J. Malcolm O. Arnold, MD,cc Gordon W. Moe, MD, MSc,dd Jonathan G. Howlett, MD,ee
Jean-Martin Boulanger, MD,ff Pierre Larochelle, MD,gg Lawrence A. Leiter, MD,hh
Charlotte Jones, MD, PhD,ii Richard I. Ogilvie, MD,jj Vincent Woo, MD,kk Janusz Kaczorowski, PhD,ll
Luc Trudeau, MD,mm Simon L. Bacon, PhD,nn Robert J. Petrella, MD, PhD,oo Alain Milot, MD, MSc,pp
James A. Stone, MD, PhD,qq Denis Drouin, MD,rr Maxime Lamarre-Cliché, MD,ss
Marshall Godwin, MD, MSc,tt Guy Tremblay, MD,uu Pavel Hamet, MD, PhD,vv
George Fodor, MD, PhD,ww S. George Carruthers, MD,xx George Pylypchuk, MD,yy Ellen Burgess, MD,c
Richard Lewanczuk, MD,zz George K. Dresser, MD, PhD,aaa Brian Penner, MD,bbb
Robert A. Hegele, MD,ccc Philip A. McFarlane, MD, PhD,ddd Mukul Sharma, MD, MSc,eee
Norman R.C. Campbell, MD,fff Debra Reid, PhD, RD,ggg Luc Poirier, BPharm, MSc,hhh and
Sheldon W. Tobe, MD;iii for the Canadian Hypertension Education Program
Received for publication February 11, 2012. Accepted February 24, 2012.
Corresponding author: Dr Stella S. Daskalopoulou, McGill University,McGill University Health Centre, Montreal General Hospital, 1650 CedarAvenue, B2.101.4, Montreal, Québec H3G 1A4, Canada. Tel.: !514-934-1934 "42295; fax: !514-934-8564.
A version of the hypertension recommendations designed for patientand public education has been developed to assist health care practitionersmanaging hypertension. The summary is available electronically (go tohttp://www.hypertension.ca or http://www.heartandstroke.ca).
a Division of General Internal Medicine, McGill University, Montreal, Québec, Canada;b Division of General Internal Medicine, University ofBritish Columbia, Vancouver, British Columbia, Canada; c Division of Nephrology, University of Calgary, Calgary, Alberta, Canada; d Division
of Nephrology, University of Ottawa, Ottawa, Ontario, Canada; e Faculty of Medicine, Memorial University of Newfoundland, St John’s,Newfoundland and Labrador, Canada; f Department of Medicine and Endocrinology, University of Western Ontario, London, Ontario,Canada; g Division of Cardiology, University of British Columbia, Vancouver, British Columbia, Canada; h Departments of Medicine,
Community Health and Cardiac Sciences, University of Calgary, Calgary, Alberta, Canada; i St Michael’s Hospital, University of Toronto,Toronto, Ontario, Canada; j Division of General Internal Medicine, University of Alberta, Edmonton, Alberta, Canada; k Department of
Family Medicine, University of British Columbia, Vancouver, British Columbia, Canada; l Ottawa Hospital Research Institute, University ofOttawa, Ottawa, Ontario, Canada; m Department of Psychology, University of Calgary, Calgary, Alberta, Canada; n Department of Nursing,Université du Québec à Trois-Rivières, Québec, Canada; o Division of Clinical Epidemiology, Montreal General Hospital, Montreal, Québec,Canada; p Division of Cardiology, Sir Mortimer B. Davis-Jewish General Hospital, Montreal, Québec, Canada; q Department of Medicine,
University of Calgary, Calgary, Alberta, Canada; r Department of Medicine, Sir Mortimer B. Davis-Jewish General Hospital, McGillUniversity, Montreal, Québec, Canada; s Ambulatory Internal Medicine Teaching Clinic, St Catharines, Ontario, Canada; t Department of
Medicine, University of Saskatchewan, Saskatoon, Saskatchewan; Canada; u Department of Medicine, University of Western Ontario, London,Ontario, Canada; v Canadian Stroke Network, Toronto, Ontario, Canada; w Departments of Clinical Neurosciences, Medicine and
Community Health Sciences, University of Calgary, Calgary, Alberta, Canada; x Vancouver, British Columbia, Canada; y Division ofNephrology, Hôpital Maisonneuve-Rosemont, Université de Montréal, Montreal, Québec, Canada; z Division of Nephrology, University ofToronto, Toronto, Ontario, Canada; aa CHUQ, L’Hôtel-Dieu de Québec, Department of Medicine, l’Université Laval, Québec, Québec,
Canada; bb Faculty of Nursing, University of Alberta, Edmonton, Alberta, Canada; cc London Health Sciences Centre, University of WesternOntario, London, Ontario, Canada; dd University Health Network, University of Toronto, Toronto, Ontario, Canada; ee Queen Elizabeth IIHealth Sciences Centre, Halifax, Nova Scotia, Canada; ff Charles LeMoyne Hospital Research Centre, University of Sherbrooke, Sherbrooke,
Québec, Canada; gg Institut de recherché Clinique de Montréal, Montréal, Québec, Canada; hh Division of Endocrinology and Metabolism andKeenan Research Centre at the Li Ka Shing Knowledge Institute, St Michael’s Hospital, Toronto, Ontario, Canada; ii Division of
Endocrinology, Department of Medicine, University of Calgary, Calgary, Alberta, Canada; jj University Health Network, University ofToronto, Toronto, Ontario, Canada; kk Division of Endocrinology & Metabolism, University of Manitoba, Winnipeg, Manitoba, Canada;
ll Département de médecine familiale et médecine d’urgence, Université de Montréal, Montréal, Québec, Canada; mm Department of Medicine,McGill University, Montréal, Québec, Canada; nn Department of Exercise Science, Concordia University, Montréal, Québec, Canada;
oo Lawson Health Research Institute, University of Western Ontario, London, Ontario, Canada; pp Department of Medicine, Universite Laval,Québec, Québec, Canada; qq Division of Cardiology, Department of Medicine, University of Calgary, Calgary, Alberta, Canada; rr Department ofFamily Medicine, Université Laval, Québec, Québec, Canada; ss Institut de recherché Clinique de Montréal, Montréal, Québec, Canada;
tt Primary Healthcare Research Unit, Memorial University of Newfoundland, St John’s, Newfoundland and Labrador, Canada; uu UniversitéLaval, Direction de la Santé publique !03, Québec, Québec, Canada; vv Faculté de Médicine, Université de Montréal, Montréal, Québec,Canada; ww Prevention and Rehabilitation Centre, University of Ottawa Heart Institute, Ottawa, Ontario, Canada; xx Lisburn, Northern
Ireland; yy Division of Nephrology, St Paul’s Hospital, University of Saskatchewan, Saskatoon, Saskatchewan, Canada; zz University of Alberta,Edmonton, Alberta, Canada; aaa Department of Medicine, University of Western Ontario, London, Ontario, Canada; bbb Department of
Pharmacology and Therapeutics, University of Manitoba, Winnipeg, Manitoba, Canada; ccc Schulich School of Medicine and Dentistry,University of Western Ontario, London, Ontario, Canada; ddd Division of Nephrology, St Michael’s Hospital, University of Toronto, Toronto,
Ontario, Canada; eee The Canadian Stroke Network, The Ottawa Hospital, Ottawa, Ontario, Canada; fff Departments of Medicine,Community Health Sciences, and Pharmacology and Therapeutics, University of Calgary, Calgary, Alberta, Canada; ggg Canadian ForcesHealth Services Group, Department of National Defence, Ottawa, Ontario, Canada; hhh Hypertension Unit and Pharmacy Department,
CHUQ, Québec, Québec, Canada; iii Division of Nephrology, University of Toronto, Toronto, Ontario, Canada
ABSTRACTWe updated the evidence-based recommendations for the diagnosis,assessment, prevention, and treatment of hypertension in adults for2012. The new recommendations are: (1) use of home blood pressuremonitoring to confirm a diagnosis of white coat syndrome; (2) miner-alocorticoid receptor antagonists may be used in selected patientswith hypertension and systolic heart failure; (3) a history of atrialfibrillation in patients with hypertension should not be a factor indeciding to prescribe an angiotensin-receptor blocker for the treat-ment of hypertension; and (4) the blood pressure target for patientswith nondiabetic chronic kidney disease has now been changed to "140/90 mm Hg from " 130/80 mm Hg. We also reviewed the recentevidence on blood pressure targets for patients with hypertension anddiabetes and continue to recommend a blood pressure target of lessthan 130/80 mm Hg.
RÉSUMÉNous avons mis à jour les recommandations factuelles en ce qui a traitau diagnostic, à l’évaluation, à la prévention et au traitement del’hypertension chez les adultes pour 2012. Les nouvelles recomman-dations sont : 1) l’utilisation de la mesure de la pression artérielle àdomicile pour confirmer un diagnostic de « syndrome de la blouseblanche »; 2) les antagonistes du récepteur minéralocorticoïde peu-vent être utilisés chez des patients ayant de l’hypertension et uneinsuffisance cardiaque systolique; 3) un antécédent de fibrillation au-riculaire chez les patients ayant de l’hypertension ne devrait pas êtreun facteur de décision pour prescrire un inhibiteur du récepteur del’angiotensine dans le traitement de l’hypertension; 4) la pressionartérielle cible des patients non diabétiques ayant une maladie rénalechronique est maintenant de " 140/90 mm Hg au lieu de " 130/90mm Hg. Nous avons aussi revu les données récentes sur la pressionartérielle cible des patients ayant de l’hypertension et un diabète, etnous continuons de recommander une pression artérielle cible demoins de 130/80 mm Hg.
Daskalopoulou et al.2012 Canadian Recommendations for High BP
271
Executive SummaryObjective: To update the evidence-based recommenda-
tions for the prevention, diagnosis, assessment, and treatmentof hypertension in adults for 2012.
Options and Outcomes: For lifestyle and pharmacologic in-terventions, randomized trials and systematic reviews of trials werepreferentially reviewed. Changes in cardiovascular morbidity andmortality, as well as total mortality were the primary outcomes ofinterest. However, for lifestyle interventions, blood pressure low-ering was accepted as a primary outcome, and progressive renalimpairment was also accepted as a clinically relevant primary out-come among patients with chronic kidney disease.
Evidence: A Cochrane Collaboration librarian conducted anindependent MEDLINE search up to August 2011 to update the2011 recommendations. To identify additional studies, referencelists were reviewed and experts were contacted. All relevant articleswere reviewed and appraised independently by both content andmethodology experts using prespecified levels of evidence.
Recommendations
Diagnosis and assessment
A new recommendation this year relates to the diagnosis ofwhite coat hypertension, which could be confirmed either byreliable repeated home blood pressure (BP) monitoring or 24-hour ambulatory BP monitoring (ABPM). Recommendationsfor BP measurement, criteria for hypertension diagnosis andfollow-up, assessment of global cardiovascular risk, diagnostictesting, diagnosis of renovascular and endocrine causes of hy-pertension, ambulatory monitoring, and the use of echocardi-ography in hypertensive individuals are unchanged.
Prevention and treatment
New recommendations include: (1) aldosterone antagonistsare recommended for hypertension and systolic heart failure inaddition to the suggested therapy; (2) a history of atrial fibril-lation (AF) in patients with hypertension should not be a factorin deciding to prescribe an angiotensin-receptor blocker (ARB)for the treatment of hypertension; (3) from a rereview of theevidence, BP targets for patients with nondiabetic chronic kid-ney disease (CKD) is now ! 140/90 mm Hg instead of !130/80 mm Hg; (4) The BP target for patients with hyperten-sion and diabetes mellitus did not change ( ! 130/80 mm Hg)based on evaluation of recent meta-analyses. Recommenda-tions on lifestyle modifications to prevent and treat hyperten-sion, indications for pharmacologic management of hyperten-sion, treatment thresholds and targets, choice of therapy foradults with hypertension and without compelling indicationsfor other agents, isolated systolic hypertension, cerebrovasculardisease, proteinuric nondiabetic CKD, ischemic heart disease,left ventricular hypertrophy, diabetes, and global vascular pro-tection have not changed. Treatment for pheochromocytoma,primary hyperaldosteronism, and strategies to improve antihy-pertensive medication adherence are unchanged.
