The content of In the Clinic is drawn from the clinical information and educationresources of the American College of Physicians (ACP), including ACP SmartMedicine and MKSAP (Medical Knowledge and Self-Assessment Program). Annalsof Internal Medicine editors develop In the Clinic from these primary sources incollaboration with the ACP’s Medical Education and Publishing divisions and withthe assistance of science writers and physician writers. Editorial consultants fromACP Smart Medicine and MKSAP provide expert review of the content. Readerswho are interested in these primary resources for more detail can consulthttp://smartmedicine.acponline.org, http://www.acponline.org/products_services/mksap/15/?pr31, and other resources referenced in each issue of In the Clinic.
CME Objective: To review current evidence for diagnosis, treatment, and practiceimprovement of asthma.
The information contained herein should never be used as a substitute for clinicaljudgment.
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
What symptoms or elements ofclinical history are helpful indiagnosing asthma?Symptoms that should prompt clini-cians to consider asthma are episodicwheezing, dyspnea, cough, difficultytaking a deep breath, and chesttightness (2, 3). A careful history toelicit the nature and timing of symp-toms is paramount in diagnosingasthma. Characteristically, asthmasymptoms are intermittent and mayremit spontaneously or with use ofshort-acting bronchodilators. Symp-toms often vary seasonally or are as-sociated with specific triggers, suchas cold, exercise, animal dander,pollen, occupational exposures, cer-tain foods, and aspirin or nons-teroidal anti-inflammatory drugs.Clinicians should also consider asth-ma in patients with chronic cough,especially if it is nocturnal, seasonal,or related to the workplace or a spe-cific activity.
What physical examinationfindings are suggestive?Because asthma is an episodic dis-ease, the physical examination isless helpful than a carefully elicitedhistory, unless a patient is havingan active exacerbation. The clini-cian should listen for wheezingduring tidal respirations or uponforced expiration, note the presenceof a prolonged expiratory phase ofbreathing, and examine the chestfor hyperexpansion. Studies suggestthat respiratory signs (wheezing,forced expiratory time, accessorymuscle use, respiratory rate, andpulsus paradoxus) may be useful to
predict airflow obstruction, but cli-nicians often disagree about theirpresence and absence (1, 3). Thephysical examination is sometimesmost helpful in looking for evi-dence of alternative diagnoses. Inspiratory crackles may suggestinterstitial lung disease or conges-tive heart failure. Abnormal heartsounds also might indicate heartfailure or additional cardiac causesof dyspnea, such as valvular disease.
What are the indications forspirometry in a patient whoseclinical presentation is consistentwith asthma?Several studies show a poor correla-tion among the presence, severity,and timing of wheezing and thedegree of airflow obstruction (4, 5).Patients vary in degree of sensitivi-ty to airflow limitations and can ac-climate to the disability and thusbecome insensitive to airflow ob-struction (6). Therefore, the Na-tional Heart, Lung, and Blood Institute (NHLBI) Expert PanelReport 3 recommends that all pa-tients (adults and children > 5 yearsof age) in whom asthma is consid-ered have objective assessments ofpulmonary function (3). Specifical-ly, initial pulmonary function test-ing should include spirometricmeasurement of the FEV1, FVC,and the FEV1/FVC ratio, beforeand after administration of a bron-chodilator to evaluate the re-versibility of airflow obstruction.Reversibility of airflow obstructiondefines asthma. Predicted normalvalues for spirometric measures are
1. To T, Stanojevic S,Moores G, GershonAS, Bateman ED, CruzAA, et al. Global asth-ma prevalence inadults: findings fromthe cross-sectionalworld health survey.BMC Public Health.2012;12:204.[PMID: 22429515]
2. Li JT, O’Connell EJ.Clinical evaluation ofasthma. Ann AllergyAsthma Immunol.1996;76:1-13; quiz 13-5. [PMID: 8564622]
3. National Asthma Edu-cation and Preven-tion Program. ExpertPanel Report 3 (EPR-3): Guidelines for theDiagnosis and Man-agement of Asthma-Summary Report2007. J Allergy ClinImmunol.2007;120:S94-138.[PMID: 17983880]
4. McFadden ER Jr, KiserR, DeGroot WJ. Acutebronchial asthma. Re-lations between clini-cal and physiologicmanifestations. NEngl J Med.1973;288:221-5.[PMID: 4682217]
5. Shim CS, Williams MHJr. Relationship ofwheezing to theseverity of obstruc-tion in asthma. ArchIntern Med.1983;143:890-2.[PMID: 6679232]
Asthma is a common respiratory illness characterized by airway hyper-responsiveness and inflammation. It affects over 300 million peopleglobally (1), including 22 million adults in the United States alone.
Although asthma mortality in the United States has declined, the morbidityand costs remain substantial. In certain groups of Americans, such as personsof lower socioeconomic status and minority ethnicity, asthma morbidity andmortality are disproportionately high. Such trends are surprising, given theimprovement in air quality in the United States and the availability of effec-tive therapies.
Diagnosis
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
population-based and differ withage, sex, and ethnicity (7). Post-bronchodilator improvement ≥12%and 200 mL of the FEV1 or FVCindicates significant reversibilityand therefore increases the likeli-hood of an asthma diagnosis (8).Spirometry should adhere to thestandards of the American Tho-racic Society (9). Of note, spirome-try is effort-dependent, and manypatients have difficulty with theFVC maneuver. In these patients(younger children, older adults, orpatients with severe respiratorydisease), alternative approaches,such as the FEV6, may be an ac-ceptable surrogate, with reductionin the FEV1/FEV6 ratio signifyingobstruction (10).
Does normal spirometry rule out adiagnosis of asthma? Whatadditional testing should patientswith normal spirometry have?Abnormal spirometry (reversibleobstruction) can confirm an asthmadiagnosis, but normal spirometrydoes not rule out asthma. Becausespirometry has limitations in sensi-tivity and specificity, it is probablybest used as part of a diagnosticstrategy in conjunction with a com-prehensive history, physical exami-nation, and other laboratory data.Clinicians should consider furtherstudies in patients with normalspirometry who have a clinical pic-ture otherwise suggestive of asthma(Table 1).
Bronchoprovocation with metha-choline or histamine can be helpfulin establishing a diagnosis in pa-tients who report that they onlyhave symptoms during exercise orat certain times of the year. Alter-natively, marked diurnal variabilitybased on measurements recorded ina peak flow diary kept for at least 2 weeks can help to establish asth-ma as the cause of symptoms.However, peak flow measurementsare highly effort-dependent andmay offer no opportunity for quali-ty assurance of their accuracy.
