141
Imaging for the Family Physician TAFP Pulse Virtual Conference August 14, 2021

Imaging for the Family Physician
TAFP Pulse Virtual ConferenceAugust 14, 2021

Grant Fowler, MD
Professor and Chair, Dept. of FM/CMTCU/UNTHSC Medical School
JPS (Tarrant County) Healthcare System Fort Worth, Texas

Disclosure
• Consultant for AstraZeneca

Making Effective Use of Diagnostic Imaging
Goals and ObjectivesAttendees will be better able to discuss:
• Importance and appropriate selection of imaging studies• Pearls of imaging with ultrasound, computerized
tomography(CT), magnetic resonance (MRI) and cardiac imaging

Making Effective Use of Diagnostic Imaging
• Family doctors current use of diagnostic imaging in office• Benefits and limitations of various imaging studies• Most appropriate imaging for some common FM problems• How to use imaging to avoid catastrophes• When to use/avoid contrast with imaging
Diagnostically, What are Family Physicians Doing Now in the Office?

AAFP Data (July 2008)Diagnostic Procedures in Office
• ECG 90.3• MSK injections 87.0• Derm procedures 80.0• Endometrial bx 52.5• X-ray 43.1• Colposcopy 33.6• Vasectomy 25.3• Cosmetic procedures 21.7

AAFP Data (July 2008)Diagnostic Procedures in Office
• Holter monitor 25.1• Exercise testing 16.5 (? in hospitals)• LEEP 11.3• Physical therapy 12.3• Ob ultrasound 14.7• Non Ob ultrasound 12.9• Echo 11.2• EGD 3.8 (more in hospitals)• Colonoscopy 3.7 (more in hospitals)
(> 50% in certain Texas counties)

Why is Diagnostic Imaging Important?

Diagnostic Errors are Common
• More common than medication and surgical errors in primary care1-8
• Incidence unknown, estimated 5 to 15%, depending on setting and research method3,4,9
• Leading cause of malpractice claims and preventable adverse events in hospitals6

Diagnostic Errors Common
• Most common missed catastrophic diagnoses are abdominal aortic aneurysm (AAA), appendicitis, cancer, pulmonary embolism, coronary artery disease8,10,11

Getting Most From Diagnostic Imaging
• To avoid missing catastrophic diagnoses, first, you have to think about them!
• Then you have to know which diagnostic test to use (and what is available)

How did we get here with imaging?

History of Ultrasonography1880 Europe
Quartz and other crystals found to emit acoustic vibrations when compressed. These vibrations can be converted into electrical energy. From the Greek word “piezo”, or to “press”, the word piezoelectric is derived.
1917 FranceMosaic quartz crystals compressed between steel plates used to generate and receive sound waves underwater in search of enemy submarines. This became sonar in World War II.

History of Ultrasonography
1937 Soviet UnionUltrasound used in testing solid materials.
1952 United StatesFirst picture of solid human tissue produced at the University of Colorado. (A)mplitude or A-mode images were produced.




A-mode (Amplitude Mode)
• Amplitude from an oscilloscope


B Scan
• Computerized B scan (as opposed to B- mode scanning) rapidly replaced by CT scan

Further Developments
• (B)rightness or B-mode scanning developed resulting in two-dimensional images
• Real-time imagining allows for “live” scanning with improved clinical correlations
• Portable sonography allows for imaging outside of the radiology department and more affordable equipment

Point of Care Ultrasound (POCUS-ER) Characteristics
• Exam is well-defined• Purpose is to improve patient outcome• Exam is focused and goal-directed• Exam findings easily recognizable• Exam is easily learned• Exam is quickly performed• Exam performed at bedside
Kendall JL, Hoffenberg SR, Smith RS. History of emergency and critical care ultrasound: the evolution of a new imaging paradigm. Crit Care Med 2007 May;35(5 Suppl):S126-S130.

