Inflammation is a process carried out in response to either physical or immunological tissue insult. It consists of a destructive process to remove the inflammatory trigger and damaged tissue, followed by repair and replacement. The main actors in the destructive phase are neutrophils and macrophages. Inflammation is signaled by heat, pain, redness, and swelling (calor, dolor, rubor, tumor). Inflammatory conditions are named with the suffix itis. Chapter 10 Inflammation
Transcript
Inflammation is a process carried out in response to either physical or immunological tissue insult.
It consists of a destructive process to remove the inflammatory trigger and damaged tissue, followed by repair and replacement.
The main actors in the destructive phase are neutrophils and macrophages.
Inflammation is signaled by heat, pain, redness, and swelling (calor, dolor, rubor, tumor).
Inflammatory conditions are named with the suffix itis.
Chapter 10 Inflammation
Macrophages are highly complex cells engaged in normal tissue maintenance and turnover.
Among their varied functions, they are sentinels against infection, both through the use of receptors for common molecules carried by pathogens, and through opsonization.
Macrophages exist in various levels of activation, wherein they become more aggressive at destroying macromolecules, and sending distress signals to recruit other components of the inflammatory response.
The most aggressively activated macrophages are derived from blood monocytes in response to inflammatory signals. These are called “infiltrating macrophages”.
Names of Macrophages According to Tissue Locations
heparin: chopped up glycosaminoglycan released from mast cells, or administered clinically. Stimulates antithrombin III, which inhibits factors IIa, IXa, Xa, XIa, and XIIa. Reversed by protamine sulfate.
heparan sulfate: on surface of endothelial cells acts like heparin.
thrombomodulin: on surface of endothelial cells; activates Protein C & S; Protein C cleaves and inactivates factors VIIIa and Va.
prostaglandin I2 (PGI2): secreted by endothelial cells inhibits platelet activation.
Fibrinogen
fibrin
Thrombin removes N ter. propeptides
half staggered array
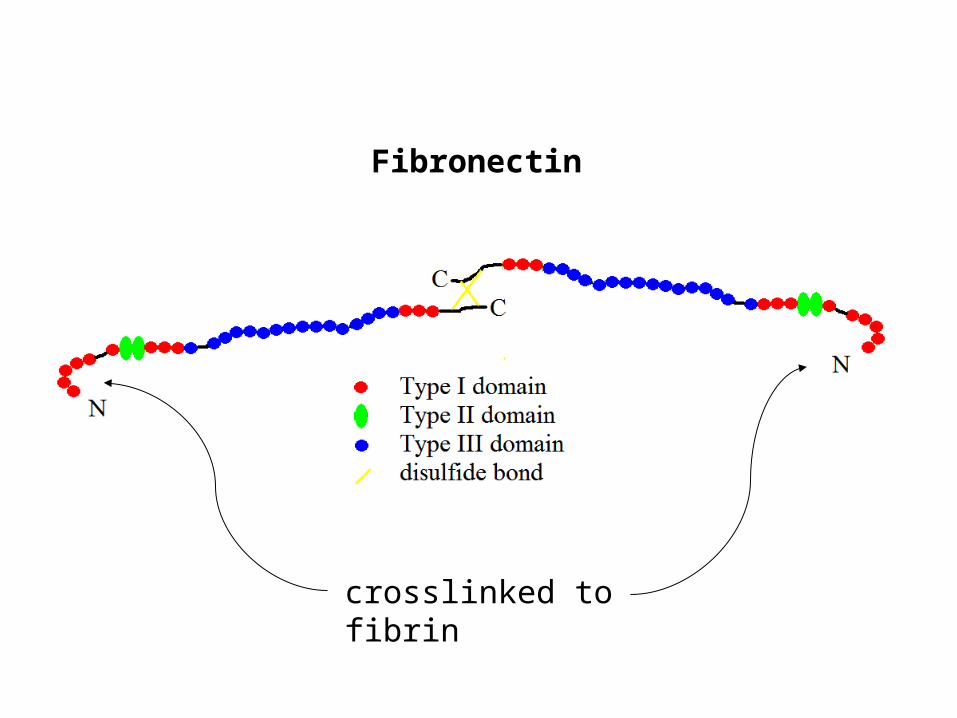
Fibronectin
crosslinked to fibrin
Fibrinolysis
plasminogen plasmin
tissue plasminogen activator
TPA resolving a clot in a coronary artery
Causes of abnormal bleeding
Genetic
hemophilia. A (F-VIII),
B (F-IX). X-linked
von Willebrand Diseaseup to 1%, men or women
Drugs
coumadin, plavix, aspirin,
Vascular fragilityvitamin C deficiency, connective tissue disorders
Diseases affecting platelets
leukemia, AIDS
Diseases affecting the liver
cirrhosis
chemotherapy, alcohol,
broad spectrum antibiotics
Laboratory Tests
Platelet count
Prothrombin time (PT/INR)
plasma from patient plus thromboplastin (contains triggers of extrinsic pathway)
Measures 3 Vit K dependent factors. VII has shortest half life of vitamin K-dependent factors.
Time to clot normalized by normal controls and adjusted for the potency of the thromboplastin is called INR (0.8 – 1.2 is normal).
Partial thromboplastin time (PTT)
plasma from patient plus thromboplastin (without TF) plus trigger of intrinsic pathway.
Functions of the clot
Stop bleeding
Seal against infection
Scaffold for epithelial cells, and for deposition of granulation tissue