12
Improving Systems of Care for Children with Special Health Needs Resources and Policy Options | SEPT 2017
Improving Systems of Care for Children with Special Health NeedsResources and Policy Options
| SEPT 2017

1 NATIONAL CONFERENCE OF STATE LEGISLATURES
BY TAHRA JOHNSON
More than one in five families has at least one child or youth with special health care needs. – Family Voices
More than 14.5 million children and youth (birth to 18 years old) in the United States have special health care needs.1 Given the financial and other consequenc-es experienced by families caring for these children and the impact on federal and state programs serving them, efforts to improve their systems of care are underway or being discussed in many states. This brief provides an overview of programs, funding options, standards, data, state approaches and policy options that states have used or may consider to improve systems of care for children and youth with special health care needs (CYSHCN) and their families.
In general, this population includes children from birth to age 18 with a wide range of physical and mental conditions. These include diabetes, asthma, develop-mental or intellectual disabilities, attention deficit disorder, autism, autoimmune deficiency and cancer, as well as complex conditions and other needs.
Approximately one-third of children and youth with special health care needs rely on Medicaid or the Children’s Health Insurance Program (CHIP) for some or all of their health care coverage.2 State policies for public and private insurance affect these children and their family’s health, well-being and financial security.
The National Survey of Children with Special Health Care Needs indicates that 25 percent of families with CYSHCN cut back on hours or stop working altogether to take care of their children.3 Families with CYSHCN have many needs beyond finan-cial concerns. Some families need assistance navigating services; accessing a medical home, education and training; or getting to and from appointments. States are explor-ing a variety of strategies to respond to the ever-changing health care landscape.
Overview of the CYSHCN System of Care The Title V Maternal and Child Health (MCH) Block Grants allocated to the states, operated through state-federal partnerships, support public health services to families in every state, the District of Colum-bia and eight territories. There are other programs that serve children with special health care needs; however, Title V is the only one with a specific responsibility for this population. At least 30 percent of the funds provided to each state must be designated for services for children with special health care needs. Title V programs for CYSHCN, which are located within each state, focus around six core health components. These are defined by the Maternal and Child Health Bureau (MCHB), Division of Services for Children with Special Health Needs, as essential components of an effective system of services for this population, including:
1. Access to coordinated, ongoing comprehensive care within a medical home
2. Family-professional partnership at all levels of decision-making
3. Access to adequate financing and private and/or public insurance to pay for needed services
4. Early and continuous screening for special health needs
5. Organized community services for easy use
6. Transition from youth to adult health care, work and independence.4
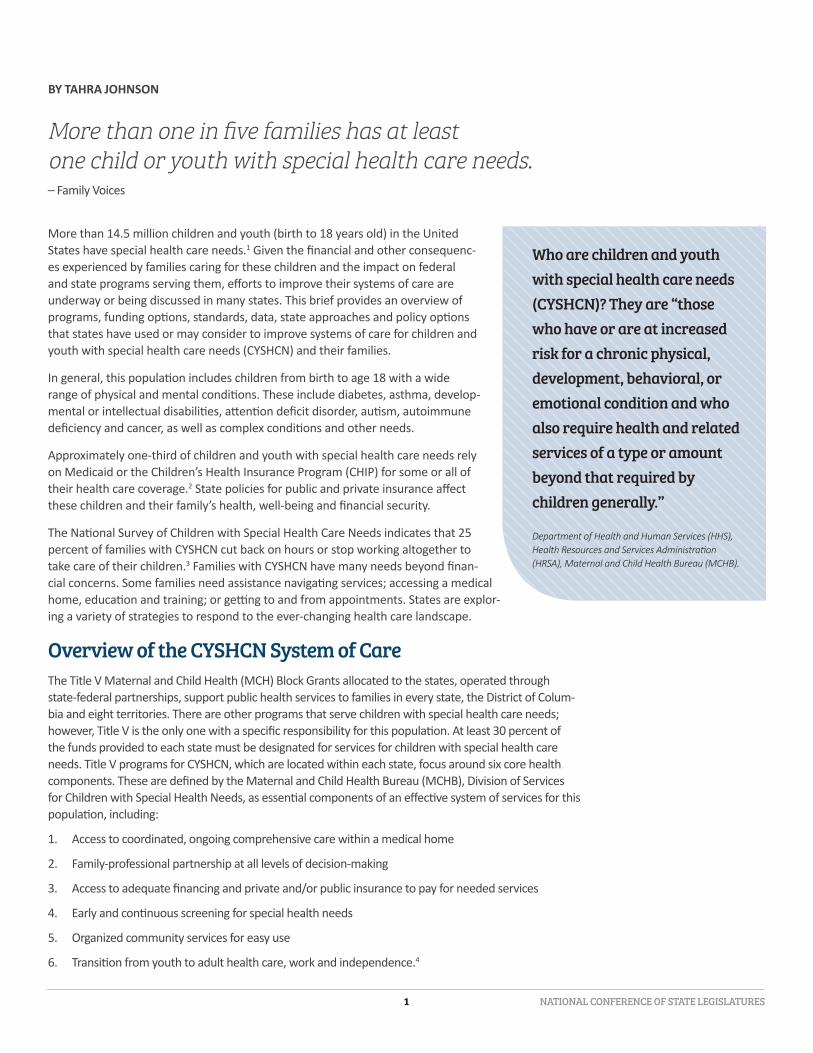
Who are children and youth with special health care needs (CYSHCN)? They are “those who have or are at increased risk for a chronic physical, development, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.”
Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA), Maternal and Child Health Bureau (MCHB).
NATIONAL CONFERENCE OF STATE LEGISLATURES 2
This system of care services, according to MCHB, is intended to be comprehensive, coordinated, com-munity-based, family-centered, and accessible, including a medical home and a set of supports that help families to navigate the various services that their children need.5 State Title V programs work with state Medicaid programs to work toward achieving an effective system of care.
A national focus on family and health professional partnerships at all levels of decision-making has been responsible for many improvements to health systems for CYSHCN at the state and national levels for more than two decades. Two funding initiatives from MCHB—the State Implementation Grants for Integrated Community Services for Children with Special Health Care Needs and the State Implementa-tion Grants for Enhancing the System of Services for Children and Youth with Special Health Care Needs through Systems Integration—have supported state efforts to enhance their service systems for CYSHCN. The three-year grants focus on promoting an understanding of the system of care for CYSHCN in the state, building public-private partnerships, expanding health care workforce capacity and strengthening performance measurement capabilities.6 Forty-eight grants were awarded over a 10-year period.7 These grants are just one example of the types of the initiatives supported by MCHB to build systems of care.8
CYSHCN Standards
The National Standards for Systems of Care for CYSHCN were developed by an expert workgroup convened by the Association of Maternal and Child Health Programs (AMCHP), to address the structural and process standards that comprise a system of care for CYSHCN. Many state agencies use these standards as a framework for their state plans. These standards are organized in 10 domains:
1. Screening, assessment and referral
2. Eligibility and enrollment
3. Access to care
4. Medical home, including pediatric preventive and primary care, care coordination and pediatric specialty care
5. Community-based services and supports, including respite care, palliative and hospice care, and home-based services
6. Family-professional partnerships
7. Transition to adulthood
8. Health information technology
9. Quality assurance and improvement
10. Insurance and financing
The Data Resource Center website includes national and state-level data on hundreds of child health indi-cators from two HRSA MCHB surveys: the National Survey of Children’s Health and the National Survey of Children with Special Health Care Needs. Legislators and staff can learn about the prevalence (number of CYSHCN) and needs of this population in their states and compare their states to others to identify policy gaps. The Data Resource Center can stratify and compare data on CYSHCN by age, race, ethnicity, sex, income, state, region, insurance type, household income, medical home status and other subgroups. For example, the data show:
• More than 21 percent of families of CYSHCN report financial problems due to their child’s health conditions.
3 NATIONAL CONFERENCE OF STATE LEGISLATURES
• 35.2 percent of minority CYSHCN were reported to have experienced one or more periods without insurance during the last year.
• 66.8 percent of Latino CYSHCN and 66.5 percent of black CYSHCN do not receive coordinated, ongoing, comprehensive care within a medical home.
• 37.2 percent of families devote one to four hours a week caring for their child with special health care needs.
• 25 percent of CYSHCN lived in families in which a family member cut back on work or stopped working.9
State Policy Options and Strategies for Systems of Care for CYSHCNState legislators may consider a number of policy options to improve the systems of care for children and youth with special health care needs.
SIMPLIFY MEDICAID/CHIP ENROLLMENT POLICIES AND PROCEDURES
Some states streamline enrollment and renewal of eligible children whom they know to be Medicaid-eligible because of their participation in other public programs, such as the Supplemental Nutrition Assistance Program (SNAP) and the Supplemental Nutrition Program for Women, Infants and Children (WIC). South Carolina uses eligibility information from SNAP and other public programs to expedite Medicaid renewals. Other states have adopted such fast-track eligibility, including Arkansas, Illinois, Oregon and West Virginia.
