50
Hemodialysis adequacy & Outcome: from NCDS to HEMO & MPO Saeed M.G Al-GHAMDI, FRCPC, FACP King Faisal Specialist Hospital & Research Center-Jeddah
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | jonas-hood |
| View: | 222 times |
| Download: | 6 times |

Hemodialysis adequacy & Outcome: from NCDS to HEMO & MPO
Saeed M.G Al-GHAMDI, FRCPC, FACPKing Faisal Specialist Hospital &
Research Center-Jeddah

Beginning of Hemodialysis

LOWRIE EG; LAIRD NM, PARKER TF; SARGENT JANEW ENGLAND JOURNAL OF MEDICINE 1981 NOVEMBER 12;305(20): 1176-81
National Cooperative Dialysis Study NCDS

Effect of hemodialysis prescription of patients morbidity: Report of NCDS
• 151 patients • 4 treatment groups – Long dialysis– Short dialysis – High time-average urea concentration – Low time-average urea concentration
• Protein intake was not restricted
Lowerie EG, et al, N Engl J Med 1981, Nov, 12; 305(20): 1176-81

NCDS: Results
• No difference in mortality between groups• Withdrawal was higher in the high urea group• Hospitalization was higher in higher urea
group • Morbidity was higher in the high ATC-urea • Morbidity may be decreased by prescription
associated with more efficient removal of urea if adequate protein intake
Lowerie EG, et al, N Engl J Med 1981, Nov, 12; 305(20): 1176-81

Mechanistic analysis of NCDS
• Gotch used NCDS data and introduced kt/v of urea – Efficiency of urea removal (small toxins)– Dietary protein intake
• Kt/v is an important measure of clinical outcome
Gotch, FA, Sargent,JA KI 1985; 28: 526-534

Kt/v: Single pool Vs double pool
• Urea is equilibrated between muscles and plasma water
• Single pool kt/v (non- equilibrated): blood urea is measured at end of dialysis from circuit
• Double pool kt/v (equilibrated): venous sample post dialysis (30 minutes)
• Single pool kt/v is 0.20 higher than double pool

Kt/v: Practice & Recommendations
• Slow the pump to 100 ml/minute • Obtain urea sample 15 seconds later • Target kt/v of 1.2 (URR of 65%)• The mean delivered sp-kt/v in USA: 1.5, more
than 90% above 1.2• The mean kt/v in Europe: 1.28-1.5
KDOQI , AJKD 2006, EBPG, NDT 2002USRDS 2007, EBPG, DOPPS 2004
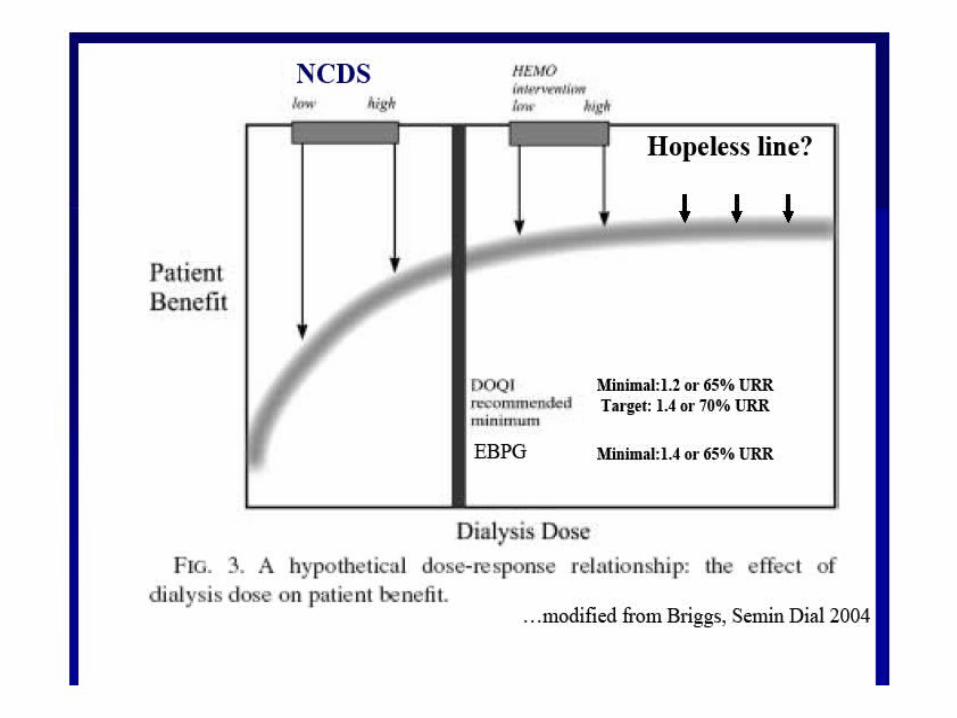
Optimal Dialysis dose
• Is the summation of clinical and biochemical parameters which refer to the adequately delivered dose of dialysis , in which patient has no symptoms which could be attributed to under-dialysis and more importantly, to a measurable value at which the dialysis patient has the lowest morbidly and mortality

