Page 1
9/18/16
1
GreaterCincinna+AcuteStroke:AttheCu(ngEdge
PoojaKhatri,MD,MScProfessorofNeurology
DirectorofAcuteStrokeResearchUniversityofCincinnaD
RelevantIndustryDisclosure
• TheUCDeptofNeurologyreceivesfundsfromGenentechformyeffortasLeadPIofthePRISMSTrial
TheLast50Years
• 1958:FirstIVthrombolysis
• 1974:ClinicalCTscans • 1983:Firstendovascularthrombolysis • 1995:IVrtPA • 1999:IApro-urokinase
• 2015:EndovascularTherapy
Page 2
9/18/16
2
Pilot NINDS Trials
NINDSStudy
• Double-blinded• Placebocontrolled• NIH-sponsored• 0.9mg/kgIVt-PA• 624paDents• Treatmentwithin3hrs
– 1/2within90minutes– 1/2within91-180minutes
• SubsequentIST3trialshowedefficacyoutto4.5hours
UCStrokeTeamCoverage• 16localhospitalsin-person
– EMSbringsptstonearesthospital– StrokeMDdrivestoalllocalhospitals– Encouragepre-noDficaDon(priortoCT)– Coordinatorgoesifpossibletrialcandidate– StarDngtelemedicineatsomeofthese
• 8regionalhospitalstelemedicineonly– Assessmentbytelemedicine– Drip/shiptoUCMCforpost-tPAcare
• Addi+onal~8regionalhospitals– Assessmentbyphone– Drip/shiptoUCMCforpost-tPAcare
• ~3000consultaDoncallsin2015– ~350treatmentsin2015– ~100treatmentsin2004
Page 3
9/18/16
3
IV Thrombolysis
Kleindorfer,Stroke2004,Adeoye,Stroke2011
IV Thrombolysis
JCAHOStrokeCtrs
IVrtPADRGbyCMS
Kleindorfer,Stroke2004,Adeoye,Stroke2011
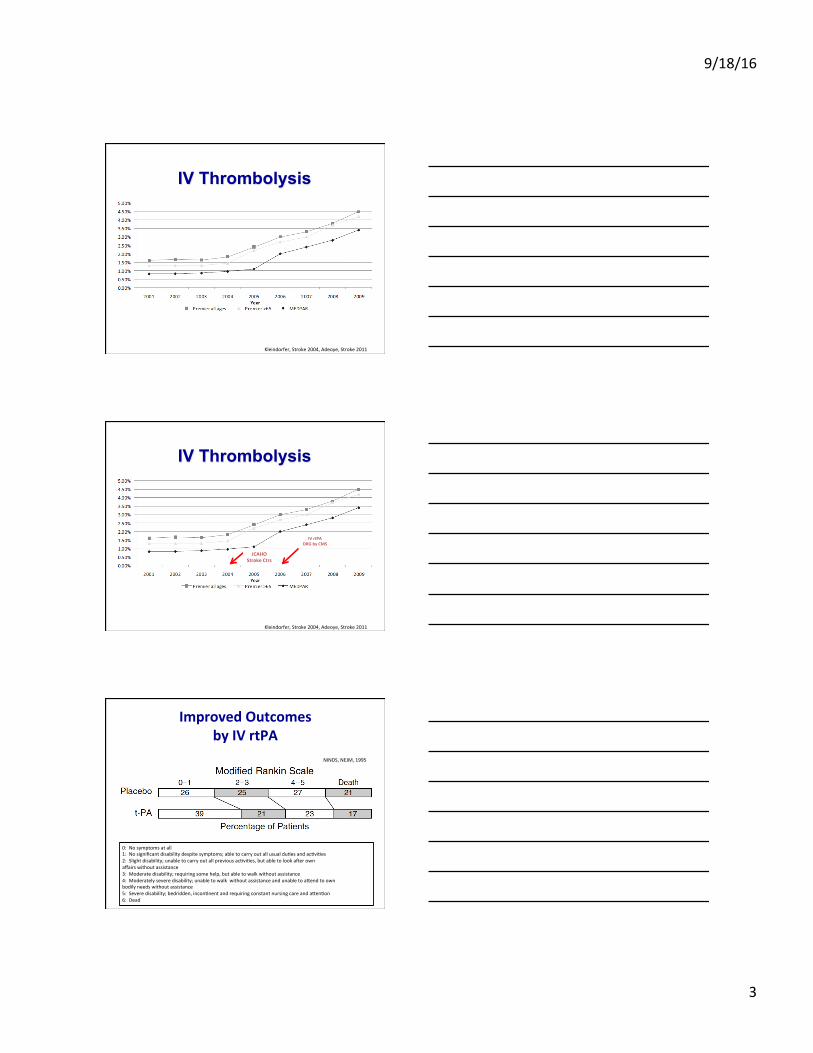
ImprovedOutcomesbyIVrtPA
