25
Influenza Clinic Volunteer Orientation 2013-2014
| Date post: | 11-Dec-2015 |
| Category: |
Documents |
| Upload: | raymundo-goldsmith |
| View: | 216 times |
| Download: | 2 times |
Influenza Clinic Volunteer Orientation
2013-2014
Introduction to Operation Immunization
Leadership
Operation Immunization Co-Chairs- Michelle Hancock, Melissa Sanders
Operation Immunization Committee Leaders- Kathleen Drobnicki, Carline Joseph, Alex Miller, Verona Xhixhi
Operation Immunization Advisor- Dr. Ohri, Dr. Castillo
Shoo the Flu Vaccine Clinic Coordinator- Sue Weston
OISSE- Kate Martens Stricklett
Additional Event Coordinator- Dr. O’Brien
Introduction to Operation Immunization
• Activities– Vaccination Clinics– Screening, Education & Promotion Events

Introduction to Operation Immunization:
Vaccine Clinics
• Shoo the Flu at CU• Community Engagements• Doses from the Dean
Introduction to Operation Immunization:
Screening, Promotion & Education
• Goal:Spread awareness of certain disease states preventable through immunizations in children, adolescent, adult, and elderly populations

Introduction to Operation Immunization:
Screening, Promotion & Education
• Binational Health Week Events• Youth Emergency Services (YES) Clinic• Holy Family Church Clinic• Joy of Life Ministries• Mexican Consulate

Introduction to Operation Immunization:
Screening, Promotion & Education
• Vaccine-Preventable Diseases
• Vaccine Promotion

Introduction to Operation Immunization:
Screening, Promotion & Education
• Opportunities to get involved– “Shoo the Flu at CU” advertising campaign
– Vaccine promotion poster creation
How to Volunteer
• Clinic Dates• Eventbrite• Approved for Service Hours
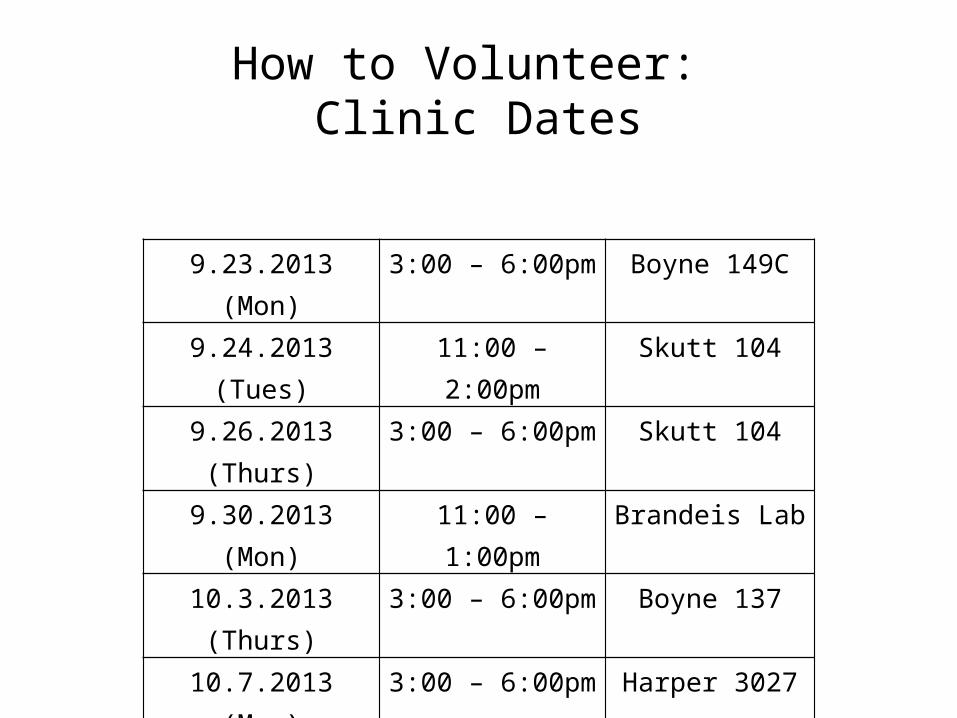
How to Volunteer: Clinic Dates
9.23.2013 (Mon) 3:00 – 6:00pm Boyne 149C9.24.2013 (Tues) 11:00 – 2:00pm Skutt 1049.26.2013 (Thurs) 3:00 – 6:00pm Skutt 1049.30.2013 (Mon) 11:00 – 1:00pm Brandeis Lab10.3.2013 (Thurs) 3:00 – 6:00pm Boyne 13710.7.2013 (Mon) 3:00 – 6:00pm Harper 3027
10.10.2013 (Thurs) 3:00 – 6:00pm Criss III L-6010.23.2013 (Wed) 11:00 – 2:00pm Skutt Ballroom10.28.2013 (Mon) 3:00 – 6:00pm Harper 3027

