HIV Clinical trials at MRC CTU. MRC CTU focus is on long-term large size clinical trials yielding definitive results that may result in changes in clinical practice Ongoing studies New study networks: INSIGHT and European networks Planned new studies. BACKGROUND. - PowerPoint PPT Presentation
80
HIV Clinical trials at MRC CTU • MRC CTU focus is on long- term large size clinical trials yielding definitive results that may result in changes in clinical practice –Ongoing studies –New study networks: INSIGHT and European networks –Planned new studies
Transcript
HIV Clinical trials at MRC CTU
• MRC CTU focus is on long-term large size clinical trials yielding definitive results that may result in changes in clinical practice–Ongoing studies–New study networks: INSIGHT and
European networks–Planned new studies
BACKGROUND
• ESPRIT is an international, phase III, open-label, randomized trial
• To compare the effects of subcutaneous rIL-2 and no rIL-2 on HIV disease progression and death
• HIV-1 patients with absolute CD4+ counts 300/ul at baseline who are taking combination antiretroviral therapy (ART)
• 3 mandatory cycles of rIL-2 then cycling to maintain CD4+ > double baseline or 1,000/ul
• Primary end points: HIV progression of disease, death.
ESPRIT: SUMMARY
• 247 sites in 25 countries• 4,150 patients recruited; 356 (9%) in UK NTCC• 2,090 patients randomised to rIL-2: 183 (9%) in UK
NTCC• 320 end-points required
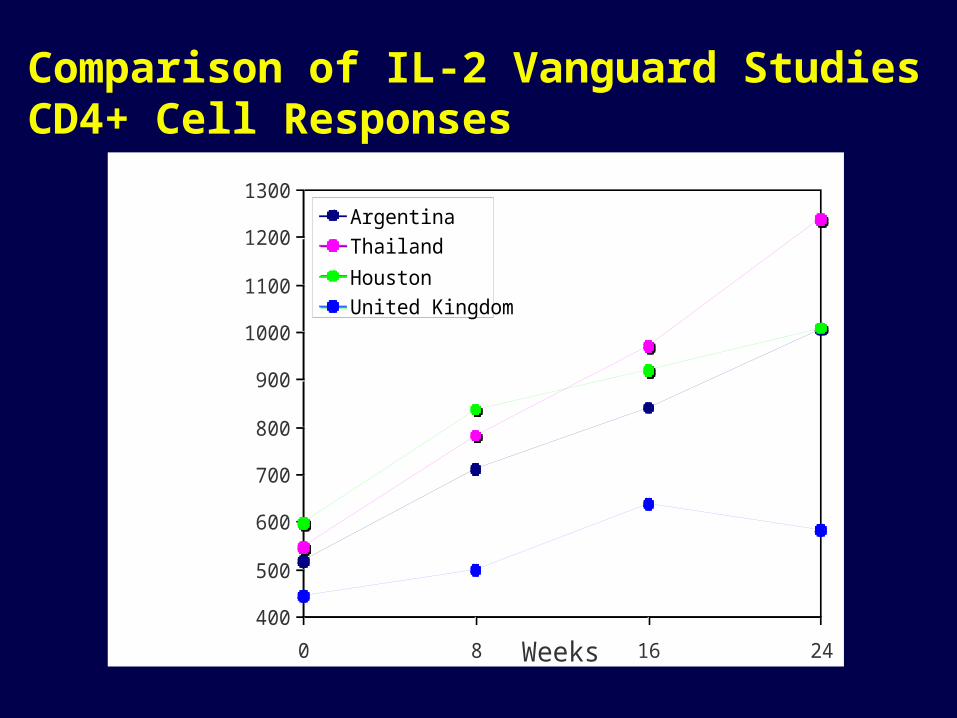
Median Change in CD4 Cell Count from Baseline with Inter-Quartile Range
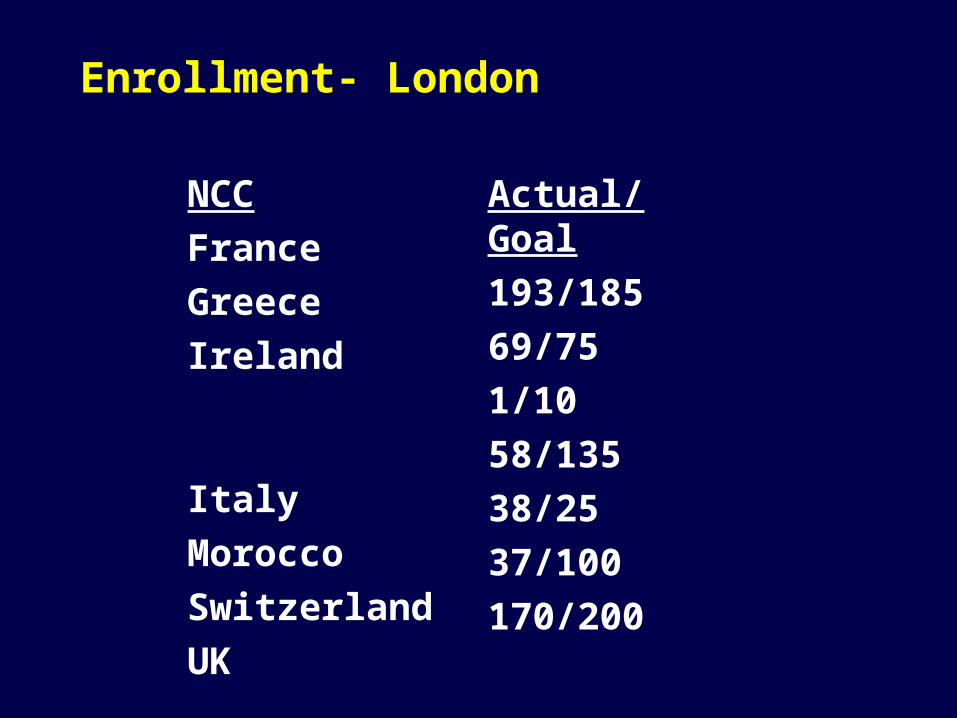
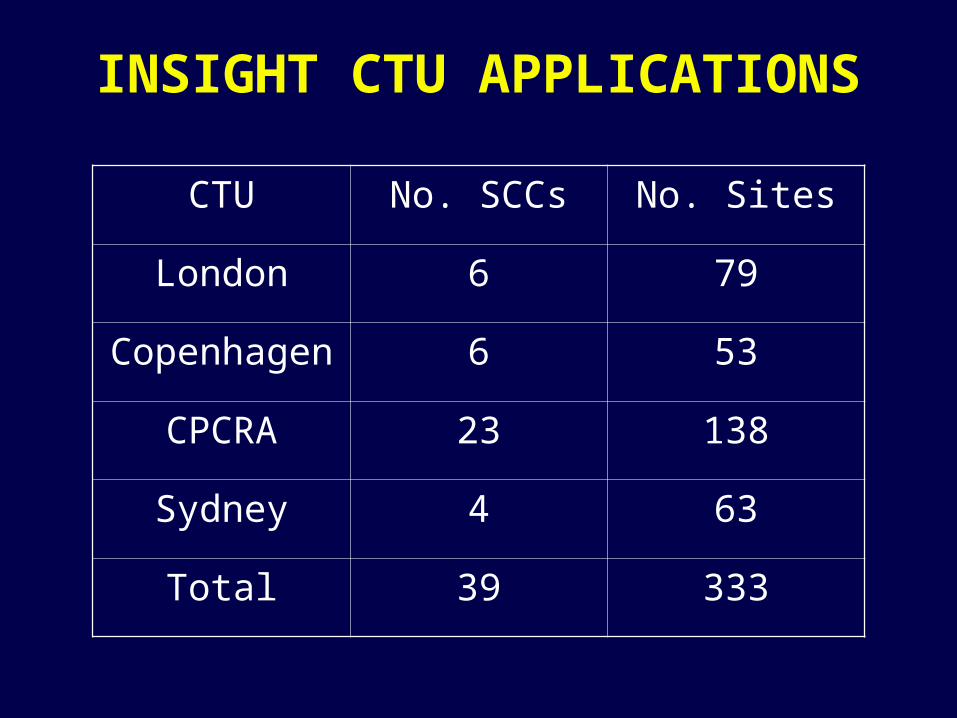
• London RCC 15 100– Italy 5 30 – Morocco 1 10– United Kingdom 9 60
• Minneapolis/CPCRA RCC 10 92– Brazil 2 20– CPCRA 3 31– DVA 2 11– Houston 2 15– NIH 1 15
TOTAL 61 541
Timeline
May 2005 – Protocol Version 1 available– Invitation letter distributed
June - July 2005– CRFs completed– Protocol Information Manual completed
July 2005– First STALWART training occurs
August 2005– First patient enrolled
SMART or STALWART?
