43
HYPERTENSION HYPERTENSION MORE THAN BLOOD PRESSURE MORE THAN BLOOD PRESSURE ALONE! ALONE!
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | anissa-benson |
| View: | 218 times |
| Download: | 1 times |
HYPERTENSIONHYPERTENSION
MORE THAN BLOOD MORE THAN BLOOD PRESSURE ALONE!PRESSURE ALONE!
Richard Bright( 1789-1858)Richard Bright( 1789-1858) the First Nephrologist* the First Nephrologist*
First observation of “hardened pulse”and
renal damage at autopsy (1827)
* Source: Richard Bright Web-page Internet
First observation association of
cardiac hypertrophy and shrunken kidneys (1836)

Hypertension: classical Hypertension: classical conceptsconcepts
Causal factors hypertension
Target organ damageBrainHeart Kidney

Hypertension: classical Hypertension: classical conceptsconcepts
Causal factors hypertension
Target organ damageBrainHeart Kidney
HYPERTENSION FOLLOWS THE KIDNEY

Hypertension: classical Hypertension: classical conceptsconcepts
Causal factors hypertension
Target organ damageBrainHeart Kidney
HYPERTENSION FOLLOWS THE KIDNEY

EpidemiologyEpidemiology
Prevalence of hypertension very different between populations
Hypertension is associated with end organ damage

Relationship between sodium intake and Relationship between sodium intake and blood pressure around the world: population blood pressure around the world: population studiesstudies
0
5
10
15
20
25
30
0 10 20 30 40 50
% hypertensives
mea
n s
od
ium
in
take
(g
ram
s)
Northern Japan
Southern JapanUS
Marshall islands
Inuit
Meneely & Dahl, 1961
Low salt and high salt populations Low salt and high salt populations

Relationship between sodium intake Relationship between sodium intake and end-organ damageand end-organ damage
500
700
900
1100
1300
1500
1700
1900
2100
7,5 8 8,5 9 9,5 10 10,5
UNaV (g/day)
dea
ths
stro
ke p
er 1
00.0
00/y
r portugal
hollandgermany
spain
italy
malta
finland
UKdenmarkiceland

Hypertension and CV Hypertension and CV mortalitymortality
Domanski, JAMA 2002
Higher BP: worse outcomeSBP and DBP are independent risk factors
There is NO clearcut lower treshold!

Hypertension and end stage renal Hypertension and end stage renal failurefailure
Brancati, NEJM 1996
Higher BP: worse outcomeSBP and DBP are independent risk factors
There is NO clearcut lower treshold!