High kt/v: Positive observational studies
• Survival in long-term hemodialysis patients: results from the annual survey of the Japanese society of dialysis therapy. Shinazato et al, NDT 1997; 12:884-8
• Body size, dose of hemodialysis and mortality. Wolfe RA et al, AJKD 2000; 35: 80-88
• Dialysis dose and body mass index are strongly associated with survival in hemodialysis patients. Port FK, et al, JASN 2002; 13: 1061-6

High kt/v: negative observational study
• The dose of hemodialysis and patient mortality. Held PJ et al, KI 1996; 50:550-6

Effect of Dialysis Dose and Membrane Flux in Maintenance Hemodialysis
HEMO study
Eknoyan G et al New Engl J Medicine 2002; 347: 2010
HEMO study: Design
• 1846 prevalent patients in 72 dialysis units in USA
• RCT: mean follow up of 2.8 year • Two-by-two factorial design – Standard dose: sp- kt/v 1.25 or URR 65% – High dose: sp-kt/v 1.65 or URR of 75%– Low-flux – High-flux

HEMO study: Outcomes
• Primary outcome: – Death from any cause
• Secondary outcome:– Rate of hospitalizations (excluding access)– Composite outcome• First hospitalization from cardiac cause or death from
any cause (ACM)• First hospitalization from infectious cause or death • First decline of 15% in serum albumin from baseline
value or death

HEMO Study Eknoyan G et al New Engl J Medicine 2002; 347: 2010

HEMO Study Eknoyan G et al New Engl J Medicine 2002; 347: 2010

HEMO Study : Primary outcomeEknoyan G et al New Engl J Medicine 2002; 347: 2010

HEMO Study Eknoyan G et al New Engl J Medicine 2002; 347: 2010
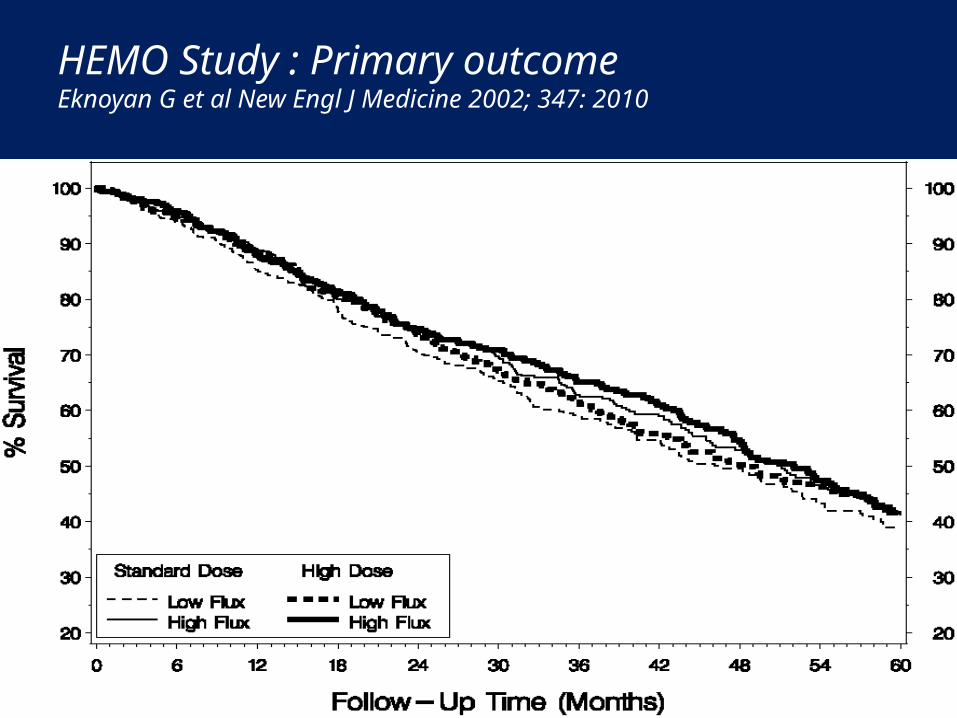
HEMO Study : Primary outcomeEknoyan G et al New Engl J Medicine 2002; 347: 2010