0:Nosymptomsatall1:Nosignificantdisabilitydespitesymptoms;abletocarryoutallusualduDesandacDviDes2:Slightdisability;unabletocarryoutallpreviousacDviDes,butabletolookacerownaffairswithoutassistance3:Moderatedisability;requiringsomehelp,butabletowalkwithoutassistance4:Moderatelyseveredisability;unabletowalkwithoutassistanceandunabletoadendtoownbodilyneedswithoutassistance5:Severedisability;bedridden,inconDnentandrequiringconstantnursingcareandadenDon6:Dead
NINDS,NEJM,1995
Page 4
9/18/16
4
ImprovedOutcomesbyIVrtPA
0:Nosymptomsatall1:Nosignificantdisabilitydespitesymptoms;abletocarryoutallusualduDesandacDviDes2:Slightdisability;unabletocarryoutallpreviousacDviDes,butabletolookacerownaffairswithoutassistance3:Moderatedisability;requiringsomehelp,butabletowalkwithoutassistance4:Moderatelyseveredisability;unabletowalkwithoutassistanceandunabletoadendtoownbodilyneedswithoutassistance5:Severedisability;bedridden,inconDnentandrequiringconstantnursingcareandadenDon6:Dead
61%
NINDS,NEJM,1995
Intra-ArterialDrugDelivery
IllustraDonbyChristafordis,AJNR,2012
PROACTII(1996-1998)
• SponsoredbyAbbodLaboratories,Inc.• R-pro-urokinase+heparinvsheparinalone• PosiDvetrial(n=180)
– mRS0-1of40%(ly+c)vs25%(p=0.04)• FDAwanted2ndtrial;r-pro-UKnolongeravailable
Furlan,JAMA,1999
Page 5
9/18/16
5
MERCIRetriever:FDA-ClearedonAugust11,2004
• Single-armtrial(n=151)• Treatmentstartedwithin8hours• RecanalizaDonin46%(ITT)• Devicescanalsoopenuparteries(FDAClearance)
Smith,Stroke,2005
MoreEffec+veDevices
2004
2007
2009
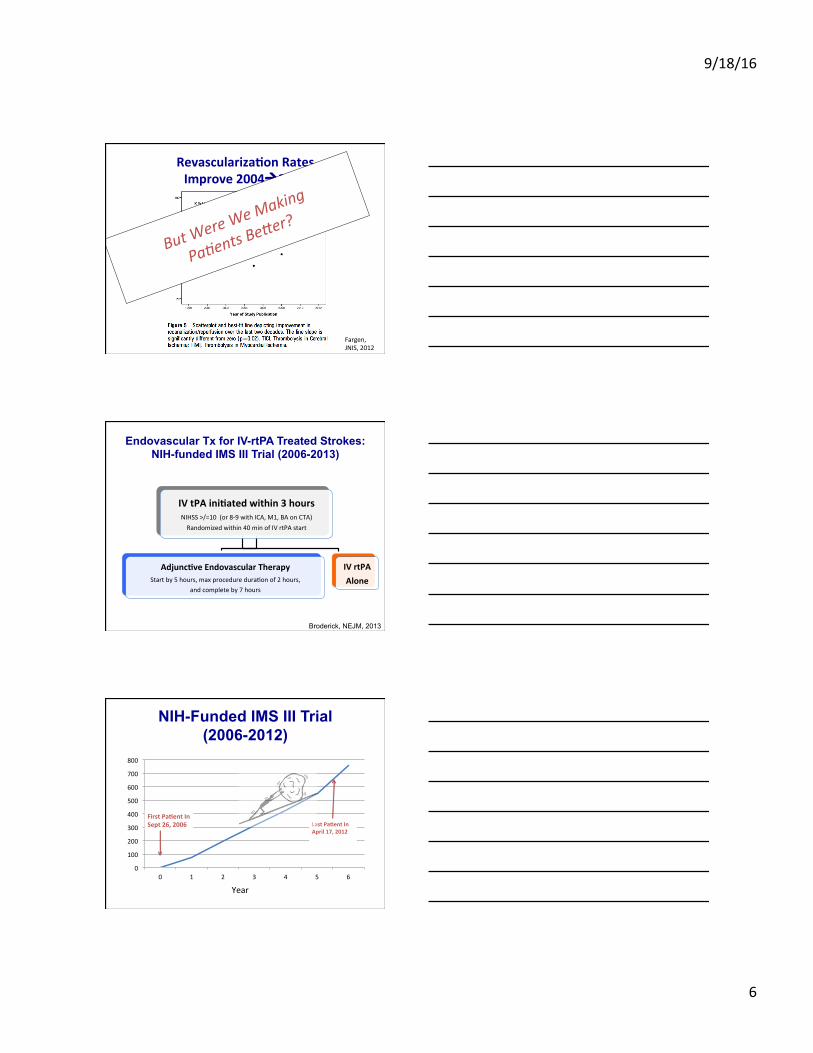
Revasculariza+onRatesImprove2004à2012
Fargen,JNIS,2012
Page 6
9/18/16
6
Revasculariza+onRatesImprove2004à2012
Fargen,JNIS,2012
ButWereW
eMaking
Pa/entsB
e1er?