• Presumptive Eligibility. States may authorize hospitals, health care providers, schools and other qualified groups to screen children for Medicaid and CHIP eligibility, help families gather documentation and enroll children in coverage. Presumptive eligibility allows children to begin receiving care immediately without waiting through the full application process. At least 18 states have presumptive eligibility, according to the Centers for Medicare and Medicaid Ser-vices (CMS).10
• Continuous Eligibility. Several states provide children with 12 months of continuous Medicaid or CHIP coverage, even if their family income changes during the year. Continuous eligibility offers ongoing access to preventive and primary care, eliminates interruptions in coverage based on changes in family income or status, and reduces costs that would otherwise be used to redetermine eligibility whenever family circumstances change.11 Thirty-four states have 12-month continuous eligibility to keep children enrolled in Medicaid and/or CHIP, according to CMS.12
IMPROVE EARLY AND PERIODIC SCREENING
Identifying developmental disorders early can prevent more costly problems later and help infants and toddlers learn skills and meet developmental milestones during their early years. It can also help to ensure they receive services to meet their mental, physical, social and emotional needs. Medicaid’s Early Periodic Screening, Diagnostic and Treatment Program (EPSDT) covers the costs of periodic, comprehen-sive screenings, including vision, dental and hearing.13
Ensuring that EPSDT services are delivered effectively and efficiently offers a cost-effective opportunity for states to detect and treat problems early, before they become more expensive and difficult to treat. Some states provide screenings through child health clinics operated by local health departments with funds from the federal Title V Maternal and Child Health Services Block Grant. Increasing provider partic-ipation rates in state Medicaid programs may also increase children’s participation in EPSDT. Some states have informed families about EPSDT services through home visiting, Women, Infants and Children (WIC) and other programs.
Data Resource CenterLearn more about CYSHCN in your state from the Data Resource Center of the Child and Adolescent Health Measurement Initiative, funded by MCHB, located at the Johns Hopkins School of Public Health. The center provides easy access to state-specific data on CYSHCN collected through national surveys at www.childhealthdata.org.

NATIONAL CONFERENCE OF STATE LEGISLATURES 4
DISSEMINATE THE BRIGHT FUTURES GUIDELINES
Bright Futures is a detailed handbook providing “how to” instructions for well-child visits (birth – 21 years) produced by the American Academy of Pediatrics (AAP) with support from MCHB. It encourages using evidence-based pediatric care in every state. As with all children, regular well visits to health care providers promote good health and help prevent disease for children with special health needs.14 Screen-ing and careful attention are more likely to identify special needs early and allow health care profession-als to provide quality follow-up and intervention.15
USE TELEHEALTH TO EXPAND ACCESS TO CARE
Telehealth is a tool that uses technology to provide health care remotely. It can help states extend the health care workforce and increase access in rural areas. Even in urban areas, telehealth can help increase access to care by decreasing burdens for parents who must take time off work, and by simply improving convenience for patients. Telehealth can be used in a wide variety of ways, from primary care to specialty and acute care. It is also used in chronic care management and behavioral health, and in a variety of settings including schools and homes. For children with special health needs, such as autism, telehealth may increase the ability to connect with health care providers when travel for the child and parent is a challenge.
• Consider expanding telehealth definitions and/or reimbursement to additional modalities and specialties. For example, nearly all state Medicaid programs reimburse for telehealth services via live video, but far fewer reimburse for remote patient monitoring and store-and-forward, which is when information is sent to an intermediate location, where it is kept and forwarded at a later time to its final destination. In addition, examine which specialties and types of providers are included in the state’s reimbursement policies.
5 NATIONAL CONFERENCE OF STATE LEGISLATURES
• Convene stakeholders, such as providers, payers, consumers, vendors, etc., when considering policy decisions.
• Consider allowing patients’ homes to be classified as an originating site (the location of the patient) for telehealth services or removing restrictions on requiring a provider to be present.
