-11- Instructions for Completion of Medical Services/Supplies (MA 319) Invoice All invoices must be completed legibly. COMPLETENESS AND ACCURACY ARE IMPOR- TANT, SINCE INFORMATION IS KEY-PUNCHED EXACTLY AS IT APPEARS ON THE INVOICE. The invoices need not be typed,however, typing will reduce the chance of data entry errors and decrease processing time by taking advantage of the Department's Image Character Recognition (lCR) capabilities. If completing the invoices by hand, please use black ink. One (1) MA 319 Invoice can accommodate a maximum of four (4) claim lines for a patient. In certain instances, however, separate invoices must be completed. These are: 1. Invoices submitted for Medicare Part B deductible and/or coinsurance. 2. Services provided from different office locations by the same provider. 3. All services covered by another third party payor must be separated from those not covered. 4. Services requiring prior authorization should be separated from those which do not require prior authorization. Invoices for the retroactive period up to and including March 1998 must be submitted within the time frames specified under Procedure: of this bulletin. For services provided on or after April 1, 1998, invoices should be submitted as soon after completion of the service as possible. However, all original invoices must be received within 180 days following the date of service. The MA 319 Invoice is divided into four (4) sections: Patient Information Provider Information Compensable Medical Services Remarks and Signatures The following billing instructions identify the types of items appearing on the ,MA 319 Invoice: 1. Must - These items require completion in order to process the claim for payment. Failure to complete these items will result in the claim being rejected. 2. Must, if applicable - These items require completion if the item applies to the patient, the provider, or the service rendered. Failure to complete these items when applicable may result in the claim being rejected or pended for manual review. 3. Optional - These items do not require completion in order to process the claim. How- ever, completion of these items may aid the Department in processing your invoice or may assist you in your record keeping. 4. Leave Blank - These items are for Department use or are reserved for use at a later time.
Transcript
-11-
Instructions for Completion of Medical Services/Supplies (MA 319) Invoice
All invoices must be completed legibly. COMPLETENESS AND ACCURACY ARE IMPORTANT, SINCE INFORMATION IS KEY-PUNCHED EXACTLY AS IT APPEARS ON THE INVOICE.The invoices need not be typed,however, typing will reduce the chance of data entry errors anddecrease processing time by taking advantage of the Department's Image Character Recognition(lCR) capabilities. If completing the invoices by hand, please use black ink.
One (1) MA 319 Invoice can accommodate a maximum of four (4) claim lines for a patient. Incertain instances, however, separate invoices must be completed. These are:
1. Invoices submitted for Medicare Part B deductible and/or coinsurance.
2. Services provided from different office locations by the same provider.
3. All services covered by another third party payor must be separated from those notcovered.
4. Services requiring prior authorization should be separated from those which do notrequire prior authorization.
Invoices for the retroactive period up to and including March 1998 must be submitted within thetime frames specified under Procedure: of this bulletin. For services provided on or after April 1,1998, invoices should be submitted as soon after completion of the service as possible. However, alloriginal invoices must be received within 180 days following the date of service.
The MA 319 Invoice is divided into four (4) sections:
Patient InformationProvider InformationCompensable Medical ServicesRemarks and Signatures
The following billing instructions identify the types of items appearing on the ,MA 319 Invoice:
1. Must - These items require completion in order to process the claim for payment.Failure to complete these items will result in the claim being rejected.
2. Must, if applicable - These items require completion if the item applies to the patient,the provider, or the service rendered. Failure to complete these items when applicablemay result in the claim being rejected or pended for manual review.
3. Optional - These items do not require completion in order to process the claim. However, completion of these items may aid the Department in processing your invoice ormay assist you in your record keeping.