Ultrasound Physics
• Air is scanner’s worst enemyAir-filled images are difficult to visualize and may impair view of surrounding organs (e.g., lungs, gastrointestinal tract)
• Fluid is scanner’s best friendFluid filled organs are more readily visualized and may act as “windows” for surrounding tissue (e.g., heart, liver, spleen, bladder, and uterus)


Ultrasound Limitations
• Ultrasound is very operator and interpreter dependent• Difficult to use near bony structures

Ultrasound Limitations
• Very dependent upon patient body habitus and conditions
(e.g., early morning fasting is best time for abdominal ultrasound, when there is the least bowel air)
(e.g., full bladder enhances abdominal ultrasound scanning of pelvis)

Ultrasound Benefits
• No radiation!• About half the cost of CT (¼ the cost of MRI)• Live scanning, instant results, patient can be moved around



Ultrasound Special Abilities
• Can use higher frequency ultrasound with special probes for better resolution than CT
(e.g., transesophageal echo, transvaginal ultrasound)

Ultrasound Special Abilities
• Portable, live scanning (videos)• Ultrasonically directed procedures• Hi frequency (small-parts) probes very good for examining
objects near skin surface (e.g., breast or thyroid nodule, testicle, vascular, musculoskeletal)

Ultrasound Interpretation
• Fluid is dark by convention • Solid structures are white or “echogenic” (hyperechoic) by
convention• If solid and larger than 3mm in diameter, will usually cast
a shadow

Ultrasound Orientation
• Transverse views on ultrasound (marker dot turned toward patients' right side) same as CT orientation
• Longitudinal (sagittal) views (marker dot turned toward patient’s head)





Back to those catastrophes!

Getting Most From Diagnostic Imaging (AAA)
• AAA is the 10th leading killer in males in America and the incidence is increasing
• Physical exam notoriously inaccurate for diagnosing, sensitivities range from 24 to 60%
• When a patient presents with symptomatic AAA, diagnosis missed in 30 to 60% of cases

AAA
• Most common missed diagnosis for AAA is left sided renal colic
• Therefore, think AAA in the appropriate patient, even in the patient with hematuria!

AAA
• Medicare reimburses for one lifetime ultrasound screen for AAA
• Family history of AAA or men aged 65 to 75 who have ever smoked 100 cigarettes

AAA
• CT abdomen is the gold standard• FAST exam in Emergency Dept (ED) can be performed in
5 min using US

Trauma: The FAST Scan
• FAST: Focused Abdominal Sonography of Trauma• Rapid, focused abdominal and cardiac views for diagnosis
of free abdominal or pericardial fluid

Trauma: The FAST Scan
• Fluid is proxy marker for significant intraabdominal or cardiac injury
• Can also be used to rule out AAA

Fresh Blood Looks BLACK (Anechoic) and Moves Thus:

The “FAST Diamond”
Heart
SplenorenalMorison’spouch
Pelvis

FAST (+) = (+)Fluid = OR
Negative FAST = Observe and repeat scan shortly OR CT scan




What else in the Belly? Cholecystitis
• Clinical accuracy only 50%• Positive Sonographic Murphy’s sign is probably most
accurate way to diagnose • This is pain with inspiration while palpating over RUQ (and
gallstones present)• Some surgeon’s also want HIDA scan



Nephrolithiasis
• CT stone protocol is preferred diagnostic test, if available



Renal Cyst
• Very common, 50% of people by age of 50 have one (hepatic cysts slightly less common)


Another Abdominal Catastrophe –Ruptured Ectopic
• Attempt to rule in intrauterine pregnancy• When intrauterine pregnancy confirmed, likelihood of
“combination pregnancy” is < 1 in 2500 (except patients taking ovulatory meds)


US and bHCG Correlations for IUP

Yet Another Possible Abdominal Catastrophe – Chronic Abdominal Pain
• If not possibly attributable to any other diagnosis (e.g., GI related, colicky in nature), 10% of chronic abdominal pain (> 1 month duration) in patient over 50 years of age is due to malignancy
• These patients probably warrant CT scan



Imaging Pancreas
• Pancreas not visualized in up to 50% of abdominal ultrasounds due to bowel gas pattern
• CT scan usually adequate• MRI can be used to fine tune (e.g., MRCP vs. ERCP)

Imaging Acute Abdominal Pain (All with Level of Evidence C)
• Ultrasound initial imaging of choice RUQ• CT initial imaging of choice RLQ and LLQ• Conventional radiography limited value• Beta HCG all reproductive age women before imaging
acute abd pain
Cartwright SL, Knudson MP: Am Fam Physician. 2015 Apr 1;91(7):452-459.