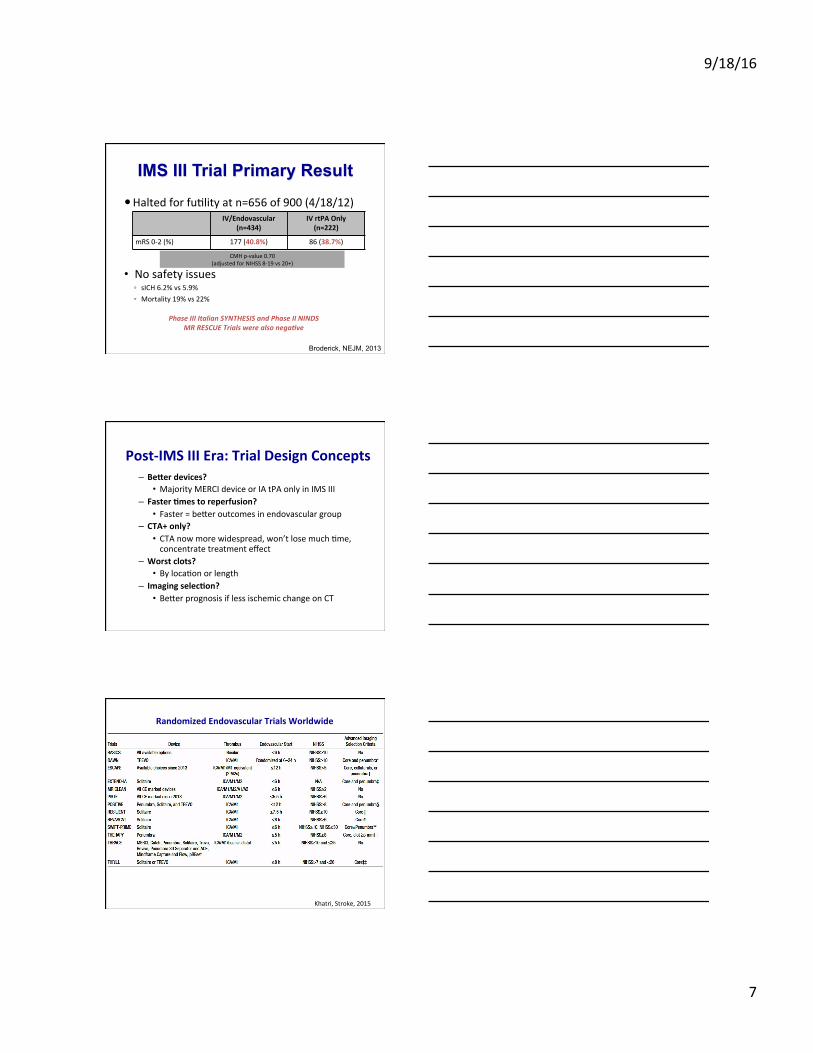
Endovascular Tx for IV-rtPA Treated Strokes: NIH-funded IMS III Trial (2006-2013)
IVtPAini+atedwithin3hoursNIHSS>/=10(or8-9withICA,M1,BAonCTA)Randomizedwithin40minofIVrtPAstart
Adjunc+veEndovascularTherapyStartby5hours,maxprocedureduraDonof2hours,
andcompleteby7hours
IVrtPAAlone
Broderick, NEJM, 2013
NIH-Funded IMS III Trial (2006-2012)
0
100
200
300
400
500
600
700
800
0 1 2 3 4 5 6
LastPa+entInApril17,2012
Year
FirstPa+entInSept26,2006
Page 7
9/18/16
7
IMS III Trial Primary Result
� HaltedforfuDlityatn=656of900(4/18/12)
• Nosafetyissues◦ sICH6.2%vs5.9%◦ Mortality19%vs22%
IV/Endovascular(n=434)
IVrtPAOnly(n=222)
mRS0-2(%) 177(40.8%) 86(38.7%)
CMHp-value0.70(adjustedforNIHSS8-19vs20+)
Broderick, NEJM, 2013
PhaseIIIItalianSYNTHESISandPhaseIININDSMRRESCUETrialswerealsonega?ve
Post-IMSIIIEra:TrialDesignConcepts
– Bederdevices?• MajorityMERCIdeviceorIAtPAonlyinIMSIII
– Faster+mestoreperfusion?• Faster=bederoutcomesinendovasculargroup
