28
Handling over medical care of adolescents to adult teams safely Mignon McCulloch Red Cross Hospital, University of Cape Town Evelina Children’s Hospital (Guys’…and St Thomas’…and King’s )
| Date post: | 31-Dec-2015 |
| Category: |
Documents |
| Upload: | marion-horton |
| View: | 216 times |
| Download: | 2 times |

Handling over medical care of adolescents to adult
teams safelyMignon McCulloch Red Cross Hospital, University of Cape Town Evelina Children’s Hospital (Guys’…and St Thomas’…and King’s )
Introduction
Transition challenges Paediatric and Adult services
Developing countries failure of transplanted kidneys due to non-adherence to:– Medication– Follow-up
NO further renal replacement
‘1 strike and you’re out’
‘Crazy’ cut-off at 13years
Transition is defined as…..
“……a purposeful, planned movement of adolescents with chronic physical and
medical conditions from child centered to adult-oriented healthcare systems”
American Society for Adolescent Medicine 1993
“…. A guided educational, therapeutic process, rather than an administrative event”
UK DOH 2003
• Idealistic• Individual• Immature• Irrational• Invincible• Immortal• Immune• Infertile
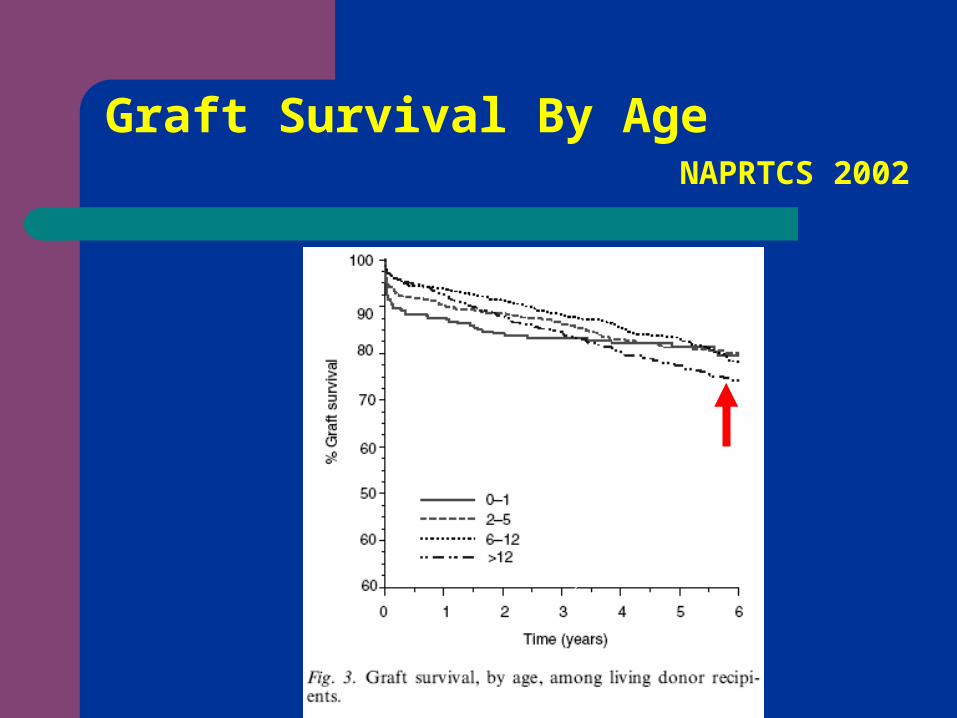
Graft Survival By AgeNAPRTCS
2002
Models of Transition
A dedicated follow-up service provided within adult setting without a combined paediatric-adult clinic and with no direct input or continuity from paediatric services
A ‘seamless’ clinic which begins in childhood or adolescence and continues into adulthood, with both child and adult professionals providing ongoing care as appropriate.
Life-long follow-up within the paediatric setting
Paediatric vs. Adult Care
• Parent focussed• Dependent• Younger kids!• Personal• Bustling & loud• Fun• Large team
•Individual focussed
•Independent
•Elderly patients
•Impersonal
•Quiet and Serious
•Small Team
Transplant Clinics ECH vs. Guys Adults
• 80 transplant patients
2 nephrologists in clinic
1 Clinical Nurse Specialist(CNS)
Clinic held daily; 10 slots
1000 transplant patients
7 nephrologists & 2 surgeons in clinic
2 CNS & nursing team
Clinic with up to 100 appointment slots

“In whatever healthcare setting it is delivered; services need to be
appropriate for both chronological age and development attainment”
Society of Adolescent Medicine 2003

