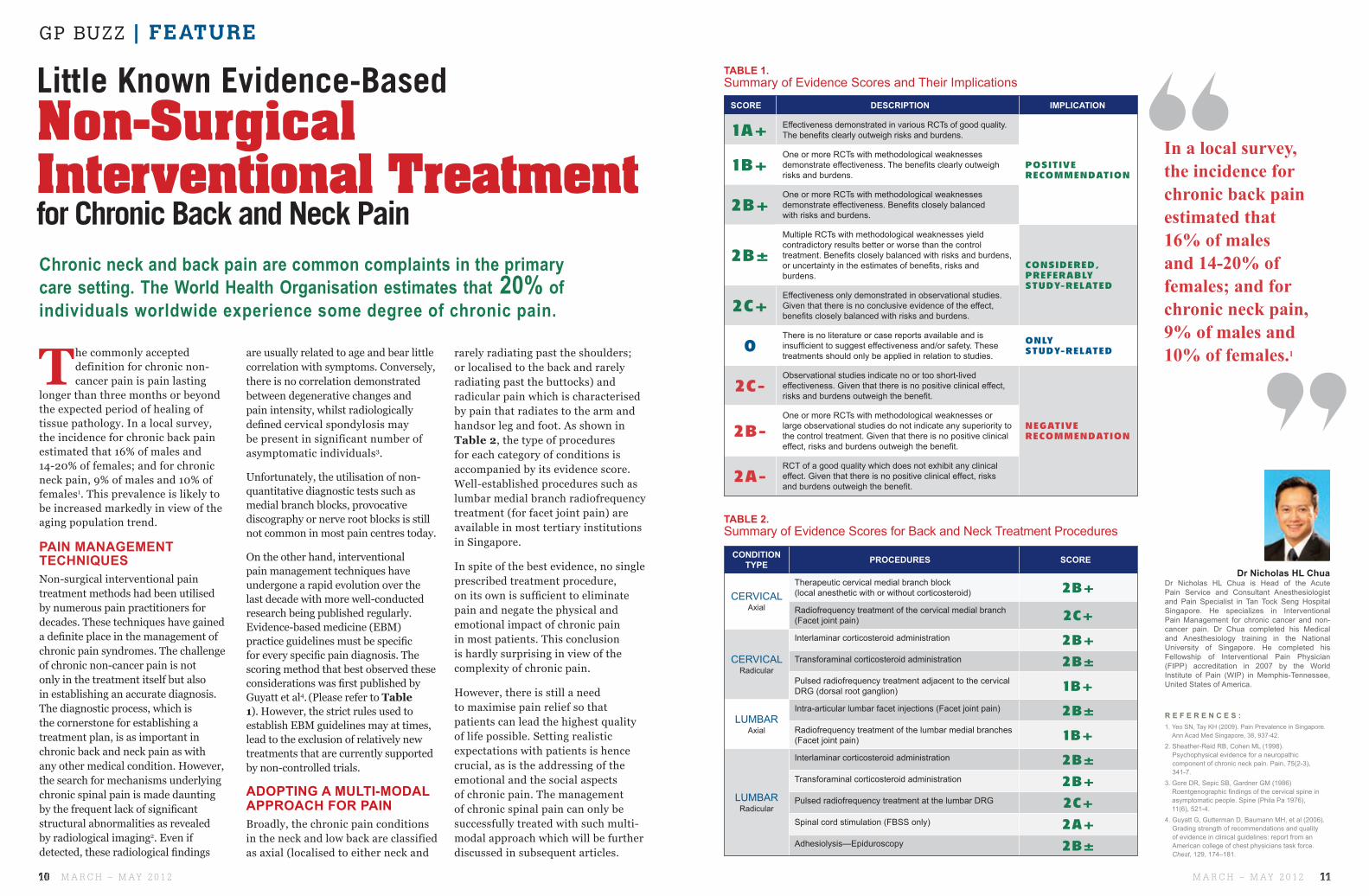
On the other hand, interventional pain management techniques have undergone a rapid evolution over the last decade with more well-conducted research being published regularly. Evidence-based medicine (EBM) practice guidelines must be specific for every specific pain diagnosis. The scoring method that best observed these considerations was first published by Guyatt et al4. (Please refer to Table 1). However, the strict rules used to establish EBM guidelines may at times, lead to the exclusion of relatively new treatments that are currently supported by non-controlled trials.
ADOPTING A MULTI-MODAL APPROACH FOR PAINBroadly, the chronic pain conditions in the neck and low back are classified as axial (localised to either neck and
rarely radiating past the shoulders; or localised to the back and rarely radiating past the buttocks) and radicular pain which is characterised by pain that radiates to the arm and handsor leg and foot. As shown in Table 2, the type of procedures for each category of conditions is accompanied by its evidence score. Well-established procedures such as lumbar medial branch radiofrequency treatment (for facet joint pain) are available in most tertiary institutions in Singapore.
In spite of the best evidence, no single prescribed treatment procedure, on its own is sufficient to eliminate pain and negate the physical and emotional impact of chronic pain in most patients. This conclusion is hardly surprising in view of the complexity of chronic pain.
However, there is still a need to maximise pain relief so that patients can lead the highest quality of life possible. Setting realistic expectations with patients is hence crucial, as is the addressing of the emotional and the social aspects of chronic pain. The management of chronic spinal pain can only be successfully treated with such multi-modal approach which will be further discussed in subsequent articles.