Validation
All recommendations were graded according to the strengthof the evidence and voted on by the 65 members of the Cana-dian Hypertension Education Program (CHEP) Recommen-dations Task Force. All recommendations reported herein
achieved at least 80% consensus. CHEP will continue to up-date recommendations annually. All recommendations areoutlined in this document.
IntroductionHypertension affects 27% of the Canadian adult popula-
tion aged 35-64 years1 and over 50% of people aged 65 yearsand older.2,3 Hypertension remains one of the most commonmodifiable risk factors for cardiovascular disease in Canada andglobally.4,5 Each year, numerous studies are published that mayaffect the clinical practice of hypertension. The objective of theannual updates on the CHEP recommendations is to providetimely evidence-based recommendations to primary care pro-viders to improve hypertension prevention, detection, andcontrol in Canadians. Key clinical questions addressed include:(1) How is hypertension diagnosed? (2) How do we diagnosewhite coat hypertension? (3)What frequency of follow-up andlaboratory testing is necessary for hypertensive patients? (4)How is risk assessed for future cardiovascular events in thesepatients? (5) When should we start pharmacological therapy tocontrol hypertension? (6) What BP level should be attained inhypertensive patients and in patients with coexisting diabetesor CKD? (7) What lifestyle interventions are effective in pre-venting hypertension and reducing BP? (8) What are the opti-mal pharmacological agents for treatment of hypertension, aswell as hypertension occurring in patients with specific comor-bid conditions, including diabetes, cardiovascular disease,stroke, or kidney disease? (9) How can we improve adherenceto antihypertensive medications? (10) How do we diagnoseand treat secondary causes of hypertension, renovascular hy-pertension, pheochromocytoma, and hyperaldosteronism?
In this document, we outline all of the recommendationsand discuss the evidence and rationale on those recommenda-tions that are new or updated. More detailed discussion ofprevious changes to the Canadian recommendations is avail-able in prior publications.6-17 This year, the recommendationsunderwent significant revision based on recently published trialsand rereview of earlier studies: Eplerenone in Mild Patients Hos-pitalization and Survival Study in Heart Failure (EMPHASIS-HF) trial,18 Eplerenone Post-Acute Myocardial InfarctionHeart Failure Efficacy and Survival Study (EPHESUS),19 andRandomized Aldactone Evaluation Study (RALES)20 for theheart failure recommendation; Atrial Fibrillation ClopidogrelTrial With Irbesartan for Prevention of Vascular Events(ACTIVE I),21 Angiotensin II Antagonist in Paroxysmal AtrialFibrillation (ANTIPAF)22 and Gruppo Italiano per lo Studiodella Sopravvivenza nell’Infarto Miocardico-Atrial Fibrillation(GISSI-AF),23 for AF; African American Study of Kidney Dis-ease and Hypertension (AASK) follow-up extension trial,24-26
Ramipril Efficacy in Nephropathy-2 (REIN-2),27 and Modifi-cation of Diet in Renal Disease (MDRD)28,29 trials for the BPtargets for CKD; and 2 meta-analyses of large clinical trialsrecently published on BP treatment targets for patients withdiabetes.30,31 Also, the evidence base for diagnosing white coathypertension using home BP monitoring was reviewed.
These recommendations are targeted toward primary careproviders and apply to adults at risk for or with hypertension.For issues related to the diagnosis and evaluation of high BP inchildren and adolescents, the reader is referred to separateguidelines.32 A version of the hypertension recommendations
272 Canadian Journal of CardiologyVolume 28 2012
designed for patient and public education has been developedto assist health care practitioners managing hypertension. Thesummary is freely available at: http://www.hypertension.ca.
Although we mention individual antihypertensive agents whendiscussing trials, the reader may assume that all drug-specific rec-ommendations are applicable to the entire drug class in question,unless otherwise stated. Finally, although these recommendationsare based on best evidence, health care providers must also usetheir own clinical judgement and consider patient preferenceswhen applying these recommendations for their patients.
MethodsA Cochrane Collaboration librarian conducted a MEDLINE/
PubMed search using text words and MeSH headings (copies ofthe different strategies are available upon request). Commonsearch terms were hypertension[MeSH], hypertens*[ti, ab], andblood pressure, which were then combined with terms forthe specific concept each subgroup investigated. A highlysensitive search strategy for randomized trials and systematicreviews published up to August 2011 was used, and in orderto ensure that all relevant studies were included, bibliogra-phies of identified articles were also manually searched (de-tails of search strategies and retrieved articles are available onrequest). Studies were selected if they included the relevantoutcomes. The outcomes primarily considered includedchanges in cardiovascular morbidity and mortality as well astotal mortality. However, BP lowering was accepted as aprimary outcome for lifestyle modification recommenda-tions and progressive renal impairment was also accepted forpatients with CKD. Randomized controlled trials (RCTs)and systematic reviews of randomized trials were selected fortreatment recommendations and cross sectional and cohortstudies were reviewed for assessing diagnosis and prognosis.Study characteristics and study quality were assessed usingpre-specified, standardized algorithms for RCTs and cohortstudies developed by CHEP.33
Draft recommendations were developed for each sectionby national and international hypertension experts based onreview of all identified articles relevant to their topic area(see Supplemental Appendix S1). Members of the CanadianDiabetes Association Guidelines Committee, Canadian So-ciety of Nephrology, Canadian Stroke Network, and theCanadian Cardiovascular Harmonized National GuidelineEndeavour Initiative also collaborated with CHEP sub-group members for the development of 2012 draft recom-mendations to ensure harmonized hypertension recommen-dations between guidelines. Cardiovascular and mortalitybenefits as well as adverse effects and risks were consideredwhen formulating the draft recommendations. Costs werenot considered. Subsequently, the central review committeecomposed of clinical epidemiologists, reviewed draft recom-mendations from each subgroup and, in an iterative process,helped to refine and standardize all recommendations andtheir grading across subgroups; recommendations were clas-sified according to the strength of evidence (for details, seeTable 1), ranging from A (strongest evidence, high-preci-sion randomized clinical trials) to D (expert opinion alone).CHEP members then discussed and vetted the draft recom-mendations and evidence from each subgroup at the 2012consensus conference held in Alliston, Ontario. Based on
the deliberations at the consensus conference, the 2012 rec-ommendations were finalized and then submitted to all 65voting members of the CHEP Evidence-Based Recommen-dations Task Force for approval. External observers fromthe Canadian Agency for Drugs and Health, the BrazilianSociety of Cardiology, and the Public Health Agency ofCanada were also present at the consensus meeting. Members withconflicts of interest were recused from voting on the specific rec-ommendations (a list of conflicts can be found in SupplementalAppendix S2). Recommendations were finalized after achievingconsensus, defined as recommendations approved by ! 70% ofthe task force. In the actual vote, all recommendations received atleast 80% approval.
The 2012 CHEP Diagnosis and AssessmentRecommendations
I. Accurate measurement of BPRecommendations
1. Health care professionals who have been specifically trainedto measure BP accurately should assess BP in all adult pa-tients at all appropriate visits to determine cardiovascularrisk and monitor antihypertensive treatment (Grade D).
2. Use of standardized measurement techniques (see Supple-mental Table S1) is recommended when assessing BP(Grade D).
3. Automated office BP measurements (OBPM) can be usedin the assessment of office BP (Grade D).
4. When used in proper conditions, automated office systolicBP (SBP) of ! 135 mm Hg or diastolic BP (DBP) of ! 85mm Hg should be considered analogous to mean awakeambulatory SBP of ! 135 mm Hg and DBP of ! 85 mmHg, respectively (Grade D).
Background. Several automated OBPM devices have been in-dependently validated for clinical accuracy, including theBpTRU automatic BP monitor, the BPM-100 electronic oscillo-metric office BP monitor (VSM MedTech Ltd, Vancouver, BC),and the Omron office digital BP HEM-907 monitor (OmronHealthcare Inc, Lake Forest, IL).34-36 However, further research isneeded to determine whether automated OBPM accurately pre-dict future target organ damage and cardiovascular events betterthan manual OBPM. CHEP is actively evaluating this area.
Table 1. Grading scheme for recommendations
Grade A Recommendations are based on randomized trials (orsystematic reviews of trials) with high levels of internalvalidity and statistical precision, and for which the studyresults can be directly applied to patients because of similarclinical characteristics and the clinical relevance of thestudy outcomes.
Grade B Recommendations are based on randomized trials, systematicreviews or pre-specified subgroup analyses of randomizedtrials that have lower precision, or there is a need toextrapolate from studies because of differing populationsor reporting of validated intermediate/surrogate outcomesrather than clinically important outcomes.
Grade C Recommendations from trials that have lower levels ofinternal validity and/or precision, or report unvalidatedsurrogate outcomes, or results from nonrandomizedobservational studies.
Grade D Recommendations are based on expert opinion alone.
Daskalopoulou et al.2012 Canadian Recommendations for High BP
273
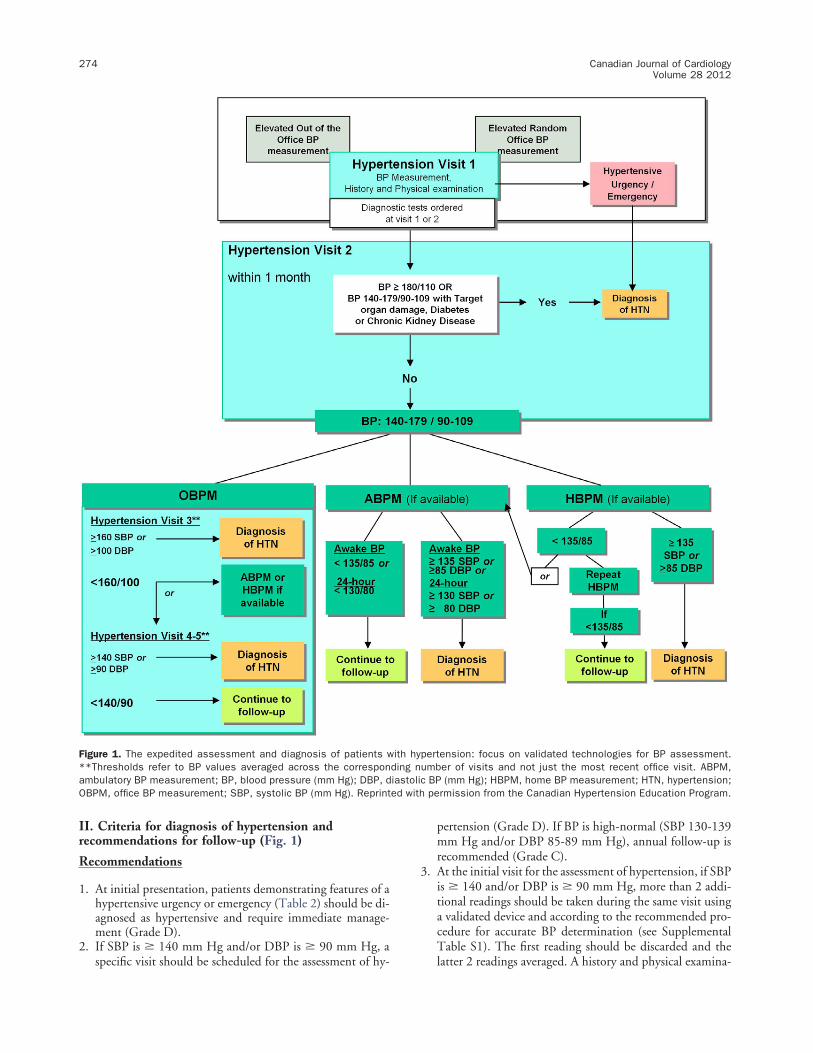
II. Criteria for diagnosis of hypertension andrecommendations for follow-up (Fig. 1)Recommendations
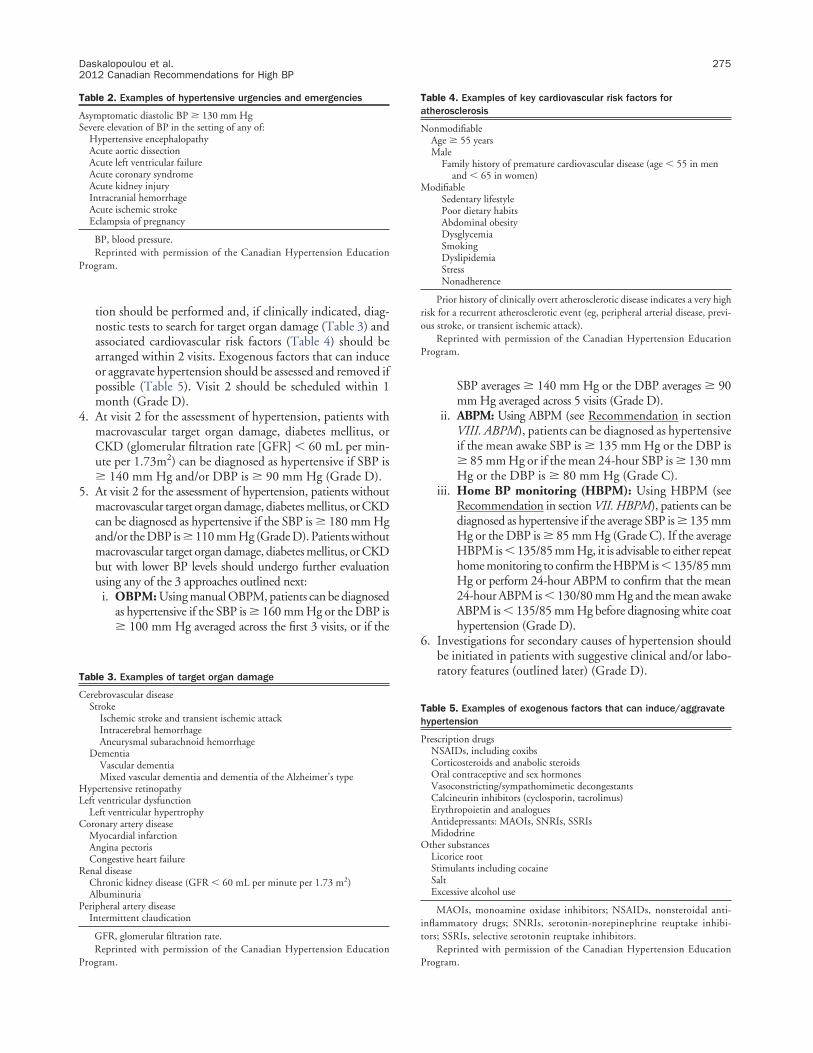
1. At initial presentation, patients demonstrating features of ahypertensive urgency or emergency (Table 2) should be di-agnosed as hypertensive and require immediate manage-ment (Grade D).