MRI in the Belly
• CT is usually adequate for ruling out malignancies in the abdomen
• Exception: Density of hepatocellular carcinoma very similar to surrounding liver: Therefore, MRI preferred
• Searching for metastases to lymph nodes, especially pelvis, MRI probably preferred

MRI
• Approximately twice the cost of CT• No radiation• Takes much longer to perform than ultrasound or CT • Can be problem with claustrophobic patient (open MRI
loses resolution)

MRI
• Basically, used to fine tune what is seen or could be seen on CT (subtle cancers, metastases to lymph nodes)
• Exception: CT head better for noting blood than MRI (e.g., subarachnoid hemorrhage)

Getting Most From Diagnostic Imaging –Contrast Dye
• When to add contrast to CT scan?• To help better visualize internal organs and the structures
around them

Contrast Dye for CT
• IV contrast brightens internal organs, arteries, veins, and tissue
• Often important for diagnosing subtle cancers

Contrast for CT
• For abdominal CT, both oral and IV are often used at same time
• Oral barium in abdominal CT is 2% of concentration of regular barium, so have to wait a week or more until passed out of colon
Contrast Dye Allergy?
• No longer contraindication if allergic to shellfish (tropomyosin) or topical iodine solution (other substances in solution)
• No such thing as iodine allergy (iodine is essential to life, present in thyroid hormone)
www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast%20Manual/2013_Contrast_Media.pdf

Contrast Dye Allergy?
• Prior allergic reaction to contrast increases risk five-fold• Prior anaphylactic reaction to anything should raise
concern a little
www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast%20Manual/2013_Contrast_Media.pdf

Contrast Dye Allergy?
• Most forms atopy increases risk by two to three-fold• A history of asthma may increase the risk
www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast%20Manual/2013_Contrast_Media.pdf

Contrast Dye and Metformin?
• IV iodinated contrast media in patients taking metformin only a concern in the presence of underlying renal dysfunction
• Metformin should be temporarily discontinued prior to IV radiocontrast study (DC at time of study and hold for 48 hours)
www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast%20Manual/2013_Contrast_Media.pdf

Contrast for CT
• For chest CT, IV contrast generally indicated• Exceptions to using contrast with chest CT: If
contraindicated, when doing coronary calcium scoring or when screening for lung cancer

MRI Contrast
• Gadolinium most common• Shortens relaxation time of atoms within body tissues under
very strong magnetic field (e.g., protons in water)• Very useful for MRA, disruption of blood brain barrier (by
stroke or tumor)

What about Dizzy Patient?
• Most patients do not require imaging (MRI) (Level of Evidence C when no other neurologic abnormalities)– Unless suspected posterior fossa tumor or stroke– New onset vertigo associated with dysarthria or numbness– Age > 65 with CV risk factors (esp. if presyncope)– CT only if post concussion or suspected normal pressure
hydrocephalus (NPH = dementia, incontinence, gait abnormality)

Back to those Catastrophes: Pulmonary Embolism
• CT angiogram procedure of choice• Has slight false positive rate• VQ scan if unable to use contrast


Extremities – Deep Venous Thrombosis
• Clinical diagnosis reported notoriously inaccurate – 50% at best
• However, this was older data based on seriously ill hospitalized patients
• More recent data says history/Wells criteria useful, especially in ambulatory patients

