65
1 Human Growth and Development: Geriatrics Small Group Session Karen Hall, M.D. Division of Geriatric Medicine University of Michigan and Ann Arbor VA Health Systems
| Date post: | 09-Aug-2015 |
| Category: |
Documents |
| Upload: | dentistryinfo |
| View: | 183 times |
| Download: | 1 times |
1
Human Growth and Development:
Geriatrics Small Group Session
Karen Hall, M.D.
Division of Geriatric Medicine
University of Michigan and Ann Arbor VA Health Systems
2
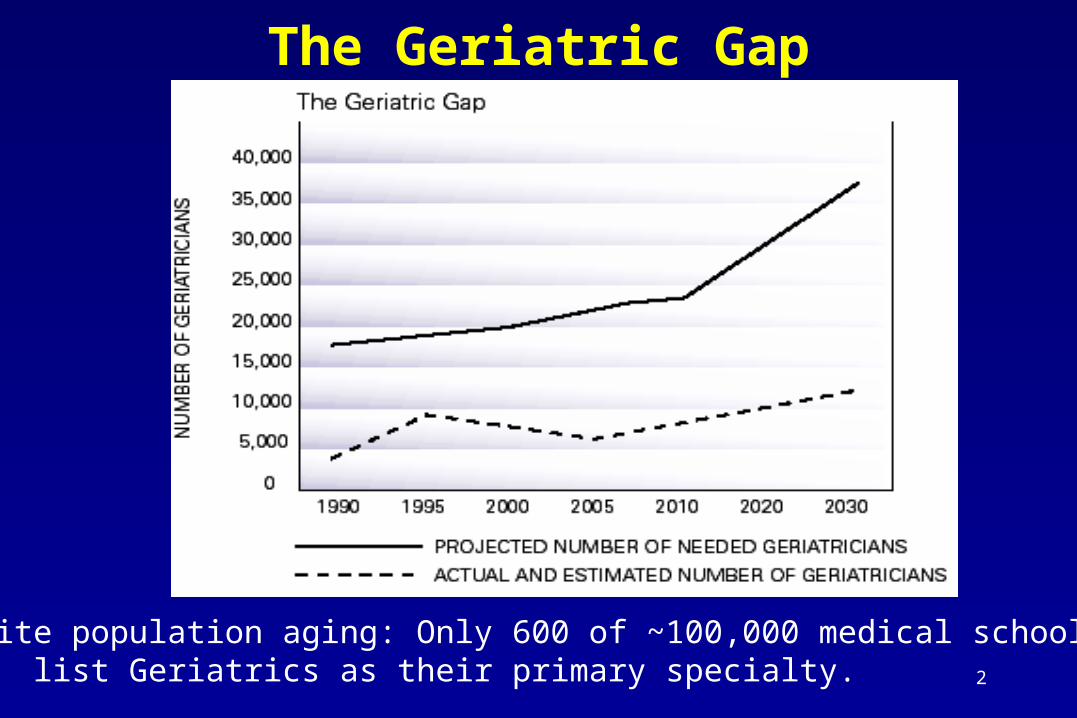
The Geriatric Gap
Despite population aging: Only 600 of ~100,000 medical school faculty list Geriatrics as their primary specialty.
3
How can you deliver “good” geriatric medical care?
• Recognize FUNCTION as an outcome.
• Learn how to assess FUNCTION. Activities of Daily Living (ADLs, IADLs)
Mobility, Cognition, Affect ABCDE Nutritional Assessment: (Anthropometry,
Biochemical, Clinical, Dietary intake, Energy expenditure).
4
Intended Learning Outcomes
• Understand how a functionally-oriented geriatrics assessment differs from a standard medical evaluation.
• Identify and quantify major domains of functional assessment (cognition, affect, mobility).
• Identify key activities that constitute basic (physical) and instrumental activities of daily living.
• Become familiar with nutritional assessment (Anthropometry, Biochemical, Clinical, Dietary intake, Energy expenditure) in older individuals.
5
Functional Assessment in Older Adults
• Most useful in patients with:
Complex, multiple medical disease Frailty, age >75 Atypical and obscure disease presentation Physical, cognitive, and affective problems Vulnerability to iatrogenic disability Socially isolated and economically deprived High risk for institutionalization

6
Clinical Uses of Functional Assessment
• Screen for risk factors or undetected problems.
• Assist in diagnosis.
• Establish baseline, set rehabilitation or therapeutic goals, and monitor patient course.
• Plan for appropriate care needs.
• Use in a variety of environments (e.g. inpatient units or consultation, outpatient, home visit, nursing home).

7
Positive Effects of Assessment
• Improve: functional status, diagnostic accuracy, living situation
• Reduce polypharmacy, prescribe appropriate medications
• Decrease hospitalizations/nursing home use
• Increase home health care
• Reduce medical costs
• Prolong survival
8
Functional status predicts outcomes
• Sager et al., 1996
Risk factors for greatest risk of functional decline following hospitalization among patients > 70 years:• increasing age• preadmission IADL disability• lower cognitive status
9
Functional status predicts outcomes
Dargent-Molina et al., 1996
• Fall-related predictors of hip fracture:• slower gait speed• difficulty with tandem (heel-toe) walk• decreased visual acuity• small calf circumference
10
A CONTROLLED TRIAL OF INPATIENT AND OUTPATIENT GERIATRIC EVALUATION
AND MANAGEMENT
Conclusions: Inpatient and Outpatient Geriatric Assessment
significantly reduced functional decline and improved
mental health with no increase in costs.