CONDITION TYPE PROCEDURES SCORE
CERVICAL Axial
Therapeutic cervical medial branch block (local anesthetic with or without corticosteroid) 2B+Radiofrequency treatment of the cervical medial branch (Facet joint pain) 2C+
CERVICAL Radicular
Interlaminar corticosteroid administration 2B+Transforaminal corticosteroid administration 2B±Pulsed radiofrequency treatment adjacent to the cervical DRG (dorsal root ganglion) 1B+
LUMBAR Axial
Intra-articular lumbar facet injections (Facet joint pain) 2B±Radiofrequency treatment of the lumbar medial branches (Facet joint pain) 1B+
LUMBAR Radicular
Interlaminar corticosteroid administration 2B±Transforaminal corticosteroid administration 2B+Pulsed radiofrequency treatment at the lumbar DRG 2C+Spinal cord stimulation (FBSS only) 2A+Adhesiolysis—Epiduroscopy 2B±
SCORE DESCRIPTION IMPLICATION
1A+ Effectiveness demonstrated in various RCTs of good quality. The benefits clearly outweigh risks and burdens.
POSITIVE RECOMMENDATION
1B+One or more RCTs with methodological weaknesses demonstrate effectiveness. The benefits clearly outweigh risks and burdens.
2B+One or more RCTs with methodological weaknesses demonstrate effectiveness. Benefits closely balanced with risks and burdens.
2B±Multiple RCTs with methodological weaknesses yield contradictory results better or worse than the control treatment. Benefits closely balanced with risks and burdens, or uncertainty in the estimates of benefits, risks and burdens.
CONSIDERED, PREFERABLYSTUDY-RELATED
2C+Effectiveness only demonstrated in observational studies. Given that there is no conclusive evidence of the effect, benefits closely balanced with risks and burdens.
0There is no literature or case reports available and is insufficient to suggest effectiveness and/or safety. These treatments should only be applied in relation to studies.
ONLY STUDY-RELATED
2C-Observational studies indicate no or too short-lived effectiveness. Given that there is no positive clinical effect, risks and burdens outweigh the benefit.
NEGATIVE RECOMMENDATION2B-
One or more RCTs with methodological weaknesses or large observational studies do not indicate any superiority to the control treatment. Given that there is no positive clinical effect, risks and burdens outweigh the benefit.
2A-RCT of a good quality which does not exhibit any clinical effect. Given that there is no positive clinical effect, risks and burdens outweigh the benefit.
TABLE 1. Summary of Evidence Scores and Their Implications
Chronic neck and back pain are common complaints in the primary care setting. The World Health Organisation estimates that 20% of individuals worldwide experience some degree of chronic pain.
R E F E R E N C E S :1. Yeo SN, Tay KH (2009). Pain Prevalence in Singapore.
Ann Acad Med Singapore, 38, 937-42.
2. Sheather-Reid RB, Cohen ML (1998). Psychophysical evidence for a neuropathic component of chronic neck pain. Pain, 75(2-3), 341-7.
3. Gore DR, Sepic SB, Gardner GM (1986)Roentgenographic findings of the cervical spine in asymptomatic people. Spine (Phila Pa 1976), 11(6), 521-4.
4. Guyatt G, Gutterman D, Baumann MH, et al (2006). Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American college of chest physicians task force. Chest, 129, 174–181.
Dr Nicholas HL Chua is Head of the Acute Pain Service and Consultant Anesthesiologist and Pain Specialist in Tan Tock Seng Hospital Singapore. He specializes in Interventional Pain Management for chronic cancer and non-cancer pain. Dr Chua completed his Medical and Anesthesiology training in the National University of Singapore. He completed his Fellowship of Interventional Pain Physician (FIPP) accreditation in 2007 by the World Institute of Pain (WIP) in Memphis-Tennessee, United States of America.
Dr Nicholas HL Chua
Little Known Evidence-Based
for Chronic Back and Neck PainInterventional Treatment Non-Surgical
In a local survey, the incidence for chronic back pain estimated that 16% of males and 14-20% of females; and for chronic neck pain, 9% of males and 10% of females.1
TABLE 2. Summary of Evidence Scores for Back and Neck Treatment Proceduresures
11M A R C H – M A Y 2 0 1 210 M A R C H – M A Y 2 0 1 2
GP BUZZ | FEATURE
RECOVERING FROM
MUSCULOSKELETAL
PAINLIFESTYLE AND AGING
With modernisation of society, our lifestyles have become increasingly sedentary. We spend more time in our daily work routine sitting
down and maintaining a static posture. Our postural muscles tend to become less flexible. On the other hand, the muscles that we use for dynamic activities gradually lose their bulk and strength. Through relative inactivity and disuse, these muscles become lax and weak. This static-dynamic muscle imbalance is prevalent in a modern society.
With aging, our soft tissues, tendons and ligaments become more fibrous, stiff and rigid. Coupled with the muscle imbalance, there is a gradual loss of flexibility, strength and coordination, as well as cushioning and support.
Rehabilitation helps to rebalance postural and dynamic muscles, and optimise the function of our musculoskeletal soft tissues. It helps to lessen the likelihood of chronic pain developing, while facilitate a faster recovery from pain.
ACHES AND PAINChronic pain can be an unpleasant sensory and emotional experience. It can be a complex multi-dimensional problem. Some of us have undergone physical therapy, medical or surgical treatment to deal with it. The outcome, however, may be unsatisfactory. An integrated multi-modal holistic approach, addressing important pain contributing factors from all dimensions, is often needed for effective management of chronic pain.
The goals of rehabilitation include: reduce pain intensity, pain frequency and physical limitations; as well as restore daily activities and improve function. Rehabilitation also helps to improve your confidence, productivity, and quality of life.
NON-PHARMACOLOGICAL MANAGEMENTPhysical modalities relieve pain by their local effects on soft tissues. However, you may have found that mechanical traction, heat or electrical therapy only help ease your pain temporarily. Physical modalities are helpful supplementary treatments. When combined with appropriate exercises to actively rebalance our muscles, together with addressing any physical, postural, environmental or psychosocial factors aggravating the pain, we achieve longer and more lasting efficacy.
Many of us suffer from aches and pain. Some are acute and self limiting while others can be chronic with long lasting functional consequences. The treatment of pain itself does not always guarantee full functional recovery. Rehabilitation can help pain sufferers achieve a better recovery and reduced recurrence.