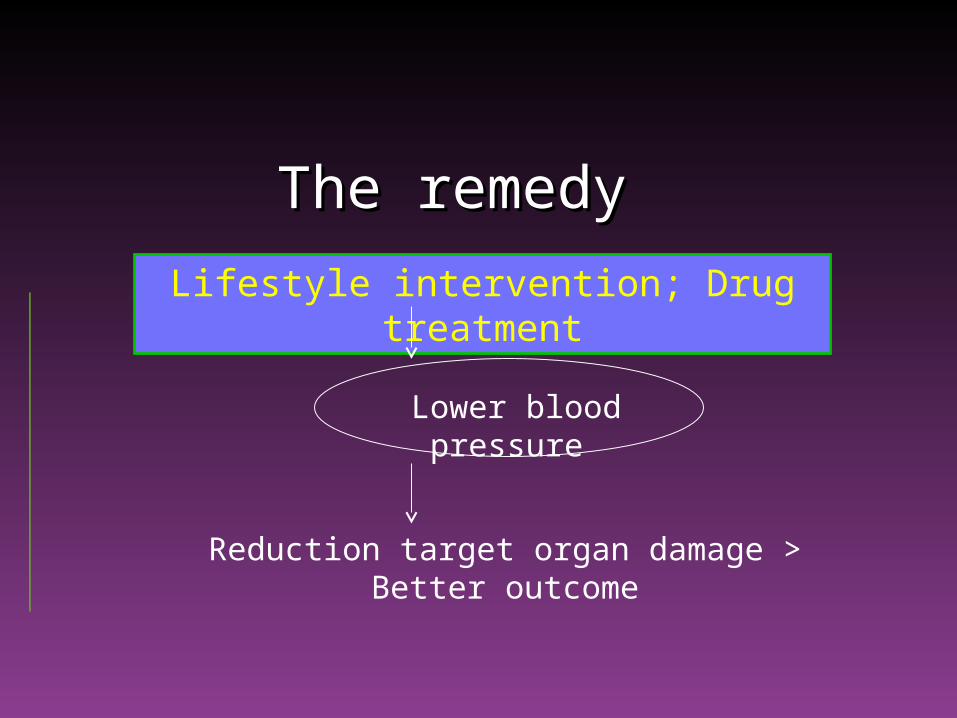
The remedyThe remedy
Lower blood pressureLower blood pressure
The remedyThe remedy
Lifestyle intervention; Drug treatment
Lower blood pressure
Reduction target organ damage > Better outcome
The remedyThe remedy
Lifestyle intervention; Drug treatment
Lower blood pressure
Reduction target organ damage > Better outcome
BENEFIT OF TREATMENT IS NOT EQUAL FOR ALL PATIENTS !
LIFESTYLE INTERVENTION & DRUG TREATMENT CAN POTENTIATE EACH OTHER !
INTERVENTION CAN IMPROVE OUTCOME ALSO INDEPENDENT OF EFFECT ON BLOOD PRESSURE !

The remedyThe remedy
Lifestyle intervention; Drug treatment
Lower blood pressure
Reduction target organ damage > Better outcome
BENEFIT OF TREATMENT IS NOT EQUAL FOR ALL PATIENTS !
LIFESTYLE INTERVENTION & DRUG TREATMENT CAN POTENTIATE EACH OTHER !
INTERVENTION CAN IMPROVE OUTCOME ALSO INDEPENDENT OF EFFECT ON BLOOD PRESSURE !