4. Leave Blank - These items are for Department use or are reserved for use at a latertime.
-12-
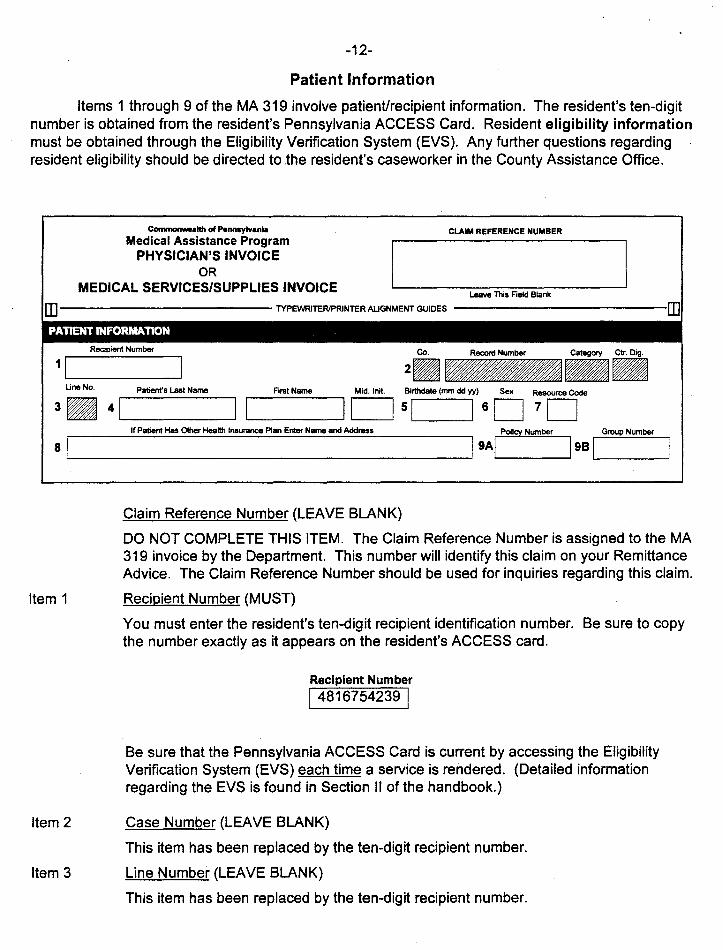
Patient Information
Items 1 through 9 of the MA 319 involve patient/recipient information. The resident's ten-digitnumber is obtained from the resident's Pennsylvania ACCESS Card. Resident eligibility informationmust be obtained through the Eligibility Verification System (EVS). Any further questions regardingresident eligibility should be directed to the resident's caseworker in the County Assistance Office.
~altll of Pennsylvania
Medical Assistance ProgramPHYSICIAN'S INVOICE
ORMEDICAL SERVICES/SUPPLIES INVOICE
CLAIM REFERENCE NUMBER
Leave This Field Blank
If Patiem Has Other Health Insurance Plan Enter Name and Address
DO NOT COMPLETE THIS ITEM. The Claim Reference Number is assigned to the MA319 invoice by the Department. This number will identify this claim on your RemittanceAdvice. The Claim Reference Number should be used for inquiries regarding this claim.
Item 1 Recipient Number (MUST)
You must enter the resident's ten-digit recipient identification number. Be sure to copythe number exactly as it appears on the resident's ACCESS card.
Recipient Number
I 4816754239 I
Be sure that the Pennsylvania ACCESS Card is current by accessing the EligibilityVerification System (EVS) each time a service is rendered. (Detailed informationregarding the EVS is found in Section II of the handbook.)
Item 2 Case Number (LEAVE BLANK)
This item has been replaced by the ten-digit recipient number.
Item 3 Line Number (LEAVE BLANK)
This item has been replaced by the ten-digit recipient number.
Item 4 Patient's Name (OPTIONAL)
Enter the resident's last name, first name, and middle initial, if any, in the appropriateboxes.
Patient's Last Name
DOE IFirst Name
MARYMid.lnit.
[TI
The name entered in item 4 is not keypunched. The names appearing on the Remittance Advice are taken from the Department's computerized list of recipients. If theten-digit recipient number you have recorded on the invoice does not match with anumber on the Department's file, a blank space will appear on the Remittance Advicewhere the resident's name would normally appear.
Item 5 Birthdate (OPTIONAL)
Enter the resident's birthdate in six-digit format (month, day, year). Enter a zero to theleft of all one-digit numbers.
For example, if the resident's birthday is November 9, 1957, enter:
Birthdate (mmddyy)
51 110957 IItem 6 Sex (OPTIONAL)
Enter the appropriate letter: M (Male), F (Female)
-13-
Item 7 Resource Code (MUST, IF APPLICABLE)
If the resident has another resource available to pay for the service, bill the other resource before billing Medical Assistance. The resource code can be obtained throughthe EVS. Also, ask the resident if he/she has any medical resources not listed on theEVS.