HEMO Study : Secondary outcomeEknoyan G et al New Engl J Medicine 2002; 347: 2010
HEMO conclusion: Primary outcome
• Neither the difference between the two dose groups nor the difference between flux groups were significant
• After adjustment of base-line factors– High dose group: risk of death 4% lower P= 0.53– High-flux group: risk of death 8% lower P= 0.23

HEMO conclusion: Secondary outcomes
• The risk of main secondary outcome was the same for both dialysis dose groups and for both flux groups.
HEMO study: Conclusion
• Among patients undergoing maintenance hemodialysis who were receiving thrice-weekly treatment lasting 2.5-4.5 hours each, neither a higher dose nor the use of high-flux membranes significantly improved survival or reduced morbidity
• This support the current guidelines of single-pool kt/v of 1.2-1.4 , and make no recommendation for or against routine use of high-flux membranes

HEMO study: Subgroup analysis
• In high-flux there is significant reduction in RR of death (20%) from cardiac causes and combined outcome of first hospitalization or death from cardiac cause
• Longer dialysis duration– High-flux dialysis for > 3.7 year has 32% lower risk
of death when compared with low-flux
Cheung A, et al , JASN 2003; 14: 3251-63

HEMO Study: Subgroup analysis
• Sex and dialysis dose– Women with high dose has 19% lower risk of
death– Men with high dose has 16% higher risk of death
• Beta-2-microglobulin: serum level correlated with mortality particularly from infectious causes
Effect of Membrane Permeability on Survival of Hemodialysis Patients
(MPO Study)Locatelli F, Martin-Malo A, Hannedouche T, Loureiro A, Papadimitriou M, Wizemann V,
Jacobson SH, Czekalski S, Ronco C, Vanholder R , JASN 2009; 20: 645-654
MPO: Hypothesis
• Mortality in dialysis patients 24% in USA and 14-26% in Europe
• Retention of high MW molecules may be implicated in the high mortality
• High-flux membranes can remove those molecules
• Epidemiologic data suggested benefits• Only one underpowered RCT which did not
show benefit

MPO Study: Design
• RCT: 59 European study centers• 738 incident hemodialysis patients – Follow up from 3-7.5 years (mean 3 year)
• Patients were randomized to receive high or low-flux membrane according to – Low albumin <4 g/dl (567 patients)– Normal albumin > 4 g/dl (171 patients)
• Minimal single-pool kt/v of 1.2

MPO study; Methodology
Locatelli, F. et al. J Am Soc Nephrol 2009;20:645-654

MPO study: Results: Kaplan-Meier survival curves for the complete intention-to-treat population (Log-rank test P = 0.214) Locatelli, F. et al. J Am Soc Nephrol 2009;20:645-654
Locatelli, F. et al. J Am Soc Nephrol 2009;20:645-654
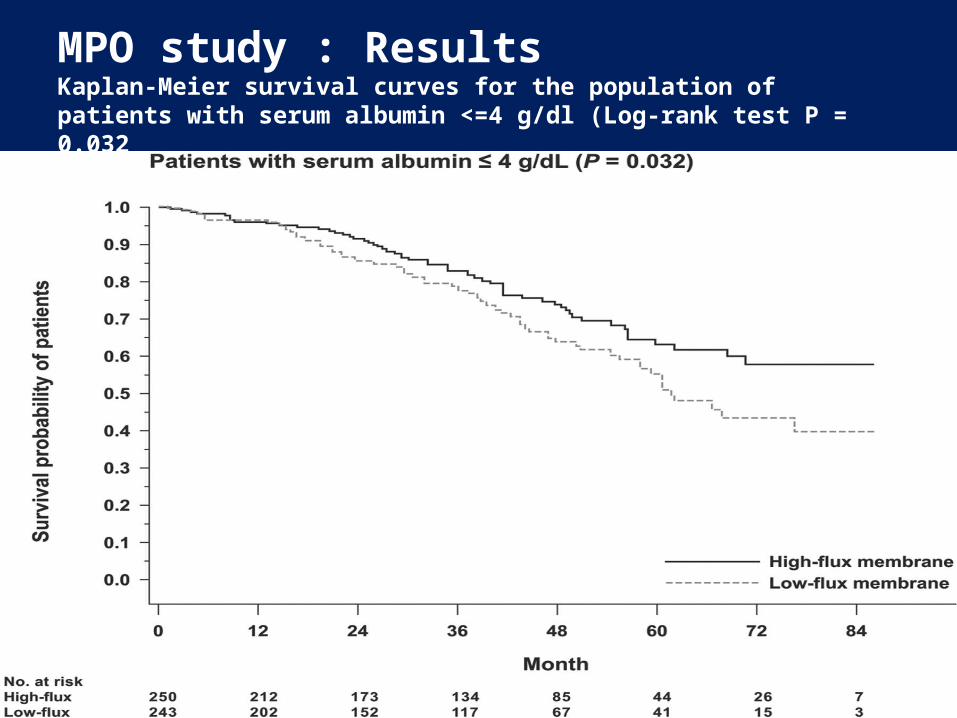
MPO study : Results Kaplan-Meier survival curves for the population of patients with serum albumin <=4 g/dl (Log-rank test P = 0.032