Rehabilitation helps to rebalance postural and dynamic muscles, and optimise the function of our musculoskeletal soft tissues.
CONTRIBUTING FACTORS
1MEDICAL FACTORSIs there an underlying cause to your chronic pain? Is it a serious cause? Although uncommon,
it is important that serious causes, such as fractures, inflammation, infections and cancer receive early attention and treatment.
2PHYSICAL AND ENVIRONMENTAL FACTORSDo you experience poor bio-mechanics of body movement when performing your daily activities?
Do you overuse your muscles too intensively or repetitively, resulting in strain or sprain? Do you have poor ergonomics, a sub-optimal working environment or a poor working posture? Physical and environmental factors are common causes of aches and pain in today’s modern society.
3PSYCHO-SOCIAL FACTORSIs there a psychosocial factor to your aches and pain? Stress and anxiety, low mood and lack of sleep,
may precipitate, amplify and perpetuate your aches and pain. The attendant emotional toll may impede recovery. Cognitive counselling and behavioural therapy, as well as relaxation techniques with coping skills are helpful adjunctive treatments. They are important components of a holistic chronic pain management programme.
Most aches and pain will improve with conservative rehabilitation – one that is without surgery or invasive treatment. Occasionally, some of us may need surgery or invasive treatment. After the operation, the symptoms may improve. However, you may still have decreased functional participation. Rehabilitation may further help to improve your daily function and quality of life.
Needling and injection help to relieve pain by mechanically disrupting and releasing taut bands in achy painful muscles; modulating the pain signal transmission between the peripheral and central nervous systems and stimulating the release of endorphins – natural pain relieving substances within our body system. During needling, local anaesthetics are occasionally infiltrated to reduce soft tissue soreness. Steroids are occasionally injected to treat any attendant inflammation. However, it is important that any underlying aggravating or perpetuating factor is addressed, and our musculoskeletal soft tissues are actively reconditioned and rebalanced with appropriately prescribed exercises, to reduce pain recurrence.
YOU OWN YOUR BODYYou are the owner of your body, your muscles, bones and joints. You have to use them, actively and regularly, to keep them in a good condition. If you don’t, you will lose them. They will become de-conditioned and waste away. General exercises condition our musculoskeletal system and build up physical endurance. Specific exercises help rebalance our musculoskeletal system and optimise biomechanical function. General conditioning and specific rebalancing exercises complement each other in the rehabilitation of chronic aches and pain.
Chronic pain can be disruptive. It can bring despair, anxiety and a feeling of worthlessness. It can make us tense and irritable. It may trigger avoidance of daily activities and affect our psychosocial well being. Behavioural therapy is another important component of chronic pain rehabilitation. Through relearning and remediation, we can manage and cope better with chronic pain, and lead a more productive life.
QUESTIONS A PATIENT MAY ASK!
MANAGE YOUR ACHES AND PAINRehabilitation of musculoskeletal pain starts with diagnosing the pain generators and identifying the environmental and psychological contributors to pain. Conservative management including physical modalities, needling and injections, therapeutic exercises, modification of ergonomics and biomechanical body usage, together with pacing of activity and cognitive behavioural therapy is helpful, not only to treat pain, but also to lessen likelihood of its recurrence.
Adj Asst Prof Tjan Soon Yin (MBBS, FRCP, FAMS(Rehab) is Consultant and Deputy Head at the Department of Rehabilitation Medicine in Tan Tock Seng Hospital. Adj Asst Prof Tjan completed his rehab speciality training in 2006 and has also done a HMDP in chronic pain management in Adelaide, Australia. He is concurrently Consultant, Pain Management Clinic of Tan Tock Seng Hospital. Adj Asst Prof Tjan’s subspeciality interest is in cognitive behavioral therapy for chronic pain management, musculoskeletal medicine and amputee rehabilitation.
Adj Asst Prof Tjan Soon Yin
Dr Yap Eng Ching is a Consultant at the Department of Rehabilitation Medicine in Tan Tock Seng Hospital. He is fellowship trained in musculoskeletal rehabilitation. His main interest is in medical rehabilitation of the spine and musculoskeletal conditions.
Dr Yap Eng Ching
13M A R C H – M A Y 2 0 1 212 M A R C H – M A Y 2 0 1 2
GP BUZZ | FEATURE
the person behind theUNVEILING PATIENTS MUST
REALISE THAT BEING INVOLVED IN THEIR OWN RECOVERY, AND TAKING RESPONSIBILITY FOR THEIR CONDITION IS IMPORTANT
R E F E R E N C E S :1. Yeo, S.N., & Tay, K.H. (2009). Pain Prevalence
in Singapore Ann Acad Med Singapore, 38(11), 937-942.
2. Jensen, M.P., Turner, J.A., Romano, J.M. (1991). Self-efficacy and outcome expectancies: Relationship to chronic pain coping strategies and adjustment. Pain, 44, 263-269.
Jensen, M.P., Nielson, W.R., Turner, J.A., Romano, J.M., Hill, M.L. (2004). Changes in readiness to self-manage pain are associated with improvement in multidisciplinary pain treatment and pain coping. Pain, 111, 84-95.
3. Arnstein, P., Caudill, M., Mandle, C.L., Norris, A., Beasley, R. (1999). Self-efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain, 80, 483-491.
4. Turner, J., Jensen, M., Romano, J. (2000). Do beliefs, coping and catastrophsing independently predict functioning in patients with chronic pain after spinal cord injury. Pain, 85, 115-125.
5. Walsh, D.A., & Radcliffe, J.C. (2002). Pain beliefs and perceived physical disability of patients with chronic low back pain. Pain, 97, 23-31.
6. McCracken, L.M., & Yang, S.Y. (2006). The role of values in a contextual cognitive-behavioural approach to chronic pain. Pain, 123, 137-145.
7. McCracken L.M., Carson, J.S., Eccleston, C., Keefe, F. (2004). Acceptance and change in the context of chronic pain. Pain, 109, 4-7.