If there is more than one resource available, enter the code for the one most likely tocover the service provided. If none of the following apply, leave this item blank.
1 - Medicare Part B2 - Blue Cross3 - Blue Shield4 - Champus6 - Medicare Part A7 - Other8 - Worker's Compensation/Casualty Insurance
For example, if the resident has private insurance, such as Prudential, Aetna, etc., andit covers the service provided, enter:
Resource Code
71 7
Items 8and 9Aand 9B
Other Insurance, Name and Address, Policy Number, and Group Number (MUST, IFAPPLICABLE)
Complete these items only if the Resource Code is not on the patient's EVS record or isa Resource Code 7 (Other).
For example, if the patient has G.G.P. Mutual Insurance, enter:
If Patient Has Other Health Insurance Plan Enter Name and Address
81 G.G.P. MUTUAL INSURANCE ANYTOWN, PA. I
Policy Number
9AI 12576 43 8279D
810007981
-14-
Provider Information
Items 10 through 18 of the MA 319 involve information about you, the provider of service. Theinformation is obtained from your Provider Notice Information, which was sent to you by the Department. (See Section IV of the handbook - Provider Notice Information Form.)
Name of Provider
--------------------------------------PROVIDER INFORMATION .
Provider Type Provider MA 10 Number Provider Address Code Provider's Own Reference Number
101L....- 111D 121 113 D 141 ITo Delete Payee Payee Type Payee MA 10 Number
~:m.. 151 110 171 I 18D For Setvices Related toContaining . ... Hospitelization Care Give Oates!;
191 F~lny Name I 20r'nx MA 10 NumberI ~~e rdmilted (mm ddr~;i Discharged (mmi yy)
Box
fXl Name of Referring/Supervising/Attending Practitioner or Prescriber Referring Practitioner's or Prescriber's Ucense Number
Enter the name of the provider of service as indicated on the Provider Notice InformationForm.
Name of Provider
101 OUR TOWN NURSING HOME I
Item 11 Provider Type (MUST)Enter your two-digit provider type. The provider type is assigned by the Departmentand is found on the enrollment notice sent to you by the Department.
Provider Type
11~
Item 12 Provider MA ID Number (MUST)Enter your current seven-digit Medical Assistance identification number. The identification number is assigned by the Department.
Provider MA 10 Number
121 0628066 I
Item 13 Provider Address Code (MUST)
Enter the two-digit address code for the office where the service was provided. If youare billing for nursing facility services, enter the site address code. The address code isfound on the enrollment notice sent to you by the Department.
Provider Address Code
13~
Item 14 Provider's Own Reference Number (OPTIONAL, BUT RECOMMENDED)
Enter a patient file number or the patient's name (up to ten (10) digits or letters). Thiswill appear on the Remittance Advice and will help identify your claim.
It is recommended that you use this field as it will provide a second claim identifier if therecipient eligibility number does not match the Department's file.
Provider's Own Reference Number
141 DOEM IOR
Provider's Own Reference Number
141 98134766 I
Item 15 Payee Name (LEAVE BLANK)
Nursing facilities should leave this item blank.
Item 16 Payee Type (LEAVE BLANK)
Nursing facilities should leave this item blank.
Item 17 Payee MA 10 Number (LEAVE BLANK)
Nursing facilities should leave this item blank.
Item 18 Payee Address Code (LEAVE BLANK)
Nursing facilities should leave this item blank.
Items 19 Facility Name/MA 10 Number (LEAVE BLANK)and 20
Nursing facilities should leave these items blank.
Items 21 Hospitalization - Date Admitted/Date Discharged (LEAVE BLANK)and 22
Nursing facilities should leave these items blank.
Item 23 Name of Referring/Supervising/Attending Practitioner or Prescriber (MUST, IF APPLICABLE)
Enter the name and degree of the referring/supervising/attending practitioner or prescriber.