SMART–the right choice for those who are willing to
take a 50/50 chance of starting ARVs now
STALWART–the right choice for those who want to
postpone starting ARVs and see what IL-2 will do versus waiting
SPARTAC TRIAL= Short Pulse Anti-Retroviral Treatment At seroConversion
An International Randomised Controlled Trial of Treatment at Primary HIV-1 infection
International trial recruiting from Australia, Brazil, Ireland, Italy, South Africa,
Uganda and UK
British HIV Association guidelines state:
“There is still no answer to the question of whether treatment at an early stage will influence the longer-term natural history.
Given the present lack of clarity, it remains reasonable to consider treating primary HIV infection, ideally within a clinical trial”
Primary study question
Does treatment of Primary HIV infection delay damage to the immune system and consequently time to starting long-term
anti-HIV therapy?
Scientific rationale for the study
• Early treatment may preserve HIV-specific immunity before irreversible damage occurs
• May be no gain in treating early, so better to delay treatment to reduce toxicity and possible resistance
• No randomised trials on effect of HAART on primary HIV infection
• Pilot studies have shown immune system may benefit from early treatment but unable to show whether this delays damage to immune system in the long term.
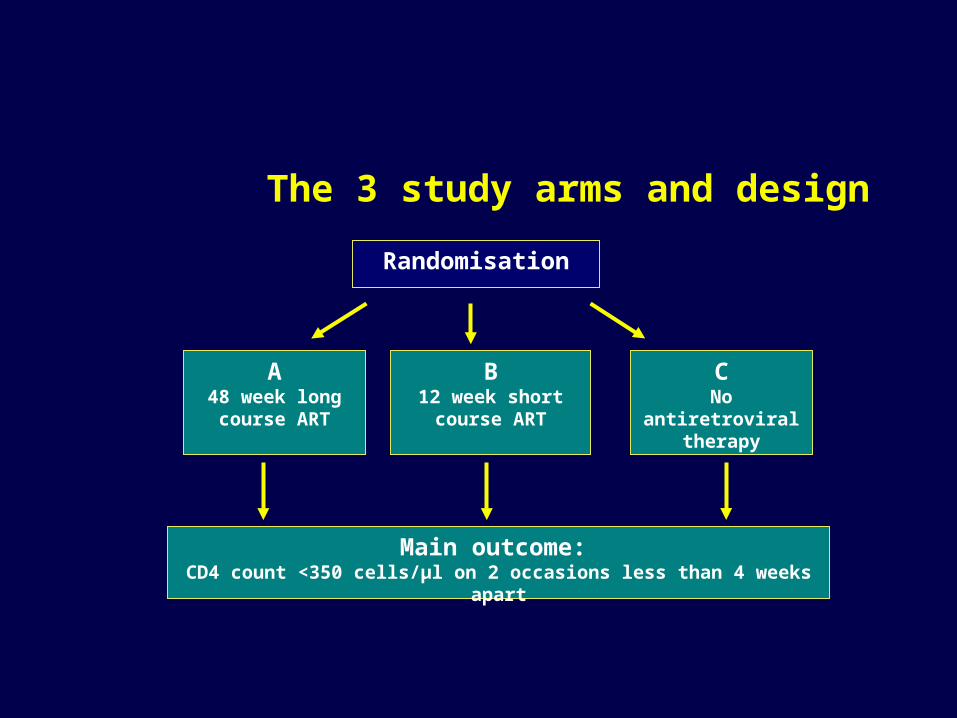
The 3 study arms and design
Randomisation
A48 week long course ART
B12 week short
course ART
CNo
antiretroviral therapy
Main outcome: CD4 count <350 cells/μl on 2 occasions less than 4 weeks
apart
Secondary study questions
Does treatment of Primary HIV infection have an effect on:
HIV-specific immune response?