SUPPORT HOME VISITING AND OTHER EVIDENCE-BASED DELIVERY SYSTEMS
State legislators play an important role in establishing effective home visiting policy. Home visiting programs support workers--such as trained nurses, social workers, early childhood educators or oth-er trained professionals—who help expecting and new parents in their homes. Participation in evi-dence-based home visiting services is voluntary and home visits help prevent child abuse and neglect, support positive parenting, improve maternal and child health, and promote child development and school readiness.16 Since 2008, more than 20 states have enacted legislation to address home visiting effectiveness, accountability and continuous quality improvement. These actions include creating comprehensive, statewide home vis-iting definitions, standards, outcomes, and funding and reporting requirements. State legislation also addresses the importance of home visiting as a component in states’ comprehensive early childhood systems.17
Minnesota passed legislation in 2008 to support and promote using health care homes to improve coordination of care for children with complex conditions, as recommended by the Governor’s Transformation Task Force and the Legisla-ture’s Health Care Access Commission.18 The Legislature charged the Minnesota Department of Health and Human Services with developing and implementing certification standards for health care homes and ensured they could receive “care coordination payments” from public and private insurers. Health homes are now a standard of care for children with special health care needs in Minnesota. The state Department of Health and Human Services developed a strategic plan (2013-2018) specifically around systems of care for CYSHCN; the overarching vi-sion is for Minnesota CYSHCN and their families to have increased access to health care homes as their primary care source.
ENCOURAGE INNOVATIVE PROVIDER REIMBURSEMENT AND INCENTIVES FOR APPROPRIATE SERVICES
For example, providers could receive incentives encouraging them to increase well-care visit rates for children with special health needs. These incentives could include paying bonuses for EPSDT screenings, realigned reimbursement levels to account for time and complexity of well-care visits of this population, or other financial incentives to increase well-care visit rates.19 The CMS State Innovation Models Initiative awards, also known as SIM awards, can be leveraged to support innovation and transformation of health care systems for CYSHCN, including payment issues. States are able to implement and test innovative payment and service models.
Illinois focuses services on screening and treatment for behavioral health in Medicaid for children and ad-olescents. The Illinois Children’s Mental Health Act (SB1951-PA 93-0495) created a cross-agency initiative called Screening, Assessment and Support Services (SASS). According to the National Academy for State Health Policy, SASS “provides prompt treatment and a single, statewide system for children and adoles-cents with acute behavioral health care needs.”20 Illinois Medicaid supports multiple billing codes to cover mental health and behavioral screenings in primary care settings.
The Texas Legislature passed legislation (SB7/Chapter 534) creating a system redesign for delivery of Medicaid services to individuals with intellectual and developmental disabilities. The Legislature direct-ed the Texas Health and Human Services department to establish a mandatory, capitated “STAR Kids” managed care program to provide Medicaid benefits to children and young adults with disabilities. In a capitated program, providers are paid by the number of people in the program over a period of time, ver-
NATIONAL CONFERENCE OF STATE LEGISLATURES 6
sus number of visits. The legislation required incorporating the Medically Dependent Children Program waiver services for community-based care, which are available to members who meet income, resource and medical requirements. The STAR Kids services started Nov. 1, 2016 and serves about 163,000 mem-bers across 13 service areas. Families have a choice between at least two health plans in their service area and can switch at any time.
DEVELOP PARTNERSHIPS WITH KEY STATE AND COMMUNITY STAKEHOLDERS
Working with Title V agencies, faith-based organizations and other community-based organizations can help mitigate barriers to access by increasing convenience to care. This might include offering care in more accessible locations, such as communities or schools, and improving well-care visit rates with evening and weekend appointments.21
Several state legislatures have established work groups or task forces specific to systems of care for CYSHCN. In 2011 the Michigan Legislature directed the state Department of Community Health to
develop a transition plan for Medicaid-eligible children who require special health care services into Medicaid managed care plans. The system changes required an 18-month planning process to ensure network adequacy and IT system capability to track the population and generate measures of utilization, access and quality of care, as well as to coordinate medical and behavioral health services. The state had a working group, consisting of many stakeholders that met monthly to discuss infrastructure needed to effectively transition CYSHCN into managed care.22 Michigan has a parent-directed section of the Children with Special Health Care Needs (CSHCS) Department named the Family Center for Children and Youth with Special Health Care Needs. These parents help shape CSHCS policies and procedures and help families navigate CSHCS.
Other State InitiativesStates are improving systems of care for CYSHCN in a variety of other ways, such as funding specific activities, evaluating pilot programs and creating standards of care or guidelines for this population. Below are examples of state initiatives intending to improve systems of care for CYSHCN.