Extremities – Deep Venous Thrombosis
• Venography previously “Gold Standard”
– 10-20% incidence of post-venography syndrome– Usually don’t compare opposite side or repeat– Unavailable after-hours, remote hospitals– Dependent on venous access

Extremities – Deep Venous Thrombosis
• Accuracy duplex scanning compared to venography –limited in obese patients, cannot visualize above the inguinal ligament or below the popliteal vein (questionable clinical significance)

Wells Scoring System(Wells PS, JAMA. 2006 Jan 11;295(2):199-207)
Clinical Variable ScoreActive cancer (ongoing treatment or active within the last 6 months or palliative care for cancer)
1
Paralysis, paresis, or recent plaster immobilization of the lower extremities
1
Recently bedridden for 3 or more days, or major surgery within the last 12 weeks requiring regional or general anesthesia
1
Localized tenderness along the distribution of the deep venous system
1
Entire leg swelling 1

Wells Scoring System (Wells PS, JAMA. 2006 Jan 11;295(2):199-207)
Clinical Variable ScoreCalf swelling at least 3 cm larger in circumference than that of the asymptomatic leg, measured 10 cm below the tibial tuberosity
1
Pitting edema confined to the affected leg
1
Distended collateral superficial veins (not varicosities)
1
Previously documented DVT 1Alternative diagnosis at least as likely as DVT
-2
Scoring method: if 1 or less, DVT unlikely; if 2 or greater, DVT likely

Compression Ultrasonography
• This is currently most common method of excluding DVT in United States
• However, most tests also incorporate duplex scanning

Deep Venous Thrombosis – Interpretation
• Echogenic matter in lumen is diagnostic and thickened walls should be compared to opposite side.
• Record venous response to compression, Valsalva and respiration

Deep Venous Thrombosis – Interpretation
• Valve motion should be recorded when noted• Wells system scoring, d-dimer, compression US or duplex
scanning should be completed before withholding anticoagulation

Final Catastrophe –Coronary Artery Disease

Echocardiography
• An echocardiogram is merely an ultrasound of the heart• It is performed with the transducer at 2nd to 4th intercostal
space, parasternum, wherever best window obtained (same location as where we use stethoscope)

Transducer Positions in Cardiac Scanning (Stethoscope)

Echocardiography
• Orientation is shifted: – Transverse = Short axis of heart– Longitudinal = Long axis of heart

Echocardiography
• Marker dot directed at 8 o’clock (right hip) in short axis view (basically transverse view of heart)
OR• Marker dot directed at 4 o’clock (left hip) in long axis view
(basically longitudinal view of heart)