Progression to AIDS?
Virological failure of long-term therapy?
Drug resistance?
Inclusion criteria
• Patient reached age of consent
• Patient able and willing to give written informed consent
• Patient confirmed Primary HIV Infection by at least one of the 5 criteria for PHI
Anti-HIV regimen at PHI
• Recommend Combivir and Kaletra but other regimens allowed
• Following this intervention at PHI, all patient will cease treatment.
•If disease progression necessitates treatment, anti-HIV drugs will be introduced according to the local standards of care.
Recruitment
• Sample size = 360
• Recruitment over 18 months
• Patients seen every 12 weeks
• Total duration of trial is 5 years
Current Status of SPARTAC Trial
70 patients recruited to date
Sites set up:
• 8 in UK (7 in London, 1 in Brighton)
• 1 in Ireland (Dublin)
• 1 in Johannesburg
• 10 in Australia (Sydney and Melbourne)
• 1 in Italy
Awaiting set up:
• Durban, Cape Town, Uganda, Brazil
International Network for Strategic
Initiatives in Global HIV Trials
INSIGHT
Response to NIH RFA for adult clinical trial networks
Mission of INSIGHT
To develop strategies for the optimization of treatment -- ART, immunomodulatory therapies, and interventions to prevent and treat the complications of HIV and ART – in order to prolong disease-free survival in an demographically, socio-economically, and geographically diverse group of individuals with HIV.
Relationship of the Key Groups in the INSIGHT Organization
• Aim to create a network of excellence for clinical resaerch in HIV/AIDS
• Designing and coordinating clinical trials and “data gathering” on HIV/AIDS at European level
• Define optimal strategies for management of HIV and guide the implementation of interventions
• Participation of new member states and EE encouraged
European HIV clinical trials network
European HIV Clinical Trials network
• Brain storming meeting convened by EU, 6 June 05
• Follow-up meeting 11 July 05
• Aim to define objectives and design of a network
Studies planned at MRC
TOSCA
• Trial Of Short Course Antiretrovirals
Concept:
Brian Gazzard
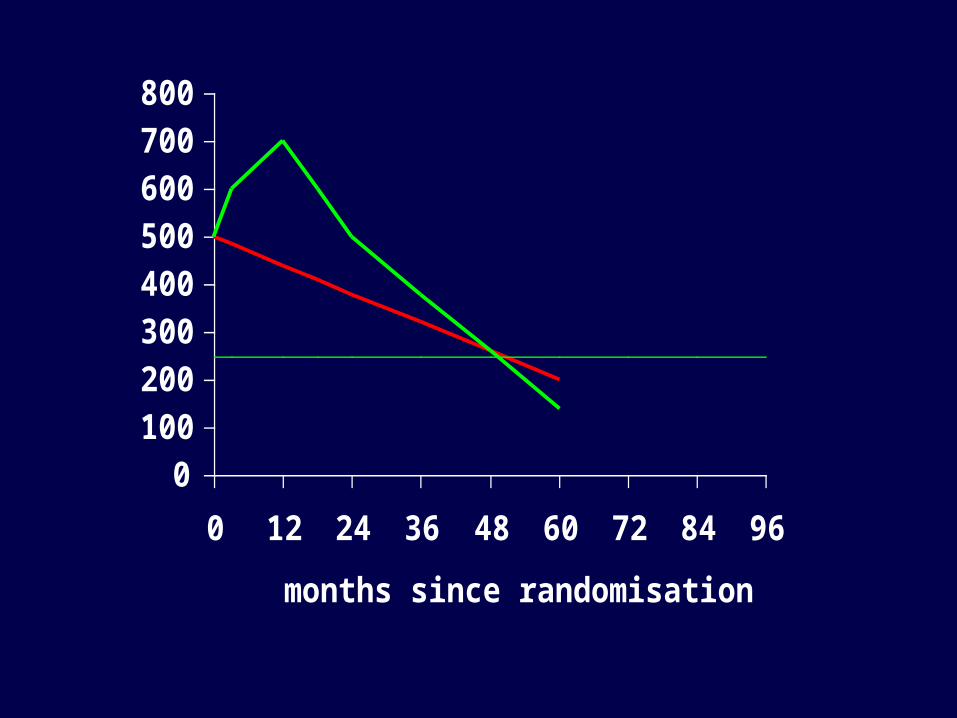
TOSCA rationale• Stopping HAART at high CD4 cell count is safe
• Biphasic CD4 loss, initial rapid followed by slow decline
• BIG Q = Can early HAART “buy time” before need to start continuous HAART
• Initial Q = After a 1y course of ART, is the rate of subsequent CD4 decline equal, faster or slower than the rate without treatment?