When should clinicians considerprovocative pulmonary testing?A gold standard for diagnosis ofasthma remains elusive. However,methacholine hyperresponsiveness inthe pulmonary function laboratoryhas high reproducibility and accept-ed standardization (11). The test re-quires sophisticated instrumentationand is labor-intensive and expensive.Although generally considered safe,it is generally not recommended inpatients with an FEV1 <65% of thepredicted value (3). A low PC20 (theconcentration of inhaled metha-choline needed to induce a 20% de-crease in the FEV1) on methacholinechallenge testing is diagnostic forairway hyperresponsiveness, a keyfeature of (though not limited to)asthma. Studies of methacholinechallenge suggest that it is sensitiveand has a high negative predictivevalue for the diagnosis of asthma(12-14). Although cold air has been
6. Chetta A, Gerra G,Foresi A, Zaimovic A,Del Donno M, Chit-tolini B, et al. Person-ality profiles andbreathlessness per-ception in outpa-tients with differentgradings of asthma.Am J Respir Crit CareMed. 1998;157:116-22. [PMID: 9445288]
7. Hankinson JL, Oden-crantz JR, Fedan KB.Spirometric referencevalues from a sampleof the general U.S.population. Am JRespir Crit Care Med.1999;159:179-87.[PMID: 9872837]
9. Miller MR, HankinsonJ, Brusasco V, BurgosF, Casaburi R, CoatesA, et al; ATS/ERS TaskForce. Standardisa-tion of spirometry.Eur Respir J.2005;26:319-38.[PMID: 16055882]
10. Swanney MP, JensenRL, Crichton DA,Beckert LE, CardnoLA, Crapo RO. FEV(6)is an acceptable sur-rogate for FVC in thespirometric diagno-sis of airway ob-struction and restric-tion. Am J Respir CritCare Med.2000;162:917-9.[PMID: 10988105]
11. Crapo RO, CasaburiR, Coates AL, EnrightPL, Hankinson JL,Irvin CG, et al. Guide-lines for metha-choline and exercisechallenge testing-1999. This officialstatement of theAmerican ThoracicSociety was adoptedby the ATS Board ofDirectors, July 1999.Am J Respir Crit CareMed. 2000;161:309-29. [PMID: 10619836]
12. Cockcroft DW, KillianDN, Mellon JJ, Harg-reave FE. Bronchialreactivity to inhaledhistamine: a methodand clinical survey.Clin Allergy.1977;7:235-43.[PMID: 908121]
13. Hopp RJ, Bewtra AK,Nair NM, TownleyRG. Specificity andsensitivity of metha-choline inhalationchallenge in normaland asthmatic chil-dren. J Allergy ClinImmunol.1984;74:154-8.[PMID: 6747136]
Table 1. Laboratory and Other Studies for AsthmaTest Comments
Pulmonary function tests Spirometry demonstrating reversible air-flow obstruction supports the diagnosis of asthma but normal spirometry does not exclude it; lung volume and flow-volume loops should be evaluated to rule out other diagnoses
Bronchoprovocation Positive results are diagnostic of airway hyperresponsiveness, which is a feature of, but may exist even in the absence of, asthma; negative results essentially rule out asthma
Chest radiograph Useful in ruling out other diagnoses; a finding of hyperinflation is consistent with asthma but is often a transient phenomenon found in the setting of an acute exacerbation
Allergy testing Skin or in vitro testing to determine sensitivity may be useful in patients with persistent disease to evaluate the role of allergens in asthma management; however, there is no clear diagnostic value
Complete blood count Mild eosinophilia is common in asthma; with differential however, routine use has limited clinical
utilitySputum evaluation Not indicated for routine initial evaluationIgE Mild elevation is common with asthma;
however, routine measurement is not recommended for initial evaluation
Biomarkers of inflammation Utility not yet established; clinical trials under way
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
14. Perpiñá M, Pellicer C,de Diego A, CompteL, Macián V. Diag-nostic value of thebronchial provoca-tion test withmethacholine inasthma. A Bayesiananalysis approach.Chest. 1993;104:149-54. [PMID: 8325060]
used in research to define mecha-nisms of bronchoconstriction,methacholine challenge remains theprovocative test of choice in patientswith normal pulmonary functiontests who have symptoms consistentwith asthma. Spirometry before,during, or after exercise may be theonly method to document bron-choconstriction in patients with exercise-induced asthma. As an al-ternative, monitoring peak flow iseasy and inexpensive, but the meas-urement is less precise and limited inreproducibility and sensitivity (15).
How should clinicians classifyasthma?Two reports, Expert Panel Report 3by the National Asthma Educationand Prevention Program, NHLBI,and National Institutes of Health,and Global Strategy for AsthmaManagement and Prevention by theGlobal Initiative for Asthma, havelaid out specifics for assessing andmanaging asthma in children and
adults. Both guidelines emphasizeasthma control, defined as a patienthaving few or no symptoms, no activity limitations, few or no in-stances of need for rescue medica-tion, normal lung function, and fewexacerbations.
Patient assessment is split into 2measures. Disease severity is definedas the intrinsic intensity of disease,which is assessed to initiate appropri-ate medication. Severity is most ef-fectively assessed in patients not yeton long-term medication but can beestimated based on the lowest level oftherapy needed to maintain control.Disease control is defined as the de-gree to which the manifestations ofasthma are minimized and the goalsof long-term control therapy are met.This measure is needed to maintainand adjust treatment as necessary.Responsiveness to treatment is gen-erally defined as the ease with whichasthma control is achieved by thera-py, although precise parameters for
Table 2. Classification of Asthma SeverityComponents of Severity Intermittent Persistent
Mild Moderate Severe
Impairment*
Symptoms ≤2 d/wk >2 d/wk but not daily Daily Throughout the dayNighttime awakenings ≤2 ×/mo 3–4 ×/mo >1 ×/wk but Often 7 ×/wk
not nightlySABA use for symptom control ≤2 d/wk >2 d/wk but not more Daily Several times a day
(not prevention of EIB) than 1 ×/dInterference with normal activity None Minor limitation Some limitation Extremely limitedLung function Normal FEV
1between FEV
1>80% of predicted; FEV
1>60% but FEV
1<60% of predicted;
exacerbations; FEV1
>80% FEV1/FVC normal <80% of predicted; FEV
1/FVC reduced >5%
of predicted; FEV1/FVC FEV
1/FVC reduced 5%
normalRiskExacerbations 0-1/y ≥2/y‡ ≥2/y‡ ≥2/y‡
Consider frequency and severity†
Recommended step for initiating Step 1 Step 2 Step 3§; consider short Step 4 or 5§; consider short treatment (see Figure for courses of systemic courses of systemic cortico-treatment steps)‡ corticosteroids steroids
Adapted from reference 3. EIB = exercise-induced bronchospasm; SABA = short-acting β2-agonist.
*Normal FEV1/FVC ratio: 8-19 years old, 85%; 20-39 years old, 80%; 40-59 years old, 75%; 60-80 years old, 70%.
†Frequency and severity may fluctuate over time for patients in any severity category. Relative annual risk for exacerbations may be related to FEV1.
‡Level of severity is determined by assessment of both impairment and risk. Assess impairment domain by patient's/caregiver's recall of previous 2–4 wk andspirometry. Assign severity to the most severe category in which any feature occurs.§In 2–6 weeks, evaluate the level of asthma control that is achieved and adjust therapy accordingly. Therapy should be initiated based on the severity of impairment at the time of initiation of therapy: step 1 for intermittent impairment, step 2 for mild persistent impairment, step 3 for moderate persistent impairment, and step 4 or 5 for severe persistent impairment.
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
responsiveness measurement havenot been determined.
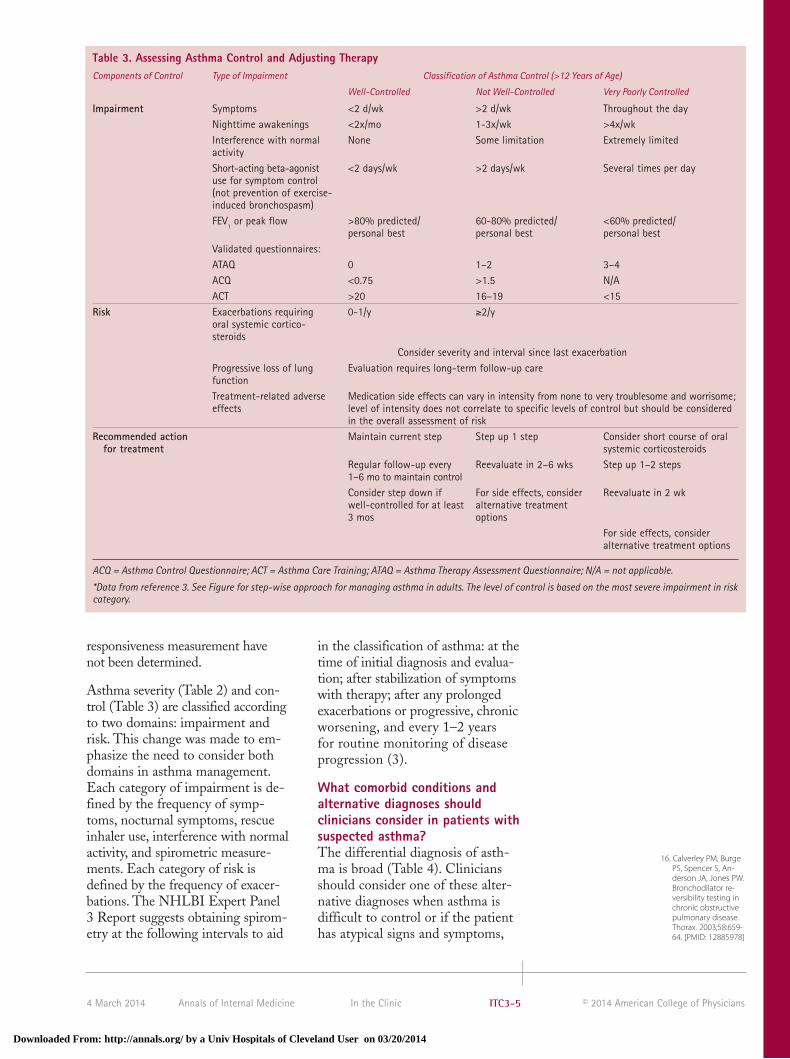
Asthma severity (Table 2) and con-trol (Table 3) are classified accordingto two domains: impairment andrisk. This change was made to em-phasize the need to consider bothdomains in asthma management.Each category of impairment is de-fined by the frequency of symp-toms, nocturnal symptoms, rescueinhaler use, interference with normalactivity, and spirometric measure-ments. Each category of risk is defined by the frequency of exacer-bations. The NHLBI Expert Panel3 Report suggests obtaining spirom-etry at the following intervals to aid
in the classification of asthma: at thetime of initial diagnosis and evalua-tion; after stabilization of symptomswith therapy; after any prolongedexacerbations or progressive, chronicworsening, and every 1–2 years for routine monitoring of diseaseprogression (3).