Meta Analysis: Lower SBP Results in Less GFR Meta Analysis: Lower SBP Results in Less GFR Decline in Diabetics and Non-DiabeticsDecline in Diabetics and Non-Diabetics
95 98 101 104 107 110 113 116 119
r = 0.69; P <0.05
MAP (mm Hg)
GFR
(mL/min/year)
Untreatedhypertension
0
-2
-4
-6
-8
-10
-12
-14Parving HH et al. Br Med J. 1989Viberti GC et al. JAMA. 1993Klahr S et al. N Eng J Med. 1993*Hebert L et al. Kidney Int. 1994Lebovitz H et al. Kidney Int. 1994
Maschio G et al. N Engl J Med. 1996*Bakris GL et al. Kidney Int. 1996Bakris GL. Hypertension. 1997GISEN Group. Lancet. 1997*
*:Studies in nondiabetic nephropathy. Bakris GL et al. Am J Kidney Dis. 2000;36:646-661.
140/90130/85
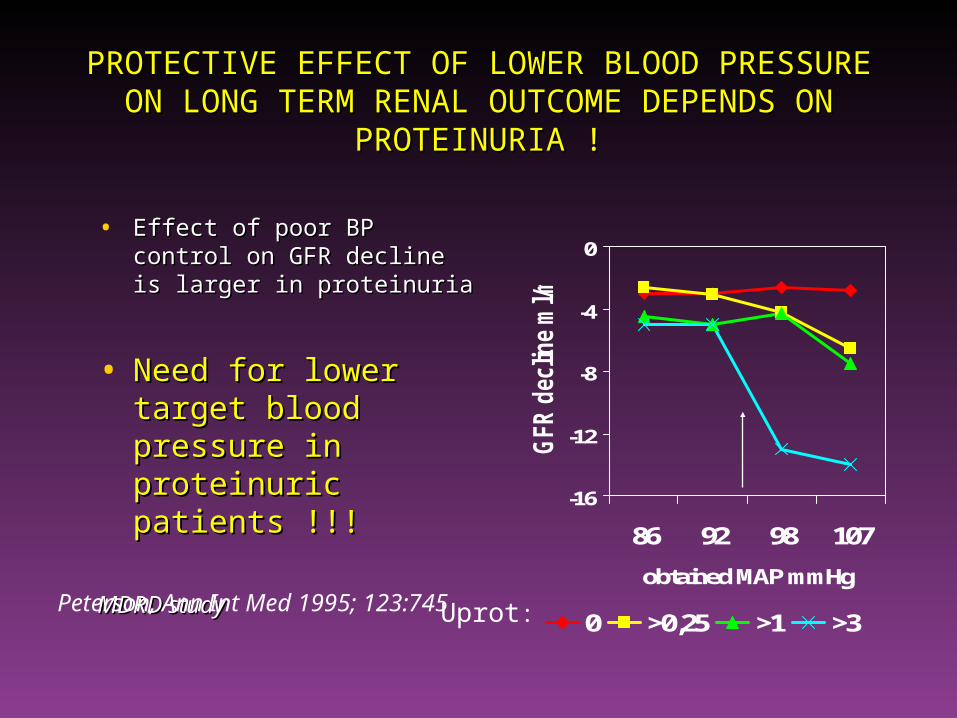
PROTECTIVE EFFECT OF LOWER BLOOD PROTECTIVE EFFECT OF LOWER BLOOD PRESSURE ON LONG TERM RENAL OUTCOME PRESSURE ON LONG TERM RENAL OUTCOME
DEPENDS ON PROTEINURIA !DEPENDS ON PROTEINURIA !
• Effect of poor BP control on Effect of poor BP control on GFR decline is larger in GFR decline is larger in proteinuriaproteinuria
• Need for lower target Need for lower target blood pressure in blood pressure in proteinuric proteinuric patients !!!patients !!!
MDRD studyMDRD study
-16
-12
-8
-4
0
86 92 98 107
obtained MAP mmHg
GFR d
ecline m
l/m
in/y
r
0 >0,25 >1 >3Peterson, Ann Int Med 1995; 123:745
Uprot:
Patients with vulnerable Patients with vulnerable kidneys need a lower kidneys need a lower
blood pressure !blood pressure !
ProteinuriaProteinuria
DiabetesDiabetes

No specific vulnerability:No specific vulnerability:
More liberal regimen jusitifiedMore liberal regimen jusitified

The remedyThe remedy
Lifestyle intervention; Drug treatment
Lower blood pressure
Reduction target organ damage > Better outcome
BENEFIT OF TREATMENT IS NOT EQUAL FOR ALL PATIENTS !
LIFESTYLE INTERVENTION & DRUG TREATMENT CAN POTENTIATE EACH OTHER !
INTERVENTION CAN IMPROVE OUTCOME ALSO INDEPENDENT OF EFFECT ON BLOOD PRESSURE !

Control of sodium status improves response Control of sodium status improves response to RAAS-blockadeto RAAS-blockade
0
1
2
3
4
5
6
7
80
85
90
95
100
105
110
Uprot, g/dMAP, mmHG
Heeg, Kidney Int 1989; 36,272
0
0.5
1
1.5
2
2.5
3
3.5
4
80
85
90
95
100
105
Vogt en Waanders, JASN 2008
ACEi
AIIA

The remedyThe remedy
Lifestyle intervention; Drug treatment
Lower blood pressure
Reduction target organ damage > Better outcome
BENEFIT OF TREATMENT IS NOT EQUAL FOR ALL PATIENTS !
LIFESTYLE INTERVENTION & DRUG TREATMENT CAN POTENTIATE EACH OTHER !
INTERVENTION CAN IMPROVE OUTCOME ALSO INDEPENDENT OF EFFECT ON BLOOD PRESSURE !