-16-
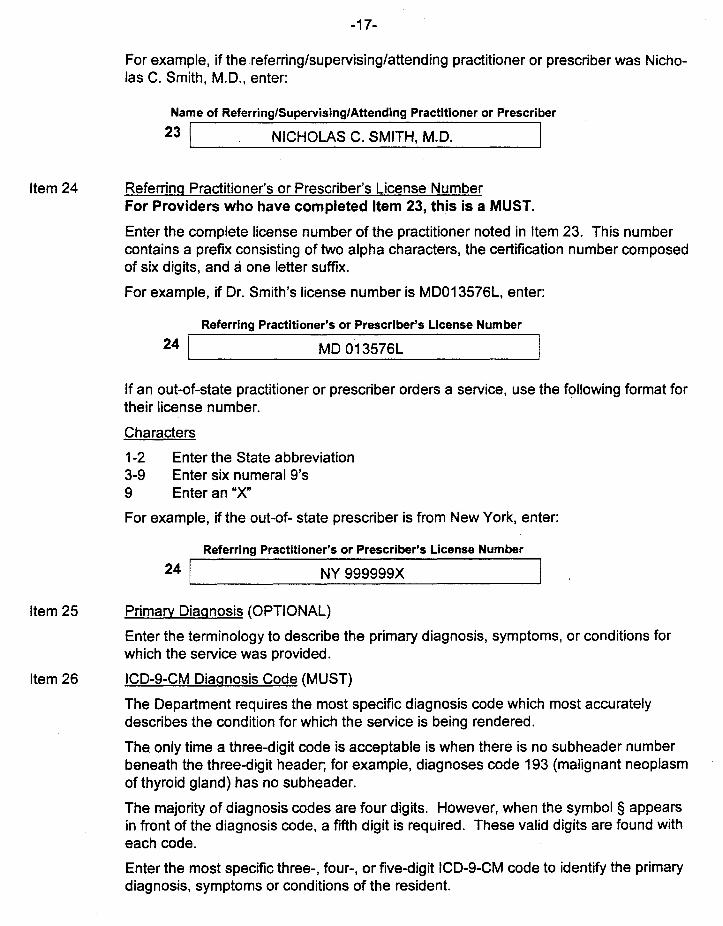
For example, if thereferring/supervising/attending practitioner or prescriber was Nicholas C. Smith, M.D., enter:
Name of Referring/Supervising/Attending Practitioner or Prescriber
23 I NICHOLAS C. SMITH, M.D. I
Item 24 Referring Practitioner's or Prescriber's License NumberFor Providers who have completed Item 23, this is a MUST.
Enter the complete license number of the practitioner noted in Item 23. This numbercontains a prefix consisting of two alpha characters, the certification number composedof six digits, and a one letter suffix.
For example, if Dr. Smith's license number is MD013576L, enter:
MD 013576L
Referring Practitioner's or Prescriber's License Number
241--------------------
If an out-of-state practitioner or prescriber orders a service, use the following format fortheir license number.
Characters
1-2 Enter the State abbreviation3-9 Enter six numeral 9's9 Enter an "X"
For example, if the out-of- state prescriber is from New York, enter:
Referring Practitioner's or Prescriber's License Number
24 1 N_Y_9_9_9_99_9_X _
Item 25 Primary Diagnosis (OPTIONAL)
Enter the terminology to describe the primary diagnosis, symptoms, or conditions forwhich the service was provided.
Item 26 ICD-9-CM Diagnosis Code (MUST)
The Department requires the most specific diagnosis code which most accuratelydescribes the condition for which the service is being rendered.
The only time a three-digit code is acceptable is when there is no subheader numberbeneath the three-digit header; for example, diagnoses code 193 (malignant neoplasmof thyroid gland) has no subheader.
The majority of diagnosis codes are four digits. However, when the symbol § appearsin front of the diagnosis code, a fifth digit is required. These valid digits are found witheach code.
Enter the most specific three-, four-, or five-digit ICD-9-CM code to identify the primarydiagnosis, symptoms or conditions of the resident.
-17-
Note: The ICD-9-CM Diagnosis Codes pUblications may be obtained from:
ICD-9-CM Third EditionVolumes 1 & 2P. O. Box 360121Pittsburgh, PA 15250-6121
ICD-9-CMP.O. Box 971Ann Arbor, MI 481060971
Note: Only Volumes 1 &2 can be obtained from the first address. Volume 3 can beobtained from:
.Superintendent of DocumentsU.S. Government Printing OfficeDepartment 33Washington, D.C. 204029325
For example, if the patient's diagnosis is colostomy status, enter:
-18-
ICD-9-CM DIAGNOSIS CODE
26 1 V443 I
To bill for radiological services, electrocardiograms or electroencephalograms and thediagnosis is not furnished, enter XRY11.