What comorbid conditions andalternative diagnoses shouldclinicians consider in patients withsuspected asthma?The differential diagnosis of asth-ma is broad (Table 4). Cliniciansshould consider one of these alter-native diagnoses when asthma isdifficult to control or if the patienthas atypical signs and symptoms,
Table 3. Assessing Asthma Control and Adjusting TherapyComponents of Control Type of Impairment Classification of Asthma Control (>12 Years of Age)
Well-Controlled Not Well-Controlled Very Poorly Controlled
Impairment Symptoms <2 d/wk >2 d/wk Throughout the dayNighttime awakenings <2x/mo 1-3x/wk >4x/wkInterference with normal None Some limitation Extremely limitedactivityShort-acting beta-agonist <2 days/wk >2 days/wk Several times per dayuse for symptom control (not prevention of exercise-induced bronchospasm)FEV
Consider severity and interval since last exacerbationProgressive loss of lung Evaluation requires long-term follow-up carefunctionTreatment-related adverse Medication side effects can vary in intensity from none to very troublesome and worrisome;effects level of intensity does not correlate to specific levels of control but should be considered
in the overall assessment of riskRecommended action Maintain current step Step up 1 step Consider short course of oral
for treatment systemic corticosteroidsRegular follow-up every Reevaluate in 2–6 wks Step up 1–2 steps1–6 mo to maintain controlConsider step down if For side effects, consider Reevaluate in 2 wkwell-controlled for at least alternative treatment 3 mos options
For side effects, consider alternative treatment options
ACQ = Asthma Control Questionnaire; ACT = Asthma Care Training; ATAQ = Asthma Therapy Assessment Questionnaire; N/A = not applicable.
*Data from reference 3. See Figure for step-wise approach for managing asthma in adults. The level of control is based on the most severe impairment in riskcategory.
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
particularly if spirometry is incon-sistent with or nondiagnostic ofasthma. Further testing, such ascomplete pulmonary function test-ing that includes lung volumes anddiffusing capacity, may be revealing.For example, evidence of a lack ofreversibility of airflow obstructionsuggests chronic obstructive pul-monary disease (COPD), or re-strictive patterns with diminutionsin the FEV1 and FVC but a normalFEV1/FVC ratio suggests interstitiallung disease. These conditions canalso coexist in a patient who hasasthma and referral to a specialistmay be indicated is these situations(see next section). An important dif-ference between asthma and COPDis the history of smoking. Although30% of patients with asthma in theUnited States smoke, COPD oftenoccurs in older persons with a sub-stantial history of cigarette smokingand is manifest by chronic bronchi-tis and emphysema. Patients withCOPD may demonstrate reversibil-ity with bronchodilators on pul-monary function testing, but it isless common, can vary between andwithin patients, can change overtime, and can differ according tothe bronchodilator used (16). In-spection of the flow-volume loop
may reveal evidence of a fixed orvariable airway obstruction or, to-gether with direct visualization ofthe larynx during acute symptoms,may be useful in indentifying vocalcord paralysis. A plain chest radi-ograph or computed tomography ishelpful in identifying bronchiectasisor lung masses. Echocardiographycan help to identify cardiovasculardisorders, including ischemic heartdisease, ventricular dysfunction, andpulmonary hypertension. Chroniccough, dyspnea, or recurrent wheez-ing, although each consistent withasthma, may be due to other disor-ders including COPD, vocal corddysfunction, cystic fibrosis, obstruc-tive sleep apnea, the Churg-Strausssyndrome, allergic bronchopul-monary aspergillosis, interstitiallung disease, bronchiectasis, conges-tive heart failure, and pulmonaryhypertension, or may be side effectsof medications. Evidence showsthat difficult-to-control asthma maybe a result of comorbid conditionsand that standardized evaluation ofpatients for comorbidity was associ-ated with improved asthma control(17).
When should primary careclinicians consider referringpatients with suspected asthma tospecialists for diagnosis?Consultation with a pulmonologistshould be considered before orderingprovocative pulmonary function test-ing because testing is time- and la-bor-intensive and requires skilledperformance and interpretation. Patients presenting with atypicalsymptoms, who have abnormal chestradiographs, pulmonary functiontests suggesting both obstruction andrestriction, unusual manifestations ofthe disease, or who display subopti-mal response to therapy may benefitfrom referral to a pulmonologist. Re-ferral to an allergist may be helpfulfor patients with asthma that seemsto have an allergic component, suchas seasonal variation in asthma sever-ity or sensitivity to specific environ-mental exposures.
Table 4. Differential Diagnosis of AsthmaCondition Characteristics
COPD Airway destruction less reversible; typically seen in older patients with a history of smoking
Vocal cord dysfunction Abrupt onset and end of symptoms; monophonic wheeze; more common in younger patients; confirm with laryngoscopy and/or flow-volume loop
Heart failure Dyspnea and often wheezing; crackles on auscultation; limited response to asthma therapy; cardiomegaly; edema; elevated BNP; other features of heart failure
Bronchiectasis Cough productive of large amounts of purulent sputum; rhonchi and crackles are common; may have wheezing and clubbing; confirmed by CT imaging
Allergic bronchopulmonary Recurrent infiltrates on chest radiograph; eosinophilia; high aspergillosis IgE levels; frequent need for corticosteroid treatment
Cystic fibrosis Cough productive of large amounts of purulent sputum; rhonchi and crackles are common; prominent clubbing; may have wheezing
Mechanical obstruction More localized wheezing; if central in location, flow-volume loop may provide a clue
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
20. Ho G, Tang H, Rob-bins JA, Tong EK.Biomarkers of tobac-co smoke exposureand asthma severityin adults. Am J PrevMed. 2013;45:703-9.[PMID: 24237911]
21. Ostro BD, Lipsett MJ,Mann JK, Wiener MB,Selner J. Indoor airpollution and asth-ma. Results from apanel study. Am JRespir Crit Care Med.1994;149:1400-6.[PMID: 8004290]
22. Institute of MedicineCommittee on theAssessment of Asth-ma and Indoor Air.Executive summary.In: Clearing the Air:Asthma and IndoorAir Exposures. Wash-ington, DC: NationalAcademies Pr; 2000.