Cohen et al.; N Engl J Med 2002;346:905-12
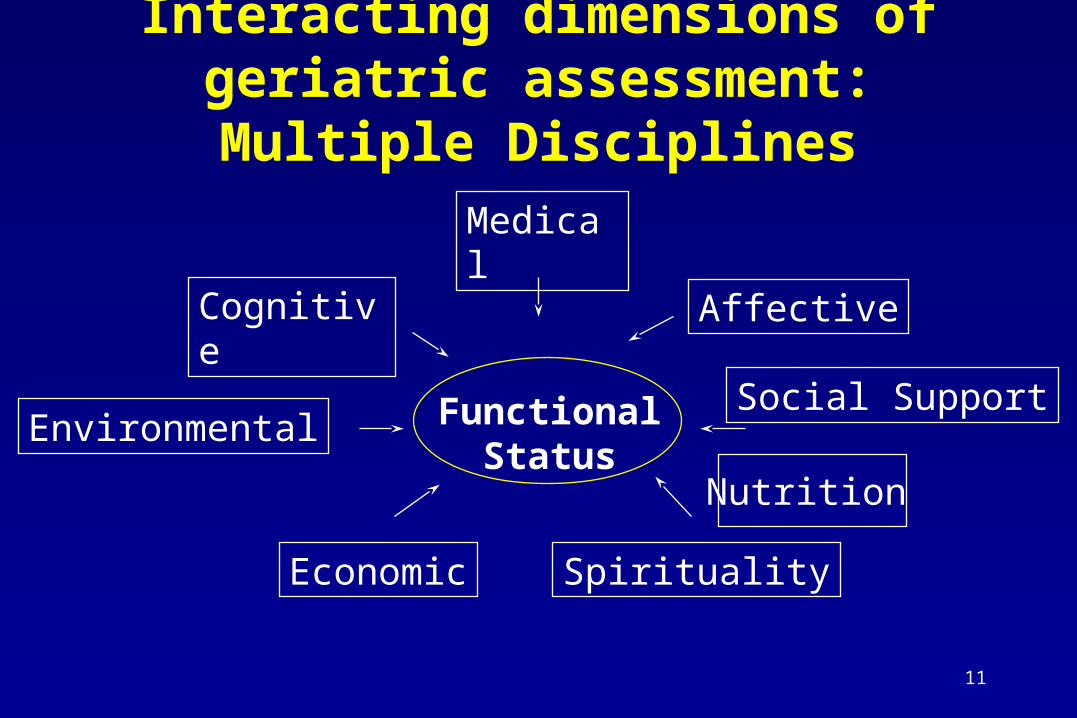
11
Interacting dimensions of geriatric assessment: Multiple Disciplines
Social Support
Cognitive
Medical
Affective
Environmental
Economic Spirituality
FunctionalStatus
Nutrition

12
Multidisciplinary Team Approach
• Physician or Physician Assistant or Nurse Practitioner
• Nurse
• Social Worker
• Pharmacist
• Dietician
• Physical Therapist
• + others
13
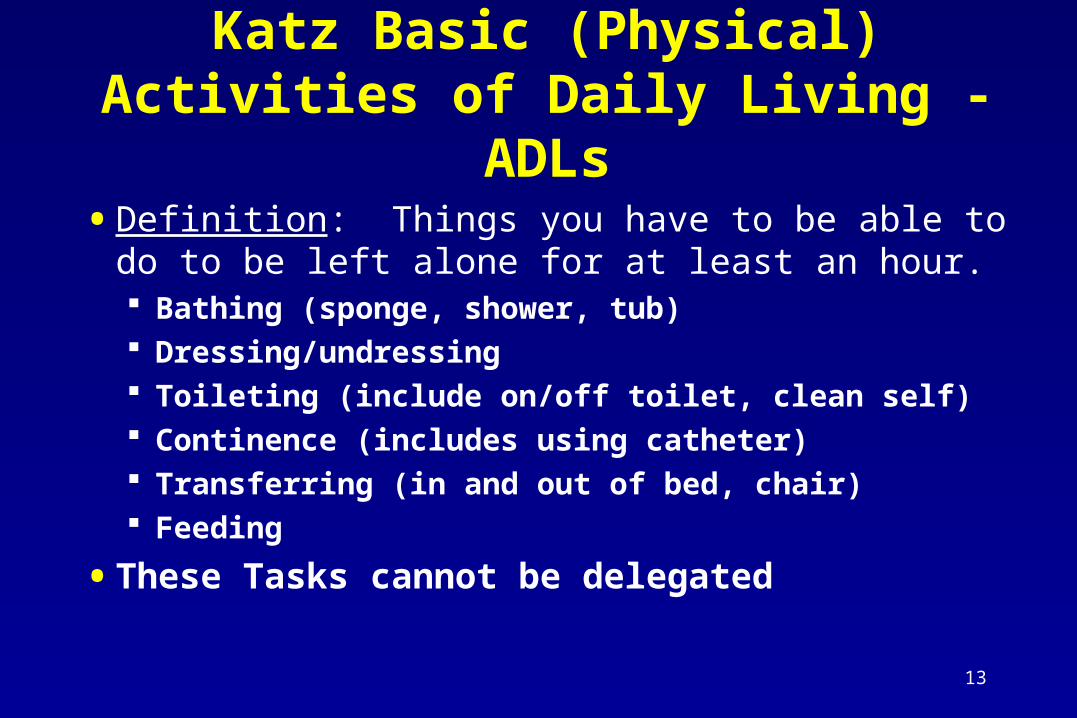
Katz Basic (Physical) Activities of Daily Living - ADLs
• Definition: Things you have to be able to do to be left alone for at least an hour. Bathing (sponge, shower, tub) Dressing/undressing Toileting (include on/off toilet, clean self) Continence (includes using catheter) Transferring (in and out of bed, chair) Feeding
• These Tasks cannot be delegated
14
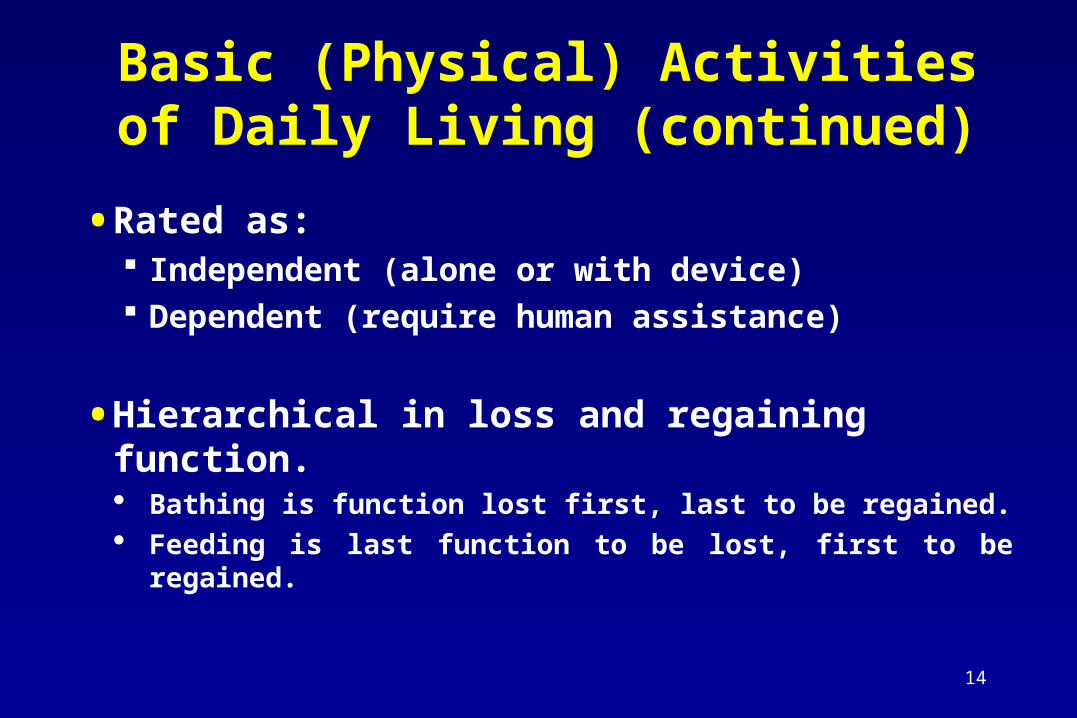
Basic (Physical) Activities of Daily Living (continued)
• Rated as: Independent (alone or with device) Dependent (require human assistance)
• Hierarchical in loss and regaining function. Bathing is function lost first, last to be regained. Feeding is last function to be lost, first to be regained.