2. If SBP is ! 140 mm Hg and/or DBP is ! 90 mm Hg, aspecific visit should be scheduled for the assessment of hy-
pertension (Grade D). If BP is high-normal (SBP 130-139mm Hg and/or DBP 85-89 mm Hg), annual follow-up isrecommended (Grade C).
3. At the initial visit for the assessment of hypertension, if SBPis ! 140 and/or DBP is ! 90 mm Hg, more than 2 addi-tional readings should be taken during the same visit usinga validated device and according to the recommended pro-cedure for accurate BP determination (see SupplementalTable S1). The first reading should be discarded and thelatter 2 readings averaged. A history and physical examina-
Figure 1. The expedited assessment and diagnosis of patients with hypertension: focus on validated technologies for BP assessment.**Thresholds refer to BP values averaged across the corresponding number of visits and not just the most recent office visit. ABPM,ambulatory BP measurement; BP, blood pressure (mm Hg); DBP, diastolic BP (mm Hg); HBPM, home BP measurement; HTN, hypertension;OBPM, office BP measurement; SBP, systolic BP (mm Hg). Reprinted with permission from the Canadian Hypertension Education Program.
274 Canadian Journal of CardiologyVolume 28 2012
tion should be performed and, if clinically indicated, diag-nostic tests to search for target organ damage (Table 3) andassociated cardiovascular risk factors (Table 4) should bearranged within 2 visits. Exogenous factors that can induceor aggravate hypertension should be assessed and removed ifpossible (Table 5). Visit 2 should be scheduled within 1month (Grade D).
4. At visit 2 for the assessment of hypertension, patients withmacrovascular target organ damage, diabetes mellitus, orCKD (glomerular filtration rate [GFR] ! 60 mL per min-ute per 1.73m2) can be diagnosed as hypertensive if SBP is! 140 mm Hg and/or DBP is ! 90 mm Hg (Grade D).
5. At visit 2 for the assessment of hypertension, patients withoutmacrovascular target organ damage, diabetes mellitus, or CKDcan be diagnosed as hypertensive if the SBP is ! 180 mm Hgand/or the DBP is ! 110 mm Hg (Grade D). Patients withoutmacrovascular target organ damage, diabetes mellitus, or CKDbut with lower BP levels should undergo further evaluationusing any of the 3 approaches outlined next:
i. OBPM: Using manual OBPM, patients can be diagnosedas hypertensive if the SBP is ! 160 mm Hg or the DBP is! 100 mm Hg averaged across the first 3 visits, or if the
SBP averages ! 140 mm Hg or the DBP averages ! 90mm Hg averaged across 5 visits (Grade D).
ii. ABPM: Using ABPM (see Recommendation in sectionVIII. ABPM), patients can be diagnosed as hypertensiveif the mean awake SBP is ! 135 mm Hg or the DBP is! 85 mm Hg or if the mean 24-hour SBP is ! 130 mmHg or the DBP is ! 80 mm Hg (Grade C).
iii. Home BP monitoring (HBPM): Using HBPM (seeRecommendation in section VII. HBPM), patients can bediagnosed as hypertensive if the average SBP is ! 135 mmHg or the DBP is ! 85 mm Hg (Grade C). If the averageHBPM is ! 135/85 mm Hg, it is advisable to either repeathome monitoring to confirm the HBPM is ! 135/85 mmHg or perform 24-hour ABPM to confirm that the mean24-hour ABPM is ! 130/80 mm Hg and the mean awakeABPM is ! 135/85 mm Hg before diagnosing white coathypertension (Grade D).
6. Investigations for secondary causes of hypertension shouldbe initiated in patients with suggestive clinical and/or labo-ratory features (outlined later) (Grade D).
Table 2. Examples of hypertensive urgencies and emergencies
Asymptomatic diastolic BP ! 130 mm HgSevere elevation of BP in the setting of any of:
Hypertensive encephalopathyAcute aortic dissectionAcute left ventricular failureAcute coronary syndromeAcute kidney injuryIntracranial hemorrhageAcute ischemic strokeEclampsia of pregnancy
BP, blood pressure.Reprinted with permission of the Canadian Hypertension Education
Program.
Table 3. Examples of target organ damage
Cerebrovascular diseaseStroke
Ischemic stroke and transient ischemic attackIntracerebral hemorrhageAneurysmal subarachnoid hemorrhage
DementiaVascular dementiaMixed vascular dementia and dementia of the Alzheimer’s type
Prior history of clinically overt atherosclerotic disease indicates a very highrisk for a recurrent atherosclerotic event (eg, peripheral arterial disease, previ-ous stroke, or transient ischemic attack).
Reprinted with permission of the Canadian Hypertension EducationProgram.
Table 5. Examples of exogenous factors that can induce/aggravatehypertension
Prescription drugsNSAIDs, including coxibsCorticosteroids and anabolic steroidsOral contraceptive and sex hormonesVasoconstricting/sympathomimetic decongestantsCalcineurin inhibitors (cyclosporin, tacrolimus)Erythropoietin and analoguesAntidepressants: MAOIs, SNRIs, SSRIsMidodrine
Other substancesLicorice rootStimulants including cocaineSaltExcessive alcohol use
Reprinted with permission of the Canadian Hypertension EducationProgram.
Daskalopoulou et al.2012 Canadian Recommendations for High BP
275
7. If at the last diagnostic visit the patient is not diagnosed as hyper-tensiveandhasnoevidenceofmacrovascular targetorgandamage,the patient’s BP should be assessed at yearly intervals (Grade D).
8. Hypertensive patients receiving lifestyle modification advicealone (nonpharmacological treatment) should be followed upat 3- to 6-month intervals. Shorter intervals (every 1 or 2months) are needed for patients with higher BP (Grade D).
9. Patients given antihypertensive drug treatment should be seenmonthly or every 2 months, depending on the level of BP, untilreadings on 2 consecutive visits are below their target (GradeD). Shorter intervals between visits will be needed for symp-tomatic patients and those with severe hypertension, intoler-ance to antihypertensive drugs, or target organ damage (gradeD). When the target BP has been reached, patients should beseen at 3- to 6-month intervals (grade D).
Background. White coat hypertension is associated with a bet-ter cardiovascular prognosis compared with those with elevatedBP at the office and in nonoffice settings.37 However, diagnos-ing white coat hypertension is challenging and has relied on24-hour ABPM to confirm its diagnosis. There is now cumu-lative evidence to indicate that repeated HBPM provides sig-nificant prognostic accuracy to be used in confirming whitecoat hypertension. Recent evidence from 163 subjects enrolledin an observational study suggests that HBPM demonstratedthe lowest variability when compared with office and ambula-tory monitoring.38 Within-person variability improved withlonger self-monitoring duration and lower intervals betweenmonitoring; the lowest coefficients of variation (2.7 %) wasachieved after 4 weeks of monitoring without intervals, and thehighest (6.1%) when there was a 10-week interval in a total of1 week duration of measurements. Although it is recognizedthat neither HBPM nor ABPM are perfectly reproducible andhave moderate diagnostic agreement, patients with white coathypertension diagnosed by either HBPM or awake-ABPM wereshown to have a more favourable risk profile and less target organdamage than those with sustained hypertension, with the percent-age of patients with high or very high cardiovascular risk decreas-ing progressively from sustained hypertension to white coat hyper-tension confirmed by both techniques (P ! 0.005 for trend).39
Furthermore, longitudinal evidence suggests that HBPM has abetter prognostic accuracy than OBPM; the incidence of cardio-vascular events in patients with white coat syndrome was high andnot significantly different from the incidence of cardiovascularevents in patients with controlled hypertension (hazard ratio[HR], 1.18, 95% confidence interval [CI], 0.67-2.10).40
III. Assessment of overall cardiovascular risk inhypertensive patientsRecommendations
1. Global cardiovascular risk should be assessed. Multifactorialrisk assessment models can be used to predict more accu-rately an individual’s global cardiovascular risk (Grade A)and to use antihypertensive therapy more efficiently (GradeD). In the absence of Canadian data to determine the accu-racy of risk calculations, avoid using absolute levels of risk tosupport treatment decisions (Grade C).
2. Consider informing patients of their global risk to improve theeffectiveness of risk factor modification (Grade B). Consider
also using analogies that describe comparative risk such as “car-diovascular age,” “vascular age,” or “heart age” to inform pa-tients of their risk status (Grade B).
Background. Risk calculators are freely available at: www.myhealthcheckup.com, and www.monbilansante.com. TheSystematic Cerebrovascular and Coronary Risk Evaluation(SCORE) risk calculation was updated using Canadian dataand is now available at http://www.scorecanada.ca. There areno changes to these recommendations for 2012.
IV. Routine and optional laboratory tests for theinvestigation of patients with hypertensionRecommendations
1. Routine laboratory tests that should be performed for theinvestigation of all patients with hypertension include thefollowing:
i. Urinalysis (Grade D);ii. Blood chemistry (potassium, sodium, and creatinine)
(Grade D);iii. Fasting blood glucose (Grade D);iv. Fasting serum total cholesterol and high-density lipo-
protein cholesterol, low-density lipoprotein cholesterol,and triglycerides (Grade D);
v. Standard 12-lead electrocardiography (Grade C).2. Assess urinary albumin excretion in patients with diabetes
(Grade D).3. All treated hypertensive patients should be monitored ac-
cording to the current Canadian Diabetes Associationguidelines for the new appearance of diabetes (Grade B).