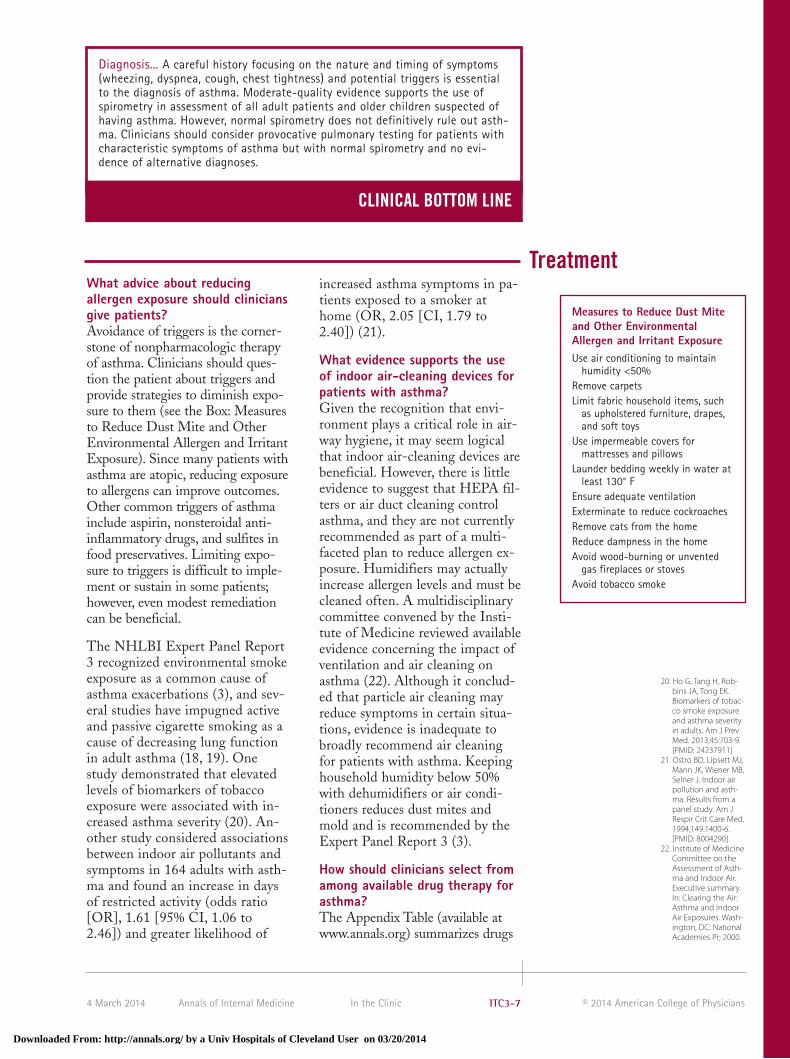
increased asthma symptoms in pa-tients exposed to a smoker athome (OR, 2.05 [CI, 1.79 to2.40]) (21).
What evidence supports the useof indoor air-cleaning devices forpatients with asthma?Given the recognition that envi-ronment plays a critical role in air-way hygiene, it may seem logicalthat indoor air-cleaning devices arebeneficial. However, there is littleevidence to suggest that HEPA fil-ters or air duct cleaning controlasthma, and they are not currentlyrecommended as part of a multi-faceted plan to reduce allergen ex-posure. Humidifiers may actuallyincrease allergen levels and must becleaned often. A multidisciplinarycommittee convened by the Insti-tute of Medicine reviewed availableevidence concerning the impact ofventilation and air cleaning onasthma (22). Although it conclud-ed that particle air cleaning mayreduce symptoms in certain situa-tions, evidence is inadequate tobroadly recommend air cleaningfor patients with asthma. Keepinghousehold humidity below 50%with dehumidifiers or air condi-tioners reduces dust mites andmold and is recommended by theExpert Panel Report 3 (3).
How should clinicians select fromamong available drug therapy forasthma?The Appendix Table (available atwww.annals.org) summarizes drugs
What advice about reducingallergen exposure should cliniciansgive patients?Avoidance of triggers is the corner-stone of nonpharmacologic therapyof asthma. Clinicians should ques-tion the patient about triggers andprovide strategies to diminish expo-sure to them (see the Box: Measuresto Reduce Dust Mite and OtherEnvironmental Allergen and IrritantExposure). Since many patients withasthma are atopic, reducing exposureto allergens can improve outcomes.Other common triggers of asthmainclude aspirin, nonsteroidal anti-inflammatory drugs, and sulfites infood preservatives. Limiting expo-sure to triggers is difficult to imple-ment or sustain in some patients;however, even modest remediationcan be beneficial.
The NHLBI Expert Panel Report3 recognized environmental smokeexposure as a common cause ofasthma exacerbations (3), and sev-eral studies have impugned activeand passive cigarette smoking as acause of decreasing lung functionin adult asthma (18, 19). Onestudy demonstrated that elevatedlevels of biomarkers of tobacco exposure were associated with in-creased asthma severity (20). An-other study considered associationsbetween indoor air pollutants andsymptoms in 164 adults with asth-ma and found an increase in daysof restricted activity (odds ratio[OR], 1.61 [95% CI, 1.06 to2.46]) and greater likelihood of
Diagnosis... A careful history focusing on the nature and timing of symptoms(wheezing, dyspnea, cough, chest tightness) and potential triggers is essentialto the diagnosis of asthma. Moderate-quality evidence supports the use ofspirometry in assessment of all adult patients and older children suspected ofhaving asthma. However, normal spirometry does not definitively rule out asth-ma. Clinicians should consider provocative pulmonary testing for patients withcharacteristic symptoms of asthma but with normal spirometry and no evi-dence of alternative diagnoses.
CLINICAL BOTTOM LINE
Treatment
Measures to Reduce Dust Miteand Other EnvironmentalAllergen and Irritant ExposureUse air conditioning to maintain
humidity <50%Remove carpetsLimit fabric household items, such
as upholstered furniture, drapes,and soft toys
Use impermeable covers formattresses and pillows
Launder bedding weekly in water atleast 130° F
Ensure adequate ventilationExterminate to reduce cockroachesRemove cats from the homeReduce dampness in the homeAvoid wood-burning or unvented
gas fireplaces or stovesAvoid tobacco smoke
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
available to treat asthma. The goalsof asthma therapy are to achieveasthma control by the followingmeans: reduce impairment throughreduction of chronic and trouble-some symptoms; minimize rescuebronchodilator use; maintain nor-mal (or near normal) spirometry;minimize interference with activi-ties; and meet patient’s satisfactionwith care and to reduce risk by thefollowing means: prevent exacerba-tions; prevent loss of lung func-tion; and provide optimal pharma-cotherapy with minimal adverseeffects.
The Figure presents a stepwise ap-proach to pharmacotherapy. Step-wise therapy consists of agents foracute relief of symptoms (rescuetherapy) and for long-term control.
Rescue therapy is critical for all patients regardless of asthma sever-ity. Even patients with intermittentasthma can have severe exacerba-tions. Patients with persistentsymptoms require a long-term con-troller in addition to rescue therapy.Therapy should be initiated basedon the severity of impairment atthe time of initiation of therapy:step 1 for intermittent impairment,step 2 for mild persistent impair-ment, step 3 for moderate persist-ent impairment, and step 4 or 5 forsevere persistent impairment. Im-pairment status is determined bythe most impaired variable (e.g.,worst of symptoms, nighttimeawakenings).
After initiation of therapy, the regi-men should be adjusted based on
Quick relief medication for all patients:• SABA as needed for symptoms. Intensity of treatment depends on severity of symptoms: up to 3 treatments at 20-minute intervals
as needed. Short course of oral systemic corticosteroids may be needed.• Use of SABA >2 days a week for symptom relief (not prevention of EIB) generally indicates inadequate control and the need to step
up treatment.
Each step: Patient education, environmental control, and management of comorbiditiesSteps 2-4: Consider subcutaneous allergen immunotherapy for patients who have allergic asthma
Step 1
Preferred:SABA PRN
Intermittentasthma
Persistent asthma: Daily medicationConsult with asthma specialist if step 4 care or higher is required
Preferred:High-dose ICS+ LABA + oralcorticosteroid
AND
Consideromalizumab for
patients whohave allergies
Step up ifneeded
(first checkadherence,
environmentalcontrol, and
comorbidconditions)
Step down ifpossible
(and asthma iswell controlled
at least3 months)
Assesscontrol
Figure. Stepwise approach for managing asthma in adults. EIB = exercise-induced bronchospasm; ICS = inhaled corticosteroids; LABA = long-acting β-agonists; LTRA = leukotriene-receptor agonists; SABA = short-acting β-agonists.