B I B L I O G R A P H Y1. Prochaska, J., & DiClemente, C. (1984). The
transtheoretical approach: Crossing traditional boundaries of therapy. Homewood, IL: Dow Jones Irwin.
COGNITIONS AND BEHAVIOURS
BELIEFSSome beliefs that chronic pain patients hold are detrimental to their ability to function. Patients may hold folk beliefs or unhelpful beliefs, that lead them to think that they are and should be disabled by their pain. An example of an unhelpful belief within the context of chronic pain is that, “pain equates harm”, which is a statement that does not necessarily hold true all the time. Unhelpful thoughts about one’s pain condition are likely to become unhelpful behaviours that lead patients away from managing their pain condition effectively.
Studies have shown that beliefs about pain are associated with physical dysfunction2, 3, 4. These include beliefs that “one is by necessity disabled by pain, that one has little personal control over pain, or that pain will be an enduring part of life in the future”5.
NEGATIVE THOUGHTSIn addition to unhelpful beliefs, chronic pain patients may also endorse negative self-statements, such as “I am useless”, “I am going to become an invalid” and “ I can no longer do anything”, when in pain. These exaggerated, general sweeping statements otherwise known as catastrophising, can affect daily activities and function. Catastrophising is a maladaptive coping strategy which allows the patient to solicit support or empathy and at the same time present with helplessness, pessimism and rumination of a poor pain-related outcome.
FEAR AVOIDANCEAnother common behaviour of a chronic pain patient is fear-avoidance. Fear-avoidance refers to the avoidance of movements or activities based on fear of triggering pain. Patients who avoid activities that they anticipate would trigger pain, are caught in a downward spiral of increasing avoidance, disability and pain. Such unhelpful behaviours are rarely corrected and tend to persist. Patients continue to have wrongful expectancies and beliefs about pain as a signal of threat to their physical well-being. These unhealthy learned behaviours become difficult to treat over time and often lower patients’ confidence to manage pain.
EMOTIONSNaturally, futile attempts to get rid or decrease pain, will result in emotional reactions. Patients are often depressed, anxious or may experience symptoms of both emotional conditions. Depression results from helplessness over a long drawn illness that does not have a cure. Anxiety happens when patients fear that any new perceived symptom is a sign of pain or disease progression, especially when told that there is no quick fix to their condition. Often, other feelings, like that of anger, frustration, irritation and helplessness also follow.
Imagine how this might feel for a patient who has to bear not only with physical pain but also emotional discomfort and possible social isolation?
TREATMENTAs chronic pain is a multifaceted condition, effective treatment requires not only a multidisciplinary approach but more importantly, for patients to adopt a self-management style in managing pain. Group treatment sessions, in which patients are taught how to pace their activities, to know their limits of tolerance, to identify negative and unhelpful thoughts, and challenge these thoughts with helpful effective ones are recommended. Through these processes and others taught during the session, patients’ behaviours may be modified.
A recent popular focus of pain treatment is in the area of pain acceptance. Treatment approaches that utilise psychological acceptance as a main feature of therapy often incorporate some work related to the patient’s personal values6, 7 found that the patients with higher success at coping were living according to their values, they experience less depression, depression-related interference with functioning and pain related anxiety.
Often, the challenge for treatment is to engage patients’ low willingness to self-manage, accept their current pain, to stop doctor hop and to try to lead as normal a life as possible. Moving patients’ focus away from pain to living out the life they have missed out due to pain is a challenge all practitioners face.
MOVING ONChronic pain conditions ‘motivate’ the patient towards persistence to seek a cure, and chase a “pain-free” lifestyle that they may never achieve or experience. Patients often start by pursuing “curative” avenues of both invasive and non-invasive options in the medical field or pharmaceutical market. Patients often buy easily into ideas of passive coping (example massage, acupuncture, medication) as opposed to management techniques that require active coping (example, self-management of pain through psychological acceptance, self-monitoring, pacing, and thought management).
Patients must realise that being involved in their own recovery, and taking responsibility for their condition is important. They should not leave pain control to a medical professional or someone else. There is no easy cure for chronic pain problems, but it is possible to regain control of daily life when patients direct their energies and thoughts away from pain to areas of life that hold more meaning.
Ms Yang Su-Yin is a Senior Psychologist at the Pain Management Clinic in Tan Tock Seng Hospital. She is a member of the British Psychological Society and the International Association for the Study of Pain. Her clinical interest is in chronic pain management.
Ms Yang Su-Yin
Chronic pain is a debilitating disease that affects every facet of an individual’s life, encompassing not only the physical but the social, emotional and, mental dimension of life. It is portrayed as a silent enemy with an estimated prevalence of 8.7 % of the population in Singapore experiencing it1.
Pharmaceutical companies brandish new drugs, advertising them as the unique solutions to pain. However, with chronic pain, it is imperative to address the cognitive, emotional and behavioural aspects that tag on to the patient.
15M A R C H – M A Y 2 0 1 214 M A R C H – M A Y 2 0 1 2
GP BUZZ | FEATURE
Ms Loy Fong Ling is a Principal Physiotherapist at the Physiotherapy Department and the Pain Management Clinic in Tan Tock Seng Hospital. Ms Loy graduated from King’s College, London, and obtained a postgraduate (MScMed) in Pain Management from University of Sydney in 2006. She has a special interest in pain management, specifically chronic musculoskeletal pain.
Ms Loy Fong Ling
R E F E R E N C E S :1. Hoheisel U, Unger T, Mense S (2007). Sensitization of rat dorsal horn neurons by NGF
induced subthreshold potentials and low-frequency activation. A study employing intracellular recordings in vivo. Brain Res, 1169, 34–43.
2. Lannersten L, Kosek E (2010). Dysfunction of endogenous pain inhibition during exercise with painful muscles in patients with shoulder myalgia and fibromyalgia. Pain, 151, 77–86.