15
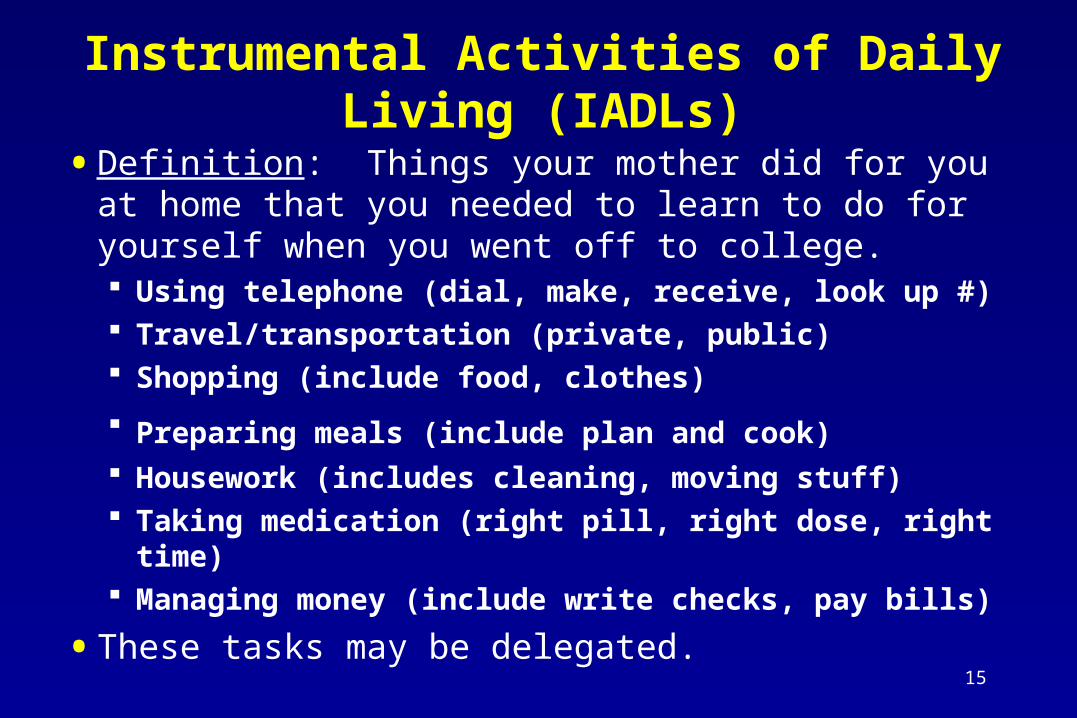
Instrumental Activities of Daily Living (IADLs)
• Definition: Things your mother did for you at home that you needed to learn to do for yourself when you went off to college. Using telephone (dial, make, receive, look up #) Travel/transportation (private, public) Shopping (include food, clothes)
Preparing meals (include plan and cook) Housework (includes cleaning, moving stuff) Taking medication (right pill, right dose, right time) Managing money (include write checks, pay bills)
• These tasks may be delegated.
16
• Folstein MMSE:- Orientation (date, place)
- Registration (immediate repetition: Ball, Cup, Flag)
- Serial 7’s (100-93-86-79-72-65) (or WORLD backwards)
- Recall of 3 items after 1 minute
- Language: naming, repeating, writing
- Executive: 3-step command; copy intersecting pentagons
Cognitive Assessment
17
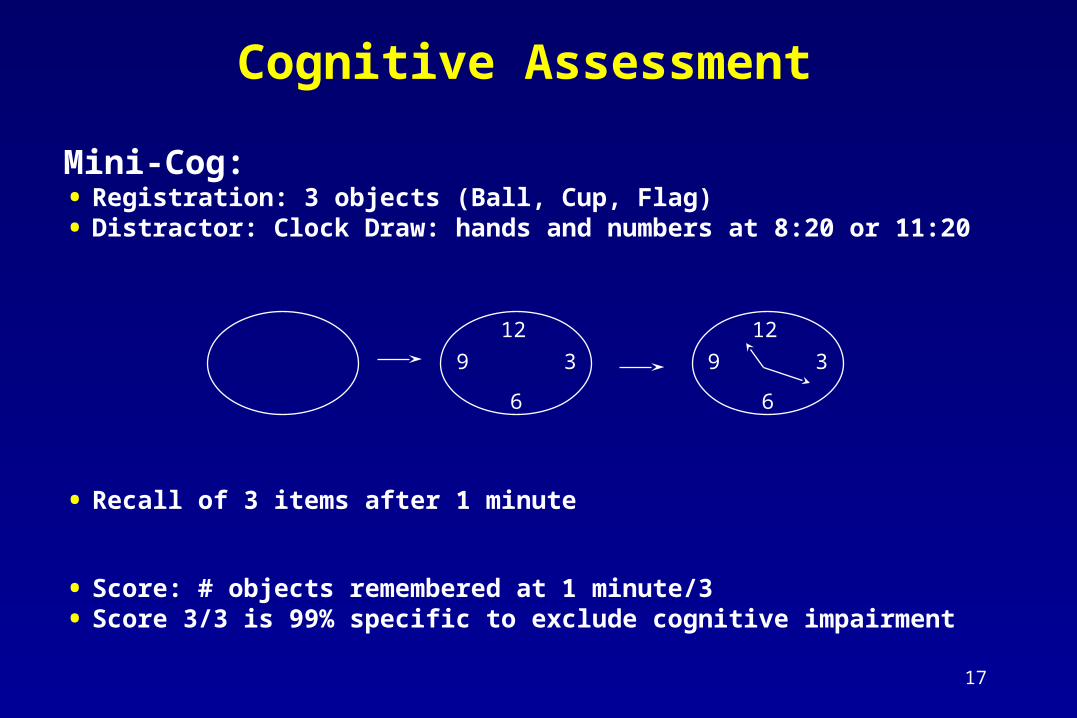
Mini-Cog:• Registration: 3 objects (Ball, Cup, Flag)• Distractor: Clock Draw: hands and numbers at 8:20 or 11:20
• Recall of 3 items after 1 minute
• Score: # objects remembered at 1 minute/3• Score 3/3 is 99% specific to exclude cognitive impairment
Cognitive Assessment
12
6
39
12
6
39
18
Screening for Depression (Affect)
Depression is the most common psychiatric condition in older patients
- May present as anxiety, anhedonia
Validated screening tools:
- 2 question screen (rapid “rule-out”)
- Geriatric Depression Scale (GDS)
19
Two-Question Screen
1. "During the past month, have you often been bothered by feeling down, depressed, or hopeless?
2. "During the past month, have you often been bothered by little interest or pleasure in doing things?"
“No” to both: 99% specific to exclude depression
20
Geriatric Depression Scale
- Dropped many of your activities and interests?- Feel your life is empty?- Often get bored?- Afraid something bad will happen to you?- Often feel helpless?- Prefer to stay at home rather than going out?- Feel you have more problems with memory than most?- Feel pretty worthless the way you are now?- Feel your situation is hopeless?- Think that most people are better off than you? - Not satisfied with life? Poor spirits most of the time? Not wonderful to be
alive? Lacking energy?