• Not done before (SMART: CD4 vs VL strategy; few naïve patients; no untreated control)
0100200300400500600700800
0 12 24 36 48 60 72 84 96
months since randomisation
CD4 count
0100200300400500600700800
0 12 24 36 48 60 72 84 96
months since randomisation
CD4 count
0100200300400500600700800
0 12 24 36 48 60 72 84 96
months since randomisation
CD4 count
0100200300400
500600700800
0 12 24 36 48 60 72 84 96
months since randomisation
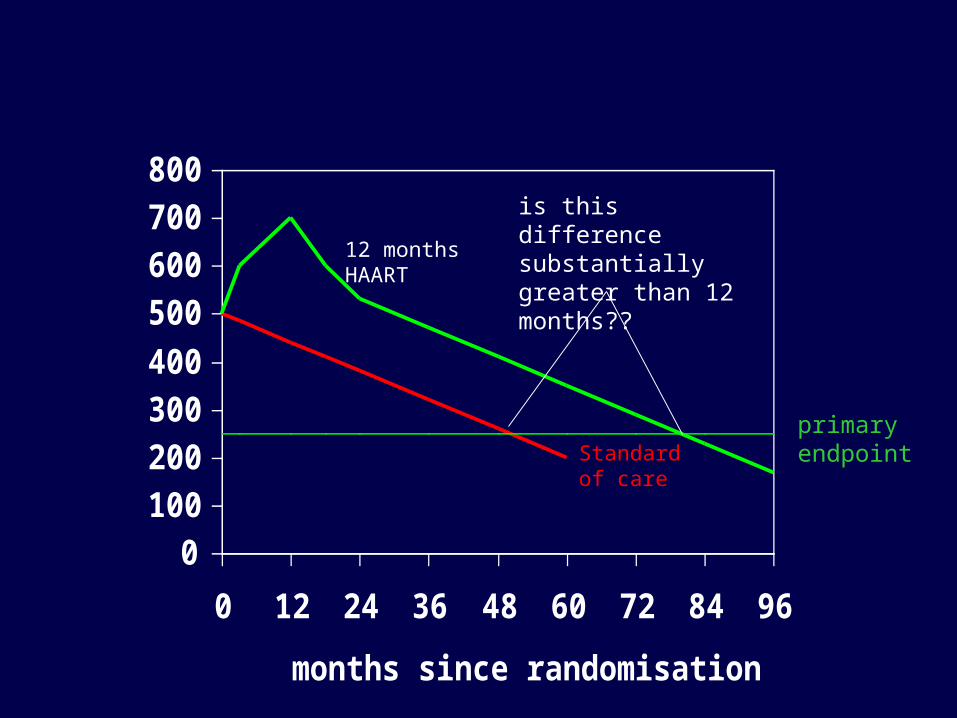
CD4 countStandard of care
12 months HAART
is this difference substantially greater than 12 months??