3. Slater H, Arendt-Nielsen L, Wright A, Graven-Nielsen T (2005). Sensory and motor effects of experimental muscle pain in patients with lateral epicondylalgia and controls with delayed onset muscle soreness. Pain, 114, 118-130.
B I B L I O G R A P H Y1. William D McArdle WD, Katch FI, Katch, VL. Exercise Physiology ( 2001): Energy,
Nutrition, and Human Perfoce. Lippincott Williams & Wilkins, 5th Ed .
Exercising for such individuals would therefore require a re-think about what can be considered “an acceptable” exercise intensity, and what does the resultant exercise-induced pain mean. To reap the benefits of reconditioning exercises and not lapse into a pain flare up, exercise has to be done with sound pacing and one has to be educated about pain and the effects of exercise. With good pacing, pain levels can be kept more stabilised.
Individuals can start exercising at a lower intensity that does not cause a flare up in pain. Exercise should also be interspersed with stretching and rest breaks. Exercise would then be progressed gradually with consideration of post exercise pains. This must be done in a structured manner and recorded to help an individual plan and evaluate. While exercising in the presence of pain can cause more pain, it need not have to be a very painful process.
While the neurophysiology of exercise and pain gets somewhat complicated, an individual may not be clued in to them and would just perceive that exercise simply worsens his or her condition and he or she should stop it. In an acute pain model, pain is a warning sign and should be avoided. It is yet another mantra that extends beyond the pain sufferer and can include even health care practitioners. While the solution that one should just avoid exercises altogether seems sound in the acute pain setting, in the long run, progressive deconditioning would eventually make simple daily activities difficult and painful. Psychological sequelae like reduced mood and motivation can ensue – “exercises just didn’t help” and “it is painful even when I am not doing anything”.
The Truth
Exercises like jogging, resistive strength training, aerobics and ball games can leave a person with muscle pains and post exercise aches. Such aches and pain come about from building up of lactic acid during the intense muscle contractions, and microscopic tears from unaccustomed muscle exertion, especially eccentric contractions. Even for healthy, untrained individuals, blood lactate begins to accumulate and rise in an exponential fashion at about 55% of their maximal capacity for aerobic metabolism.
For a healthy, untrained person, the threshold for lactate build up occurs at a lower percentage of the aerobic metabolism, compared to that of an athlete.
When lactate accumulates, muscle and blood acidity will increase during exercise. This is especially so when a person is unaccustomed to physical activities or exercise. Over time, with a regular exercise regime, such local changes will be reduced given the same exercise intensity. Also, in response to these physical activities, pain relief can be augmented via the activation of the endogenous inhibitory system.
CHRONIC PAIN AND EXERCISEIn individuals suffering from chronic pain, this physiological process and post exercising pains get a bit more complicated. Chronic pain brings with it a certain degree of sensitisation to the peripheral and central nervous systems. High threshold mechanosensitive muscle afferent can now be activated at lower exercise intensity.1 This will further contribute to the sensitisation state. In the presence of sensitisation, symptoms can get amplified and disproportionate to the provoking action. In the course of exercising, lactic acid forms a potent sensitising chemical that can further wind up the system.
Such increase in sensitisation is worsened by the reduction in activation of the endogenous inhibitory system. When pain is localised, this effect only occurs when the painful area is being exercised. When there is a widespread myalgia, this inhibitory pathway will be poorly activated2.
When pacing is suboptimal or when the person subscribes to the mantra of “No Pain, No Gain”, this resulting the subsequent wind up effect can be great. Symptoms can worsen dramatically and post exercise pains can persist for weeks. The greater the sensitisation, the greater is the unpredictability of the symptoms.
As chronic pain sufferers are commonly deconditioned, more so in the painful areas, the delayed muscle soreness is worse. Whenever there is deconditioning, the force produced by the muscle can be reduced.3 What is considered an “average” exercise regime could expose the area to acute muscle, soft tissue strain and injuries. Presence of pain flares and acute pain from muscle strains create a pain-inhibition effect of the surrounding muscles, affecting the efficiency of muscular reconditioning.
THE WRONG PERCEPTION
THE RIGHT APPROACH
Exercising: Is it necessarily PAIN GAINNO ?
17M A R C H – M A Y 2 0 1 216 M A R C H – M A Y 2 0 1 2
GP BUZZ | FEATURE
Dr Stephen Chan
CHRONIC PELVIC PAIN
The pain started when I was sixteen. I tried to act as normally as I could, but it was difficult. I felt as if someone had poured acid on my genitals. Sitting was unbearable. Standing was not much better. And sex was out of the question. I became desperate. I wanted to cut it away,
A SILENT ENEMYUp to one in five women suffers from chronic pelvic pain at some point in her life.
As there is a wide array of possible causes of pelvic pain, the underlying cause can often be difficult to pinpoint. A typical patient sees as many as five doctors, including a family physician, gynecologist, urologist, surgeon, and psychiatrist, before finding one who believes that she has a real problem. Patients are often told that nothing is wrong with them, and many undergo extensive tests which turn out negative. Some even end up taking medication and undergoing surgery which may not be necessary.
A REAL PROBLEMDespite the lack of certainty with regards to the underlying cause,
the problem is all too real. Women with chronic pelvic pain find every aspect of their lives affected. Sitting down for even a short dinner or movie becomes an exercise in endurance. Needless to say, work is impaired. Sex is painful instead of pleasurable. And a good night of sleep becomes an unattainable dream.
“My doctors would tell me that it was all in my head. They would explain that all the tests were negative and there was no good reason why I was still feeling pain. I would leave each consultation feeling guilty and ashamed. I wanted to kill myself, because I felt so utterly useless,” Anna stated.
A lack of awareness of the causes of chronic pelvic pain can lead women to consult multiple doctors
I offered her a course of pelvic floor physiotherapy, oral muscle relaxants and antiepileptics, as well as a session with a pain psychologist. Her pain was reduced by about half. With the addition of topical local anesthetic and botox injections, she could get back to work. She is currently in a stable relationship and looking forward to marriage.