21
Detailed Assessment: DepressionGeriatric Depression Scale
- Questions exclude “pains, aches” from Standard Depression Scale of 30 items
- Score as # positive/15
- Positive: > 5/15
- Significant predictor for depression (raises pre-test likelihood from 30% to 70+% in geriatric age patients)
22
Nutrition: “Determine” Nutritional Risk
• D - Disease, acute and chronic
• E - Eating poorly
• T - Teeth problems
• E - Economic hardship
• R - Reduced social contact
• M - Medications
• I - Involuntary weight loss
• N - Needs ADL assistance
• E – Elderly
Rapid Screen: Has there been weight loss >10% in 6 months? Yes – do Mini Nutritional Assessment
23
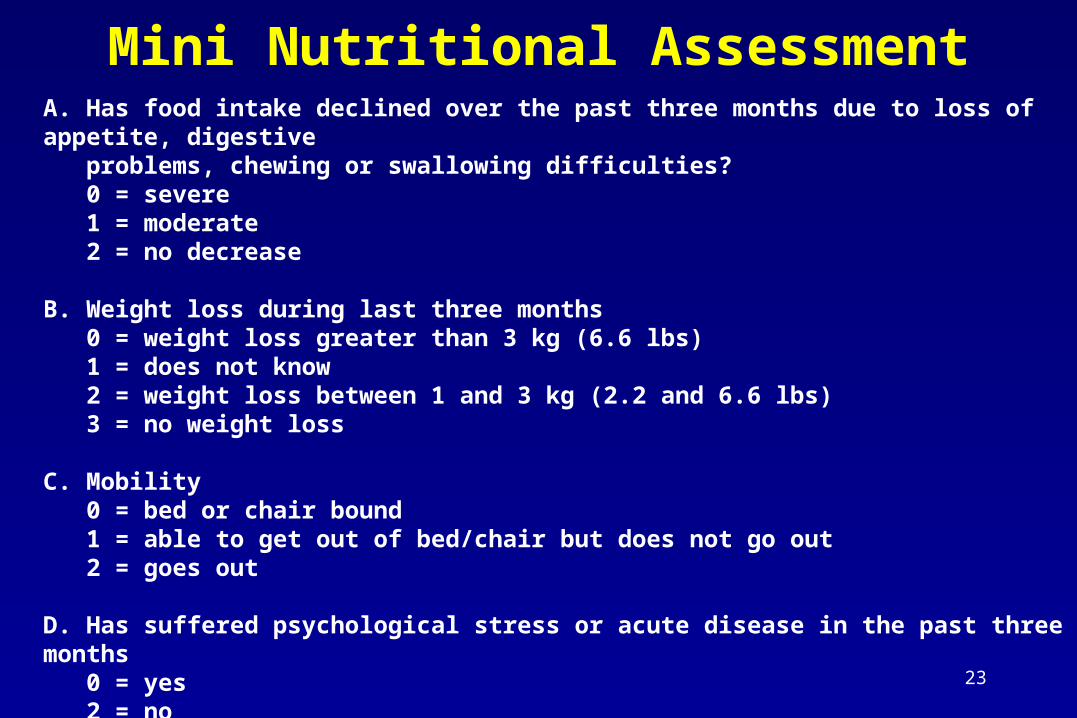
Mini Nutritional AssessmentA. Has food intake declined over the past three months due to loss of appetite, digestive problems, chewing or swallowing difficulties? 0 = severe 1 = moderate 2 = no decrease B. Weight loss during last three months 0 = weight loss greater than 3 kg (6.6 lbs) 1 = does not know 2 = weight loss between 1 and 3 kg (2.2 and 6.6 lbs) 3 = no weight loss C. Mobility 0 = bed or chair bound 1 = able to get out of bed/chair but does not go out 2 = goes out D. Has suffered psychological stress or acute disease in the past three months 0 = yes 2 = no
24
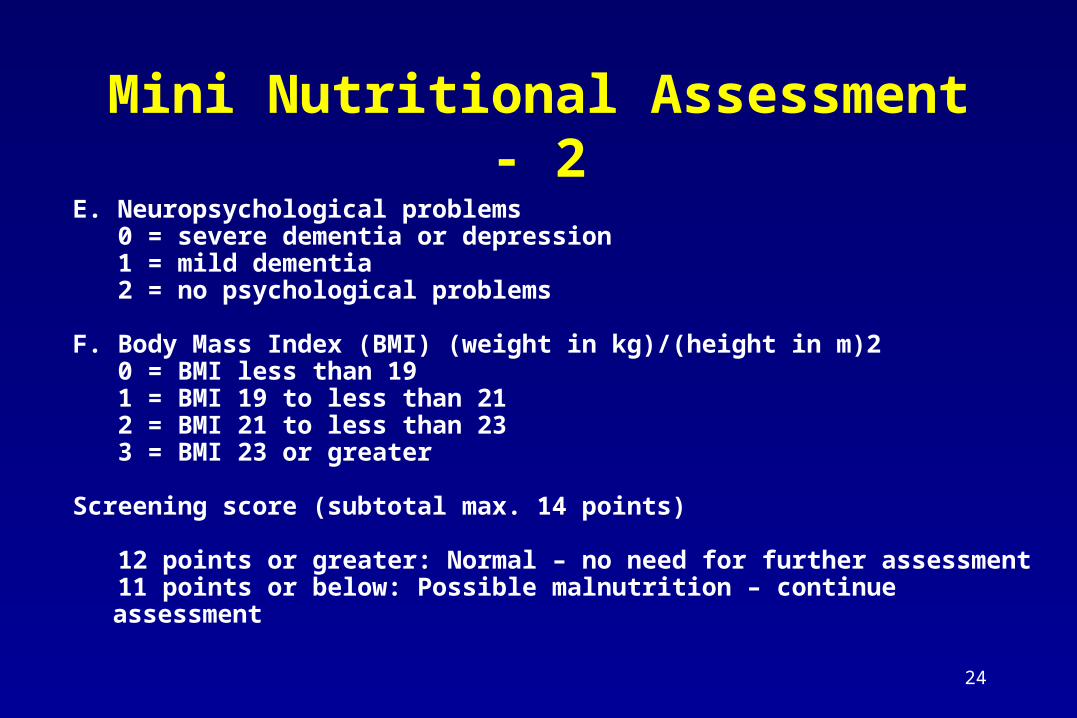
Mini Nutritional Assessment - 2
E. Neuropsychological problems 0 = severe dementia or depression 1 = mild dementia 2 = no psychological problems
F. Body Mass Index (BMI) (weight in kg)/(height in m)2 0 = BMI less than 19 1 = BMI 19 to less than 21 2 = BMI 21 to less than 23 3 = BMI 23 or greater Screening score (subtotal max. 14 points)
12 points or greater: Normal – no need for further assessment 11 points or below: Possible malnutrition – continue assessment

25
Mobility: Document Impairment
Validated:• Timed Up and Go (TUG: a quick screen)• Tinetti Gait and Balance (detailed)
Not validated but very useful:Observed Gait – comment on rising from
chair, walking, turning, get on exam table.