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
23. Salpeter SR, BuckleyNS, Ormiston TM,Salpeter EE. Meta-analysis: effect oflong-acting beta-ag-onists on severeasthma exacerba-tions and asthma-re-lated deaths. Ann In-tern Med.2006;144:904-12.[PMID: 16754916]
24. Greening AP, Ind PW,Northfield M, ShawG. Added salmeterolversus higher-dosecorticosteroid inasthma patientswith symptoms onexisting inhaled cor-ticosteroid. Allen &Hanburys LimitedUK Study Group.Lancet.1994;344:219-24.[PMID: 7913155]
25. Ukena D, Harnest U,Sakalauskas R, Mag-yar P, Vetter N, Stef-fen H, et al. Compari-son of addition oftheophylline to in-haled steroid withdoubling of thedose of inhaledsteroid in asthma.Eur Respir J.1997;10:2754-60.[PMID: 9493656]
26. Woolcock A, Lund-back B, Ringdal N,Jacques LA. Compar-ison of addition ofsalmeterol to in-haled steroids withdoubling of thedose of inhaledsteroids. Am J RespirCrit Care Med.1996;153:1481-8.[PMID: 8630590]
the level of asthma control (Table 3and Figure). If asthma is not well-controlled, stepping up to more in-tense therapy is indicated. A step upin treatment may involve any or all ofthe following: an increase in the in-haled corticosteroid (ICS) dose, ad-dition of a second controller, and abrief course of oral steroids to achievecontrol more rapidly. If symptoms arewell-controlled on a given regimenfor 3 months or more, stepping downto less intensive therapy is indicated.A step down in treatment may in-volve stopping the second controller(such as a long-acting β
2-agonist
[LABA] bronchodilator) or reducingthe dose of ICS. A decrease in ICSdose by 25%–50% over time is an ap-propriate initial target. It is importantthat the patient have instructions tocall immediately if symptoms start toincrease.
Clinicians should review therapy2–6 weeks after initiation of or step-ping up/down therapy and thenevery 1–6 months. The frequency offollow-up should depend on level ofcontrol. Asthma is a chronic diseasethat often requires long-term thera-py. Given the complexity of airwayinflammation, multiple drugs withdifferent actions against the variousaspects of the inflammatory responseare often necessary.
Rescue TherapyPatients with intermittent asthmamay only need a quick-relief med-ication (short-acting β-agonists[SABAs]) on an as-needed basis.SABAs are the drugs of choice forreversal of acute bronchospasm andare safe and well-tolerated. Patientswith persistent asthma (mild, mod-erate, or severe) maintained on long-term controller therapy should alsoreceive a SABA and advice to keepthe medication readily available forrelief of acute symptoms.
Patients with mild persistent asth-ma should receive a long-termcontroller medication, usually alow-dose ICS. Compared with pa-tients with intermittent asthma,patients with mild persistent asth-ma are more prone to underlyinginflammation and disease exacer-bations. Low-dose ICSs have beenshown to reduce risk for exacerba-tions, bronchial hyperresponsive-ness, and need for rescue β-agonistuse and to control symptoms. Al-ternatives to ICSs are leukotriene-receptor antagonist medications(e.g., montelukast, zafirlukast) orcromolyn. Of note, LABA mono-therapy is not recommended forlong-term control of asthma be-cause studies suggest a risk for in-creased morbidity and mortality insome patients (23).
The therapy of choice in patientswith moderate persistent asthma iseither low-dose ICSs and a LABAor a moderate dose of a single long-term controller medication (exclud-ing LABAs as outlined above). Evi-dence suggests that patients whoremain symptomatic while takingmoderate doses of ICSs benefitfrom the addition of a long-actingbronchodilator, such as salmeterol orformoterol. The additive effect ofthe long-acting bronchodilator im-proves lung physiology, decreasesuse of rescue β-agonists, and reducessymptoms better than doubling thedose of an ICS alone (24-26). How-ever, there is little evidence to guidethe best choice of combinations.Clinicians and patients must weighthe reduced risk for adverse effectsof steroids against the use of morecomplicated regimens. It is unclearwhether controlling the disease withhigh-dose ICSs or moderate-doseICSs plus a long-acting broncho-dilator results in a better long-termoutcome.
In a 12-week, randomized, controlled trial of447 patients who remained symptomaticon treatment with ICSs, a dry-powder in-haler containing salmeterol and fluticas-one was more effective in improving
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
27. Nelson HS, BusseWW, Kerwin E,Church N, EmmettA, Rickard K, et al.Fluticasone propi-onate/salmeterolcombination pro-vides more effectiveasthma control thanlow-dose inhaledcorticosteroid plusmontelukast. J Aller-gy Clin Immunol.2000;106:1088-95.[PMID: 11112891]
28. Löfdahl CG, Reiss TF,Leff JA, Israel E, Noo-nan MJ, Finn AF, etal. Randomised,placebo controlledtrial of effect of aleukotriene receptorantagonist, mon-telukast, on taperinginhaled corticos-teroids in asthmaticpatients. BMJ.1999;319:87-90.[PMID: 10398629]
29. Laviolette M, Malm-strom K, Lu S,Chervinsky P, PujetJC, Peszek I, et al.Montelukast addedto inhaled be-clomethasone intreatment of asthma.Montelukast/Be-clomethasone Addi-tivity Group. Am JRespir Crit Care Med.1999;160:1862-8.[PMID: 10588598]
31. Kerstjens HA, EngelM, Dahl R, PaggiaroP, Beck E, Vandewalk-er M, et al. Tiotropi-um in asthma poorlycontrolled with stan-dard combinationtherapy. N Engl JMed. 2012;367:1198-207.[PMID: 22938706]
32. Humbert M, BeasleyR, Ayres J, Slavin R,Hébert J, Bousquet J,et al. Benefits ofomalizumab as add-on therapy in pa-tients with severepersistent asthmawho are inadequate-ly controlled despitebest available thera-py (GINA 2002 step4 treatment): INNO-VATE. Allergy.2005;60:309-16.[PMID: 15679715]
physiologic endpoints, reducing rescuetherapy use, and reducing exacerbationsthan was the addition of montelukast tothe ICS fluticasone (27).
LABAs may help improve asthmasymptoms, but as mentioned above,they may also increase risks for ad-verse outcomes. Therefore, patientsstarted on these medications shouldbe followed closely. A meta-analysisof 19 randomized clinical trials foundthat, compared with placebo, LABAsincreased severe exacerbations requir-ing hospitalization (OR, 2.6 [CI, 1.6to 4.3]), life-threatening exacerba-tions (OR, 1.8 [CI, 1.1 to 2.9]), andasthma-related deaths (OR, 3.5 [CI,1.3 to 9.3]; risk difference, 0.07%)(23). Risks were similar for salme-terol and formoterol and in childrenand adults. Several trials did not re-port information about potentialharms, and the number of reporteddeaths was small. Black patients andpatients not using ICSs seemed to beat highest risk for these outcomes.Guidelines suggest that adding aLABA to low-dose ICS and increas-ing the dose of ICS (step 3, see Fig-ure) are equally preferred options.This balances the established benefi-cial effects of combination therapy inolder children and adults and the po-tential increased risk for severe exac-erbations reported with daily use ofLABA.
Patients with severe persistent asth-ma may require three controllermedications to adequately controlsymptoms. Patients with this level ofdisease are extremely prone to exacer-bations and have profound underlyinginflammation. Direct comparisons ofhigh-dose ICSs to leukotriene recep-tor modifiers (such as montelukast)revealed that the ICSs were more ef-fective. The addition of montelukastto the regimen of a patient requiringhigh-dose ICSs, however, allowed asignificant reduction in the dose ofthe ICS while maintaining asthmacontrol (28).
In a randomized clinical trial of patientswith inadequate symptom control despite
low- to moderate-dose ICS, the addition ofmontelukast improved FEV
1, daytime symp-
toms, and nocturnal awakenings (29). Asystematic review of trials comparing the addition of daily leukotriene-receptor an-tagonists or LABAs to ICSs in patients withsevere asthma concluded that LABAs werebetter than leukotriene antagonists in pre-venting the need for rescue therapy and sys-temic steroids and improved lung functionand symptoms (30).
Until recently, anticholinergic agentswere not a part of the chronic med-ication regimen for asthma. Howev-er, recent studies have suggested thatthere may be a role for long-actinganticholinergic agents in chronicasthma therapy.
In one randomized trial of symptomaticpatients with an FEV
1<80% predicted and
a history of at least one exacerbation in theprior year, addition of tiotropium to a regi-men of inhaled glucocorticoid and LABAwas associated with a longer time untilanother exacerbation and a modest im-provement in FEV
1compared with placebo
(31). As such, tiotropium can be consideredin patients who remain poorly controlleddespite two agents.