4. During the maintenance phase of hypertension manage-ment, tests (including those for electrolytes, creatinine, andfasting lipids) should be repeated with a frequency reflectingthe clinical situation (Grade D).
Background. There are no changes to these recommendationsfor 2012.
V. Assessment for renovascular hypertensionRecommendations
1. Patients presenting with ! 2 of the clinical clues listed next,suggesting renovascular hypertension, should be investi-gated (Grade D):i. Sudden onset or worsening of hypertension and age "
55 or ! 30 years;ii. Presence of an abdominal bruit;
iii. Hypertension resistant to ! 3 drugs;iv. Rise in serum creatinine level !30% associated with use of an
angiotensin-converting enzyme (ACE) inhibitor or ARB;v. Other atherosclerotic vascular disease, particularly in pa-
tients who smoke or have dyslipidemia;vi. Recurrent pulmonary edema associated with hypertensive
surges. When available, the following tests are recom-mended to aid in the usual screening for renal vasculardisease: captopril-enhanced radioisotope renal scan, Dopp-ler sonography, magnetic resonance angiography, andcomputed tomography angiography (for those with nor-mal renal function) (Grade B). Captopril-enhanced radio-
276 Canadian Journal of CardiologyVolume 28 2012
isotope renal scan is not recommended for those with CKD(GFR ! 60 mL per minute per 1.73m2) (Grade D).
Background. There are no changes to these recommendationsfor 2012.
VI. Endocrine hypertensionRecommendationsA. Hyperaldosteronism: screening and diagnosis
1. Screening for hyperaldosteronism should be considered forthe following patients (Grade D):
i. Hypertensive patients with spontaneous hypokalemia(K" ! 3.5 mmol/L);
ii. Hypertensive patients with marked diuretic-inducedhypokalemia (K" ! 3.0 mmol/L);
iii. Patients with hypertension refractory to treatment with! 3 drugs;
iv. Hypertensive patients found to have an incidental ad-renal adenoma.
2. Screening for hyperaldosteronism should include assess-ment of plasma aldosterone and plasma renin activity (Sup-plemental Table S2).
3. For patients with suspected hyperaldosteronism (on thebasis of the screening test, Supplemental Table S2, Item3), a diagnosis of primary aldosteronism should be estab-lished by demonstrating inappropriate autonomous hy-persecretion of aldosterone using at least one of the ma-noeuvres listed in Supplemental Table S2, Item 4. Whenthe diagnosis is established, the abnormality should belocalized using any of the tests described in SupplementalTable S2, Item 5.
B. Pheochromocytoma: screening and diagnosis
1. If pheochromocytoma is strongly suspected, the patientshould be referred to a specialized hypertension centre, par-ticularly if biochemical screening tests (Supplemental TableS3) have already been found to be positive (Grade D).
2. The following patients should be considered for screeningfor pheochromocytoma (Grade D):
i. Patients with paroxysmal and/or severe (BP ! 180/110mm Hg) sustained hypertension refractory to usual an-tihypertensive therapy;
ii. Patients with hypertension and multiple symptomssuggestive of catecholamine excess (eg, headaches, pal-pitations, sweating, panic attacks, and pallor);
iii. Patients with hypertension triggered by "-blockers,monoamine oxidase inhibitors, micturition, or changesin abdominal pressure;
iv. Patients with incidentally discovered adrenal mass andpatients with hypertension and multiple endocrine neo-plasia 2A or 2B, von Recklinghausen’s neurofibroma-tosis, or von Hippel-Lindau disease;
v. For patients with positive biochemical screening tests, lo-calization of pheochromocytomas should involve the useof magnetic resonance imaging (preferable), computed to-mography (if magnetic resonance imaging unavailable),and/or iodine I-131 meta-iodobenzylguanidine scintigra-phy (Grade C for each modality).
Background. There are no changes to these recommendationsfor 2012.
VII. HBPMRecommendations
1. HBPM can be used in the diagnosis of hypertension(Grade C).
2. The use of HBPM on a regular basis should be consideredfor patients with hypertension, particularly those with:
i. Diabetes mellitus (Grade D);ii. CKD (Grade C);
iii. Suspected nonadherence (Grade D);iv. Demonstrated white coat effect (Grade C);v. BP controlled in the office but not at home (masked
hypertension) (Grade C).3. When white coat hypertension is suggested by HBPM, its
presence should be confirmed by repeat HBPM (see Rec-ommendation 8) or ABPM before treatment decisions aremade (Grade D).
4. Patients should be advised to purchase and use only HBPMdevices that are appropriate for the individual and have metstandards of the Association for the Advancement ofMedical Instrumentation, the most recent requirementsof the British Hypertension Society protocol, or the In-ternational Protocol for validation of automated BPmeasuring devices. Patients should be encouraged to usedevices with data recording capabilities or automaticdata transmission to increase the reliability of reportedHBPM (Grade D).
5. Home SBP values ! 135 mm Hg or DBP values ! 85 mm Hgshould be considered elevated and associated with an increasedoverall mortality risk analogous to office SBP readings of !140 mm Hg or DBP ! 90 mm Hg (Grade C).
6. Health care professionals should ensure that patients whomeasure their BP at home have adequate training and, ifnecessary, repeat training in measuring their BP. Patientsshould be observed to determine that they measure BP cor-rectly and should be given adequate information about in-terpreting these readings (Grade D).
7. The accuracy of all individual patients’ validated devices(including electronic devices) must be regularly checkedagainst a device of known calibration (Grade D).
8. HBPM for assessing white coat hypertension or sustainedhypertension should be based on duplicate measures, morn-ing and evening, for an initial 7-day period. First-day homeBP values should not be considered (Grade D).
Background. Information on validated BP monitors can befound at: http://www.hypertension.ca/devices-endorsed-by-hypertension-canada-dp1.
Updated background information on white coat hyperten-sion is provided in section II. Criteria for Diagnosis of Hyper-tension and Recommendations for Follow-up. There are no otherchanges to these recommendations for 2012.
VIII. ABPMRecommendations
1. BP monitoring can be used in the diagnosis of hyperten-sion (Grade C). ABPM should be considered when anoffice-induced increase in BP is suspected in treated pa-tients with:
Daskalopoulou et al.2012 Canadian Recommendations for High BP
277
i. BP that is not below target despite receiving appropriatechronic antihypertensive therapy (Grade C);
ii. Symptoms suggestive of hypotension (Grade C);iii. Fluctuating office BP readings (Grade D).
2. Physicians should use only ABPM devices that have been val-idated independently using established protocols (Grade D).
3. Therapy adjustment should be considered in patients with amean 24-hour ambulatory SBP of ! 130 mm Hg or DBPof ! 80 mm Hg or a mean awake SBP of ! 135 mm Hg orDBP of ! 85 mm Hg (Grade D).
4. The magnitude of changes in nocturnal BP should be takeninto account in any decision to prescribe or withhold drugtherapy based upon ABPM (Grade C) because a decrease innocturnal BP of ! 10% is associated with increased risk ofcardiovascular events.
Background. There are no changes to these recommendationsfor 2012.
IX. Role of echocardiographyRecommendations
1. Routine echocardiographic evaluation of all hypertensivepatients is not recommended (Grade D).
2. An echocardiogram for assessment of left ventricular hyper-trophy is useful in selected cases to help define the futurerisk of cardiovascular events (Grade C).
3. Echocardiographic assessment of left ventricular mass, as wellas of systolic and diastolic left ventricular function is recom-mended for hypertensive patients suspected to have left ven-tricular dysfunction or coronary artery disease (Grade D).
4. Patients with hypertension and evidence of heart failure shouldhave an objective assessment of left ventricular EF, either byechocardiogram or nuclear imaging (Grade D).
Background. There are no changes to these recommendationsfor 2012.
The CHEP 2012 Prevention and TreatmentRecommendations
I. Lifestyle managementRecommendationsA. Physical exercise
1. For nonhypertensive individuals (to reduce the possibility ofbecoming hypertensive) or for hypertensive patients (to reducetheir BP), prescribe the accumulation of 30-60 minutes ofmoderate intensity dynamic exercise (eg, walking, jogging, cy-cling or swimming) 4-7 days per week in addition to the rou-tine activities of daily living (Grade D). Higher intensities ofexercise are not more effective (Grade D).
B. Weight reduction
1. Height, weight, and waist circumference should be measured,and body mass index calculated for all adults (Grade D).
2. Maintenance of a healthy body weight (body mass index18.5 to 24.9, and waist circumference ! 102 cm for menand ! 88 cm for women) is recommended for nonhyper-tensive individuals to prevent hypertension (Grade C) andfor hypertensive patients to reduce BP (Grade B). All over-
weight hypertensive individuals should be advised to loseweight (Grade B).
3. Weight loss strategies should employ a multidisciplinary ap-proach that includes dietary education, increased physical ac-tivity, and behavioural intervention (Grade B).
C. Alcohol consumption
1. To reduce BP, alcohol consumption should be in accor-dance with Canadian low-risk drinking guidelines in bothnormotensive and hypertensive individuals. Healthy adultsshould limit alcohol consumption to " 2 drinks per day,and consumption should not exceed 14 standard drinks perweek for men and 9 standard drinks per week for women(Grade B). (Note: One standard drink is considered to beequivalent of 13.6 g or 17.2 mL of ethanol or approximately44 mL [1.5 oz] of 80 proof [40%] spirits, 355 mL [12 oz] of5% beer, or 148 mL [5 oz] of 12% wine).
D. Dietary recommendations
1. It is recommended that hypertensive patients and normo-tensive individuals at increased risk of developing hyperten-sion consume a diet that emphasizes fruits, vegetables, low-fat dairy products, dietary and soluble fibre, whole grains,and protein from plant sources that is reduced in satu-rated fat and cholesterol (Dietary Approaches to StopHypertension [DASH] diet41-44) (Supplemental TableS4) (Grade B).
E. Sodium intake
1. For prevention and treatment of hypertension, a dietarysodium intake of 1500 mg (65 mmol) per day is recom-mended for adults aged "50 years; 1300 mg (57 mmol) perday for age 51-70 years; and 1200 mg (52 mmol) per day forage " 70 years (Grade B).
F. Potassium, calcium, and magnesium intake
1. Supplementation of potassium, calcium, and magnesium isnot recommended for the prevention or treatment of hy-pertension (Grade B).
G. Stress management
1. In hypertensive patients in whom stress may be contribut-ing to BP elevation, stress management should be consid-ered as an intervention (Grade D). Individualized cogni-tive-behavioural interventions are more likely to be effectivewhen relaxation techniques are used (Grade B).
Background. There are no changes to these recommendationsfor 2012.
II. Indications for drug therapy for adults withhypertension without compelling indications forspecific agentsRecommendations
1. Antihypertensive therapy should be prescribed for averageDBP measurements of ! 100 mm Hg (Grade A) or averageSBP measurements of ! 160 mm Hg (Grade A) in patientswithout macrovascular target organ damage or other cardio-vascular risk factors.
2. Antihypertensive therapy should be strongly considered ifDBP readings average ! 90 mm Hg in the presence of
278 Canadian Journal of CardiologyVolume 28 2012
macrovascular target organ damage or other independentcardiovascular risk factors (Grade A).
3. Antihypertensive therapy should be strongly considered ifSBP readings average ! 140 mm Hg in the presence ofmacrovascular target organ damage (Grade C for 140-160mm Hg; Grade A for ! 160 mm Hg).
4. Antihypertensive therapy should be considered in all pa-tients meeting the above indications regardless of age(Grade B). Caution should be exercised in elderly patientswho are frail.
Background. There are no changes to these recommendationsfor 2012.