26
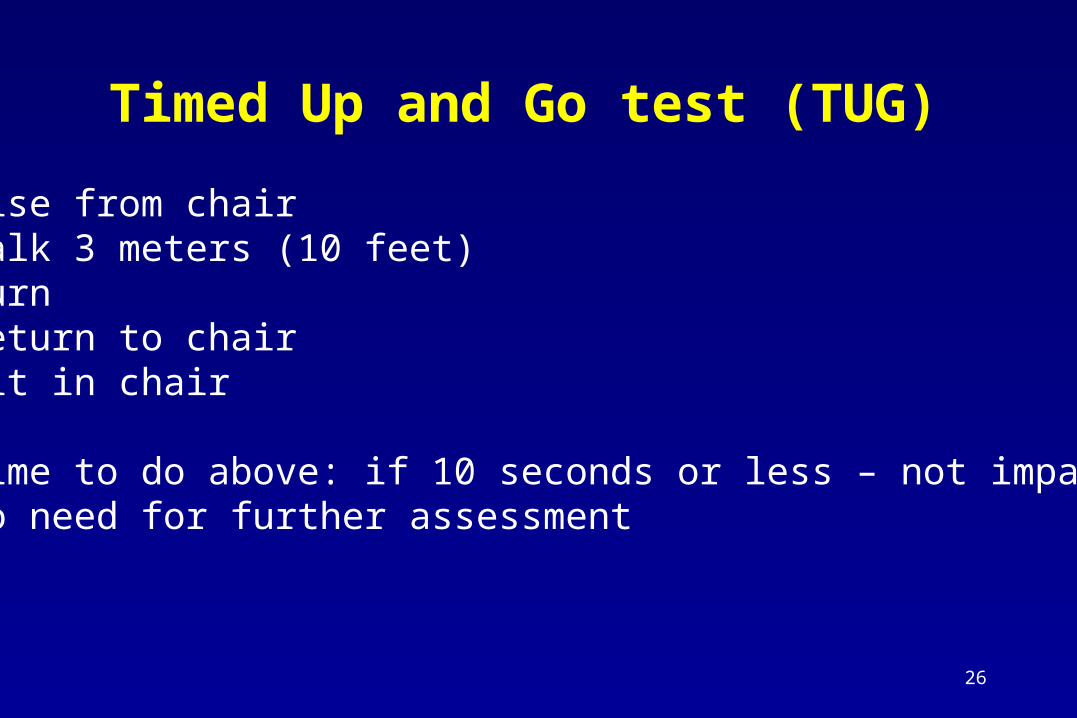
Timed Up and Go test (TUG)
Rise from chairWalk 3 meters (10 feet)TurnReturn to chairSit in chair
Time to do above: if 10 seconds or less – not impairedNo need for further assessment
27
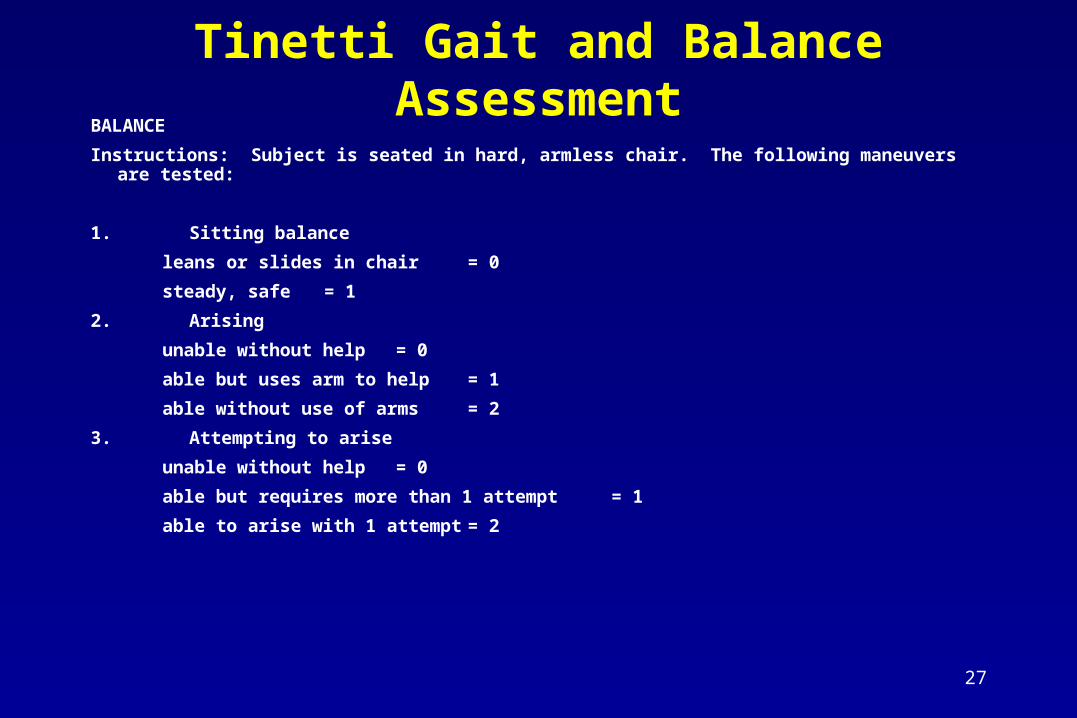
Tinetti Gait and Balance AssessmentBALANCE
Instructions: Subject is seated in hard, armless chair. The following maneuvers are tested:
1. Sitting balance
leans or slides in chair = 0
steady, safe = 1
2. Arising
unable without help = 0
able but uses arm to help = 1
able without use of arms = 2
3. Attempting to arise
unable without help = 0
able but requires more than 1 attempt = 1
able to arise with 1 attempt = 2
28
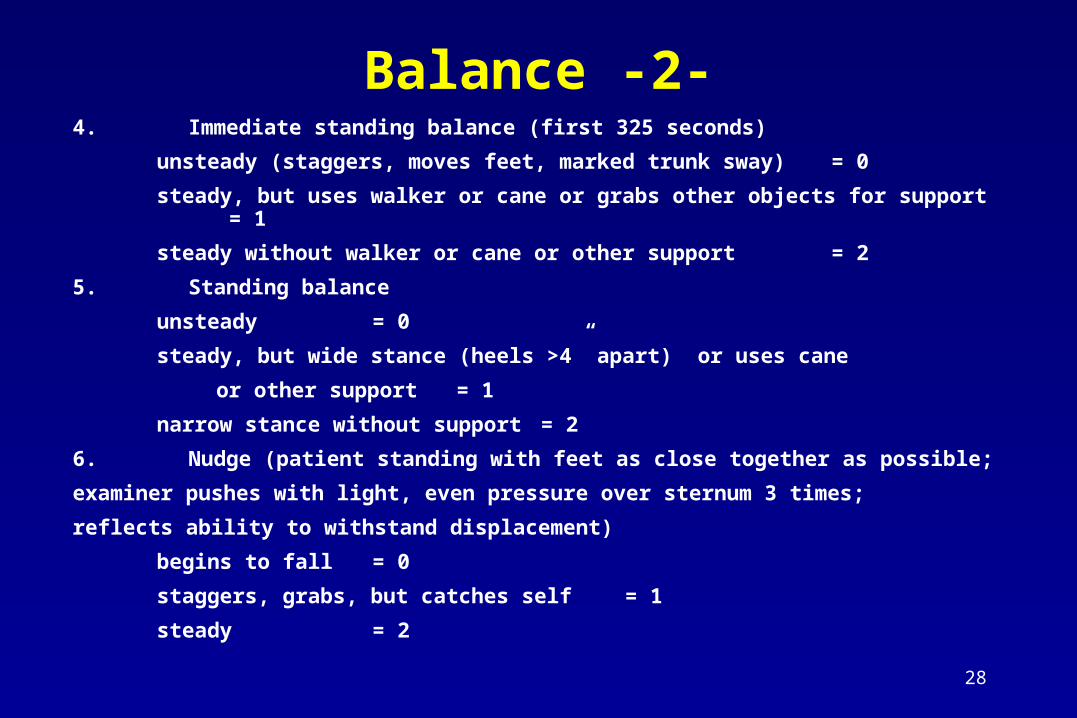
Balance -2-4. Immediate standing balance (first 325 seconds)
unsteady (staggers, moves feet, marked trunk sway) = 0
steady, but uses walker or cane or grabs other objects for support = 1
steady without walker or cane or other support = 2
5. Standing balance
unsteady = 0
steady, but wide stance (heels >4” apart) or uses cane
or other support = 1
narrow stance without support = 2
6. Nudge (patient standing with feet as close together as possible;
examiner pushes with light, even pressure over sternum 3 times;
reflects ability to withstand displacement)
begins to fall = 0
staggers, grabs, but catches self = 1
steady = 2
29
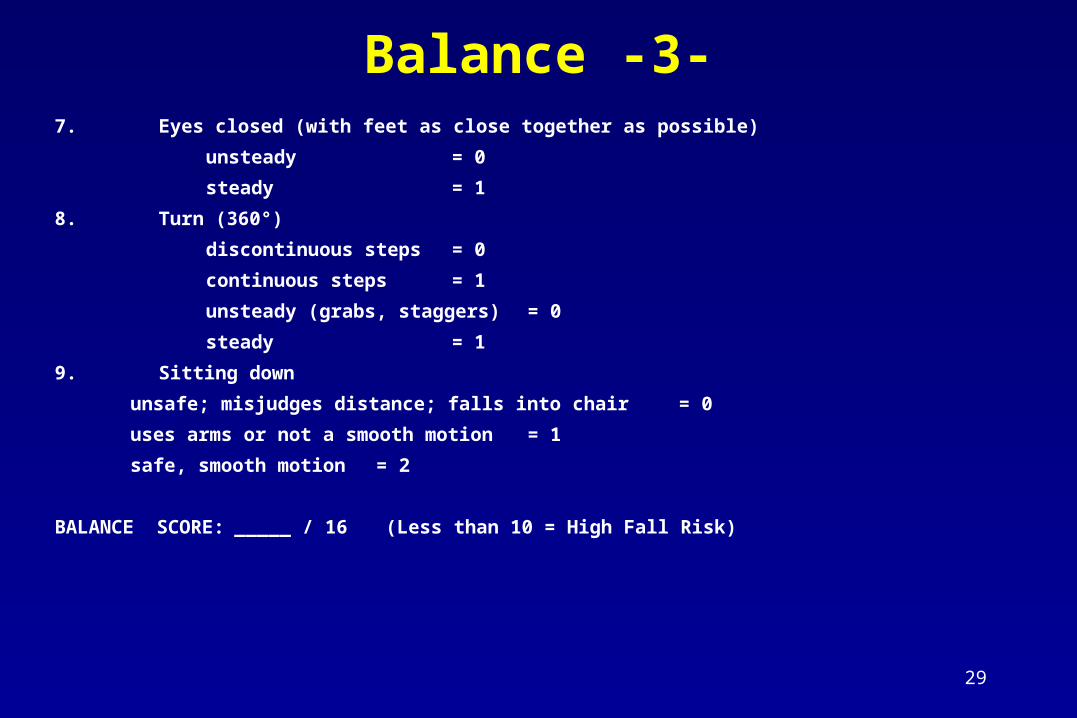
Balance -3-7. Eyes closed (with feet as close together as possible)
unsteady = 0
steady = 1
8. Turn (360°)
discontinuous steps = 0
continuous steps = 1
unsteady (grabs, staggers) = 0
steady = 1
9. Sitting down
unsafe; misjudges distance; falls into chair = 0
uses arms or not a smooth motion = 1
safe, smooth motion = 2
BALANCE SCORE: _____ / 16 (Less than 10 = High Fall Risk)
30
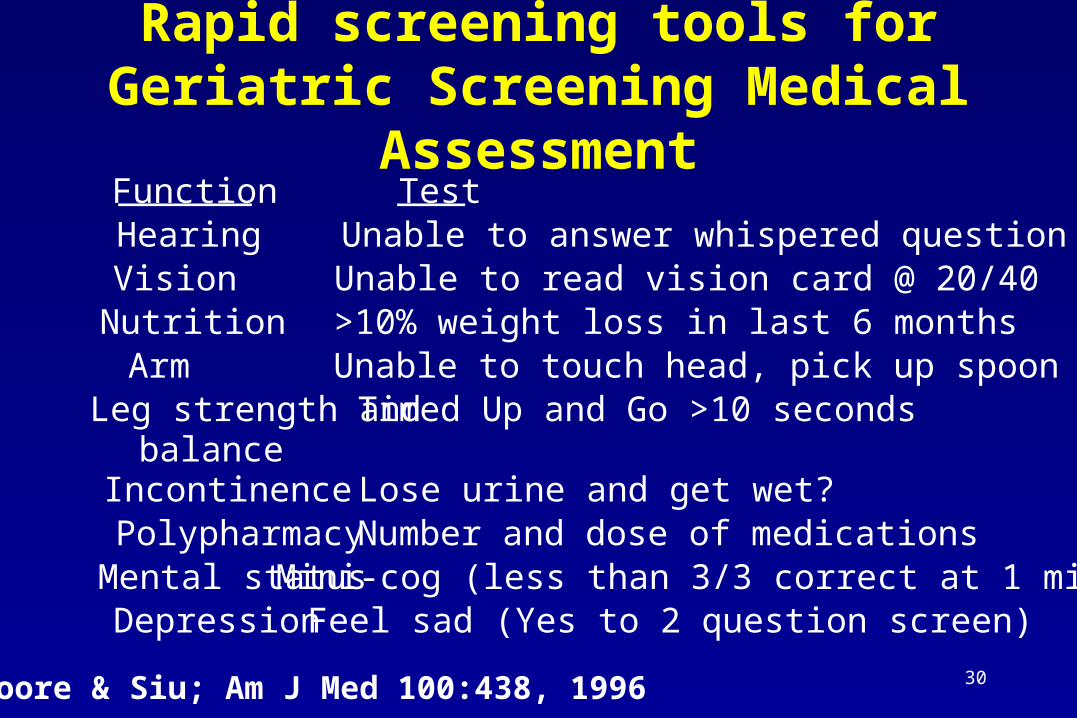
Rapid screening tools for Geriatric Screening Medical Assessment
Moore & Siu; Am J Med 100:438, 1996
Function Test Hearing Unable to answer whispered question Vision Unable to read vision card @ 20/40 Nutrition >10% weight loss in last 6 months Arm Unable to touch head, pick up spoon Leg strength and
balance Timed Up and Go >10 seconds
Incontinence Lose urine and get wet? Polypharmacy Number and dose of medications Mental status Mini-cog (less than 3/3 correct at 1 min) Depression Feel sad (Yes to 2 question screen)