Anna suffered from pudendal neuralgia, a condition which commonly resulted from entrapment of the pudendal nerve along its course, leading to pain in the genital or anal area. Like Zoe, she had also undergone numerous failed therapies, including multiple epidural steroid injections. A thorough evaluation at our centre pointed to a likely diagnosis of pudendal neuralgia.
a pelvic physiotherapist, sex therapist, pain interested gynecologist or urologist, and pain physician will ensure that no aspect of care is overlooked.
Before you go away with the idea that chronic pelvic pain is a problem that only afflicts women, think again. Men are not spared too. One in four pudendal neuralgia patients are male. Causes of chronic pelvic pain in men include surgical conditions like hernias, urological conditions such as varicocoeles and chronic prostatitis, and other nerve entrapment syndromes such as ilioinguinal, iliohypogastric, and genitofemoral neuralgias.
However time is short as space is a premium. Thus, chronic pelvic pain in men will, perhaps, be another story for another day.
and pursue multiple treatments which may not work. It is important for both patients and doctors to be aware of the possible causes, and to keep looking for it systematically until an answer is found.
COMMON CAUSESTwo common causes of chronic pelvic pain are vulvodynia and pudendal neuralgia.
Zoe suffered from vulvodynia, a painful condition of the external genitalia. Prior to our meeting, she had just finished her third course of topical antifungals. She had also undergone numerous complementary and alternative therapies but without improvement. A detailed history and physical examination pointed to a diagnosis of provoked vestibulodynia.
She underwent a diagnostic and therapeutic ultrasound guided pudendal nerve block which provided pain relief for two months. This was followed up with a series of two more blocks, together with activity modification and a short course of antidepressant therapy. She currently experiences low levels of pain and has resumed many of the activities that she loves.
SUMMING UPEvery woman suffering from chronic pelvic pain should be able to seek medical care without embarrassment, obtain an accurate diagnosis, and receive effective treatment. A sympathetic doctor with experience dealing in chronic pelvic pain is essential. A multidisciplinary management plan involving
Up to 1 in 5 women suffers from chronic pelvic pain at some point in her life.
GP BUZZ | FEATURE
Dr Stephen Chan is a Consultant Anaesthesiologist, and Head of the Chronic and Interventional Pain Management Service in Tan Tock Seng Hospital. He divides his time between the practice of anaesthesiology and pain medicine. Dr Chan obtained his medical degree from the National University of Singapore in 2000 and completed his specialist training in Anaesthesiology in 2007. He is very interested in the diagnosis and management of chronic pelvic pain, and the use of ultrasound in regional anesthesia and pain medicine.
19M A R C H – M A Y 2 0 1 218 M A R C H – M A Y 2 0 1 2
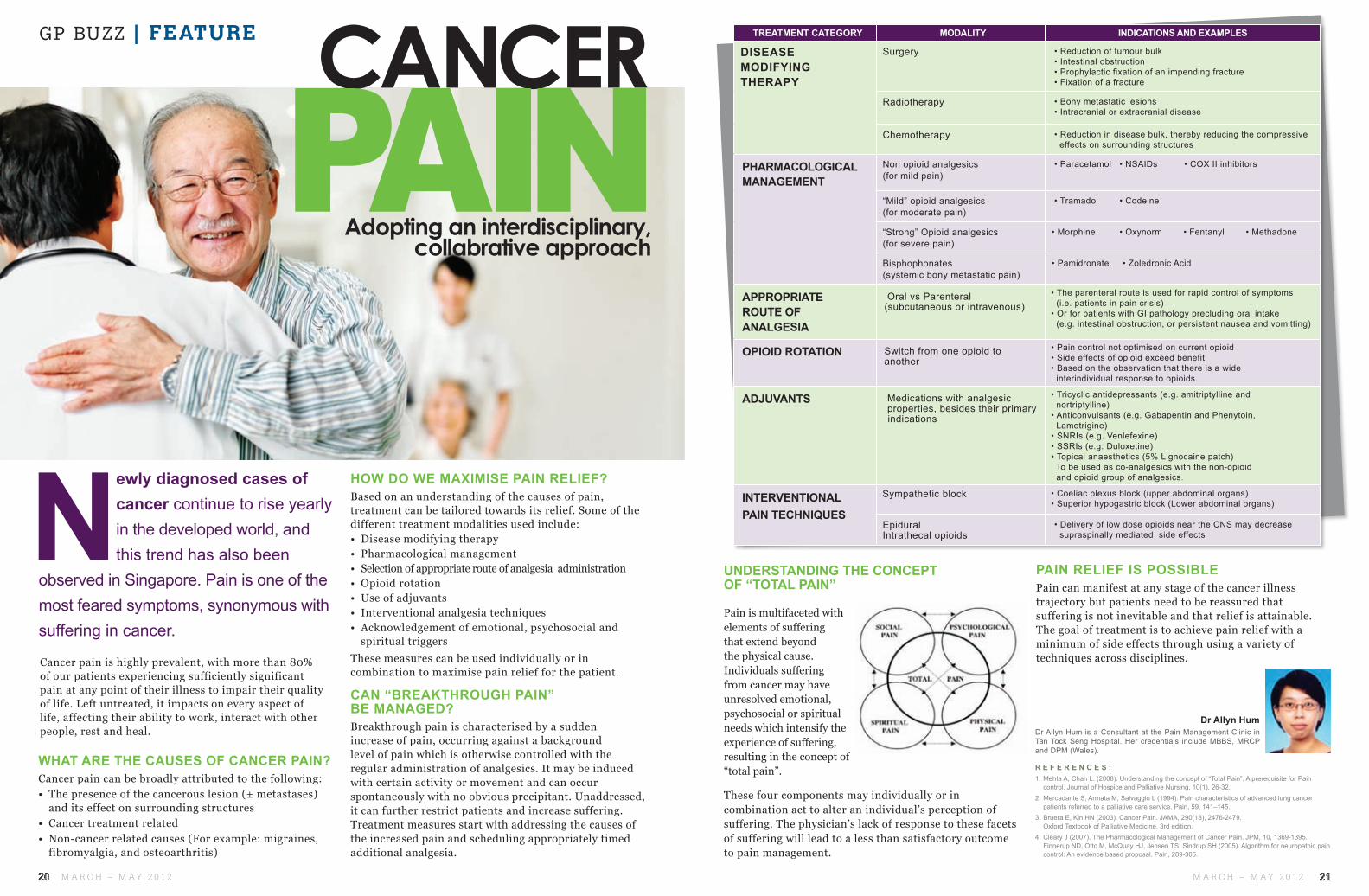
CANCER TREATMENT CATEGORY MODALITY INDICATIONS AND EXAMPLES
DISEASE MODIFYING THERAPY
Surgery • Reduction of tumour bulk • Intestinal obstruction • Prophylactic fixation of an impending fracture • Fixation of a fracture
Radiotherapy • Bony metastatic lesions • Intracranial or extracranial disease
Chemotherapy • Reduction in disease bulk, thereby reducing the compressive effects on surrounding structures
PHARMACOLOGICAL MANAGEMENT
Non opioid analgesics(for mild pain)
• Paracetamol • NSAIDs • COX II inhibitors
“Mild” opioid analgesics (for moderate pain)
• Tramadol • Codeine
“Strong” Opioid analgesics(for severe pain)
• Morphine • Oxynorm • Fentanyl • Methadone
Bisphophonates (systemic bony metastatic pain)
• Pamidronate • Zoledronic Acid
APPROPRIATE ROUTE OF ANALGESIA
Oral vs Parenteral (subcutaneous or intravenous)
• The parenteral route is used for rapid control of symptoms (i.e. patients in pain crisis) • Or for patients with GI pathology precluding oral intake (e.g. intestinal obstruction, or persistent nausea and vomitting)