Item 27 Secondary Diagnosis (OPTIONAL)
If applicable, enter the terminology to describe the secondary diagnosis, symptoms orconditions that are present.
Item 28 ICD-9-CM Diagnosis Code (MUST, IF APPLICABLE)
If there is a secondary diagnosis present, enter the appropriate ICD-9-CM DiagnosisCode to identify it.
-19-
Compensable Medical Services
Items 29 through 320 of the MA 319 identify the services you have provided to the patient.Nursing facilities billing on the MA 319 for Medicare Part B should use the procedure codes usedwhen billing Medicare for the services provided.
COMPENSABLE MEDICAL SERVICES
NOTE: THE RELATED ITEMS IN LINES 30 THROUGH 32 MUST BE COMPLETEDWHEN BILLING FOR MORE THAN ONE SERVICE.
To the left of each claim line is one (1) unnumbered box. Ifan error has been made ona claim line, place an "X" in this box at the beginning of the line. Placing an X in thisbox will delete everything entered on that claim line.
To DeleteClaimUne
ContainingErrorTypeXinBox
Thus 0In TheSpace
ProvidedBelow
~
Item 29A Procedure Name or Manufacturer's Name/Stock Number (OPTIONAL)
Enter the terminology to describe the service provided. For example, if the residentrequired a drainable pouch, enter:
Procedure Name or Manufacturer's Name/Stock Number
A I POUCH, DRAINABLE I
Item 29B Service Begin (MUST, IF APPLICABLE)
If the same service was provided on consecutive days, enter the first day of servicehere. Use a six-digit format for all dates.
If you are billing for a service that was provided on one day only, DO NOT USE THISBOX.
Item 29C Service End (MUST)
This date will indicate the date of service if the service was provided on only one day;or the last consecutive day the same service was provided. Use a six-digit format for alldates.
NOTE: CONSECUTIVE SERVICE DATES ARE THOSE CONTIGUOUS CALENDARDAYS DURING WHICH THE SAME SERVICE WAS PROVIDED. IF THEDATES ARE NOT CONSECUTIVE, SEPARATE CLAIM LINES MUST BEUSED.
For example, if the same service was provided on September 7 and September 8,
1996, enter: Ser. Beg. (mmddyy)
B I 090796 ISer. End (mmddyy)
C I 090896 IIf the service was provided on September 9, 1996 only, enter:
Ser. End (mmdd
C 090996
-20-
Items 290&29E
Visit Code (MUST, IF APPLICABLE)
Enter the appropriate code to identify the type of visit.
If none of the codes apply, leave these items blank.
04- Vehicle Accident (includes all types of vehicles covered by insurance)05- Accident (other than vehicle)06- Family Planning09- Service rendered to a pregnant woman or related to a delivery10- Service rendered to a resident of a medical facility as defined in §11 01.63(b)(2)(iii)11- Copayment was not paid by the recipient. The Department will still
deduct copay from invoice.
For example, if the visit is for a service rendered to a resident of a medical facility, enter:
Visit Code
o I 10 I
Item 29F Emergency Code (MUST, IF APPLICABLE)
If the service provided was on an emergency basis, enter the number 1. If the servicewas urgent, enter the number~. If the service was elective, leave this item blank.
Emer. Code
F I 2 I
Item 29G Diagnosis (OX) Number (MUST)
If the service was provided for the primary diagnosis, enter a 1. If the service wasprovided for the secondary diagnosis, enter a g.
OX code
G I 1 IItem 29H Type of Service (MUST)
Enter the proper code to indicate the type of service provided. For example, if theresident is receiving a medical supply, enter "AE."
Type of service
HI AE I
Item 291 Procedure Code (MUST)
Enter the code for the procedure performed. In the previous example, the residentrequired a drainable pouch. You would enter:
Procedure Code
AS063
Item 29Jand 29K
Modifier (MUST, IF APPLICABLE)
If a modifier is associated with the procedure performed, enter the modifier in Item 29J.