31
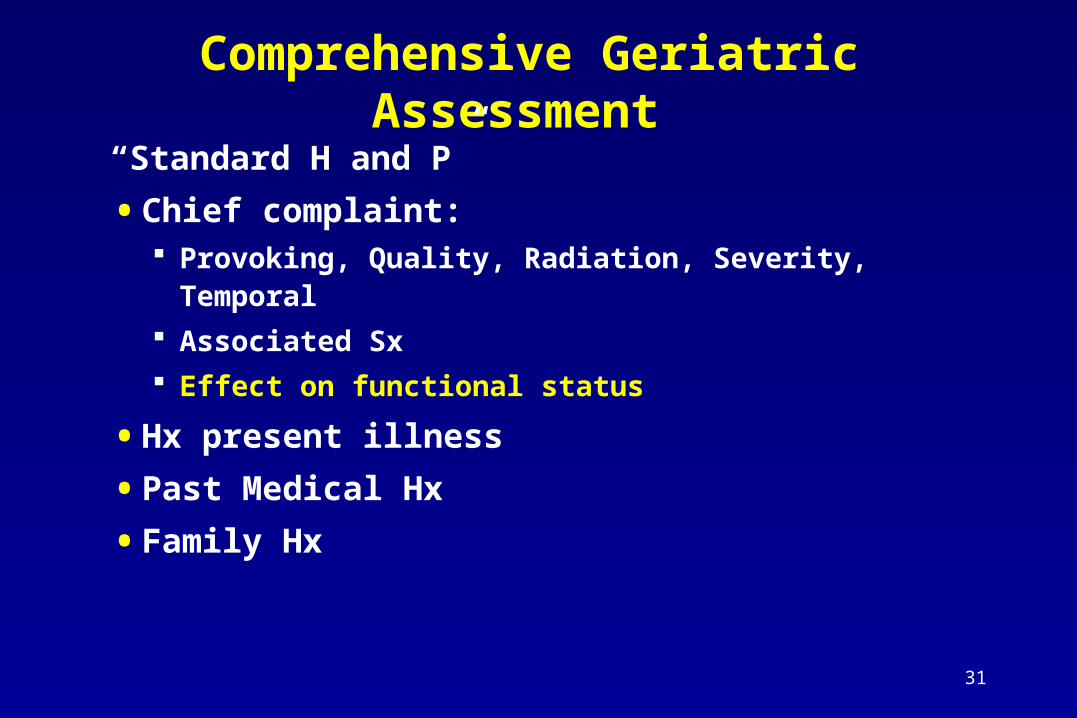
Comprehensive Geriatric Assessment
“Standard H and P”
• Chief complaint: Provoking, Quality, Radiation, Severity, Temporal
Associated Sx
Effect on functional status
• Hx present illness
• Past Medical Hx
• Family Hx
32
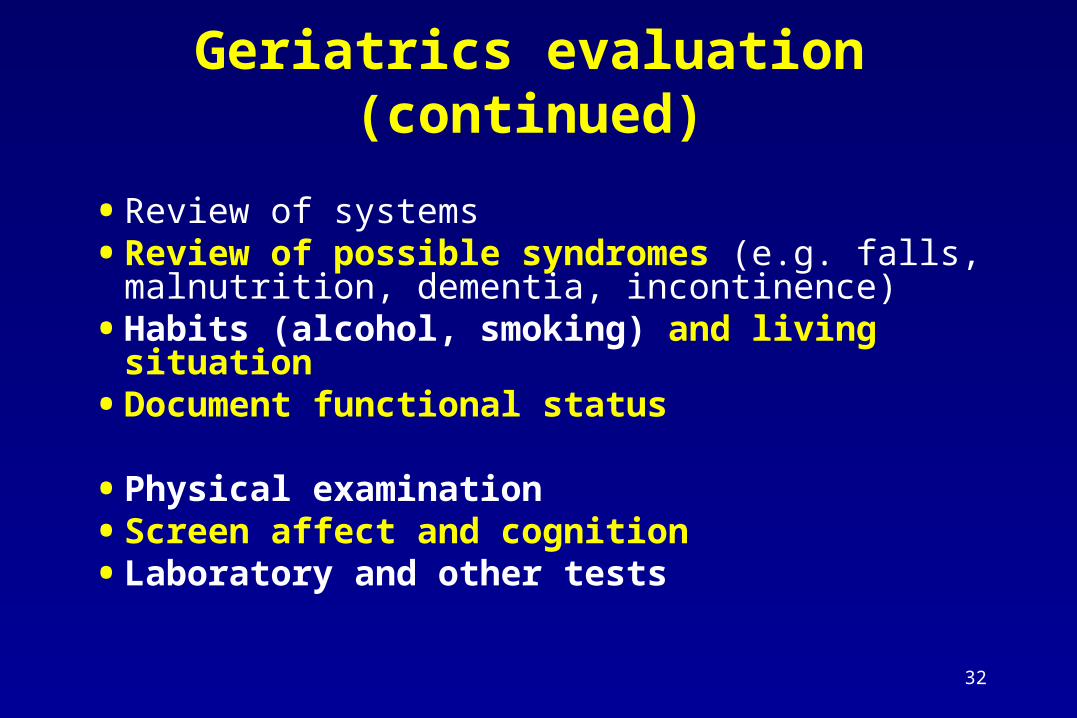
Geriatrics evaluation (continued)
• Review of systems• Review of possible syndromes (e.g. falls,
malnutrition, dementia, incontinence)• Habits (alcohol, smoking) and living situation• Document functional status
• Physical examination• Screen affect and cognition• Laboratory and other tests
33
Geriatrics evaluation (continued)
• Problem list and plan Medical Mobility Cognition and affect Mobility/upper extremity use Communication/sensory (vision, hearing) Nutrition Bladder and bowel
Family education/discharge planning
34
Mr. H., a new patient referred to your clinic…
• 84-year-old widowed man presents to the Turner Clinic for a new patient evaluation to establish primary care. The patient is accompanied by his daughter.
• The health concerns today are emphysema and a recent decline in functional status, most notably in the last three weeks since the death of his wife. This decline in his function prompted his daughter to have the patient move into her home.
35
History of Present Illness -1- • Living independently, was primary caregiver for wife (severe dementia).
• Six weeks ago, he and his wife moved into their daughter's house.
• Three weeks ago, the patient's wife died. After this - rapid decline in functional status.
• “Forgetting”: No longer able to remember medications. Daughter notes decreased recall for events of the previous day. Forgets that certain people are deceased and insists upon visiting them. More difficulty playing his favorite card game, euchre. Dresses in previous day’s clothes unless daughter lays out new ones. Requires reminder to bath. No longer able to manage his finances.
• Mood swings, mostly directed at the daughter. “More mean and angry”.
36
History of Present Illness -2-
• Two weeks ago the patient was driving to his daughter's
house and was alone in the car. He got lost and was
missing for 3 days. He was eventually found in Sault