Effect of high salt intake on long term Effect of high salt intake on long term outcome outcome
500
700
900
1100
1300
1500
1700
1900
2100
7,5 8 8,5 9 9,5 10 10,5
UNaV (g/day)
dea
ths
stro
ke p
er 1
00.0
00/y
r
Is it all blood pressure??

Salt intake: effects on mortality in general Salt intake: effects on mortality in general populationpopulation
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
haza
rd ratio
low salt high salt
• Increased mortality risk Increased mortality risk per 6 gr rise in salt intakeper 6 gr rise in salt intake
• Interaction with BMI > 27Interaction with BMI > 27– HR normal weight: 0,98 nsHR normal weight: 0,98 ns– HR overweight : 1,56 HR overweight : 1,56
– Effect ONLY present in Effect ONLY present in overweight subjectsoverweight subjects
Tuomilehto, Lancet 2001; 357:848-51
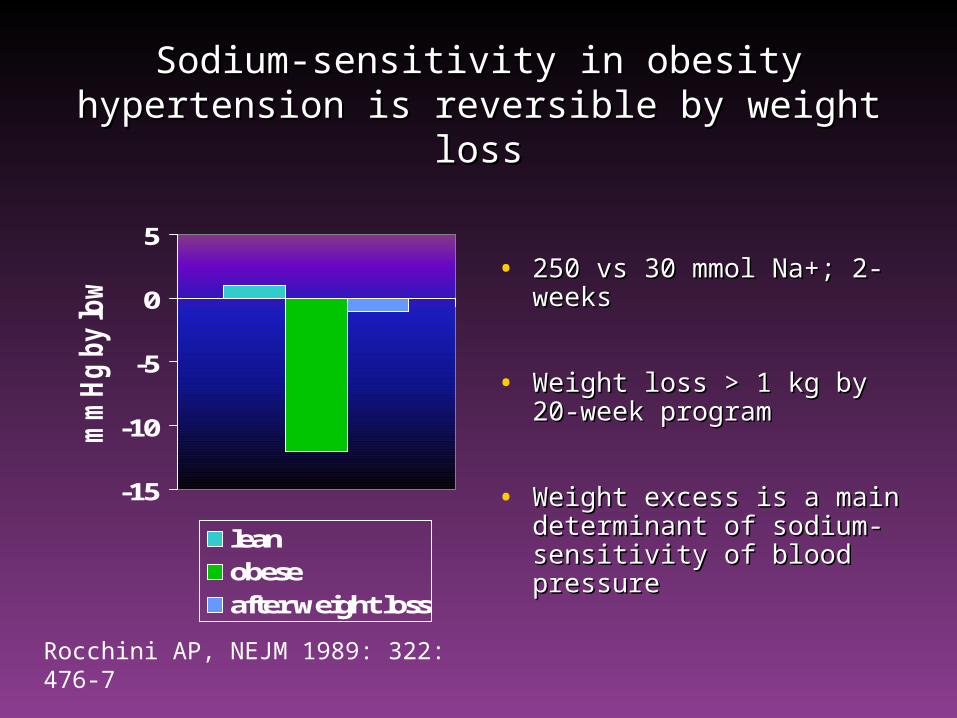
Sodium-sensitivity in obesity hypertension is Sodium-sensitivity in obesity hypertension is reversible by weight lossreversible by weight loss
-15
-10
-5
0
5
mm
Hg by low salt
leanobeseafter weight loss
• 250 vs 30 mmol Na+; 2-250 vs 30 mmol Na+; 2-weeksweeks
• Weight loss > 1 kg by 20-Weight loss > 1 kg by 20-week programweek program
• Weight excess is a main Weight excess is a main determinant of sodium-determinant of sodium-sensitivity of blood sensitivity of blood pressurepressure
Rocchini AP, NEJM 1989: 322: 476-7