OPIOID ROTATION Switch from one opioid to another
• Pain control not optimised on current opioid • Side effects of opioid exceed benefit • Based on the observation that there is a wide interindividual response to opioids.
ADJUVANTS Medications with analgesic properties, besides their primary indications
• Tricyclic antidepressants (e.g. amitriptylline and nortriptylline) • Anticonvulsants (e.g. Gabapentin and Phenytoin, Lamotrigine) • SNRIs (e.g. Venlefexine) • SSRIs (e.g. Duloxetine) • Topical anaesthetics (5% Lignocaine patch) To be used as co-analgesics with the non-opioid and opioid group of analgesics.
• Delivery of low dose opioids near the CNS may decrease supraspinally mediated side effects
WHAT ARE THE CAUSES OF CANCER PAIN? Cancer pain can be broadly attributed to the following:• The presence of the cancerous lesion (± metastases)
and its effect on surrounding structures• Cancer treatment related• Non-cancer related causes (For example: migraines,
fibromyalgia, and osteoarthritis)
Adopting an interdisciplinary,collabrative approach
R E F E R E N C E S :1. Mehta A, Chan L. (2008). Understanding the concept of “Total Pain”. A prerequisite for Pain
control. Journal of Hospice and Palliative Nursing, 10(1), 26-32.2. Mercadante S, Armata M, Salvaggio L (1994). Pain characteristics of advanced lung cancer
patients referred to a palliative care service. Pain, 59, 141–145.3. Bruera E, Kin HN (2003). Cancer Pain. JAMA, 290(18), 2476-2479.
Oxford Textbook of Palliative Medicine. 3rd edition.4. Cleary J (2007). The Pharmacological Management of Cancer Pain. JPM, 10, 1369-1395.
Finnerup ND, Otto M, McQuay HJ, Jensen TS, Sindrup SH (2005). Algorithm for neuropathic pain control: An evidence based proposal. Pain, 289-305.
Newly diagnosed cases of cancer continue to rise yearly in the developed world, and this trend has also been
observed in Singapore. Pain is one of the most feared symptoms, synonymous with suffering in cancer.
PAIN RELIEF IS POSSIBLEPain can manifest at any stage of the cancer illness trajectory but patients need to be reassured that suffering is not inevitable and that relief is attainable. The goal of treatment is to achieve pain relief with a minimum of side effects through using a variety of techniques across disciplines.
PAIN
Dr Allyn Hum is a Consultant at the Pain Management Clinic in Tan Tock Seng Hospital. Her credentials include MBBS, MRCP and DPM (Wales).
Cancer pain is highly prevalent, with more than 80% of our patients experiencing sufficiently significant pain at any point of their illness to impair their quality of life. Left untreated, it impacts on every aspect of life, affecting their ability to work, interact with other people, rest and heal.
HOW DO WE MAXIMISE PAIN RELIEF? Based on an understanding of the causes of pain, treatment can be tailored towards its relief. Some of the different treatment modalities used include:• Disease modifying therapy• Pharmacological management• Selection of appropriate route of analgesia administration• Opioid rotation• Use of adjuvants• Interventional analgesia techniques• Acknowledgement of emotional, psychosocial and spiritual triggers These measures can be used individually or in combination to maximise pain relief for the patient.
CAN “BREAKTHROUGH PAIN” BE MANAGED?Breakthrough pain is characterised by a sudden increase of pain, occurring against a background level of pain which is otherwise controlled with the regular administration of analgesics. It may be induced with certain activity or movement and can occur spontaneously with no obvious precipitant. Unaddressed, it can further restrict patients and increase suffering. Treatment measures start with addressing the causes of the increased pain and scheduling appropriately timed additional analgesia.
Dr Allyn Hum
UNDERSTANDING THE CONCEPT OF “TOTAL PAIN”
Pain is multifaceted with elements of suffering that extend beyond the physical cause. Individuals suffering from cancer may have unresolved emotional, psychosocial or spiritual needs which intensify the experience of suffering, resulting in the concept of “total pain”.