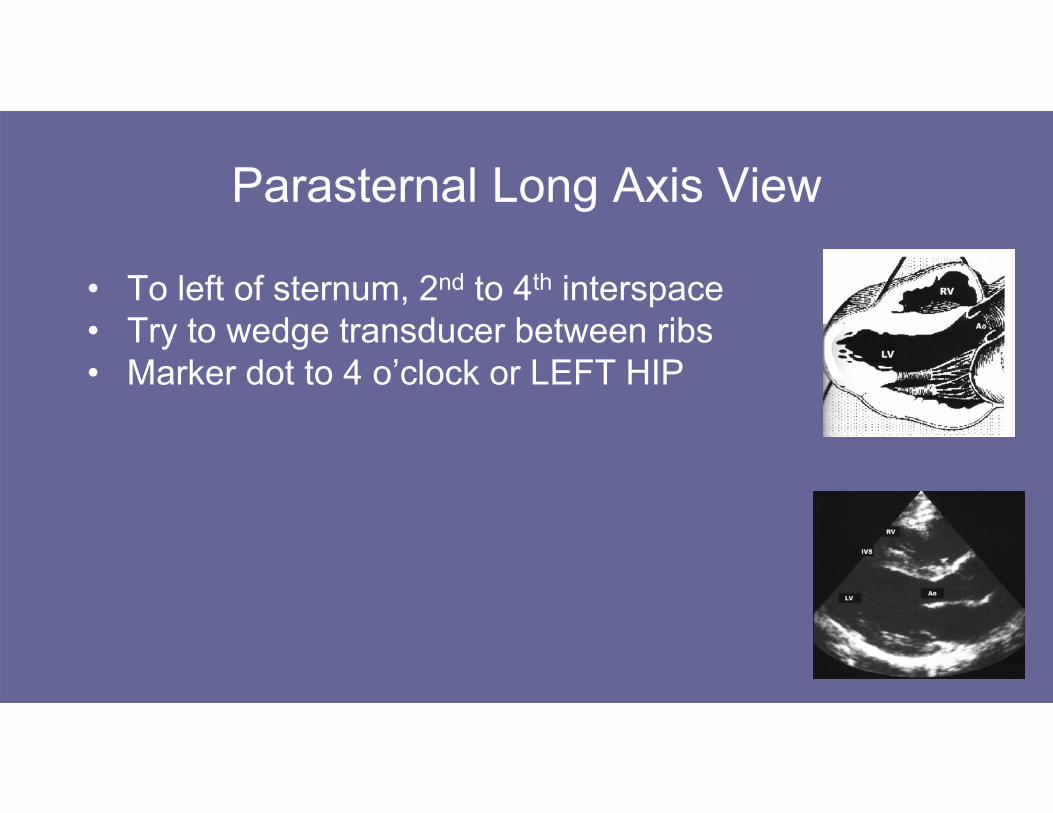
Parasternal Long Axis View
• To left of sternum, 2nd to 4th interspace• Try to wedge transducer between ribs• Marker dot to 4 o’clock or LEFT HIP



Apical View (4-chamber View)
• Marker dot angle towards RIGHT HIP• Beam directed at RIGHT SHOULDER


Echocardiogram
• Most common reason ordered in United States is to assess ejection fraction (important for prognosis)
• Since the late 1990s, stress echocardiogram has had same sensitivities, specificities, and accuracy as myocardial nuclear perfusion imaging

Myocardial Perfusion Imaging
• Uses same mechanism as exercise ECG stress testing: ischemia knocks out sodium/ potassium ATPase pump at myocyte/cellular level
• Cardiac nuclear substrate is potassium analog (e.g., thallium or technicium)
• Knockout area on image is either due to ischemia (reversible defect) or scar (fixed)

Planar vs. SPECT (Single Photon Emission Computed Tomography)
PLANAR SPECT
Older technology CT Scan Quality
Sensitivity is 75-80% Sensitivity and specificity both above 90%
Specificity 80% Bullseye technique
16–17-millimeter resolution





When to Add Cardiac Imaging?
• Plain ECG stress test can risk stratify patient• Plain ECG cannot tell which vessels involved when
positive test, cardiac imaging can

American Heart Association (AHA)/ American College of Cardiology (ACC)
Criteria for Adding Cardiac Imaging
• If the patient can exercise, that is the preferred way to test for CAD
• AHA/ ACC recommend a stepwise diagnostic strategy, if the baseline ECG can be interpreted, the preferred initial test is exercise stress ECG

PHARMACOLOGIC STRESS (Patient Cannot Exercise)
Vasodilator (adenosine, dipyridamole, regadenoson)
a. Produces coronary vasodilatationb. Steal phenomenac. Sensitivity, specificity, possibly prognostic ability matches exercised. Avoid theophylline and caffeine for 48 hourse. Chest pain normal side effectf. Cannot correlate symptoms with ischemia (ET still procedure of
choice)

Dobutamine and Arbutamine
a. Produces ischemia by increasing cardiac oxygen demandb. Superior regional wall motion studyc. Can be used with bronchospasm

• Vasodilators seem preferable for Myocardial Nuclear Perfusion Imaging
• Dobutamine and Arbutamine seem preferable for Stress Echo

PET Scanning
• Resolution – 6 millimeters (able to inject higher radiation dose with short t ½)
1) Perfusion (similar to thallium/technicium for cardiac uses)a. Rubidium chloride R82b. Oxygen – 15 labeled waterc. Nitrogen – 13 labeled ammonia

PET Scanning
2) MetabolismLabeled glucose, fatty acids and amino acids that viable tissue will uptake (cyclotron produced isotopes of carbon, with nitrogen and fluorine attached)Used for cardiac viability and cancer




L. Gould
Small basal inferior scar with myocardial stealin distribution of Posterior Descending

The Future?