Omalizumab is a monoclonal anti-body that binds to IgE and has beenshown to reduce exacerbations in pa-tients with severe persistent asthmadespite therapy with high-dose ICSsand LABA therapy and often addi-tional pharmacologic therapies (32).However, severe anaphylaxis hasbeen reported up to 24 hours afterinjection. Clinicians should view thedrug as an option only in carefullyselected cases of severe persistentasthma in patients with proven IgE-mediated sensitivity to perennialaeroallergens and failure of othertherapeutic options. Additional bio-logical therapies, such as a mono-clonal antibody to the interleukin-4receptor, are under investigation forthe treatment of asthma (33).
What is the role of nonpharma-cologic therapy?Many patients are interested innonpharmacologic therapy forasthma, such as acupuncture, and
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
complementary or herbal therapies.The Expert Panel Report 3 advisesthat there is inadequate evidence toeither support or refute the role ofsuch therapies in chronic asthmamanagement in general, with theexception that the panel specificallyrecommends against acupuncture.Physicians are also advised to coun-sel patients on the possible risks ofcomplementary therapy, such asherbal medications, as regulationand formulations of these may notbe standardized.
What therapeutic options areeffective for patients withexercise-induced bronchospasm?In some patients, exercise inducesbronchospasm. Symptoms oftenoccur with vigorous exercise incold, dry air. The Expert PanelReport 3 recommends that pa-tients should not have to limit desired activity because of exer-cise-induced bronchospasm. Pa-tients who have normal baselinepulmonary function but experienceexercise-induced symptoms, suchas cough, shortness of breath, orwheezing, can be treated effective-ly with albuterol, cromolyn sodi-um, or nedocromil 15–30 minutesbefore exercise. If exercise-inducedsymptoms persist, addition oflong-acting bronchodilators orleukotriene antagonists may behelpful. Recent evidence, however,suggesting that monotherapy withlong-acting bronchodilators maycause adverse outcomes in asthmacautions against using these agentsas monotherapy in exercise-inducedasthma (23, 34). Despite theseconcerns, evidence suggests thatformoterol or salmeterol is moreeffective than placebo in prevent-ing exercise-induced bronchocon-striction (35, 36). In a study of patients with mild stable asthma,once-daily treatment with mon-telukast protected against exercise-induced bronchospasm (37). Theclinician should consider exercise-induced bronchospasm in the con-text of the patient’s overall therapy.
Many patients who present withputative exercise-induced bron-chospasm may have abnormal pul-monary function test results atbaseline. Such patients should betreated according to the regimen described by the Expert Panel Report 3 (3).
When should primary careclinicians refer patients withasthma to a specialist fortreatment?Although definitive evidenceabout the effect of specialty careon asthma outcomes is not avail-able, according to consensus recommendations referral to aspecialist may be useful in specificclinical situations (see the Box:Clinical Scenarios That ShouldPrompt Specialist Referral).Whether to consult an allergist orpulmonologist should reflect localavailability and consideration ofthe predominant comorbid condi-tions and complicating features inasthma. For example, a patientwith sleep apnea and asthma maybenefit from a pulmonary consul-tation, whereas a patient who hasasthma with an atopic componentmay benefit from referral to an allergist.
When should oral corticosteroidsbe used for outpatient treatment?Selected patients who have anacute increase in asthma symptomsmay be managed as outpatients,with appropriate escalation oftherapy and instructions to seekurgent care rapidly if symptomspersist or worsen. Oral corticos-teroids should be given to patientswho have symptoms that are in-completely controlled after 2 doseswithin 20 minutes of 2 to 6 puffsof SABAs (i.e., wheezing or dysp-nea persists). Patients who arestarted on oral corticosteroids asan outpatient should continue frequent short-acting β-agonists(every 4 hours) and follow-upwithin 1 day with a physician toensure improved control. They
Clinical Scenarios That ShouldPrompt Specialist ReferralHistory of life-threatening
exacerbationsAtypical signs and symptomsSevere persistent asthmaNeed for continuous oral
corticosteroids or high-dose inhaledsteroids or more than 2 courses oforal steroids in a 1-year period
Comorbid conditions that complicateasthma diagnosis or treatment
Need for provocative testing orimmunotherapy
Problems with adherence or allergenavoidance
Unusual occupational or otherexposures
33. Wenzel S, Ford L,Pearlman D, SpectorS, Sher L, Skobieran-da F, et al. Dupilum-ab in persistent asth-ma with elevatedeosinophil levels. NEngl J Med.2013;368:2455-66.[PMID: 23688323]
34. Nelson HS, Weiss ST,Bleecker ER, YanceySW, Dorinsky PM;SMART Study Group.The Salmeterol Mul-ticenter Asthma Re-search Trial: a com-parison of usualpharmacotherapyfor asthma or usualpharmacotherapyplus salmeterol.Chest. 2006;129:15-26. [PMID: 16424409]
35. Nelson JA, Strauss L,Skowronski M, CiufoR, Novak R, McFad-den ER Jr. Effect oflong-term salme-terol treatment onexercise-inducedasthma. N Engl JMed. 1998;339:141-6. [PMID: 9664089]
36. Nightingale JA,Rogers DF, Barnes PJ.Comparison of theeffects of salmeteroland formoterol inpatients with severeasthma. Chest.2002;121:1401-6.[PMID: 12006420]
37. Leff JA, Busse WW,Pearlman D, BronskyEA, Kemp J, Hende-les L, et al. Mon-telukast, aleukotriene-receptorantagonist, for thetreatment of mildasthma and exer-cise-induced bron-choconstriction. NEngl J Med.1998;339:147-52.[PMID: 9664090]
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
38. Emerman CL,Woodruff PG, Cydul-ka RK, Gibbs MA,Pollack CV Jr, Camar-go CA Jr. Prospectivemulticenter study ofrelapse followingtreatment for acuteasthma amongadults presenting tothe emergency de-partment. MARC in-vestigators. Multi-center AsthmaResearch Collabora-tion. Chest.1999;115:919-27.[PMID: 10208187]
39. McCarren M, McDer-mott MF, Zalenski RJ,Jovanovic B, MarderD, Murphy DG, et al.Prediction of relapsewithin eight weeksafter an acute asth-ma exacerbation inadults. J Clin Epi-demiol. 1998;51:107-18. [PMID: 9474071]
40. Rowe BH, Bota GW,Fabris L, Therrien SA,Milner RA, Jacono J.Inhaled budesonidein addition to oralcorticosteroids toprevent asthma re-lapse following dis-charge from theemergency depart-ment: a randomizedcontrolled trial. JAMA.1999;281:2119-26.[PMID: 10367823]
should also be instructed to imme-diately seek medical attention ifsymptoms persist or worsen or ifSABAs are required more fre-quently than every 4 hours.
How should the patient beeducated to respond whensymptoms increase?The Expert Panel Report 3 empha-sizes the importance of patient ed-ucation and involvement in self-management of asthma, includingacute exacerbations (3). Patientsshould know the early signs andsymptoms of deterioration and theappropriate action to take in re-sponse, as early intervention mayprevent emergency department vis-its and hospitalization. Physiciansand patients should agree on awritten action plan, which shouldinclude daily management, how torecognize signs and symptoms ofworsening, and how to adjust medications in response to acutesymptoms or changes in the peakexpiratory flow rate (PEFR). Theplan should specifically addresshow patients should adjust medica-tions and doses and when theyshould seek medical attention. Pa-tients with moderate or severe dis-ease should have medications (suchas oral corticosteroids) and equip-ment (such as a nebulizer machine)available at home for immediatetreatment of exacerbations.
When is hospitalization indicated?Patients who have a sustained re-sponse to treatment in outpatient settings generally do not need to behospitalized if they understand theimportance of continued anti-inflammatory therapy and close fol-low-up. The decision to hospitalize apatient with asthma should accountfor patient characteristics (includingfactors listed in the Box: Factors As-sociated With Poor Outcomes ofAsthma Exacerbations), severity ofdisease, and initial response to short-term therapy. Additional variables toconsider include the availability of as-sistance to the patient in case of need
and the reliability of close follow-upcare. Patients with a moderate or se-vere exacerbation and an incompleteresponse to therapy may need hospi-talization. A moderate exacerbationis defined as one where the FEV1 is40%–69% predicted or the PEFR is40%–69% of personal best, or thesymptoms and physical examinationfindings are moderate (such as per-sistent wheezing but ability to speakin full sentences). An exacerbation issevere if the FEV1 or PEFR ratio<40%; when symptoms are severe; orwhen physical examination findingsinclude signs of severe respiratorydistress, such as muscle retractions,use of accessory muscles, inability tospeak in full sentences, or confusionor lethargy. When posttreatmentPEFR remains <40% of the predict-ed value, intensive care unit admis-sion may be warranted. However,data are insufficient to support theidea that adequate oxygen saturationand PEFR at the time of emergencydepartment discharge predict a goodoutcome.