These four components may individually or in combination act to alter an individual’s perception of suffering. The physician’s lack of response to these facets of suffering will lead to a less than satisfactory outcome to pain management.
GP BUZZ | FEATURE
21M A R C H – M A Y 2 0 1 220 M A R C H – M A Y 2 0 1 2
This log is for chronic pain sufferers. The target or activities may differ for different individuals. Please consult a doctor or physical trainer before embarking on any physical activity.
REGULAR & SHORT REST BREAKS(THINK “LITTLE & OFTEN”)1REGULAR CHANGES IN POSITIONS & ACTIVITIES2GRADUAL INCREASE IN ACTIVITIES3PAIN LEVEL IS MAINTAINED AT A STEADY LEVEL4
GOAL DIRECTED5
PACING Your Way
Back To Better Health
BELOW IS AN EXAMPLE OF AN ACTIVITY LOG:
Ms Michelle Periera is a Senior Physiotherapist at the Physiotherapy Department of Tan Tock Seng Hospital with experiences in specialized clinics such as the Sports Medicine and Surgery Clinic and the Pain Management Clinic. Ms Periera is involved with the rehabilitation of patients with orthopaedic surgeries and a diverse range of musculo-skeletal injuries. She graduated from the University of Queensland, Australia with an Honours degree in Physiotherapy.
FOLLOW THESE SIMPLE STRATEGIES:
Ms Michelle Pereira
Pacing is a technique that you can use to gradually increase your level of
activity.It should be possible to pace any activity. Pacing helps to prevent any decline in activity levels when one suffers from chronic pain.
Exercise whenever possible as this will help improve physical fitness and sense of well-being. Exercise is a key component of weight management
and facilitates the body’s production of natural pain relief termed “endorphins”.
Start by choosing an activity that you want to be able to do, or are able to do for a longer period. Activities worth considering include walking, swimming, cycling and stair climbing. These activities are commonly required in our daily life and would be meaningful to start making them better. Set a starting amount of time that can be easily and comfortably achieved. Then practise that activity
regularly, or every day if possible, on good and bad days. Gradually build up the amount of time spent on the activity, but never do more than planned. Record all the information to see how much you’re improving and if you need to slow down the progression.
Pacing also involves breaking down an activity one needs to perform into tolerable chunks and taking some time out to rest. In this way you can keep track of comfort levels and how well your abilities are improving.
ACTIVITY / DAY MON TUE WED THU FRI SAT
Time taken to walk 50 metres
Number of stairs climbed in 5 minutes
Treadmill (speed / minutes / metres)
Walking (time / frequency / distance)
Swimming (time / frequency / distance)
Time taken to swim 6 laps (time / frequency / distance)
23M A R C H – M A Y 2 0 1 222 M A R C H – M A Y 2 0 1 2
GP BUZZ | FITNESS
Ingredients (Number of servings = 12 small pancakes)
2 large bananas1½ cups of wholemeal flour
3 teaspoons of baking powder
1½ cups of buttermilk
2 eggs, lightly beaten
1 tablespoon of honey Olive oil cooking spray
Low fat yogurt and extra fruits, to serve
Each serving provides 97kcal,
15g carbohydrates, 4g protein,
2g total fat, 0.8g saturated fat,
2.2g fiber and 92 mg sodium.
WHOLEMEAL
BANANA PANCAKES
MANGO SALSA
(Number of servings = 2)
1 cup fresh mango (diced)1/3 cup red onion (diced)1 large tomato (diced)2/3 cup roasted red peppers (diced)1 small red chilli (minced)2 tablespoons fresh mint (chopped)1 tablespoon fresh lime juice
MethodsCombine all ingredients and chill.
Serve with grilled fish or chicken.
Each serve provides 90cal, 4g protein,
17g carbohydrates, 1g total fat, 0.1g
saturated fat, 2.2g dietary fiber and
23mg sodium. Each serve provides
one serving of fruit and one serving of
vegetables.
Use wholemeal flour in this recipe and you get 3.4 times more fiber in your diet than white flour.
are not only naturally low in calories & fat, they are ‘POWERHOUSE’ of fibre, vitamins & antioxidants which are essential for good health.
Tips to increase
Ways to increase intake of fruits and vegetables:• Ask for more vegetables at lunch and dinner
• Add some fruits into your cereal or oats at breakfast
• Snack on fruit in between meals • Choose salad to accompany your main meal• End your meal with a piece
of fruit or fruit-based dessert
Fruits & Vegetables
• Choose brown rice over white rice whenever possible
• Enjoy oats or wholegrain cereals during breakfast
• Choose wholemeal or wholegrain sandwiches
• Substitute white noodles with whole wheat or brown rice noodles
• Use wholemeal flour when making baked products
Methods1. Mash 1 banana in a bowl. Place
flour in a bowl. Make a well in the centre.
2. Combine buttermilk, eggs, honey and mashed banana in a jug.
3. Pour into well. Whisk until smooth. Stand for 10 minutes. Spray a large, non-stick frying pan with oil. Heat over medium heat.
4. Spoon 1/4 cup batter into pan. Cook for 2 to 3 minutes or until bubbles appear on the surface. Turn. Cook for 1 to 2 minutes or until golden and cooked through.
5. Slice thinly the remaining banana. Top with sliced banana, and low fat yoghurt.
Wholegrain intake
Recipes contributed by Department of Nutrition and Dietetics, Tan Tock Seng Hospital
Ingredients
GP BUZZ | HEALTHY RECIPES
Gastroenterology and HepatologyOur sub-specialties include:• GeneralGastroenterology
• Hepatology(Liver)Service
• InflammatoryBowelDisease(IBD)
• GastrointestinalEndoscopy
• Pancreato-BiliaryDiseases
• UpperGastrointestinalMotility
• Nutrition
TTSH PEARL’s suite of clinics and services is guided by the four pillars of care through Evidence Care, Destination Care, Team Care and Personalised Care. We remain committed to delivering a higher level of patient care as we value our patients most.