III. Choice of therapy for adults with hypertensionwithout compelling indications for specific agentsRecommendationsA. Recommendations for individuals with diastolic and/orsystolic hypertension
1. Initial therapy should be monotherapy with a thiazide di-uretic (Grade A), a "-blocker (in patients younger than 60years, Grade B), an ACE inhibitor (in nonblack patients,Grade B), a long-acting calcium channel blocker (CCB)(Grade B); or an ARB (Grade B). If there are adverse effects,another drug from this group should be substituted. Hypo-kalemia should be avoided in patients treated with thiazidediuretic monotherapy (Grade C).
2. Additional antihypertensive drugs should be used if targetBP levels are not achieved with standard-dose monotherapy(Grade B). Add-on drugs should be chosen from first-linechoices. Useful choices include a thiazide diuretic or CCBwith either: ACE inhibitor, ARB, or "-blocker (Grade B forthe combination of thiazide diuretic and a dihydropyridineCCB; Grade C for the combination of dihydropyridineCCB and ACE inhibitor; and Grade D for all other com-binations). Caution should be exercised in combining anondihydropyridine CCB and a "-blocker (Grade D). Thecombination of an ACE inhibitor and an ARB is not rec-ommended (Grade A).
3. Combination therapy using 2 first-line agents may also beconsidered as initial treatment of hypertension (Grade C) ifSBP is 20 mm Hg above target or if DBP is 10 mm Hgabove target. However, caution should be exercised in pa-tients in whom a substantial fall in BP from initial combi-nation therapy is more likely to occur or in whom it wouldbe poorly tolerated (eg, elderly patients).
4. If BP is still not controlled with a combination of 2 or morefirst-line agents, or there are adverse effects, other antihy-pertensive drugs may be added (Grade D).
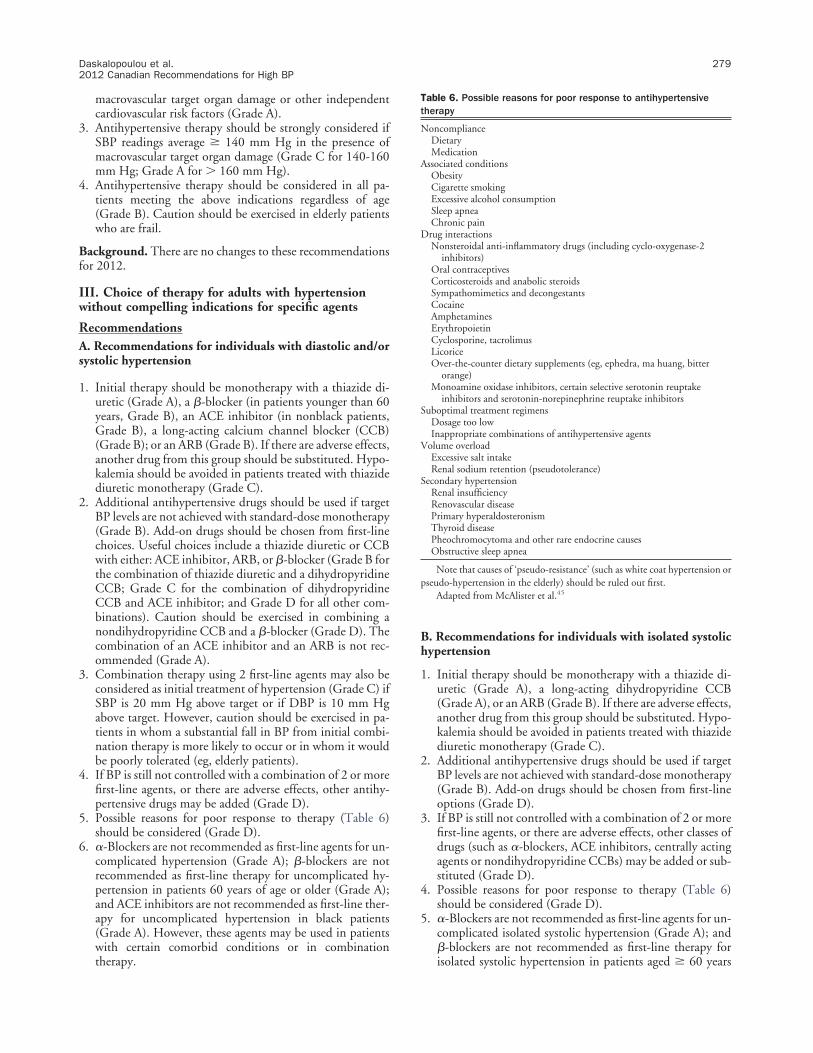
5. Possible reasons for poor response to therapy (Table 6)should be considered (Grade D).
6. #-Blockers are not recommended as first-line agents for un-complicated hypertension (Grade A); "-blockers are notrecommended as first-line therapy for uncomplicated hy-pertension in patients 60 years of age or older (Grade A);and ACE inhibitors are not recommended as first-line ther-apy for uncomplicated hypertension in black patients(Grade A). However, these agents may be used in patientswith certain comorbid conditions or in combinationtherapy.
B. Recommendations for individuals with isolated systolichypertension
1. Initial therapy should be monotherapy with a thiazide di-uretic (Grade A), a long-acting dihydropyridine CCB(Grade A), or an ARB (Grade B). If there are adverse effects,another drug from this group should be substituted. Hypo-kalemia should be avoided in patients treated with thiazidediuretic monotherapy (Grade C).
2. Additional antihypertensive drugs should be used if targetBP levels are not achieved with standard-dose monotherapy(Grade B). Add-on drugs should be chosen from first-lineoptions (Grade D).
3. If BP is still not controlled with a combination of 2 or morefirst-line agents, or there are adverse effects, other classes ofdrugs (such as #-blockers, ACE inhibitors, centrally actingagents or nondihydropyridine CCBs) may be added or sub-stituted (Grade D).
4. Possible reasons for poor response to therapy (Table 6)should be considered (Grade D).
5. #-Blockers are not recommended as first-line agents for un-complicated isolated systolic hypertension (Grade A); and"-blockers are not recommended as first-line therapy forisolated systolic hypertension in patients aged ! 60 years
Table 6. Possible reasons for poor response to antihypertensivetherapy
Drug interactionsNonsteroidal anti-inflammatory drugs (including cyclo-oxygenase-2
inhibitors)Oral contraceptivesCorticosteroids and anabolic steroidsSympathomimetics and decongestantsCocaineAmphetaminesErythropoietinCyclosporine, tacrolimusLicoriceOver-the-counter dietary supplements (eg, ephedra, ma huang, bitter
orange)Monoamine oxidase inhibitors, certain selective serotonin reuptake
inhibitors and serotonin-norepinephrine reuptake inhibitorsSuboptimal treatment regimens
Dosage too lowInappropriate combinations of antihypertensive agents
Volume overloadExcessive salt intakeRenal sodium retention (pseudotolerance)
Secondary hypertensionRenal insufficiencyRenovascular diseasePrimary hyperaldosteronismThyroid diseasePheochromocytoma and other rare endocrine causesObstructive sleep apnea
Note that causes of ‘pseudo-resistance’ (such as white coat hypertension orpseudo-hypertension in the elderly) should be ruled out first.
Adapted from McAlister et al.45
Daskalopoulou et al.2012 Canadian Recommendations for High BP
279
(Grade A). However, both agents may be used in patientswith certain comorbid conditions or in combinationtherapy.
Background. Recent concern was raised regarding the poten-tial association of cancer with ARBs amid publication of severalrecent post hoc analyses. The 2012 guidelines continue to rec-ommend the use of ARBs in appropriate clinical situationsgiven the completed safety analysis commissioned by the USFood and Drug Administration of 31 clinical trials and156,000 patients finding no evidence of an increased risk ofcancer in patients who take an ARB.46 There are no changes tothese recommendations.
IV. Global vascular protection therapy for adults withhypertension without compelling indications forspecific agentsRecommendations
1. Statin therapy is recommended in hypertensive patientswith 3 or more cardiovascular risk factors as defined in Ta-ble 7 (Grade A in patients ! 40 years), or with establishedatherosclerotic disease (Grade A regardless of age).
2. Strong consideration should be given to the addition oflow-dose acetylsalicylic acid therapy in hypertensive pa-tients (Grade A in patients ! 50 years). Caution should beexercised if BP is not controlled (Grade C).
Background. There are no changes to these recommendationsfor 2012. For further guidance in the management of patientswith dyslipidemia, readers are referred to the 2009 CanadianCardiovascular Society/Canadian guidelines for the diagnosisand treatment of dyslipidemia and prevention of cardiovascu-lar disease in the adult.48
V. Goal of therapy for adults with hypertensionwithout compelling indications for specific agentsRecommendations
1. The SBP treatment goal is a pressure level of " 140 mm Hg(Grade C). The DBP treatment goal is a pressure level of "90 mm Hg (Grade A).
Background. There are no changes to these recommendationsfor 2012.
VI. Treatment of hypertension in association withischemic heart diseaseRecommendationsA. Recommendations for hypertensive patients with coro-nary artery disease
1. An ACE inhibitor or ARB is recommended for most patientswith hypertension and coronary artery disease (Grade A).
2. For patients with stable angina, !-blockers are preferred asinitial therapy (Grade B). CCBs may also be used (Grade B).
3. Short-acting nifedipine should not be used (Grade D).4. For patients with coronary artery disease, but without co-
existing systolic heart failure, the combination of an ACEinhibitor and ARB is not recommended (Grade B).
5. In high-risk patients, when combination therapy is beingused, choices should be individualized. The combination ofan ACE inhibitor and a dihydropyridine CCB is preferableto an ACE inhibitor and a diuretic in selected patients(Grade A).
B. Recommendations for patients with hypertension whohave had a recent myocardial infarction
1. Initial therapy should include both a !-blocker and an ACEinhibitor (Grade A).
2. An ARB can be used if the patient is intolerant of an ACEinhibitor (Grade A in patients with left ventricular systolicdysfunction).
3. CCBs may be used in postmyocardial infarction patientswhen !-blockers are contraindicated or not effective. Non-dihydropyridine CCBs should not be used when there isheart failure, as evidenced by pulmonary congestion on ex-amination or radiography (Grade D).
Background. There are no changes to these recommendationsfor 2012.
VII. Treatment of hypertension in association withheart failureRecommendations
1. In patients with systolic dysfunction (ejection fraction[EF] " 40%), ACE inhibitors (Grade A) and !-blockers(Grade A) are recommended for initial therapy. Aldoste-rone antagonists (mineralocorticoid receptor antagonists)may be added for patients with a recent cardiovascular hos-pitalization, acute myocardial infarction, elevated B-typenatriuretic peptide or N-terminal pro–B-type natriureticpeptide level, or New York Heart Association (NYHA) classII to IV symptoms (Grade A). Careful monitoring for hy-perkalemia is recommended when adding an aldosteroneantagonist to ACE inhibitor or ARB. Other diuretics arerecommended as additional therapy if needed (Grade B forthiazide diuretics for BP control, Grade D for loop diureticsfor volume control). Beyond considerations of BP control,doses of ACE inhibitors or ARBs should be titrated to thosefound to be effective in trials unless adverse effects becomemanifest (Grade B).
2. An ARB is recommended if ACE inhibitors are not toler-ated (Grade A).
3. A combination of hydralazine and isosorbide dinitrate isrecommended if ACE inhibitors and ARBs are contraindi-cated or not tolerated (Grade B).
Table 7. Cardiovascular risk factors for consideration of statintherapy in nondyslipidemic patients with hypertension
Male sexAge " 55 yearsLeft ventricular hypertrophyOther electrocardiogram abnormalities: left bundle branch block, left
Peripheral arterial diseasePrevious stroke or transient ischemic attackMicroalbuminuria or proteinuriaDiabetes mellitusSmokingFamily history of premature cardiovascular diseaseTotal cholesterol to high-density lipoprotein ratio 6
If hypertensive patients have " 3 of these risk factors, statins should beconsidered.