Legislatures in at least 11 states have created funding mechanisms for certain unreimbursed catastrophic health care expenses for children and youth with special health care needs. Many are administered by, or in partnership with, the state Title V program. In Massachusetts and New Jersey, the Catastrophic Illness in Children Relief Funds are established through a fee on certain employers who are subject to unemployment compensation or health insurance at $1 or $1.50 per employee.23 The Col-orado Traumatic Brain Injury Trust Fund and the Georgia Brain and Spinal Injury Trust Fund are financed by surcharges from fines for driving under the influence (DUI).24
The California Legislature passed legislation (AB 1133/ Chapter 490) prioritizing placement for CYSHCN who are in foster care. The law grants priority consideration for these children to be placed with a foster parent who provides health services, such as an independent nurse.
Rhode Island developed a Pediatric Practice Enhancement Project in 2009 that placed and supported trained parent consultants in pediatric primary and specialty care practices. The parent consultants as-sisted families with accessing community resources and specialty services.25 The Department of Health conducted a cost-benefit analysis and documented cost savings through reduced emergency room visits.26 This was reported to the legislature, which provided funding to continue the project.
7 NATIONAL CONFERENCE OF STATE LEGISLATURES
Improving access to early childhood screenings, simplifying health insurance enrollment policies, aligning reimbursement structures for providers, and promoting telehealth are just some examples of policy deci-sions states have implemented that have significantly affected the lives of children and youth.
Oral Health for CYSHCN
Strategies to address low oral health participation rates in Medicaid might include:
• Expand pediatric dentistry residencies and training programs to include care of CYSHCN.
• Increase local services and pediatric dentists trained to treat CYSHCN.
• Encourage dental students to obtain training in caring for CYSHCN.
• Provide dental scholarships and incentives to specialize in treating CYSHCN.
• Provide dental scholarships and incentives to practice in rural areas and underserved areas.
• Increase Medicaid reimbursement.
For more information regarding CYSHCNNCSL RESOURCES
Bright Futures Issue Brief www.ncsl.org/research/health/the-bright-futures-guidelines-improving-children-s-health.aspx
Smart Investments in Children’s Health www.ncsl.org/documents/health/SmartInvestments914.pdf
Health Reform and Children with special needs www.ncsl.org/documents/health/Specialneeds914.pdf
Trends and Options for Covering Kids www.ncsl.org/documents/health/Coveringkids914.pdf
EXTERNAL RESOURCES
Association of Maternal and Child Health Programs www.amchp.org/programsandtopics/CYSHCN/Pages/default.aspx
National Academy for State Health Policy www.nashp.org/tag/children-with-special-health-care-needs/
National Maternal and Child Oral Health Resource Center www.mchoralhealth.org/highlights/children-with-special-health-care-needs.php
NATIONAL CONFERENCE OF STATE LEGISLATURES 8
Notes1 Child and Adolescent Health Measurement Initiative, “Who Are Children with Special Health Care Needs (CSHCN)” (Baltimore, Md.:
Johns Hopkins Bloomberg School of Public Health, Data Resource Center supported by Cooperative Agreement 1-U59-MC06980-01 from the U.S. Department of Health and Human Services, Health Resources and Services Administration [HRSA], Maternal and Child Health Bureau [MCHB], 2012), www.childhealthdata.org.
2 Cathy Hope and Joan Alker, “Medicaid and its Role for Children and Youth with Special Health Care Needs: A Family Perspective” (Washington, D.C.: Georgetown University Health Policy Institute, Center for Children and Families, July 2011).
3 Child and Adolescent Health Measurement Initiative, “National Survey of Children with Special Health Care Needs” (Baltimore, Md.: Johns Hopkins Bloomberg School of Public Health, Data Resource Center, n.d.), www.childhealthdata.org/learn/NS-CSHCN.
4 Naomi Friedrich, Susan Segar, and Hilary Sprangers, Impact Evaluation of the State Implementation Grants for Integrated Community Systems for Children with Special Health Needs: Classes of 2008, 2009, 2011 (Rockville, Md.: HRSA Maternal and Child Health Bureau, 2013), www.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=14231&lid=3.
5 U.S. Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau, The National Survey of Children with Special Health Care Needs Chartbook 2009–2010 (Rockville, Md.: U.S. Department of Health and Human Services, 2013), http://mchb.hrsa.gov/cshcn0910/more/introduction.html.
6 Naomi; Friedrichet al., Impact Evaluation of the State Implementation Grants for Integrated Community Systems for Children with Special Health Needs.