Salt intake: effects on mortality in general Salt intake: effects on mortality in general populationpopulation
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
haza
rd ratio
low salt high salt
• Increased mortality Increased mortality risk per 6 gr rise in risk per 6 gr rise in salt intakesalt intake
– Effect Effect INDEPENDENT OF INDEPENDENT OF BLOOD PRESSURE! BLOOD PRESSURE!
Tuomilehto, Lancet 2001; 357:848-51

High salt increases albuminuria in High salt increases albuminuria in healthy subjects, independent of blood healthy subjects, independent of blood
pressurepressure
6
6.5
7
7.5
8
8.5
3 g/day 12 g/day
UAlb, m
g/24h
• A rise in salt intake A rise in salt intake leads to a 25 % leads to a 25 % rise in UAE in rise in UAE in healthy volunteers healthy volunteers without even a rise without even a rise in BP ! in BP !
JA Krikken, Kidney Int 2007: 71: 260-265

Salt status: associated with albuminuria independent of BP, but dependent on BMI
(n=7913, Prevend population)
Urinary sodium excretion (mmol/24h)
50 100 150 200 250 300
UA
E (
mg
/24
h)
6
7
8
9
10
11
12
BMI third tertileBMI second tertileBMI first tertile
JC Verhave, Eur J Clin Invest 2004: 256: 324-30
27,3-67
24-27,3
16,3-24
BMI:

INTERACTION SODIUM STATUS-WEIGHT INTERACTION SODIUM STATUS-WEIGHT EXCESSEXCESS
• Sodium sensitivity of blood pressureSodium sensitivity of blood pressure
• Blood pressureBlood pressure
• CV outcomes – BP dependent AND BP CV outcomes – BP dependent AND BP independentindependent
• Risk markers (NT-proBNP, UAE)Risk markers (NT-proBNP, UAE)

SODIUM EXCESS AND WEIGHT EXCESSSODIUM EXCESS AND WEIGHT EXCESS
Deadly twins! Deadly twins!
In normotensive AND in hypertensive subjects

SODIUM EXCESS AND WEIGHT EXCESSSODIUM EXCESS AND WEIGHT EXCESS
Deadly twins! Deadly twins!
MECHANISM?

Effect of overweight on extracellular Effect of overweight on extracellular volume during low vs high sodium volume during low vs high sodium
intakeintake
17
18
19
20
21
22
23
low sodium high sodium
ECV, liter
s
BMI 22 BMI 25
• In slightly overweight In slightly overweight young men, ECV is higher young men, ECV is higher than in lean subjects, ONLY than in lean subjects, ONLY during high sodiumduring high sodium
• This is NOT accompanied This is NOT accompanied by higher blood pressure.by higher blood pressure.
• It IS accompanied by a rise It IS accompanied by a rise in NT-proBNP: marker of in NT-proBNP: marker of CV risk CV risk
Visser en Krikken et al, Obesity, in press
Weight excess/obesityWeight excess/obesity
• Volume expanded during high sodiumVolume expanded during high sodium
• In hypertensives: > rise in blood In hypertensives: > rise in blood pressurepressure
• In young normotensives: no signs at In young normotensives: no signs at the outsidethe outside

SODIUM SENSITIVITY = HIGHER ECVSODIUM SENSITIVITY = HIGHER ECV
• In young In young healthy healthy volunteers ECV volunteers ECV is higher in SS is higher in SS individuals, in individuals, in particular, but particular, but not only, during not only, during high sodiumhigh sodium
14
16
18
20
22
low sodium high sodiumEC
V, liter
s
SR SS
F.Visser, Am J Hyp 2008,21:323