– CTA+only?• CTAnowmorewidespread,won’tlosemuchDme,concentratetreatmenteffect
– Worstclots?• BylocaDonorlength
– Imagingselec+on?• BederprognosisiflessischemicchangeonCT
RandomizedEndovascularTrialsWorldwide
Khatri,Stroke,2015
Page 8
9/18/16
8
DutchMRCLEAN–POSITIVERESULTS October22nd,2014
WorldStrokeCongressIstanbul,Turkey
CANADIANESCAPE&AUSTRALIANEXTEND-IATRIALSANNOUNCEDINTERIMANALYSESOFOVERWHELMINGEFFICACY
November7th,2014PICommunica+ons
HereWeAre:June,2015
TRIAL Enrolled Planned Results
MRCLEAN 500 500 NEJM12/17/14
ESCAPE 316 599 NEJM2/11/15
EXTENDIA 70 100 NEJM2/11/15
SWIFTPRIME 196 833 NEJM4/17/15
REVASCAT 206 690 NEJM4/17/15
THERAPY 108 692 ESOC4/2015
THRACE 412 480 ESOC4/2015
Page 9
9/18/16
9
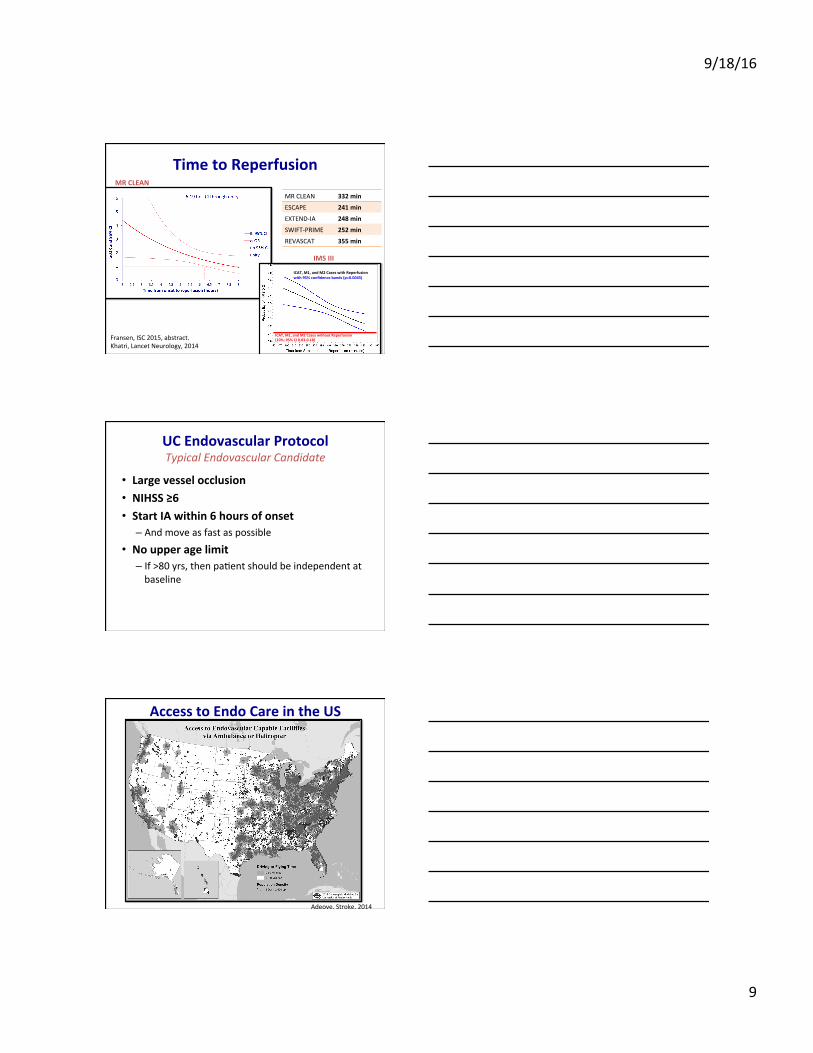
TimetoReperfusionMRCLEAN
ICAT,M1,andM2CaseswithoutReperfusion(10%;95%CI0.03-0.18)
ICAT,M1,andM2CaseswithReperfusionwith95%confidencebands(p=0.0045)
IMSIII
Fransen,ISC2015,abstract.Khatri,LancetNeurology,2014
MRCLEAN 332min
ESCAPE 241min
EXTEND-IA 248min
SWIFT-PRIME 252min