7 Ibid.8 Health Resources & Services Administration, Maternal and Child Health Bureau, “Programs and Initiatives” (Rockville, Md.: HRSA,
n.d.), https://mchb.hrsa.gov/maternal-child-health-initiatives/mchb-programs.9 Child and Adolescent Health Measurement Initiative, National Survey of Children with Special Health Care Needs.10 Medicaid.gov, “CMS Presumptive Eligibility” (Baltimore, Md.: Centers for Medicare & Medicaid Services, n.d.),
www.medicaid.gov/medicaid/outreach-and-enrollment/presumptive-eligibility/index.html. 11 Georgetown University Center for Children and Families, “Program Design Snapshot: 12-Month Continuous Eligibility,” (Washington,
D.C.: CCF, March 2009), https://ccf.georgetown.edu/2009/03/08/program-design-snapshot-12-month-continuous-eligibility/. 12 Medicaid.gov, “Continuous Eligibility for Medicaid and CHIP Coverage,” (Baltimore, Md.: Centers for Medicare & Medicaid Services,
n.d.), www.medicaid.gov/medicaid/outreach-and-enrollment/continuous-eligibility/index.html#footnote1. 13 https://www.medicaid.gov/medicaid/benefits/epsdt/index.html 14 Melissa Vickers, Betsy Anderson, Beth Dworetzyky, and Barbara Popper, Bright Futures Family Pocket Guide: Raising Healthy Infants,
Children, and Adolescents (Albuquerque, N.M.: Family Voices, 2012), 14-15.15 J.F. Hagan, J.S. Shaw, and P.M. Duncan, eds. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents
(Third Edition) (Elk Grove Village, Ill.: American Academy of Pediatrics, 2008), 205.16 U.S. Department of Health and Human Services, Administration for Children and Families, “Home Visiting Evidence of Effectiveness
(HomVEE)” (Washington, D.C.: U.S. Department of Health and Human Services, n.d.), http://homvee.acf.hhs.gov/. 17 National Conference of State Legislatures, Home Visiting (Denver, Colo.: NCSL, n.d.), www.ncsl.org/research/human-services/home-
visiting-improving-outcomes-for-children635399078.aspx 18 Minnesota Department of Health, “2008 Health Care Reform Summary” (St. Paul, Minnl: Minnesota Department of Health, June
2008), www.health.state.mn.us/divs/opa/08reformsummary.html. 19 U.S. Department of Health and Human Services, Paving the Road to Good Health: Strategies for Increasing Medicaid Adolescent
Well-Care Visits (Washington, D.C.: U.S. Department of Health and Human Services, February 2014), www.medicaid.gov/medicaid/benefits/downloads/paving-the-road-to-good-health.pdf.
20 National Academy for State Health Policy, “Behavioral Health in the Medicaid Benefit for Children and Adolescents in Illinois” (Washington, D.C.: NASHP, Oct. 21, 2013), www.nashp.org/illinois-479/.
21 J.F. Hagan, J.S. Shaw, and P.M. Duncan, eds. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents.22 American Association of Maternal and Child Health Programs, Developing Structure and Process Standards for Systems of Care
Serving Children and Youth with Special Health Care Needs, (Washington, D.C.: AMCHP, March 2014), www.amchp.org/AboutAMCHP/Newsletters/member-briefs/Documents/Standards%20White%20Paper%20FINAL.pdf.
23 Boston University, School of Public Health, Catalyst Center, Relief Funds: A Safety Net for Children and Youth with Special Health Care Needs (Boston, Mass.: Boston University School of Public Health, August 2007) http://cahpp.org/wp-content/uploads/2015/04/Relief-Funds2-2.pdf
24 Ibid. 25 Naomi; Friedrichet al., Impact Evaluation of the State Implementation Grants for Integrated Community Systems for Children with
Special Health Needs. 26 American Academy of Pediatrics, National Center for Medical Home Implementation, “Advancing the Medical Home Model for
Children and Youth: Rhode Island” (Elk Grove Village, Ill.: AAP, n.d.), https://medicalhomeinfo.aap.org/national-state-initiatives/Documents/Rhode%20Island.pdf.
William T. Pound, Executive Director
7700 East First Place, Denver, Colorado 80230, 303-364-7700 | 444 North Capitol Street, N.W., Suite 515, Washington, D.C. 20001, 202-624-5400
www.ncsl.org
© 2017 by the National Conference of State Legislatures. All rights reserved. ISBN 978-1-58024-907-2
This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number UC4MC28038, Alliance for Innovation on Maternal and Child Health, Expanding Access
to Care for Maternal and Child Health Populations. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
NCSL Contact:
Tahra Johnson, MPH303-856-1389

