primary endpoint
TOSCA design• ART naive
• CD4 > 500 (? Feasible; consider > 400 / 350)
• Randomise to HAART 1y vs no Rx• Primary endpoint = change in CD4 from
baseline at 3y (if advantage persists in HAART arm then 1 year “buys” >2 additional years….?clinically worthwhile / attractive to patients) OR time to threshold (CD4 = 250)
• N ~ 200- 300
TOSCA sub-studies
• Development of resistance after stopping (staggered vs replacement if NNRTI) using highly sensitive resistance assays
• Immune responses to HepB / C (motivated by increased risk of death in hepatitis patients given ART)
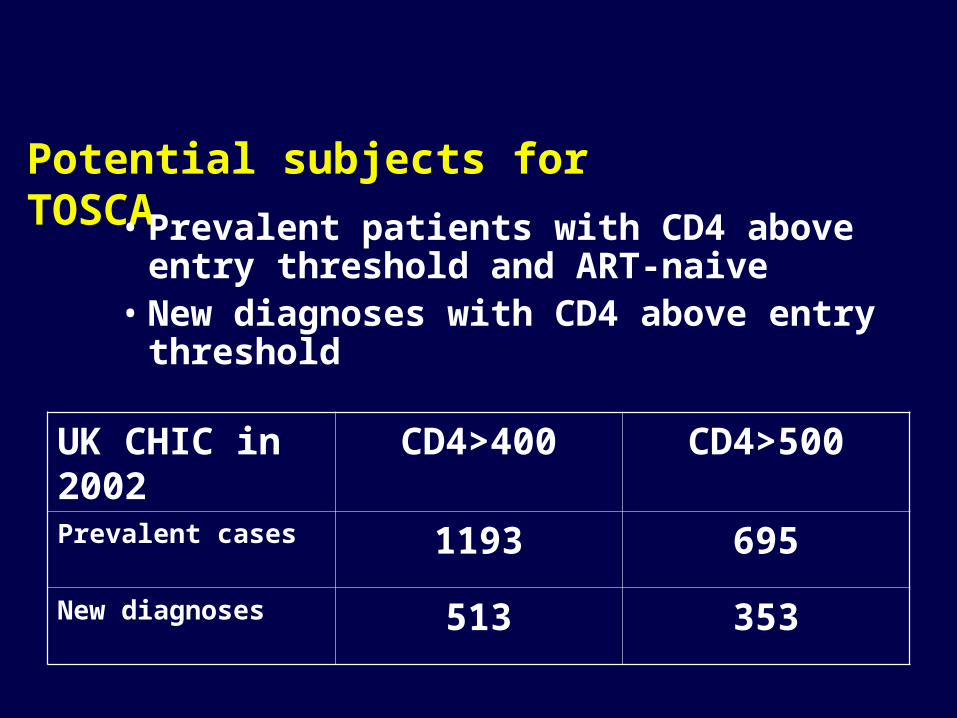
Potential subjects for TOSCA• Prevalent patients with CD4 above entry
threshold and ART-naive• New diagnoses with CD4 above entry
threshold
UK CHIC in 2002
CD4>400 CD4>500
Prevalent cases 1193 695
New diagnoses 513 353
Tenofovir as pre-exposure prophylaxis in MSM
Concept:
Mike Youle
TDF study rationale
• TDF has good safety profile and once-daily dosing
• Potential for use as PrEP in high risk individuals (taken continuously)
• Animal studies support efficacy in preventing HIV
• Ongoing transmission of HIV in MSM in spite of safe-sex education and condom promotion
• Q = Is TDF effective in preventing HIV transmission in MSM
TDF study design
• RDBPC trial• Recruitment at GUM clinics• MSM at high risk:
– recent history of UAI– Recent STD– recreational drug use– Recent use of PEP
• Randomised to TDF or placebo for 12 months
• Primary endpoint = new HIV infections at 12m
What incidence rate can we expect?
• De-tuned assay has been applied to residual serum specimens from MSM attending STI clinics. Estimate– 3% incidence in London– 1% incidence outside London
• Calculations are highly sensitive to assumed interval between reactivity of detuned assay and a standard sensitive screening assay (4-6 months??)