Modifiers applicable to bilateral procedures are as follows:
RT - Right side of bodyLT - Left side of body50 - bilateral
If the procedure performed required a modifier, for example, procedure code 19200 mastectomy, and was performed to the right side of the body, enter:
Modifier
-21-
Item 29L Place of Service (MUST)
Enter the appropriate code to identify where the service was performed.
Refer to the Medical Assistance Program Fee Schedule for a complete list of modifiers.Any fee schedule update bulletins should also contain this information.
Nursing facilities will use the code 08 to indicate the service was provided in a nursingfacility.
Place of Ser.
L I 08 I
Item 29M Units of Service (MUST)
Enter the number of times the service was performed on the same or consecutive daysof service. For example, if the same service was provided on July 28 and 29, 1996,enter:
Units of Service
If the service was provided on JUly 29, 1996, only, enter:
Units of Service
M I 1
Item 29N Usual Charge (MUST)
Enter your usual charge to the self-paying public for the service(s) provided. Forexample, if your usual charge for one (1) office visit is $30.00, enter:
Usual Charge
N I 30.00
Item 290 Medicare Approved (MUST, IF APPLICABLE)
To ensure the proper use of the patient's Medicare resources, providers are required tobill Medicare first for procedures when they are provided to persons eligible for Medicare Part B.
If the Explanation of Medicare Benefits (EOMB) statement indicates the claim hascrossed over to Medical Assistance, the claim should appear on a remittance advicewith a remittance advice explanation code 747.
Enter the amount APPROVED by Medicare for the service provided. This informationcan be obtained from the Explanation of Medicare Benefits (EOMB). Enter the totalamount in dollars and cents. For example, if the total amount approved is $15.00,
If you are billing for multiple units of service, be sure to multiply your usual charge bythe number of units billed.
enter:MEDICARE approved
o I .15.00 I
-22-
A copy of the EOMB must be maintained on file.
Item 29P Other Insurance Paid (MUST, IF APPLICABLE)
Enter the portion of the bill that was paid by another insurance company. Also, maintain on file a copy of that company's Explanation of Benefits.
NOTE: MEDICAL ASSISTANCE IS CONSIDERED THE PAYOR OF LAST RESORT. ALLOTHER COVERAGE MUST BE EXHAUSTED BEFORE BILLING MA.
For example, if the patient's insurance company paid $40.00 for the service provided,enter:
Other Insurance Paid
p I 40.00
Item 290 Patient Pay (LEAVE BLANK)
The local County Assistance Office determines when recipients are responsible to paya portion of their medical expenses. This is "patient pay liability."
Nursing facility residents pay their patient pay toward their daily care. Therefore, thisfield should be left blank.
Patient Pay
QJ _
Items 30Athru 320
These items are available for additional services, and should be completed in themanner described in Items 29A through 290.
Items 33 through 43 of the Compensable Medical Services Section include Third Partybilling totals, attachments, and Prior Authorization/Place of Service Review information.
otal No. of Unes MEDICARE Deductible MEDICARE CcHnsurance Total Charges Total MEDICARE Total Other Insurance Paid Total Patient Pay
33 D 341 I 35 1 I 361 I 371 381 I 391 Io. of Allachments Allachment Type Allachment Type Prior AulhIPI. Ser. Rev. No. DPW Use DPW Use DPW Use
40
Item 33 Total Number of Lines (OPTIONAL)
Enter the number of claim lines completed. There can be a maximum of four (4) claimlines recorded on each invoice. For example, if one claim line is completed, enter:
Total No. of Lines
33 1~ 1 _
-23-
NOTE: DO NOT INCLUDE DELETED CLAIM LINES.