REVASCAT 355min
UCEndovascularProtocolTypicalEndovascularCandidate
• Largevesselocclusion• NIHSS≥6• StartIAwithin6hoursofonset
– Andmoveasfastaspossible
• Noupperagelimit– If>80yrs,thenpaDentshouldbeindependentatbaseline
AccesstoEndoCareintheUS
Adeoye,Stroke,2014
Page 10
9/18/16
10
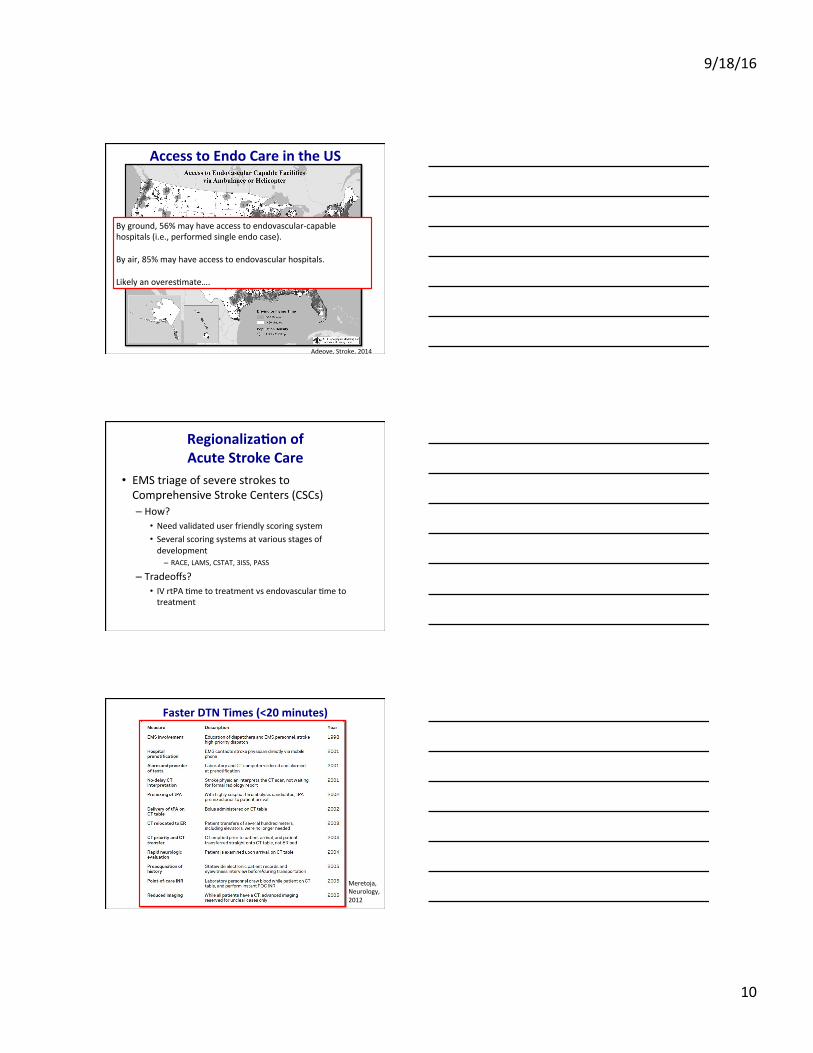
AccesstoEndoCareintheUS
Adeoye,Stroke,2014
Byground,56%mayhaveaccesstoendovascular-capablehospitals(i.e.,performedsingleendocase).Byair,85%mayhaveaccesstoendovascularhospitals.LikelyanoveresDmate….
Regionaliza+onofAcuteStrokeCare
• EMStriageofseverestrokestoComprehensiveStrokeCenters(CSCs)– How?
• Needvalidateduserfriendlyscoringsystem• Severalscoringsystemsatvariousstagesofdevelopment
– RACE,LAMS,CSTAT,3ISS,PASS
– Tradeoffs?• IVrtPADmetotreatmentvsendovascularDmetotreatment
FasterDTNTimes(<20minutes)
Meretoja,Neurology,2012
Page 11
9/18/16
11
CURRENTANDUPCOMINGCLINICALTRIALSINCINCINNATI
TheCurrentCutngEdge
Selec+ngPa+entsforLaterTreatmentUsingPenumbralImaging?