Data from Sever et al.47
280 Canadian Journal of CardiologyVolume 28 2012
4. For hypertensive patients whose BP is not controlled, anARB may be added to an ACE inhibitor and other antihy-pertensive drug treatment (Grade A). Careful monitoringshould be used if combining an ACE inhibitor and an ARBdue to potential adverse effects such as hypotension, hyper-kalemia, and worsening renal function (Grade C). Addi-tional therapies may also include dihydropyridine CCBs(Grade C).
Background. This year, we have expanded our recommenda-tion for mineralocorticoid receptor antagonists in patients withboth hypertension and chronic systolic heart failure (EF !40%) on the basis of compelling evidence from 3 RCTs. Ourprevious recommendation was guided by 2 earlier trials,RALES19 and EPHESUS.20 This year, the EMPHASIS-HFprovided definite evidence that establishes the beneficial effectof mineralocorticoid receptor antagonists on morbidity andmortality across a broad spectrum of systolic heart failure pa-tients.18 EMPHASIS-HF enrolled 2737 patients with heartfailure, who were randomized to receive either the mineralo-corticoid receptor antagonist eplerenone (up to 50 mg daily) orplacebo in addition to recommended therapy. Patients wereincluded if they were at least 55 years of age, had NYHA func-tional class II symptoms, an EF of no more than 30% (or, if "30% to 35%, a QRS duration " 130 ms on electrocardiogram)and treatment with an ACE inhibitor, an ARB or both, and a!-blocker (unless contraindicated) at the recommended doseor maximal tolerated dose. The trial was stopped prematurelyafter a median follow-up period of 21 months. The primaryoutcome, a composite of death from cardiovascular causes orhospitalization for heart failure, was significantly reduced inthe eplerenone group when compared with the placebo group(HR, 0.63; 95% CI, 0.54-0.74) as was risk of death (HR, 0.76;95% CI, 0.62-0.93). Importantly, excluded from the trial werepatients with a baseline serum potassium level " 5.0 mmol/Land a baseline estimated GFR ! 30 mL per minute per1.73m2. Despite this, compared with placebo there was a morethan 2-fold increased risk of hyperkalemia in the eplerenonegroup (3.7% vs 8.0%, respectively, P ! 0.001). This finding,coupled with earlier concerns regarding the risk of hyperkale-mia with spironolactone in more severe stages of heart failure,and in combination with other renin angiotensin antagonistsunderscore the importance of regular electrolyte monitoring inpatients who receive mineralocorticoid receptor antagonists.Thus, most patients with CKD and those with a history ofsevere hyperkalemia should not receive a mineralocorticoid re-ceptor antagonist.
This year, data from 3 ARB RCTs including patients withhypertension and AF (ACTIVE I, ANTIPAF, and GISSI-AF)were examined in detail.21-23 In ACTIVE I, irbesartan did notreduce either coprimary end point comprising major cardio-vascular events in patients with AF and at least 1 additionalstroke risk factor (HR, 0.99; 95% CI, 0.91-1.08; and HR,0.94; 95% CI, 0.87-1.02).21 Although irbesartan reduced therisk of hospitalization for heart failure (HR, 0.86; 95% CI,0.76-0.98), it did not significantly reduce the risk of hospital-ization for AF (HR, 0.95; 95% CI, 0.85-1.07). Furthermore,symptomatic hypotension was more common in the irbesartangroup (P ! 0.001) as was any renal dysfunction leading to drugdiscontinuation (P # 0.02). A similar lack of benefit for olm-esartan was noted in the ANTIPAF trial (in patients with par-
oxysmal AF without structural heart disease in sinus rhythm atrecruitment)22 and for valsartan in the GISSI-AF trial (in pa-tients with a history of recurrent AF in sinus rhythm at recruit-ment).23 Based on this evidence, the Task Force concluded thatARBs did not prevent recurrent AF or major cardiovascularevents in patients with AF. Therefore, the presence of AF inpatients with hypertension should not mandate selection of anARB for the treatment of hypertension.
VIII. Treatment of hypertension in association withstrokeRecommendationsA. BP management in acute stroke (onset to 72 hours)
1. For patients with ischemic stroke not eligible for thrombo-lytic therapy, treatment of hypertension in the setting ofacute ischemic stroke or transient ischemic attack shouldnot be routinely undertaken (Grade D). Extreme BP eleva-tion (eg, SBP " 220 mm Hg or DBP " 120 mm Hg) maybe treated to reduce the BP by approximately 15% (GradeD), and not more than 25%, over the first 24 hours withgradual reduction thereafter (Grade D). Avoid excessivelowering of BP as this may exacerbate existing ischemia ormay induce ischemia, particularly in the setting of intracra-nial arterial occlusion or extracranial carotid or vertebralartery occlusion (Grade D). Pharmacological agents androutes of administration should be chosen to avoid precip-itous falls in BP (Grade D).
2. For patients with ischemic stroke eligible for thrombolytictherapy, very high BP (" 185/110 mm Hg) should betreated concurrently in patients receiving thrombolytictherapy for acute ischemic stroke to reduce the risk of sec-ondary intracranial hemorrhage (Grade B).
B. BP management after acute stroke
1. Strong consideration should be given to the initiation ofantihypertensive therapy after the acute phase of a stroke ortransient ischemic attack (Grade A).
2. After the acute phase of a stroke, BP-lowering treatment isrecommended to a target of consistently ! 140/90 mm Hg(Grade C).
3. Treatment with an ACE inhibitor/diuretic combination ispreferred (Grade B).
4. For patients with stroke, the combination of an ACE inhib-itor and ARB is not recommended (Grade B).
Background. There are no changes to these recommendationsfor 2012.
IX. Treatment of hypertension in association with leftventricular hypertrophyRecommendations
1. Hypertensive patients with left ventricular hypertrophyshould be treated with antihypertensive therapy to lower therate of subsequent cardiovascular events (Grade C).
2. The choice of initial therapy can be influenced by the pres-ence of left ventricular hypertrophy (Grade D). Initial ther-apy can be drug treatment using ACE inhibitors, ARBs,long-acting CCBs, or thiazide diuretics. Direct arterial va-sodilators such as hydralazine or minoxidil should not beused.
Daskalopoulou et al.2012 Canadian Recommendations for High BP
281
Background. There are no changes to these recommendationsfor 2012.
X. Treatment of hypertension in association withnondiabetic CKDRecommendations
1. For patients with nondiabetic CKD, target BP is ! 140/90mm Hg (Grade B).
2. For patients with hypertension and proteinuric CKD (uri-nary protein " 500 mg/24 hours or albumin-to-creatinineratio " 30 mg/mmol), initial therapy should be an ACEinhibitor (Grade A) or an ARB if there is intolerance toACE inhibitors (Grade B).
3. Thiazide diuretics are recommended as additive antihy-pertensive therapy (Grade D). For patients with CKDand volume overload, loop diuretics are an alternative(Grade D).
4. In most cases, combination therapy with other antihyper-tensive agents may be needed to reach target BP levels(Grade D).
5. The combination of an ACE inhibitor and ARB is notrecommended for patients with nonproteinuric CKD(Grade B).
Background. This year, the results of 3 RCTs were examinedin detail and led to the revision of the previous BP target forhypertensive patients with nondiabetic CKD.
The MDRD trial included patients with GFR between 13and 55 mL per minute per 1.73m2 who were randomly as-signed to either a usual BP target (mean arterial pressure[MAP], 107 mm Hg, equivalent to 140/90 mm Hg) or a lowBP target (MAP 92 mm Hg, equivalent to 125/75 mmHg).28,29,49 In the primary analysis, there was no differencebetween the usual and low BP groups with respect to the slopeof decline in GFR. Secondary outcomes including kidney fail-ure, death, a composite of kidney failure or death, and cardio-vascular events were also not significantly different betweengroups. A post hoc, subgroup analysis showed that the rate ofGFR decline appeared to increase above a MAP of 98 mm Hgin patients with proteinuria between 0.25-3.0 gr/day, while inpatients with proteinuria of ! 3.0 gr/day, the rate of GFRdecline increased above a MAP of 92 mm Hg. However, thispost hoc analysis was limited by the fact that there was nostratification based on prespecified levels of proteinuria, a prioripower calculations were not performed for subgroups, baselinepatient characteristics were not presented according to sub-groups, and adjustment for multiple testing was not per-formed. Furthermore, the use of ACE inhibitors was higher inthe low BP target group.
In the AASK trial, African-American individuals with hy-pertensive CKD and GFR between 20 and 65 mL per minuteper 1.73m2 were randomly assigned to a usual BP target (MAP,102-107 mm Hg) or a low BP target (MAP, 92 mm Hg).24-26
In addition, patients were randomly assigned to treatment withramipril, metoprolol, or amlodipine in a 2 # 3 factorial design.There was no significant difference in the chronic slope or theoverall rate of decline in GFR per year between groups. Patientsin the low BP group experienced a 17% reduction in protein-uria as compared with an increase of 7% in the usual BP group.There was no difference in the risk of other secondary out-comes including kidney failure, the composite of kidney failure
or death, the composite of a GFR event or death, or the com-bined endpoint of GFR event, kidney failure, or death. Therewas no difference in cardiovascular mortality or nonfatal car-diovascular events. In the original AASK trial there was aninteraction between baseline proteinuria and BP target, whichwas not reported in the original analysis but in a subsequentanalysis. Similar to the MDRD trial, this was a post hoc sub-group analysis and randomization was not stratified based onprespecified levels of proteinuria, there were no a priori powercalculations for the subgroups, and adjustment for multipletesting was not performed. The suggestion that patients withproteinuria of " 300 mgr per day at baseline may derive benefitfrom a lower BP target, and that those with less proteinuria mayexperience worse outcomes, should be interpreted ashypothesis-generating.
The REIN-2 trial randomly assigned patients with nondia-betic CKD and " 1 gr/day of proteinuria to usual BP target(target DBP ! 90 mm Hg) or low BP target (target BP !130/80 mm Hg).27 All patients were treated with ramipril andthe low BP group received felodipine 5-10 mg/day togetherwith additional agents as needed to achieve targets. The trialwas stopped early due to futility after a median follow-up of19 months; this was defined a priori. Mean achieved BP was134/82 mm Hg in the usual BP group compared with130/80 mm Hg in the low BP group. There was no differ-ence in the risk of progression to kidney failure betweengroups (adjusted HR, 1.0; 95% CI, 0.61-1.64). Significantlimitations of this study included use of dihydropyridineCCB in the low BP group, the small difference in achievedBP (4/2 mm Hg) between groups, limited follow-up, as wellas the fact that all patients received therapy with a fixed doseof an ACE inhibitor.
Overall, there is no compelling evidence to support a lowBP target of ! 130/80 mm Hg in all patients with hyperten-sion and nondiabetic CKD. Despite observational evidencesuggesting that more intensive BP control may be beneficial inindividuals with " 300 mgr or " 1 gr/day of proteinuria, theonly RCT examining this issue was negative. Although asmaller benefit cannot be ruled out, the current evidence basedoes not support a more intensive BP target in this group.Therefore, the Task Force voted to remove the previous low BPtarget and resume the general BP target (! 140/90 mm Hg)recommended for patients with hypertension.
XI. Treatment of hypertension in association withrenovascular diseaseRecommendations
1. Renovascular hypertension should be treated in the samemanner as hypertension without compelling indications,except for caution in the use of ACE inhibitors or ARBs dueto the risk of acute renal failure in bilateral disease or uni-lateral disease with a solitary kidney (Grade D).
2. Close follow-up and early intervention (angioplasty andstenting or surgery) should be considered for patients withuncontrolled hypertension despite therapy with ! 3 drugs,deteriorating kidney function, bilateral atherosclerotic renalartery lesions (or tight atherosclerotic stenosis in a singlekidney), or recurrent episodes of flash pulmonary edema(Grade D).
282 Canadian Journal of CardiologyVolume 28 2012
Background. There are no changes to these recommendationsfor 2012.