• More direct data from cohorts of gay men in Australia – indicate ~2% incidence in those with multiple risk factors
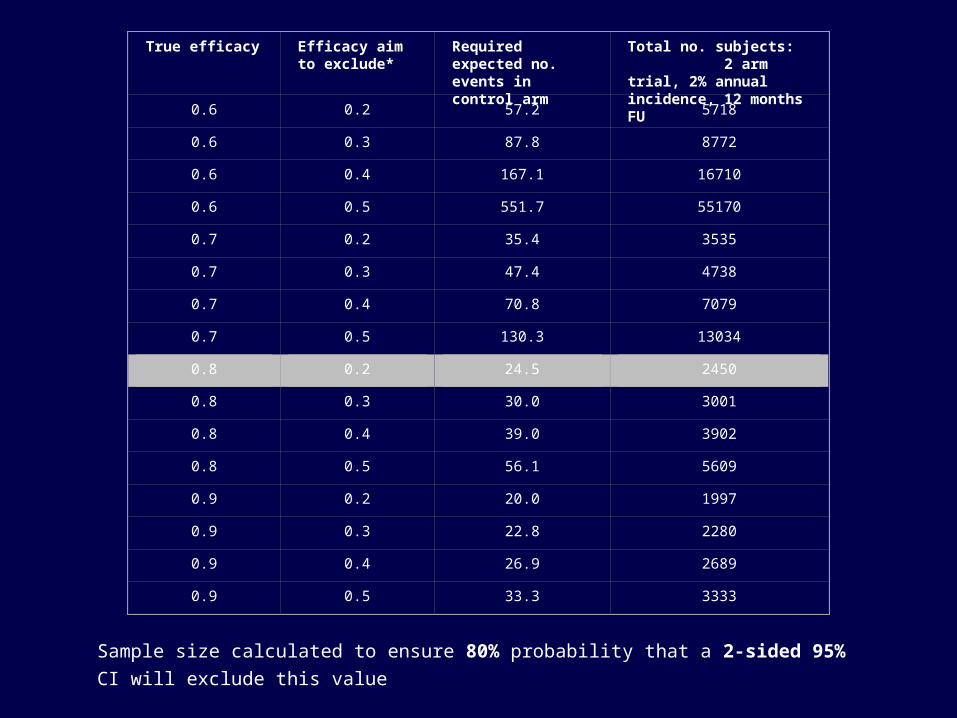
True efficacy Efficacy aim to exclude*
Required expected no. events in control arm
Total no. subjects: 2 arm trial, 2% annual incidence, 12 months FU
0.6 0.2 57.2 5718
0.6 0.3 87.8 8772
0.6 0.4 167.1 16710
0.6 0.5 551.7 55170
0.7 0.2 35.4 3535
0.7 0.3 47.4 4738
0.7 0.4 70.8 7079
0.7 0.5 130.3 13034
0.8 0.2 24.5 2450
0.8 0.3 30.0 3001
0.8 0.4 39.0 3902
0.8 0.5 56.1 5609
0.9 0.2 20.0 1997
0.9 0.3 22.8 2280
0.9 0.4 26.9 2689
0.9 0.5 33.3 3333
Sample size calculated to ensure 80% probability that a 2-sided 95% CI will exclude this
value
TDF study potential problems (1)
• 1) Politics / controversy / competition• Cambodia : stopped• Nigeria : stopped• Cameroon : suspended• Thailand : started but in jeopardy• Ghana : ongoing• Botswana : ongoing• Malawi (MSM) starting Sept• Peru (MSM) starting Sept
TDF study potential problems (2)
• Incidence may be low• Standard of care will need to include
counselling, condom provision AND ensuring easy access to post-exposure prophylaxis (now recommended by DHHS in MMWR 15 January 2005; and European guidelines and BHIVA guidelines)
• May result in ? 1% incidence
TDF study problems (3)
• Funding!! Will need many countries involvement to get study numbers ? Who will fund this?
• Long term considerations of public health implications / counteracting effect of behaviour change