Kidwell,Stroke,2013
DEFUSE3Trial
• NIH-funded,Phase3trial//Thisisanewtrial!– NIHSS6+,largevesselocclusiononCTA– 6-16hoursfromlastknownwell– TesDngendovasculartxvsstandardmedmgmtinpaDentswithpenumbraonstudy-specificCTP
• LocalPIsAchalaVagalandAndyRinger;Coordinator:CindyWerner
Page 12
9/18/16
12
NIHStrokeNET• UniversityofCincinnaDhousesthenaDonalclinicalcoordinatorcenter(NCC)forallmulDcentertrialsfundedbyNIH– PI:Broderick,Co-PIs:Khatri,Chimowitz,Cramer;ProgramManagers:Spilker,Frasure
• AlsoleadstheregionalcoordinaDoncenter(RCC)forbringingNIH-fundedtrialstothemetropolitanregion– PIs:Khatri,Kleindorfer;ProgramMgr:EmilyGoodall
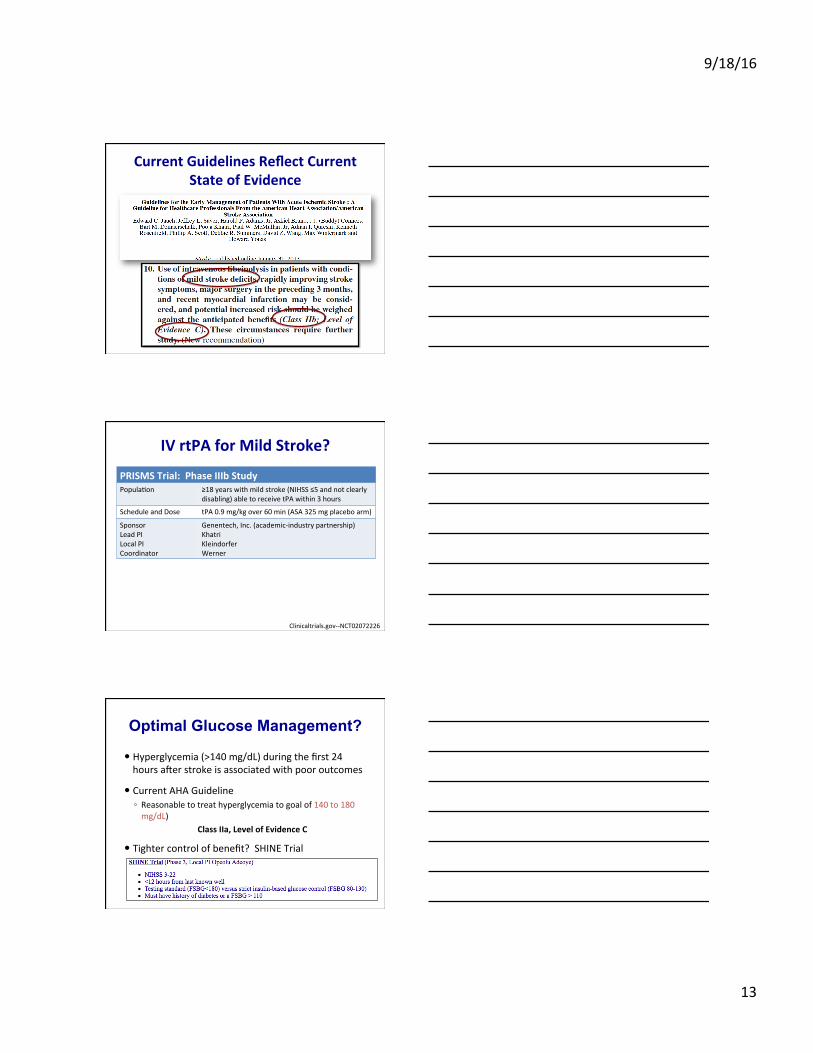
NINDSStudyBaselineNIHSSvsFavorableOutcome
0
20
40
60
80
100
0-5 6-10 11-15 16-20 >20
Percen
tfavorab
leoutcome
BaselineNIHSS
t-PA
Placebo
Ingall,Stroke,2004
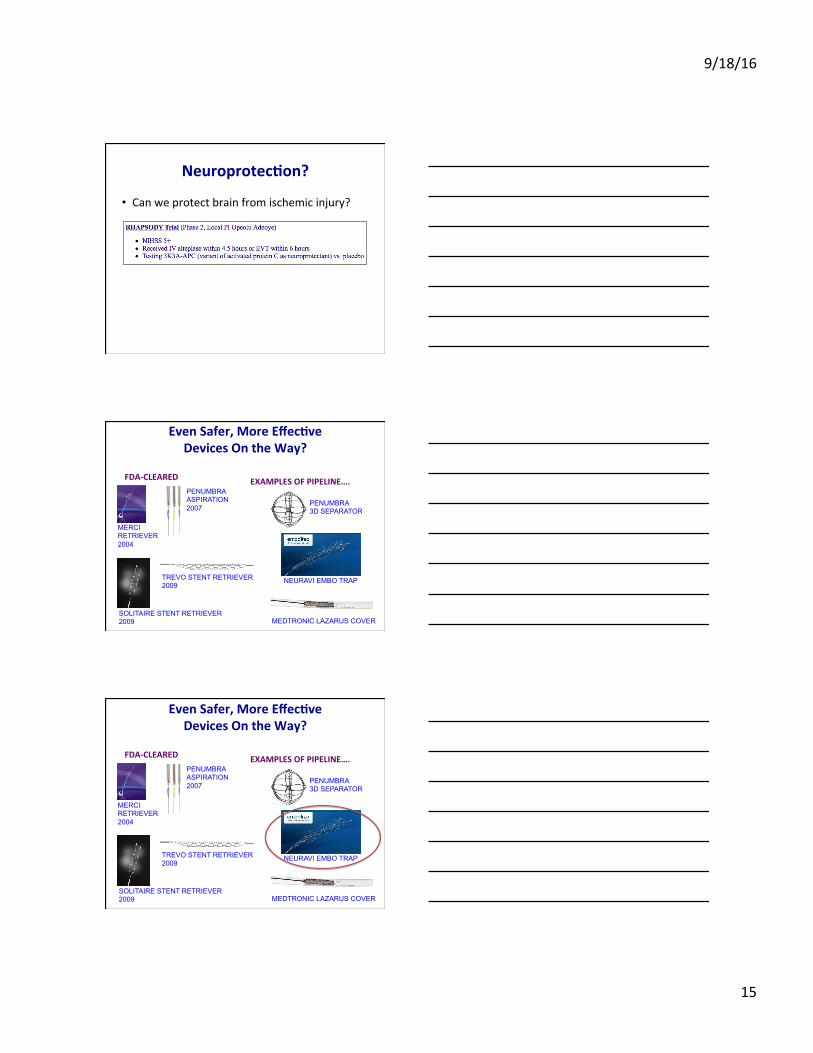
NINDSStudyBaselineNIHSSvsFavorableOutcome
0
20
40
60
80
100
0-5 6-10 11-15 16-20 >20
Percen
tfavorab
leoutcome
BaselineNIHSS
t-PA
Placebo
n=5816placebo,81.3%goodoutcome(95%C.I.54-96%)42IVrtPA78.6%goodoutcome(95%C.I.63-90%)
Nointerac/onbystrokeseveritybutmildstrokeswerelargelyexcluded
Ingall,Stroke,2004
Page 13
9/18/16
13
CurrentGuidelinesReflectCurrentStateofEvidence
IVrtPAforMildStroke?
