4
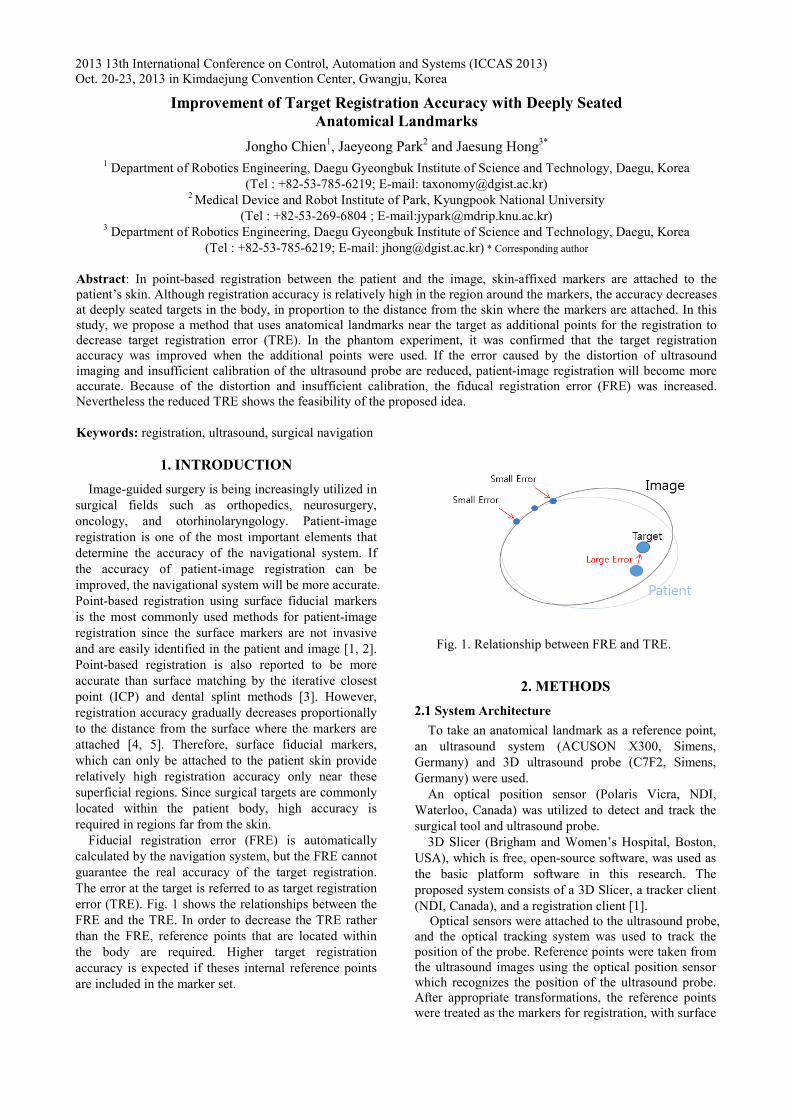
2013 13th International Conference on Control, Automation and Systems (ICCAS 2013) Oct. 20-23, 2013 in Kimdaejung Convention Center, Gwangju, Korea 1. INTRODUCTION Image-guided surgery is being increasingly utilized in surgical fields such as orthopedics, neurosurgery, oncology, and otorhinolaryngology. Patient-image registration is one of the most important elements that determine the accuracy of the navigational system. If the accuracy of patient-image registration can be improved, the navigational system will be more accurate. Point-based registration using surface fiducial markers is the most commonly used methods for patient-image registration since the surface markers are not invasive and are easily identified in the patient and image [1, 2]. Point-based registration is also reported to be more accurate than surface matching by the iterative closest point (ICP) and dental splint methods [3]. However, registration accuracy gradually decreases proportionally to the distance from the surface where the markers are attached [4, 5]. Therefore, surface fiducial markers, which can only be attached to the patient skin provide relatively high registration accuracy only near these superficial regions. Since surgical targets are commonly located within the patient body, high accuracy is required in regions far from the skin. Fiducial registration error (FRE) is automatically calculated by the navigation system, but the FRE cannot guarantee the real accuracy of the target registration. The error at the target is referred to as target registration error (TRE). Fig. 1 shows the relationships between the FRE and the TRE. In order to decrease the TRE rather than the FRE, reference points that are located within the body are required. Higher target registration accuracy is expected if theses internal reference points are included in the marker set. Fig. 1. Relationship between FRE and TRE. 2. METHODS 2.1 System Architecture To take an anatomical landmark as a reference point, an ultrasound system (ACUSON X300, Simens, Germany) and 3D ultrasound probe (C7F2, Simens, Germany) were used. An optical position sensor (Polaris Vicra, NDI, Waterloo, Canada) was utilized to detect and track the surgical tool and ultrasound probe. 3D Slicer (Brigham and Women’s Hospital, Boston, USA), which is free, open-source software, was used as the basic platform software in this research. The proposed system consists of a 3D Slicer, a tracker client (NDI, Canada), and a registration client [1]. Optical sensors were attached to the ultrasound probe, and the optical tracking system was used to track the position of the probe. Reference points were taken from the ultrasound images using the optical position sensor which recognizes the position of the ultrasound probe. After appropriate transformations, the reference points were treated as the markers for registration, with surface Improvement of Target Registration Accuracy with Deeply Seated Anatomical Landmarks Jongho Chien 1 , Jaeyeong Park 2 and Jaesung Hong 3* 1 Department of Robotics Engineering, Daegu Gyeongbuk Institute of Science and Technology, Daegu, Korea (Tel : +82-53-785-6219; E-mail: [email protected]) 2 Medical Device and Robot Institute of Park, Kyungpook National University (Tel : +82-53-269-6804 ; E-mail:[email protected]) 3 Department of Robotics Engineering, Daegu Gyeongbuk Institute of Science and Technology, Daegu, Korea (Tel : +82-53-785-6219; E-mail: [email protected]) * Corresponding author Abstract: In point-based registration between the patient and the image, skin-affixed markers are attached to the patient’s skin. Although registration accuracy is relatively high in the region around the markers, the accuracy decreases at deeply seated targets in the body, in proportion to the distance from the skin where the markers are attached. In this study, we propose a method that uses anatomical landmarks near the target as additional points for the registration to decrease target registration error (TRE). In the phantom experiment, it was confirmed that the target registration accuracy was improved when the additional points were used. If the error caused by the distortion of ultrasound imaging and insufficient calibration of the ultrasound probe are reduced, patient-image registration will become more accurate. Because of the distortion and insufficient calibration, the fiducal registration error (FRE) was increased. Nevertheless the reduced TRE shows the feasibility of the proposed idea. Keywords: registration, ultrasound, surgical navigation