Ste. Marie, Ontario.
• Some depressive symptoms in the past 5 weeks.
• Daughter thinks that for the last year or so, father was
having difficulties remembering dates, some places, and
names of grandchildren.
37
Past Medical History
• COPD. The patient reports an approximately 20-pack-year history of tobacco use, quit 25 years ago. No intubation, chronic steroid treatment or supplemental oxygen. No PFT data available.
• Medications: Combivent 2 puffs t.i.d. There are no known drug allergies.
38
Additional History
• Social History: He is a retired fireman. He previously drank alcohol socially, denies current use. The patient has 3 other daughters, one who lives in Troy, Michigan, and is willing to help as needed.
• Family History: Non-contributory.
• Review of Systems: 10-20 pound weight loss in the last year. He states his appetite is “fair”. He does not have complaints of any bowel or bladder problems.
39
QUESTION
• Based on the information you have so far,
what do you think is the most likely cause
of the patient’s decline in function?
• Do you want any other information?
40
Review of Functional Status
• Independent in most ADLs: personal grooming, toileting, continence, transferring, and walking.
• Needs assistance with dressing (daughter helps him select clothes each day), bathing (requires prompting).
• Requires assistance with several IADLs: Housework, shopping, using transportation, preparing meals, taking medications and managing his finances.
41
Mini-Nutritional Assessment
• Scored 6/14: positive score was <12
• Significant positives: weight loss > 10 lbs, recent stressor (wife’s death), possible dementia
• Major issue is obtaining meals, not eating them
42
Physical Exam and Laboratory Evaluation
• Vital Signs: blood pressure 110/60, pulse was 92, weight of 157 pounds. Height 6 feet.
• General: Well-nourished, well-developed gentleman in no acute distress with a mild psychomotor retardation. He was alert. His speech was fluent, and he was socially appropriate.
43
Cognitive and Affective Assessment
• Folstein Mini Mental State Examination: 22/30 missed points on orientation (wrong date, day of week and season) and recall (unable to recall two of the three objects) and serial sevens (two incorrect responses).