Clinicaltrials.gov--NCT02072226
PRISMSTrial:PhaseIIIbStudyPopulaDon ≥18yearswithmildstroke(NIHSS≤5andnotclearly
disabling)abletoreceivetPAwithin3hours
ScheduleandDose tPA0.9mg/kgover60min(ASA325mgplaceboarm)
SponsorLeadPILocalPICoordinator
Genentech,Inc.(academic-industrypartnership)KhatriKleindorferWerner
Optimal Glucose Management?
� Hyperglycemia(>140mg/dL)duringthefirst24hoursacerstrokeisassociatedwithpooroutcomes
� CurrentAHAGuideline◦ Reasonabletotreathyperglycemiatogoalof140to180mg/dL)
ClassIIa,LevelofEvidenceC
� Tightercontrolofbenefit?SHINETrial
Page 14
9/18/16
14
Optimal Antiplatelet Therapy?
� AllpaDentsshouldbestartedonaspirin(325mg)within48hours◦ Youwillprevent1recurrentstrokeoverthetwoweeksaceracuteischemicstrokeforevery100paDentsyoutreat(CAST,IST)
AHAClassI,LevelofEvidenceA
� EarlyASAandclopidogrelinTIA/mildstroke?
MoreEfficaciousIVThrombolysis?
• PriorstudiescombiningeptafibaDdeandrtPA:– CLEAR– CLEAR-ER– CLEARFDR
• Trialindevelopment– MOSTTrial(LeadPI:Adeoye)
EvenSafer,MoreEffec+veDevicesOntheWay?
FDA-CLEARED EXAMPLESOFPIPELINE….
MERCI RETRIEVER 2004
PENUMBRA ASPIRATION 2007
SOLITAIRE STENT RETRIEVER 2009
TREVO STENT RETRIEVER 2009
PENUMBRA 3D SEPARATOR
NEURAVI EMBO TRAP
MEDTRONIC LAZARUS COVER
Page 15
9/18/16
15
Neuroprotec+on?