What Does Successful Transition Need?
• Young people!! • Commitment• Planning• Resources
‘‘Collaborating, health professionals who demonstrate ‘mutual professional
respect’’
Watson 2006
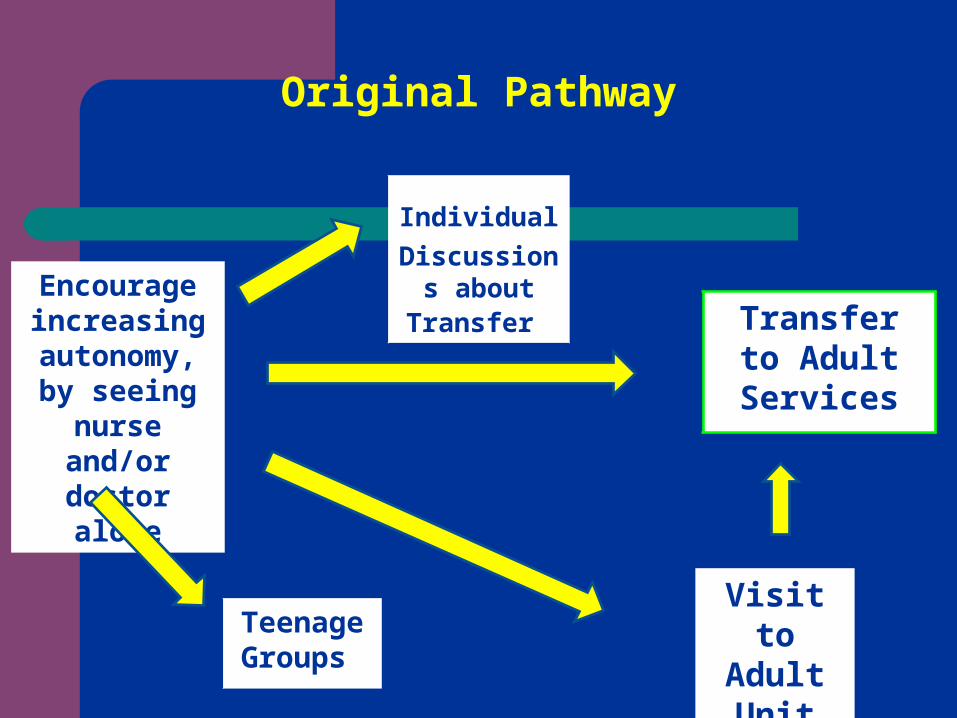
Original Pathway
Encourage increasing autonomy, by seeing
nurse and/or doctor alone
Individual
Discussions about
Transfer
Teenage
Groups
Transfer to Adult
Services
Visit to Adult Unit
Objective
Review of Adolescent Clinic at Groote Schuur Hospital(GSH) 2002-2009
Support from Red Cross Hospital(RXH) doctors and clinical social worker
Development of Adolescent Transition Service requires:
Link person in Adult unit – ‘Champion’
Committed Doctor – remembers what it is like to be a teenager?
Nursing staff – Sr ‘Golly’
Social worker + psychologist
Commitment from Administrators
Adult units HUGE
Paeds Renal Transplants– 44 patients
Adult Renal Transplants – 400 patients

Patients seen in last 2 years @ GSH
0
2
4
6
8
10
J F M A M J J A S O N D
2008
2009
Month per year
Nos
of
pats
per
clin
ic

Results of Program 2002 - 2009
Nos of Adolescents transferred GSH
19
Nos received re-transplant 2
Nos awaiting transplant 2
Nos died after transfer 2
Nos lost to follow-up 0
Deaths at RXH
7 patients in last 5 years died at RXH during adolescent years >13 years of age
Not reflected on the Adolescent stats previous slide

RXH
Active decision NOT to ‘re-list’ some patients
Not transferring those patients
Allowing to stay in ‘familiar environment’ during end-stage disease
Holding back those deemed ‘not ready’ medically or psychosocially
Psychology input
Separate monthly groups at GSH for – Parents/Carers– Adolescents
Motivational events– ‘Graduation ‘ lunches– Welcome meetings/tours at Adult unit

Medically
Don’t transfer in crisis
Making more decisions NOT to transfer
Keeping older patients @ RXH as limitation of slots on adult side
Allocation of organs doesn’t mirror this
Where are we know?
Initially aimed at transitioning backlog of older adolescents(18-21year olds)
Then proceeding to 16-18year olds
Now working with younger groups
Generic Adolescent Workshops
Younger group 13 – 15 year olds of all disciplines with chronic implications
68 Parents and patients attended workshop at April 2009 RXH
Topics addressed
Pregnancy and Contraceptive advice– Termination of pregnancy– Drugs affecting foetus – AECI’s
Recreational drugs and alcohol Crime Non-adherence/compliance/concordance
– Do you take your meds ? how many times per week do you forget?

‘Embarrassing moments’
Group support
Medical intervention
Cultural beliefs
Successful times
What is our Collaboration?
• Long term approach• Named individuals • Communication • Adult team in paediatric clinic • Timing of transfer • Paediatric team in adult clinic• Young adult services
Conclusions
Successful adolescent transition is possible
BUT: Requires significant staff input
Ideally medically stable at transfer
Adolescents/Young Adult Clinic
Real life dilemmas
How do you manage if medical and nursing staff think ‘adolescents’ are not useful members of the community as ‘no dependants’?
Social worker feels their role is only in securing grants?
Administrators insist on transition at 13 years?

