XII. Treatment of hypertension in association withdiabetes mellitusRecommendations
1. Persons with diabetes mellitus should be treated to attainSBPs of ! 130 mm Hg (Grade C) and DBPs of ! 80 mmHg (Grade A). (These target BP levels are the same as the BPtreatment thresholds.) Combination therapy using 2 first-line agents may also be considered as initial treatment ofhypertension (Grade B) if SBP is 20 mm Hg above target orif DBP is 10 mm Hg above target. However, caution shouldbe exercised in patients in whom a substantial fall in BP ismore likely or poorly tolerated (eg, elderly patients and pa-tients with autonomic neuropathy).
2. For persons with cardiovascular or kidney disease, includingmicroalbuminuria or with cardiovascular risk factors in ad-dition to diabetes and hypertension, an ACE inhibitor or anARB is recommended as initial therapy (Grade A).
3. For persons with diabetes and hypertension not included inthe above recommendation, appropriate choices include (inalphabetical order): ACE inhibitors (Grade A), ARBs(Grade B), dihydropyridine CCBs (Grade A), and thiazide/thiazide-like diuretics (Grade A).
4. If target BP levels are not achieved with standard-dosemonotherapy, additional antihypertensive therapy shouldbe used. For persons in whom combination therapy with anACE inhibitor is being considered, a dihydropyridine CCBis preferable to hydrochlorothiazide (Grade A).
Background. This year, 2 meta-analyses that addressed thequestions about relative benefits and risks of achieving lowerSBP in patients with diabetes mellitus and hypertension werepublished.
The Bangalore et al. meta-analysis included trials that com-pared achieved SBP levels of ! 135 mm Hg, ! 130 mm Hg,and ! 140 mm Hg50 in patients with diabetes or impairedfasting glucose (IFG). The primary outcome was major adversecardiovascular events including mortality, cardiovascular mor-tality, myocardial infarction, stroke, and heart failure. SBP lev-els of ! 135 mm Hg were associated with reduced mortality(odds ratio [OR], 0.87; 95% CI, 0.79-0.95), and levels ! 130mm Hg were associated with reduced risk of stroke (OR, 0.53;95% CI, 0.38-0.75). Importantly, although significant adverseevents, such as hypotension and hyperkalemia were inconsis-tently reported across trials, there was a significant increase inthe odds of adverse events with SBP below both 135 mm Hgand 130 mm Hg.
The meta-analysis by Reboldi et al. included all antihyper-tensive trials that enrolled patients with hypertension and dia-betes but not impaired fasting glucose, and did a series of strat-ified meta-analyses and meta-regression analyses to determinethe benefit associated with different levels of SBP on myocar-dial infarction and stroke.51 Decreasing levels of SBP were as-sociated with increasing benefit in terms of stroke, but not interms of myocardial infarction. A meta-regression examiningthe association between the degree of SBP lowering and strokefound that for every 5% reduction in SBP, the risk of stroke wasreduced by 13%. Such a linear association between SBP reduc-tion and myocardial infarction risk reduction was not noted.
Both of these reviews were limited by the fact that they didnot examine target SBPs but rather SBPs achieved in the con-text of a clinical trial. Further, these reviews could not controlfor differences in duration of diabetes or glycemic control. Asthe Action to Control Cardiovascular Risk in Diabetes BloodPressure (ACCORD BP) trial suggested that an interactionbetween glycemic control and SBP lowering may exist, theinability to account for differences in diabetes managementshould be noted.45,52
Although the optimal BP target remains uncertain, thesemeta-analyses and results from ACCORD BP do not provideany compelling evidence to alter the present recommendation(! 130/80 mm Hg). This was mainly supported by the asso-ciation between SBP levels ! 130 mm Hg and reduction instroke on 1 hand, and the increased risk of adverse events, suchas hypotension and hyperkalemia with lower SBP targets onthe other hand, with the majority of adverse effects associatedwith SBP ! 120 mm Hg.
XIII. Adherence strategies for patientsRecommendations
1. Adherence to an antihypertensive prescription can be im-proved by a multipronged approach (Table 8).
Background. There are no changes to these recommendationsfor 2012.
XIV. Treatment of secondary hypertension due toendocrine causesRecommendations
1. Treatment of hyperaldosteronism and pheochromocytomaare outlined in Supplemental Tables S2 and S3.
Background. There are no changes to these recommendationsfor 2012.
Table 8. Strategies to improve patient adherence
Assist your patient to adhere by:! Tailoring pill-taking to fit patients’ daily habits (Grade D)! Simplifying medication regimens to once-daily dosing (Grade D)! Replacing multiple pill antihypertensive combinations with single pill
combinations (Grade C)! Utilizing unit-of-use packaging (of several medications to be taken
together) (Grade D)! Using a multidisciplinary team approach to improve adherence to an
antihypertensive prescription (Grade B)Assist your patient in getting more involved in their treatment by:
! Encouraging greater patient responsibility/autonomy in monitoringtheir blood pressure and adjusting their prescriptions (Grade C)
! Educating patients and patients’ families about their disease andtreatment regimens (Grade C)
Improve your management in the office and beyond by:! Assessing adherence to pharmacological and nonpharmacological
therapy at every visit (Grade D)! Encouraging adherence with therapy by out-of-office contact (either by
phone or mail), particularly during the first three months of therapy(Grade D)
! Coordinating with pharmacists and work-site health care givers toimprove monitoring of adherence with pharmacological and lifestylemodification prescriptions (Grade D)
! Utilizing electronic medication compliance aids (Grade D)
Reprinted with permission of the Canadian Hypertension EducationProgram.
Daskalopoulou et al.2012 Canadian Recommendations for High BP
283
Table 9. Considerations in the individualization of antihypertensive therapy
Hypertension without other compelling indications (target BP < 140/90 mm Hg)Diastolic with or without systolic
hypertensionThiazide diuretics, !-blockers, ACE
inhibitors, ARBs, or long-actingCCBs (consider ASA and statins inselected patients). Considerinitiating therapy with acombination of first-line drugs if theBP is " 20 mm Hg systolic or " 10mm Hg diastolic above target
Combinations of first-linedrugs
Not recommended for monotherapy:#-blockers, !-blockers in those"60 years of age, ACE inhibitorsin blacks. Hypokalemia should beavoided in those prescribeddiuretic monotherapy. ACEinhibitors, ARBs, and direct renininhibitors are potential teratogens,and caution is required ifprescribing to women of child-bearing potential. Combinationof an ACE-inhibitor with an ARBis not recommended.
Isolated systolic hypertension without othercompelling indications
Thiazide diuretics, ARBs, or long-actingdihydropyridine CCBs
Combinations of first-linedrugs
Same as diastolic with or withoutsystolic hypertension
Diabetes mellitus (target BP < 130/80 mm Hg)Diabetes mellitus with microalbuminuria,*
ACE inhibitors or ARBs Addition ofdihydropyridine CCBis preferred overthiazide
A loop diuretic could be consideredin hypertensive CKD patientswith extracellular fluid volumeoverload
Diabetes mellitus not included in the abovecategory
ACE inhibitors, ARBs, dihydropyridineCCBs, or thiazide diuretics
Combination of first-linedrugs. If combinationwith an ACE inhibitoris being considered, adihydropyridine CCBis preferable tothiazide diuretic
Normal ACR ! 2.0 mg/mmol inmen and ! 2.8 mg/mmol inwomen
Cardiovascular disease (target BP < 140/90 mm Hg)Coronary artery disease ACE inhibitors or ARBs (except in low-
risk patients); !-blockers for patientswith stable angina
Long-acting CCBs. Whencombination therapy isbeing used for highrisk patients, an ACEinhibitor/dihydropyridineCCB is preferred
Avoid short-acting nifedipine.Combination of an ACEinhibitor with an ARB isspecifically not recommended
Recent myocardial infarction !-Blockers and ACE inhibitors (ARBs ifACE inhibitor-intolerant)
Long-acting CCBs if !-blockercontraindicated or noteffective
Nondihydropyridine CCBs shouldnot be used with concomitantheart failure
Heart failure ACE inhibitors (ARBs if ACE inhibitor-intolerant) and !-blockers.Aldosterone antagonists(mineralocorticoid receptorantagonists) may be added forpatients with a recent cardiovascularhospitalization, acute myocardialinfarction, elevated B-typenatriuretic peptide or N-terminal-proBNP level, or NYHA class II toIV symptoms
ACE inhibitor and ARBcombined.Hydralazine/isosorbidedinitrate combinationif ACE inhibitor andARB contraindicatedor not tolerated.Thiazide or loopdiuretics arerecommended asadditive therapy.Dihydropyridine CCB
Titrate doses of ACE inhibitors andARBs to those used in clinicaltrials. Carefully monitorpotassium and renal function ifcombining any of ACE inhibitor,ARB, and/or aldosteroneantagonist
Left ventricular hypertrophy ACE inhibitor, ARB, long-acting CCB,or thiazide diuretics.
Combination of additionalagents
Hydralazine and minoxidil shouldnot be used
Past stroke or TIA ACE inhibitor/diuretic combinations Combination of additionalagents
Treatment of hypertension shouldnot be routinely undertaken inacute stroke unless extreme BPelevation. Combination of anACE inhibitor with an ARB isnot recommended
Nondiabetic CKD (target BP < 140/90 mm Hg)Nondiabetic CKD with proteinuria† ACE inhibitors (ARBs if ACE inhibitor-
intolerant) if there is proteinuria.Diuretics as additive therapy
Combinations ofadditional agents
Carefully monitor renal function andpotassium for those taking anACE inhibitor or ARB.Combinations of an ACEinhibitor and ARB are notrecommended in patients withoutproteinuria
Renovascular disease Does not affect initial treatmentrecommendations
Combinations ofadditional agents
Avoid ACE inhibitors or ARB ifbilateral renal artery stenosis orunilateral disease with solitarykidney
284 Canadian Journal of CardiologyVolume 28 2012
ImplementationThe implementation task force conducts an extensive
knowledge translation effort to enhance uptake and applicabil-ity of these recommendations. These efforts briefly includeknowledge exchange forums, targeted educational materials forprimary care providers, as well as patients, and freely available slidekits and summary documents of all recommendations on the Ca-nadian Hypertension Society Web site (www.hypertension.ca).Documents are available in French and English, and some doc-uments are translated into other languages. The CHEP out-comes task force conducts hypertension surveillance studiesand review of existing Canadian health surveys to identify gapsbetween current and best practices. The implementation taskforce also regularly receives feedback from end users to improveguideline processes and content. Although the number of pri-mary care providers that directly receive CHEP materials on aregular basis has dramatically increased, CHEP is continuingto address the barrier and challenge of identifying and reachingall active primary care providers across Canada for dissemina-tion of CHEP materials.
Future DirectionsThe present report (see Table 9 for the summary of phar-
macological management of hypertension) represents the 13thiteration of the annually updated CHEP recommendations forthe management of hypertension, and we will continue to con-duct yearly systematic reviews of the clinical trial evidence toupdate our recommendations for therapy annually. The prev-alence of hypertension in Canada continues to increase and ispredicted to reach 7,500,000 people in 2012/2013 with over1000 people newly diagnosed with hypertension every day.53
Therefore, there is a need to focus our efforts on prevention ofhypertension, which is the CHEP theme for 2012. The overallgoal of the CHEP is to improve awareness, treatment, andcontrol of hypertension in Canada.
Funding SourcesThe CHEP process is sponsored by Hypertension Canada,
the College of Family Physicians of Canada, the CanadianPharmacy Association, the Canadian Council of Cardiovascu-lar Nurses, and the Heart and Stroke Foundation of Canada.CHEP members are unpaid volunteers. Although meetingsponsors are also stakeholders in the CHEP, the views or inter-
ests of the sponsors have not influenced the final recommen-dations.
DisclosuresDisclosures can be found in Supplemental Appendix S2
available online at www.onlinecj.ca.
References
1. Wolf-Maier K, Cooper RS, Kramer H, et al. Hypertension treatment andcontrol in five European Countries, Canada, and the United States. Hy-pertension 2004;43:10-7.
2. Wolf-Maier K, Cooper RS, Banegas JR, et al. Hypertension prevalenceand blood pressure levels in 6 European countries, Canada, and theUnited States. JAMA 2003;289:2363-9.