• Canweprotectbrainfromischemicinjury?
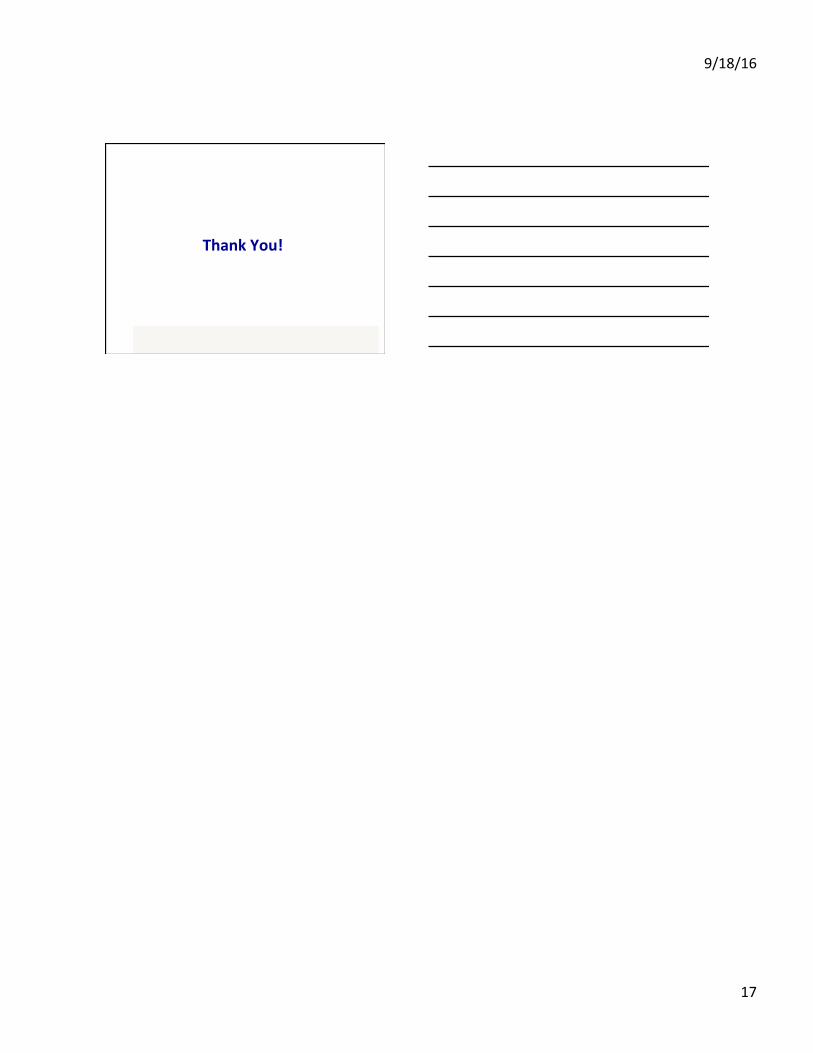
EvenSafer,MoreEffec+veDevicesOntheWay?
FDA-CLEARED EXAMPLESOFPIPELINE….
MERCI RETRIEVER 2004
PENUMBRA ASPIRATION 2007
SOLITAIRE STENT RETRIEVER 2009
TREVO STENT RETRIEVER 2009
PENUMBRA 3D SEPARATOR
NEURAVI EMBO TRAP
MEDTRONIC LAZARUS COVER
EvenSafer,MoreEffec+veDevicesOntheWay?
FDA-CLEARED EXAMPLESOFPIPELINE….
MERCI RETRIEVER 2004
PENUMBRA ASPIRATION 2007
SOLITAIRE STENT RETRIEVER 2009
TREVO STENT RETRIEVER 2009
PENUMBRA 3D SEPARATOR
NEURAVI EMBO TRAP
MEDTRONIC LAZARUS COVER
Page 16
9/18/16
16
PreventMalignantEdema?
Conclusions
• TheCincinnaDregionhasplayedacriDcalroleinthedevelopmentofcurrentacutestroketherapies– IVrtPAwithin4.5hoursoflastknownwell– Endovasculartherapywithin6hoursoflastknownwell
• TheregionconDnuestodevelopnewtherapiesthroughclinicaltrials– DEFUSE-3,StrokeNET,PRISMS,SHINE,POINT,RHAPSODYongoing
Reminder:WhentoCallStrokeTeam
• Callstroketeamforallstrokes<12hoursfromDmethatpaDentwas“lastknownwell”
• CallusforallTIAsandstrokes,nomaderhowmildthedeficitsmayseem
• Preno+fyusbeforegetngtheCT/CTAscanresults
513-844-7686
Page 17
9/18/16
17
ThankYou!