MPO study : Results Kaplan-Meier survival curves for the subpopulation of patients with diabetes (Log-rank test P = 0.039) Locatelli, F. et al. J Am Soc Nephrol 2009;20:645-654

MPO study: Results Locatelli, F. et al. J Am Soc Nephrol 2009;20:645-654

MPO: Conclusions
• No significant effect of permeability on survival was found in the population as a whole
• High-flux showed significant survival benefit in high risk population (RR reduction of 37%)
• High-flux showed significant survival benefit in diabetics (adjusted risk reduction of 38%)

HEMO & MPO: Differences
MPO HEMO
EuropeMembrane flux in high risk
groups
USADialysis dose
Membrane flux
RCT
Incident patients Mostly Prevalent patients Enrollment yes no Risk stratification
3-7 year (3 y) 2.8 years Duration

How can we decrease morbidity and mortality in HD patients?

How can we reduce morbidity and mortality in HD patients?
• Attention to traditional and non-traditional risk factors– Anemia – Hypertension – CKD-MBD
• Individualization of dialysis therapy– High flux for high risk group or non-transplant
patients – High dose kt/v for women

Future attempt to lower M&M
• More refinement of our dialysis prescription – Treatment Time – Daily dialysis or Quotidian
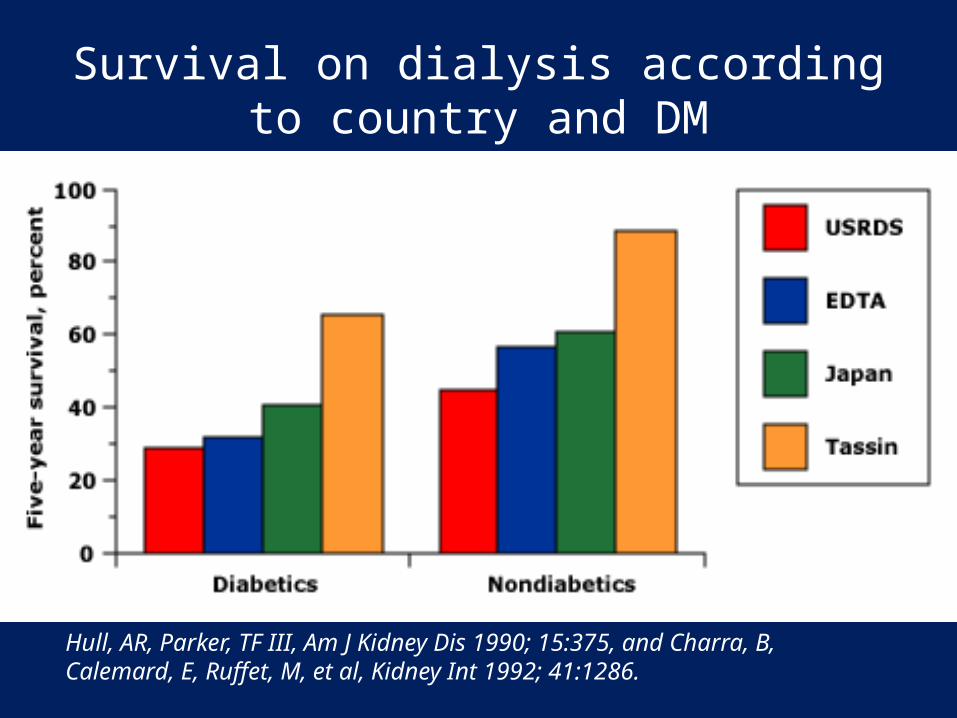
Survival on dialysis according to country and DM
Hull, AR, Parker, TF III, Am J Kidney Dis 1990; 15:375, and Charra, B, Calemard, E, Ruffet, M, et al, Kidney Int 1992; 41:1286.








Conclusions
• Targeting high kt/v has no significant impact on mortality, and the current kt/v >1.2 is still holding
• High-flux membrane might be of benefit in high risk group and in chronic HD patients
• Longer treatment time of dialysis probably is more important than kt/v
• CKD-MBD has major impact on morbidity and mortality
Conclusion
• The focus to reduce morbidity and mortality may be directed to lowering traditional and non-traditional risk factors in dialysis population

Thank You

