3. Wilkins K, Campbell NR, Joffres MR, et al. Blood pressure in Canadianadults. Health Rep 2010;21:37-46.
4. Kannel WB. Blood Pressure as a cardiovascular risk factor: prevention andtreatment. JAMA 1996;275:1571-6.
5. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable riskfactors associated with myocardial infarction in 52 countries (the INTER-HEART study): case-control study. Lancet 2004;364:937-52.
6. Hackam DG, Khan NA, Hemmelgarn BR, et al. The 2010 CanadianHypertension Education Program recommendations for the managementof hypertension: part 2 - therapy. Can J Cardiol 2010;26:249-58.
7. Khan NA, Hemmelgarn B, Herman RJ, et al. The 2008 Canadian Hy-pertension Education Program recommendations for the management ofhypertension: part 2 - therapy. Can J Cardiol 2008;24:465-75.
8. Khan NA, Hemmelgarn B, Herman RJ, et al. The 2009 Canadian Hy-pertension Education Program recommendations for the management ofhypertension: part 2–therapy. Can J Cardiol 2009;25:287-98.
9. Khan NA, McAlister FA, Campbell NRC, et al. The 2004 Canadianrecommendations for the management of hypertension: part II - therapy.Can J Cardiol 2004;20:41-54.
10. Khan NA, McAlister FA, Lewanczuk RZ, et al. The 2005 Canadian Hy-pertension Education Program recommendations for the management ofhypertension: part II - therapy. Can J Cardiol 2005;21:657-72.
11. Khan NA, McAlister FA, Rabkin SW, et al. The 2006 Canadian Hyper-tension Education Program recommendations for the management ofhypertension: part II - therapy. Can J Cardiol 2006;22:583-93.
Other conditions (target BP < 140/90 mm Hg)Peripheral arterial disease Does not affect initial treatment
recommendationsCombinations of
additional agentsAvoid !-blockers with severe disease
Dyslipidemia Does not affect initial treatmentrecommendations
Combinations ofadditional agents
—
Overall vascular protection Statin therapy for patients with 3 ormore cardiovascular risk factors oratherosclerotic disease. Low doseASA in patients with controlled BP
— Caution should be exercised with theASA recommendation if BP is notcontrolled
*Albuminuria is defined as persistent ACR ! 2.0 mg/mmol in men and ! 2.8 mg/mmol in women.† Proteinuria is defined as urinary protein ! 500 mg per 24 hours or ACR ! 30 mg/mmol.
Reprinted with permission of the Canadian Hypertension Education Program.
Daskalopoulou et al.2012 Canadian Recommendations for High BP
285
12. Khan NA, Hemmelgarn BR, Padwal R, et al. The 2007 Canadian Hyper-tension Education Program recommendations for the management ofhypertension: part 2 - therapy. Can J Cardiol 2007;23:539-50.
13. Padwal RJ, Hemmelgarn BR, Khan NA, et al. The 2008 Canadian Hy-pertension Education Program recommendations for the management ofhypertension: part 1 - blood pressure measurement, diagnosis and assess-ment of risk. Can J Cardiol 2008;24:455-63.
14. Padwal RS, Hemmelgarn BR, Khan NA, et al. The 2009 Canadian Hy-pertension Education Program recommendations for the management ofhypertension: part 1–blood pressure measurement, diagnosis and assess-ment of risk. Can J Cardiol 2009;25:279-86.
15. Padwal RS, Hemmelgarn BR, McAlister FA, et al. The 2007 CanadianHypertension Education Program recommendations for the managementof hypertension: part 1 - blood pressure measurement, diagnosis, andassessment of risk. Can J Cardiol 2007;23:529-38.
16. Quinn RR, Hemmelgarn BR, Padwal RS, et al. The 2010 Canadian Hy-pertension Education Program recommendations for the management ofhypertension: part 1 - blood pressure measurement, diagnosis and assess-ment of risk. Can J Cardiol 2010;26:241-8.
17. Rabi DM, Daskalopoulou SS, Padwal RS, et al. The 2011 CanadianHypertension Education Program recommendations for the managementof hypertension: blood pressure measurement, diagnosis, assessment ofrisk, and therapy. Can J Cardiol 2011;27:415-33.
18. Zannad F, McMurray JJ, Krum H, et al. Eplerenone in patients withsystolic heart failure and mild symptoms. N Engl J Med 2011;364:11-21.
19. Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosteroneblocker, in patients with left ventricular dysfunction after myocardial in-farction. N Engl J Med 2003;348:1309-21.
20. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone onmorbidity and mortality in patients with severe heart failure. Random-ized Aldactone Evaluation Study Investigators. N Engl J Med 1999;341:709-17.
21. Yusuf S, Healey JS, Pogue J, et al. Irbesartan in patients with atrial fibril-lation. N Engl J Med 2011;364:928-38.
22. Goette A, Schon N, Kirchhof P, et al. Angiotensin II-Antagonist in Par-oxysmal Atrial Fibrillation (ANTIPAF)-Trial. Circ Arrhythm Electro-physiol 2012;5:43-51.
23. Disertori M, Latini R, Barlera S, et al. Valsartan for prevention of recur-rent atrial fibrillation. N Engl J Med 2009;360:1606-17.
24. Wright JT Jr, Bakris G, Greene T, et al. Effect of blood pressure loweringand antihypertensive drug class on progression of hypertensive kidneydisease: results from the AASK trial. JAMA 2002;288:2421-31.
25. Norris K, Bourgoigne J, Gassman J, et al. Cardiovascular outcomes in theAfrican American Study of Kidney Disease and Hypertension (AASK)Trial. Am J Kidney Dis 2006;48:739-51.
26. Appel LJ, Wright JT Jr, Greene T, et al. Intensive blood-pressure controlin hypertensive chronic kidney disease. N Engl J Med 2010;363:918-29.
27. Ruggenenti P, Perna A, Loriga G, et al. Blood-pressure control for reno-protection in patients with non-diabetic chronic renal disease (REIN-2):multicentre, randomised controlled trial. Lancet 2005;365:939-46.
28. Klahr S, Levey AS, Beck GJ, et al. The effects of dietary protein restrictionand blood-pressure control on the progression of chronic renal disease.Modification of Diet in Renal Disease Study Group. N Engl J Med 1994;330:877-84.
29. Sarnak MJ, Greene T, Wang X, et al. The effect of a lower target bloodpressure on the progression of kidney disease: long-term follow-up of the
Modification of Diet in Renal Disease study. Ann Intern Med2005;142:342-51.
30. Bangalore S, Kumar S, Lobach I, Messerli FH. Blood pressure targets insubjects with type 2 diabetes mellitus/impaired fasting glucose: observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials. Circulation 2011;123:2799-810, 9.
31. Reboldi G, Gentile G, Angeli F, Ambrosio G, Mancia G, Verdecchia P.Effects of intensive blood pressure reduction on myocardial infarction andstroke in diabetes: a meta-analysis in 73,913 patients. J Hypertens 2011;29:1253-1269.
32. National High Blood Pressure Education Program Working Group reporton primary prevention of hypertension. Arch Intern Med 1993;153:186-208.
33. McAlister FA. The Canadian Hypertension Education Program–a uniqueCanadian initiative. Can J Cardiol 2006;22:559-64.
34. Beckett L, Godwin M. The BpTRU automatic blood pressure monitorcompared to 24 hour ambulatory blood pressure monitoring in the assess-ment of blood pressure in patients with hypertension. BMC CardiovascDisord 2005;5:18-23.
35. White WB, Anwar YA. Evaluation of the overall efficacy of the Omronoffice digital blood pressure HEM-907 monitor in adults. Blood PressMonit 2001;6:107-10.
36. Wright JM, Mattu GS, Perry TL Jr, et al. Validation of a new algorithmfor the BPM-100 electronic oscillometric office blood pressure monitor.Blood Press Monit 2001;6:161-5.
37. Stergiou GS, Bliziotis IA. Home blood pressure monitoring in the diag-nosis and treatment of hypertension: a systematic review. Am J Hypertens2011;24:123-34.
38. Warren RE, Marshall T, Padfield PL, Chrubasik S. Variability of office,24-hour ambulatory, and self-monitored blood pressure measurements.Br J Gen Pract 2010;60:675-80.
39. Coll de Tuero G, Llibre JB, Poncelas AR, et al. Isolated clinical hyperten-sion diagnosis: self-home BP, ambulatory BP monitoring, or both simul-taneously? Blood Press Monit 2011;16:11-5.
40. Bobrie G, Chatellier G, Genes N, et al. Cardiovascular prognosisof “masked hypertension” detected by blood pressure self-measurement in elderly treated hypertensive patients. JAMA 2004;291:1342-9.
41. Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure ofreduced dietary sodium and the Dietary Approaches to Stop Hypertension(DASH) diet. DASH-Sodium Collaborative Research Group. N EnglJ Med 2001;344:3-10.
42. Moore TJ, Vollmer WM, Appel LJ, et al. Effect of dietary patterns onambulatory blood pressure: results from the Dietary Approaches to StopHypertension (DASH) Trial. DASH Collaborative Research Group. Hy-pertension 1999;34:472-7.
43. Karanja NM, Obarzanek E, Lin PH, et al. Descriptive characteristics ofthe dietary patterns used in the Dietary Approaches to Stop HypertensionTrial. DASH Collaborative Research Group. J Am Diet Assoc 1999;99(suppl 8):S19-S27.
44. Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects ofdietary patterns on blood pressure. DASH Collaborative Research Group.N Engl J Med 1997;336:1117-24.
45. McAlister FA, Straus SE, Sackett DL, Altman DG. Analysis and reportingof factorial trials: a systematic review. JAMA 2003;289:2545-53.
46. Food and Drug Administration. FDA Drug Safety Communication: Noincrease in risk of cancer with certain blood pressure drugs – Angiotensine
286 Canadian Journal of CardiologyVolume 28 2012
Receptor Blockers (ARBs). Drug Safety and Availability 2011 March 6.Available at: http://www.fda.gov/Drugs/DrugSafety/ucm257516.htm#sa. Accessed January 20, 2012.
47. Sever PS, Dahlof B, Poulter NR, et al. Prevention of coronary and strokeevents with atorvastatin in hypertensive patients who have average or low-er-than-average cholesterol concentrations, in the Anglo-ScandinavianCardiac Outcomes Trial - Lipid Lowering Arm (ASCOT-LLA): a multi-centre randomised controlled trial. Lancet 2003;361:1149-58.
48. Genest J, McPherson R, Frohlich J, et al. 2009 Canadian CardiovascularSociety/Canadian guidelines for the diagnosis and treatment of dyslipide-mia and prevention of cardiovascular disease in the adult - 2009 recom-mendations. Can J Cardiol 2009;25:567-79.
49. Peterson JC, Adler S, Burkart JM, et al. Blood pressure control, protein-uria, and the progression of renal disease. The Modification of Diet inRenal Disease Study. Ann Intern Med 1995;123:754-62.
50. Bangalore S, Kumar S, Lobach I, Messerli FH. Blood pressure targets insubjects with type 2 diabetes mellitus/impaired fasting glucose: observa-
tions from traditional and bayesian random-effects meta-analyses ofrandomized trials. Circulation 2011;123:2799-810, 9 p following 810.
51. Reboldi G, Gentile G, Angeli F, et al. Effects of intensive blood pressurereduction on myocardial infarction and stroke in diabetes: a meta-analysisin 73,913 patients. J Hypertens 2011;29:1253-69.
52. Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-85.
53. Robitaille C, Dai S, Waters C, et al. Diagnosed hypertension in Can-ada: incidence, prevalence and associated mortality. CMAJ 2012;184:E49-E56.
Supplementary MaterialTo access the supplementary material accompanying this arti-
cle, visit the online version of the Canadian Journal of Cardiology atwww.onlinecjc.ca, and at doi:10.1016/j.cjca.2012.02.018.
Daskalopoulou et al.2012 Canadian Recommendations for High BP