In a prospective cohort study of adults pre-senting with asthma to urban emergencydepartments in the United States, the PEFRof those who had a relapse did not signifi-cantly differ from those who did not have arelapse after discharge from the emergencydepartment. However, such historical fea-tures as emergency department or urgentcare visits (OR, 1.3 per 5 visits), use of ahome nebulizer (OR, 2.2), multiple triggers(OR, 1.1 per trigger), and longer duration ofsymptoms (OR, 2.5 for 1 to 7 days) did pre-dict relapse (38).
What factors identify patientswith asthma at high risk for fatalor near-fatal events during anexacerbation?Historical factors reflect the risk forfatal and near-fatal asthma-relatedevents and should lower the thresh-old for hospitalization of a personwhen these factors are present. Suchfactors include asthma history, so-cioeconomic characteristics, and comorbid conditions (see the Box:Factors Associated With Poor Out-comes of Asthma Exacerbations).
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
41. Effectiveness of rou-tine self monitoringof peak flow in pa-tients with asthma.Grampian AsthmaStudy of IntegratedCare (GRASSIC). BMJ.1994;308:564-7.[PMID: 8148679]
42. Charlton I, CharltonG, Broomfield J,Mullee MA. Evalua-tion of peak flowand symptoms onlyself managementplans for control ofasthma in generalpractice. BMJ.1990;301:1355-9.[PMID: 2148702]
How often should clinicians seepatients with asthma for routinefollow-up?No definitive studies are available toguide the frequency of asthma fol-low-up, but consensus suggests thatfor patients with newly diagnosedasthma, 2–4 visits during the 6months after diagnosis can help toestablish and reinforce the patient’sbasic knowledge and managementskills. For patients with asthma whohave shown maximum improvementin pulmonary function and have
minimal to no related symptoms, theExpert Panel Report 3 suggests rou-tine follow-up every 1–6 months (3);however, evidence documenting thebenefit of this strategy is limited.The Report also suggests follow-upwithin 7 days for patients dischargedfrom the hospital and within 10 daysfor patients treated as outpatients foran exacerbation. Studies have shownthat relapse occurs in about 1% ofpatients per day until the follow-upvisit (39, 40).
Do U.S. stakeholders considerasthma care when evaluating thequality of care a physiciandelivers?In April 2005, the AmbulatoryCare Quality Alliance released aset of 26 health care quality indi-cators for clinicians, consumers,and health care purchasers to usein quality improvement efforts,public reporting, and pay-for-performance programs (www.ahrq.gov/qual/aqastart.htm), two ofwhich focus on asthma care. TheNational Quality Forum has defined and/or endorsed physician-specific similar measures of quality ofasthma care (see the Box: PhysicianQuality Measures for Asthma CareEndorsed by the National QualityForum). As part of the AffordableCare Act, beginning in 2015,
Treatment... Patients should try to understand and avoid asthma triggers. Whileair conditioners or dehumidifiers may be helpful, indoor air-cleaning devices areof unclear utility. All patients with asthma should have SABAs available for reliefof acute symptoms. For patients with persistent asthma, treatment with long-term controller medications can be stepped up or down as needed to maintaindisease control. The key to a successful step-up/step-down treatment plan is toclosely monitor symptoms. Serial measures of asthma control should guide treat-ment changes to minimize the potential risk for asthma exacerbations and long-term side effects. An acute increase in symptoms requires prompt recognition andincrease in treatment, and all patients should be instructed on how to recognizethe early signs of clinical deterioration and how to respond. Careful evaluationand monitoring are required to identify when patients with an acute increase insymptoms require hospitalization.
CLINICAL BOTTOM LINE
PracticeImprovement
Factors Associated With PoorOutcomes of AsthmaExacerbationsPrior intubationMultiple asthma-related
exacerbationsEmergency room visits for asthma
in the previous yearNonuse or low adherence to
inhaled corticosteroidsHistory of depression, substance
abuse, personality disorder,unemployment, or recentbereavement
Physician Quality Measures forAsthma Care Endorsed by theNational Quality ForumAssessment of asthma control: the
percentage of patients aged 5 to 40years with a diagnosis of asthma whowere evaluated during at least oneoffice visit during the measurementyear for frequency of daytime andnocturnal asthma symptoms.
Assessment of appropriate therapy: thepercentage of patients 5 to 64 years ofage during the measurement year whowere identified as having persistentasthma and who were appropriatelyprescribed medication during themeasurement year.
physician reimbursement from Centers for Medicare & MedicaidServices (CMS) will be subject tovalue-based modification, based onsome of the measures described
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
index.htmInformation on asthma from the National Institutes of Health
MedlinePlus, including an interactive tutorial in English andSpanish.
www.nhlbi.nih.gov/health/health-topics/topics/asthma/www.nhlbi.nih.gov/health-spanish/health-topics/temas/asthma/Information for patients on asthma, in English and in Spanish,
from the National Heart, Lung, and Blood Institute (NHLBI).www.cdc.gov/asthma/faqs.htmAnswers to frequently asked questions about asthma from the
Centers for Disease Control and Prevention.
Clinical Guidelineswww.nhlbi.nih.gov/guidelines/asthma/asthsumm.pdfEvidence-based guidelines for the diagnosis and management of
asthma from the National Asthma Education and PreventionProgram in 2007.
Practice parameter on the pathogenesis, prevalence, diagnosis, andmanagement of exercise-induced bronchoconstriction from theAmerican Academy of Allergy, Asthma and Immunology; theAmerican College of Allergy, Asthma and Immunology; and theJoint Council of Allergy, Asthma and Immunology in 2010.
www.whiar.org/docs/ARIA-Report-2008.pdfGuidelines on allergic rhinitis and its impact on asthma from the
World Health Organization in 2008.
Diagnostic Tests and Criteriahttp://smartmedicine.acponline.org/content.aspx?gbosId=108&result
previously. CMS has also developedprevention quality indicators aspart of performance measurementfor Medicare Accountable CareOrganizations and uses the ratioof observed-to-expected hospital
admissions for asthma or COPD asa reflection of quality of asthma care(www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/Measure-ACO-9-Asthma.pdf ).
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
In the ClinicAnnals of Internal Medicine
Pati
ent
Info
rmat
ion
WHAT YOU SHOULDKNOW ABOUT ASTHMA
What is asthma?• A long-term disease that affects the lungs and caus-
es wheezing, chest tightness, difficulty breathing,and coughing.
• When an asthma attack occurs, tubes (bronchi) thatbring air to the lungs tighten, and breathing be-comes difficult.
• An asthma attack can occur when something irri-tates your lungs, such as smoke, mold, or dust mites.
How is it diagnosed?• Your doctor will ask you questions about your symp-
toms and whether anyone in your family has hadasthma or other breathing problems.
• A simple breathing test called spirometry may beperformed to check how well your lungs arefunctioning.
• Spirometry measures how much air you can breatheout after taking a very deep breath.
How is it treated?• Long-term medicines that you take every day can
help prevent asthma attacks, but don’t help you dur-ing an attack.
• Quick-relief medicines can reduce your symptomswhen attacks occur.
• If you need to use your quick-relief medicines moreand more, your doctor may need to prescribe a dif-ferent medicine.
• A personalized asthma action plan helps guide youon when to take medications and how to adjustthem to keep your asthma under control.
• Call your doctor or go to the hospital if it is hard tobreathe and your medicines are not helping.
How can you prevent an asthma attack?• Stay away from what makes your asthma worse,
such as dust, smoke, animals, and cold or dry air.• Don’t smoke, and stay away from people who do.• Asthma-proof your home—for example, discard old
carpets and drapes, and use a special mattress andpillow covers.
• Use air conditioners and dehumidifiers.• Take your medicines that prevent attacks every day,
even when you don’t have symptoms.• Take your medicines that stop attacks when you
need them.• Learn the right way to use your inhalers.