Weight excess and high sodiumWeight excess and high sodium
A sodium-induced rise in BP may be the tip of the Iceberg, the ECV expansion
underneath being the true pathogenetic factor
hypothesis
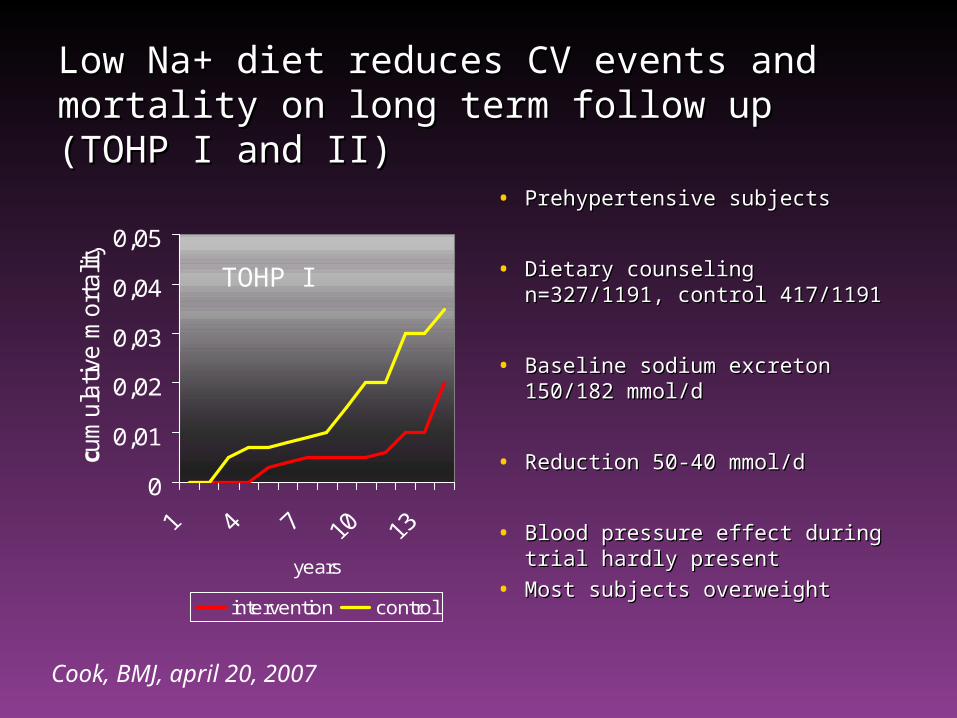
Low Na+ diet reduces CV events and Low Na+ diet reduces CV events and mortality on long term follow up (TOHP I and mortality on long term follow up (TOHP I and II)II)
0
0,01
0,02
0,03
0,04
0,05
years
c um
ula
tive m
ort
alit
y
intervention control
• Prehypertensive subjectsPrehypertensive subjects
• Dietary counseling Dietary counseling n=327/1191, control 417/1191 n=327/1191, control 417/1191
• Baseline sodium excreton Baseline sodium excreton 150/182 mmol/d150/182 mmol/d
• Reduction 50-40 mmol/dReduction 50-40 mmol/d
• Blood pressure effect during Blood pressure effect during trial hardly presenttrial hardly present
• Most subjects overweightMost subjects overweight
Cook, BMJ, april 20, 2007
TOHP I

The remedyThe remedy
Lifestyle intervention; Drug treatment
Lower blood pressure
Reduction target organ damage > Better outcome


Do you know the sodium intake of your Do you know the sodium intake of your patients?patients?

Do you know the sodium intake of your Do you know the sodium intake of your patients?patients?
24-hour urine: unbiased and cheap assessment of sodium intake
Allows unbiased feedback for patients

Do you know the Do you know the PROTEINPROTEIN intake of your intake of your patients?patients?
24-hour urine: unbiased and cheap assessment of protein intake (urea excretion)
Allows unbiased feedback for patients


Recommendations Recommendations GezondheidsraadGezondheidsraad• limited effect of lowering sodium intake on limited effect of lowering sodium intake on
prevention of hypertension on population levelprevention of hypertension on population level
• use modest amounts of sodium (max 6 g)use modest amounts of sodium (max 6 g)
• combine these diet changes with combine these diet changes with low fat and high low fat and high fruit intakefruit intake
• hypertensives: replace other minerals for sodiumhypertensives: replace other minerals for sodium

