• Geriatric Depression Screen Information: Scored three positive responses (acknowledges that he has dropped out of activities, that he does not feel happy and that he prefers to stay at home). He denies suicidality.
44
QUESTION
• Now what do you think is the most likely
cause of the patient’s decline in function?
• Tests?
• Recommendations?
45
Tests:
Labs, CXR
Neuropsychometric Testing
Recommendations:
Continue assisted living (not able to be independent)
Daughter supervise IADLs, ADLs
Respite for Daughter (Adult Day program)
Referral to Cognitive Disorders Clinic for definitive diagnosis and treatment
46
Tests:
Protein 5.4, Albumin 2.9
WBC 5.5, RBC 4.50, HGB 14.0, HCT 41.5, MCV 92.2
Lytes, BUN, Cr normal
LFTs normal, Ca normal
U/A negative
Vitamin B12 and folate normal
TSH normal
CXR: mild emphysema, no masses or infiltrates
47
Report from Neuropsychometric Testing
• Wechsler Adult Intelligence Scale-Revised Verbal I.Q. = 84 (100+/-15) Comprehension - 9 (%ile) Similarities - 5 (%ile) Arithmetic - 50 (%ile) Verbal Fluency Test - 2 (%ile)
• Benton Visual Naming Test - 5(%ile)
• Narrative Comments from Neuropsych testing:This pattern of test results, with primary memory deficit and associated difficulties with language-related abilities and reasoning, is most consistent with a primary degenerative dementia.
48
Patient Follow-up VisitAt 3 months:• Accompanied by his daughter – lives in her house.
• Stable, no new behavioral issues.
• Regularly attending and participating in an Adult Day Care program (The Silver Club based at the Turner Geriatric Clinic Senior Resource Center) during the week. This provides the daughter with time to attend to her own family’s needs.
• Daughter supervises meal preparation and eating. Weight has increased 12 pounds. Repeat albumin now in normal range.
• Seen in Cognitive Disorders Clinic where a diagnosis of probable Alzheimer’s Disease was made. Patient is considering enrolling in a clinical trial to test the effects of a new approach to treating Alzheimer’s Disease.
• Initiated on therapy with donepezil (Aricept) and Vitamin E.
49
Case 2: an Inpatient transferred to a Skilled Nursing Facility
50
JL is an 80 year old female who transferred from UM hospital to a nearby skilled nursing facility for further evaluation and rehabilitation 1 week after hip fracture. Four weeks after admission, on your 1-month Medicare recertification rounds at the nursing center, her nurse tells you that the resident has been eating progressively less food since admission.
PMHORIF for L femoral neck fracture sustained 5 weeks
ago after she tripped over a rug in her aptColon CA (cancerous polyp removed 1997)UTI (completed 10 d course of Bactrim 2 wks ago)Distant Hx CVA (no residual deficit?)HTN
51
Any additional history that you might want?
52
Additional history • Hospital course
Femoral neck pinned OR blood loss, post-op course: Minimal blood loss,
Post-op anemia Hct 32
• History of present illness Has been anorectic, with weight loss? [note fall as a
marker of other illness]• Unclear how much has been eating in her apartment
but per records normal weight was around 105 lbs.• family quoted in Hosp discharge summary as stating
that pt had been “slowing down lately”
53
Anything on Review of Systems?
54
Review of Systems
• Other GI symptoms (such as swallowing, blood in stool Occasionally coughs and chokes
• Difficulty with teeth Has misplaced lower denture
• Difficulty with thinking or mood Seems to feel her mind is “slowing down” Seems sad about present condition [Ddx Depression, Dementia, Parkinson’s?]
• Difficulty with vision Has trouble w/glare, night driving. Can see food.
55
Medications, for which conditions?
56
Medications
• HTN Dyazide (diuretic) 25 mg/day
• Post-op risk for deep venous thrombosis Coumadin (anticoagulant) titrated to give INR
of 2-3
57
Functional status: present and pre-morbid
• Present ADLs Ambulates with rolling walker, unsteady without it. Requires stand-by assist for most ADLs,
independent in eating.
• Previous ADLs Independent in basic ADLs Able to shop and cook for self. Family assist with
checkbook.
58
Examination
• Vitals: Weight 94 lbs. Temp 99.5. BP supine 140/90, pulse 70. Weak and unsteady on immediate standing. BP after 2 min standing 115/92, pulse 76.
• General: Kyphotic. Flat affect. Seems to stare. Movements slowed. Able to see letters to read.
• Lungs, heart, abdomen unremarkable except for hard stool in rectal vault. Trace + guaiac stool.
• Neuro: Strength symmetric. No tremor. Mild cogwheeling. Walks with small steps, trunk flexed, minimal arm swing but no shuffling. Rest of exam non-focal.
• Skin: 2 cm diameter area of erythema on coccyx.

59
Other laboratory evaluations?

60
Laboratory evaluations• Complete blood count: WBC for infection, Hct and indices for
type of anemia, Fe studies
• Work-up for low grade temp [older adults decreased febrile response]: Another UA, CXR, Doppler [occult DVT]? TB? Occult cancer w/u? Connective tissue disease or Temporal arteritis w/u?
• Chemistries: Electrolytes [Na, K esp. given Dyazide] BUN/Creat [check for dehydration] Cholesterol [measure of chronic illness, prognosis] Albumin
• Other?
61
Problem list and plan
62
Problem list and plan
• Medical Low-grade temp, ?infection, cancer, connective tissue disease.
Work-up as above. Plus guaiac stool x 3, GI f/u for colonoscopy. Other?
Anemia: Use indices to determine type (e.g. small cells=Fe def, large cells=?B12/Folate). Could use other Fe and vitamin, and other studies (e.g. reticulocyte count, hemolysis markers). Consider Fe supplementation (side effect=GI distress)
Sx and signs dehydration: Hold dyazide. Anorexia/weight loss: Related to conditions above. Note
possible Bactrim-induced anorexia.

63
Problem list and plan
• Medical (continued) Slowed activity, signs and sx Parkinson’s: Eval for
depression and dementia (see functional studies). Ask re:vegetative sx for depression. If depressed, consider SSRI. Consider CT head.
If AD, consider meds (Aricept), If Lewy body, avoid Haldol (will exacerbate Parkinsonian features!). If vascular consider ASA. If Parkinson’s, severe enough to warrant rx?
Other health maintainence: Osteoporosis prophylaxis: Vit D, Ca, other meds?
64
Problem list and plan
• Functional: Nutrition Dentistry: eval for replacement of lower denture Nursing: intake and output Dietician: Calorie count on actual intake. Dietary preferences,.
Soft mechanical diet until gets lower partial denture. Supplements.
Speech therapist: Bedside swallowing eval with liquids and solids. ?Formal barium swallow study?
Occupational therapist: Kitchen and safety eval to include cooking eval [Also includes ADL/upper extremity eval].
65
Problem list and plan• Functional: Mobility
Physical therapist already working on gait training
• Cognition and affect (and communication) MMSE and GDS to help guide Rx.
• Skin/wound: Decubitus care- decrease local pressure, increase activity, improve nutrition
• Bladder and bowel: Constipation may contribute to anorexia and wt loss, increase activity, fluid intake, fiber? , stool softener?, gentle laxative (such as MOM).
• Family education/discharge planning: SW to eval if able to return home independently. Home help?

