For More Informationwww.nhlbi.nih.gov/health/public/lung/asthma/have_asthma.htmwww.nhlbi.nih.gov/health/public/lung/asthma/asthma_atglance.pdfA handout titled, “So You Have Asthma: A Guide for Patients and
Their Families” and asthma facts from the NHLBI.
www.nhlbi.nih.gov/health/public/lung/asthma/actionplan_text.htmAn asthma action plan worksheet from the NHLBI.
www.nlm.nih.gov/medlineplus/ency/presentations/100200_1.htmA tutorial on proper use of a metered-dose inhaler.
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
Questions are largely from the ACP’s Medical Knowledge Self-Assessment Program (MKSAP, accessed at http://www.acponline.org/products_services/mksap/15/?pr31). Go to www.annals.org/intheclinic/
to complete the quiz and earn up to 1.5 CME credits, or to purchase the complete MKSAP program.
1. A 50-year-old woman is evaluated for arecent increase in asthma symptomscharacterized by daily cough anddyspnea. She reports waking up two tothree nights per week with asthmasymptoms. She has no postnasal drip,nasal discharge, fever, or heartburn. Hercurrent medications are medium-doseinhaled corticosteroids and albuterol asneeded. She is able to demonstrateproper use of her metered-dose inhalers.
On physical examination, she appearscomfortable and is in no respiratorydistress. Pulse rate is 76/min, andrespiration rate is 18/min. Pulmonaryexamination reveals bilateral wheezing.The remainder of the examination isnormal.
Which of the following is the mostappropriate treatment?
A. Add a long-acting β2-agonist inhalerB. Add an ipratropium metered-dose
inhalerC. Double the dose of inhaled
corticosteroidsD. Start a 10-day course of a macrolide
antibiotic
2. A 51-year-old man is evaluated forworsening of asthma symptomscharacterized by frequent daytimewheezing and cough, as well asnocturnal awakening related to asthmatwo to three times per week. He hasbeen using his inhalers regularly withoutadequate relief. He has not had recentupper respiratory tract infection,sinusitis, postnasal drip, or newexposures. He is taking an inhaledcorticosteroid and inhaled albuterol.
On physical examination, temperature is37.0°C (98.6°F), blood pressure is 135/80 mm Hg, pulse rate is 80/min, andrespiration rate is 18/min. Pulmonaryexamination reveals scattered bilateralwheezing. Spirometry shows an FEV
1of
70% of predicted. Following an inhaled
bronchodilator, FEV1improves to 90% of
predicted.
Which of the following is the mostappropriate next step in management?
A. Add a leukotriene receptor antagonistB. Add prednisoneC. Observe the patient using his inhalersD. Obtain a 2-week symptom and peak
flow diary
3. A 32-year-old man is evaluated forchronic cough that has lasted nearly 1 year. He recalls noticing the coughinitially after a “bad cold.” At that timehe received two courses of antibiotics(including a macrolide and a fluoro-quinolone) with improvement in theacute symptoms. However, hesubsequently noted persistent cough,particularly at nighttime and on colddays. Episodes of cough often occur afterexercise or laughing. He is currentlyasymptomatic, with no postnasal drip,nasal congestion, or heartburn. He doesnot smoke. He has no history ofoccupational or other exposures. He hasa remote history of hay fever. Multiplefamily members have seasonal allergies.His only medication is a proton pumpinhibitor, which he has taken for the past6 months without benefit.
On physical examination, vital signs arenormal. The oropharynx appears normal,with no cobblestone appearance. There isno mucus in the nostrils or oropharynx.Pulmonary examination is normal.Spirometry shows an FEV
1of 90% of
predicted and an FEV1/FVC ratio of 80%.
Chest radiograph is normal.
Which of the following is the mostappropriate diagnostic test to performnext?
A. Bordetella-specific antibodiesB. Bronchial challenge C. BronchoscopyD. Chest CT scan
4. A 20-year-old man is evaluated during aroutine examination. He has a history ofepisodes of bronchitis since early child-hood; symptoms include productivecough, wheezing, and shortness of breath.He is being treated for asthma, but hissymptoms have not been well-controlled.His current medications are a medium-dose inhaled corticosteroid and a long-acting β2-agonist, with documentedsatisfactory inhaler technique.
On physical examination, temperature is 37.2°C (99.0°F), blood pressure is 110/65 mm Hg, pulse rate is 82/min, andrespiration rate is 18/min; BMI is 20kg/m2. Small nasal polyps are noted.Pulmonary examination reveals diffuserhonchi and scattered wheezing. Theneck veins are flat. Cardiac examinationreveals a normal S
1and S
2with a soft
grade 1/6 systolic murmur. Clubbing isnoted. There is no pedal edema, andpulses are intact and symmetric. Oxygensaturation breathing ambient air is 93%.
Laboratory studies reveal a hemoglobinlevel of 11 g/dL (110 g/L) and a leukocytecount of 9800/µL (9.8 × 109/L). Chestradiograph shows increased bronchialmarkings consistent with bronchiectasisin the upper lung zones.
Which of the following is the mostappropriate next step in management?
A. Measure sweat chlorideB. Perform bronchoscopyC. Perform echocardiographyD. Record symptoms and medication use
over 2 weeks
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014
Inhaled long-acting Sympathomimetic effects, Black box warning: Asthma- For moderate-severe β2-agonists such as tremor and tachy- related death. persistent asthma.
cardia. Paradoxical broncho- Caution with: CV disease, Must also use an spasm, hypersensitivity reactions. hyperthyroidism, diabetes, asthma controllerRare: hypokalemia, hyper- narrow-angle glaucoma, glycemia seizure disorder. Tolerance
can occur over timeFormoterol (Foradil Powder in capsules for use with
Aerolizer) Aerolizer: 12 µg every 12 hSalmeterol (Serevent 50 µg (1 oral inhalation) every 12 h
Diskus)Oral corticosteroids Long-term use can result in: For acute exacer-
HPA suppression, immuno- bations. Not generally suppression, hypertension, for long-term useadverse neurologic effects, glucose intolerance, weight gain, myopathy, cataracts, osteoporosis
Prednisone 40-80 mg total daily dose, dosed 1-2 times/d, for a total course of 3-10 days; tapered doses may be considered
Prednisolone (Prelone, 40-80 mg total daily dose, Flo-Pred, Orapred) dosed 1-2 times/d, for a total
course of 3-10 days; tapered doses may be considered
Methylprednisolone PO or IV: 40-80 mg total daily (Medrol) dose, dosed 1-2 times/d, for a
total course of 3-10 days; tapered doses may be considered
MethylxanthineTheophylline (Theolar, Dose must be individualized. GI side effects, CV adverse Narrow therapeutic index.
Theocron, Theo-24) Aim for serum levels between effects Many drug interactions due 5 and 15 µg/mL. IV: 0.2- to CYP450 hepatic meta-0.4 mg/kg/h Immediate- bolism. Use low dose with: release: Initially 300 mg total hepatic disease, HF, elderly. daily dose, dosed every 6-8 h. Caution with: cardiac disease, Can increase to 400-1600 mg thyroid disease, peptic ulcer total daily dose, dosed every disease, prostatic hypertrophy, 6-8 h. Extended-release: Initially seizure disorder, smoking300 mg total daily dose, dosed every 8-12 h. Can increase to 400-1600 mg total daily dose, dosed every 8-12 h. Controlled-release (Theo-24): Initially 300- 400 mg every 24 h. Can increase to 400-1600 mg total daily dose, dosed every 12-24 h
struction, prostatic hypertrophyIpratropium (Atrovent, MDI (17 µg/inhalation): 2-3 May have additive benefit
Atrovent HFA) inhalations 4 times/d. Nebulizer: to inhaled beta2-agonists
500 µg 3-4 times/d for severe exacerbationsTiotropium (Spiriva) Powder in capsules for use with
HandiHaler: 18 µg once dailyAnti-IgE antibody
Omalizumab (Xolair) 150-375 mg SC every 2 or 4 CV and cerebrovascular Black box warning: Ana- For severe per-weeks. Dose based on baseline adverse events, infection, phylaxis. Caution in patients sistent asthma serum IgE and body weight rare systemic eosinophilia with high risk for malignancy, not controlled
Downloaded From: http://annals.org/ by a Univ Hospitals of Cleveland User on 03/20/2014