Periodic Health or Wellness Exam
• Ultrasonically-enhanced periodic health exam in elderly found a new diagnosis in 31% of patients who had already undergone conventional exam
• 7% required prompt treatment for a serious, unsuspected condition
Siepel T (et al) J Fam Pract 49:628–632, 2000.

Multidetector/Multislice CT Angiogram





How Much Radiation?



Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE)
• 10,003 patients with chest pain and suspected CAD • Randomized to CTA or functional testing (10% stress ECG,
22% stress echo, 68% MPI)
Douglas PS, Hoffmann U, Patel MR, et al. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med 2015;372:1291-1300

Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE)
• No difference in endpoints (3.3% vs 3.0%, p=.75)• Endpoints: all cause mortality, MI, hosp for UA, major
complications CV procedure (stroke, bleeding, renal failure, anaphylaxis)
Douglas PS, Hoffmann U, Patel MR, et al. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med 2015;372:1291-1300

Choosing Wisely Campaign (ABIM)
• Don’t order x-ray of lumbar spine for first 6 weeks unless red flags present (serious or progressive neurologic deficits or suspected serious underlying condition e.g., osteomyelitis)
AAFP Twenty Things Physicians and Patients Should Question, updated 2021

Appropriate Use Criteria for Advanced Diagnostic Imaging
• Protecting Access to Medicare (PAMA, 2014), testing phase 2020, implementation pushed back to 2022
• Appropriate use criteria (AUC) for CT, MRI, PET and nuclear medicine
• Required to consult a Clinical Decision Support Mechanism (CDSM); evidence-based and available through a portal

References
• 1. Chandra A, Nundy S, Seabury SA: The growth of physician medical malpractice payments: evidence from the National Practitioner Data Bank. Health Aff (Millwood). 2005; Suppl Web.
• 2. Greenwald L. Failure to diagnose: putting the pieces together. A Review of closed claims in selected specialties 2002–2004. Boston, MA: ProMutual Group; 2004.

References
• 3. Berner ES, Graber ML: Overconfidence as a cause of diagnostic error in medicine. Am J Med; 2008; 121(5A): S2-S23.
• 4. Shojania KG, Burton EC, McDonald KM, Goldman L: Changes in rates of autopsy-detected diagnostic errors over time: a systematic review. JAMA 2003; 289(21): 2849-56.

References
• 5. Katz HP, Kaltsounis D, Halloran L, Mondor M: Patient safety and telephone medicine: some lessons from closed claim case review. J Gen Intern Med 2008;23(5): 517–22.
• 6. Leape LL, Brennan TA, Laird N, et al: The nature of adverse events in hospitalized patients: results of the Harvard Medical Practice Study II. N Engl J Med 1991; 324: 377-84.

References
• 7. Singh H, Thomas EJ, Petersen LA, Studdert DM: Medical errors involving trainees: a study of closed malpractice claims from 5 insurers. Arch Intern Med 2007; 167(19): 2030–6.
• 8. Phillips RL Jr., Bartholomew LA, et al: Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care 2004; 13(2): 121–6.

References
• 9. Elstein AS: Clinical reasoning in medicine. In: Higgs J, Jones MA eds. Clinical Reasoning in the Health Professions. Woburn, MA: Butterworth-Heinemann; 1995: 49-59.
• 10. Kachalia A, Gandhi TK, Puopolo AL, et al: Missed and delayed diagnoses in the emergency department: a study of closed malpractice claims from 4 liability insurers. Ann Emerg Med 2007; 49(2): 196–205.

References
• 11. Gandhi TK, Kachalia A, Thomas EJ, et al: Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med 2006; 145(7): 488-96.

