How to Volunteer: Registration
• OISSE• Eventbrite • Community Engagement Cues

Operation Immunization Training Video

Special Circumstances
• Addressing Patient Anxiety • Emergency Response– Fainting– Needlestick– Anaphylaxis
Special Circumstances:ABCs of Addressing Patient Anxiety
• A = Assess your patient – Look for signs of anxiety (patient admits to fear or history of fainting; joking but appears nervous; pale, trembling; resisting vaccination)
• B = Be prepared and empathetic– Practice what to say & do to help nervous patients; No razzing!
• C = Comfort– Offer privacy and support; Ask supervisor/another vaccinator/ patient’s companion to assist you in supporting patient through process (hand on shoulder or hold patient’s hand); Care for behind screen
• D = Distraction– Ask patient about school, work……… Chat about trivia / Tell a joke; Ask patient to try whistling – Afterwards: Compliment patient on bravery in going through with vaccination even when nervous; Review benefits of vaccination

Special Circumstances:Emergency Response - Fainting
• Fainting:- Patient becomes pale or dizzy, especially upon rising from chair; may indicate that they are feeling “funny”
• Action: - Help person to sit back securely, and support to prevent falling OR help person to lay on the floor and elevate feet
• Notify supervisor immediately • The patient will typically recover within a few minutes, but
should not be released to leave until checked by the clinic faculty or staff supervisor.

Special Circumstances: Emergency Response – Needle Stick
• Needle Stick – injection of a used needle onto or below the skin of a person other than the individual just injected with the needle- Exposure to bloodborne pathogens is possible with any such exposure regardless of knowing the vaccinee, or the extent of exposure (volume or how deep under the skin)
• Seek assistance of supervisor immediately with any such exposure
• Next step will be to clean the area thoroughly with soap and water. Supervisor will direct further action.

Special Circumstances:Emergency Response - Anaphylaxis
• Symptoms of concern may present as rapid onset itching, skin redness, swelling/hives; sneezing, hoarseness, wheezing, increasing breathing difficulty; passing out
• Seek assistance of supervisor immediately • Epi Pen: An auto-injector used for the emergency
injection of epinephrine, medicine used for life-threatening allergic reactions- Must always be available during clinic. Supervisor will direct on use, and on triggering of 911.


FluMist

Influenza Vaccines
Two types of influenza vaccine:
1. Inactivated vaccine - Does not contain live virus components- Administered by injection
2. Live, attenuated vaccine- Contains weakened virus (quadrivalent)- Administered in a Nasal Spray. Available in Student Health—$20/dose

INACTIVATED INFLUENZA VACCINATION CONSENT FORM2013-2014
Circle one
1. Is this the 1st flu vaccine you have received? YES NO
2. Are you under 19 years of age? YES NO
3. Do you have a fever or active infection today? YES NO
4. Do you have a history of Guillain-Barre Syndrome YES NO (severe paralytic illness)?
5. Do you have a severe (life threatening) allergy to the following?
A. Eggs or chicken? YES NO B. Thimerosal (mercury derivative)? YES NO
6. Have you had a severe allergic reaction to any vaccine? YES NO
If yes, explain: ______________________________________________________
“I have had a chance to ask questions that were answered to my satisfaction. I believe that I understand the benefits and risks of the Fluvirin® vaccine and ask that the vaccine be given to me or to the person named below for whom I am authorized to make this request.”
NET ID: ____________________________________ DATE OF BIRTH: ______/______/______ NAME:
LAST FIRST MI
Signature of person to receive vaccine or person authorized to make request (parent or guardian)
X______________________________________ DATE: ______________
Lot: ________________Exp: 5.31.2014VIS: 07.26.2013Injection site: L / R deltoid
Administered By:_________________________________________________________________DATE:____________________
08.2013
Student/Staff
Student Health Services

Thank you! Questions? Please contact:
Michelle Hancock [email protected]
Melissa [email protected]
Dr. Ohri [email protected]


