Item 34 Medicare Deductible (MUST, IF APPLICABLE)
If Medicare has been billed, enter the amount applied to the deductible in dollars andcents. For example, if $10.00 was applied to the Medicare deductible, enter:
MEDICARE Deductible
34 I 10.00
Item 35 Medicare Co-insurance (MUST, IF APPLICABLE)
If Medicare has been billed, enter the amount of the co-insurance reported by Medicarein dollars and cents. For example, if the Medicare co-insurance is $20.00, enter:
MEDICARE Co-insurance
35 I 20.00 I
Item 36 Total Charges (OPTIONAL)
Enter the sum of items 29N, 30N, 31 Nand 32N in dollars and cents. For example, ifthe sum of your usual charges for the services provided is $60.00, enter:
Total Charges
36 1L- 6_o_.o~0 _
Item 37 Total Medicare Approved (MUST, IF APPLICABLE)
Enter the total amount APPROVED by Medicare as taken from the EOMB (The sum of290,300,310 and 320). For example, if Medicare approved a total of $45.00 for theservices provided, enter:
Total MEDICARE Approved
37 I 45.00 I
Item 38 Total Other Insurance Paid (MUST, IF APPLICABLE)Enter the total amount received from insurance sources other than Medicare (the sumof 29P, 30P, 31 P and 32P). For example, if other insurance companies paid a total of$40.00 for the services provided, enter:
Total Other Insurances Paid
40.0038 I'------------
Item 39 Total Patient Pay (MUST IF APPLICABLE)
Enter the total amount paid by the patient, excluding copayments (the sum of 290,300, 310 and 320). For example, if the patient paid a total of $50.00 for the servicesprovided, enter:
Total Patient Pay
39 I 50.00'----------
-24-
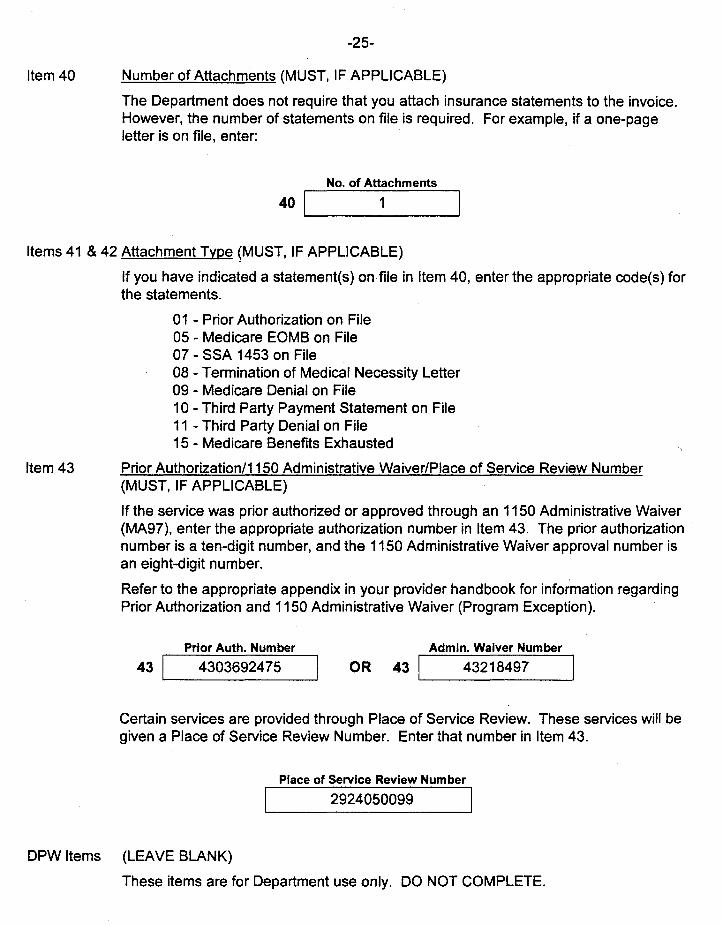
Item 40 Number of Attachments (MUST, IF APPLICABLE)
The Department does not require that you attach insurance statements to the invoice.However, the number of statements on file is required. For example, if a one-pageletter is on file, enter:
No. of Attachments
40 1 1__--'
Items 41 & 42 Attachment Type (MUST, IF APPLICABLE)
If you have indicated a statement(s) on file in Item 40, enter the appropriate code(s) forthe statements.
01 - Prior Authorization on File05 - Medicare EOMB on File07 - SSA 1453 on File08 - Termination of Medical Necessity Letter09 - Medicare Denial on File10 - Third Party Payment Statement on File11 - Third Party Denial on File15 - Medicare Benefits Exhausted
Item 43 Prior Authorization/1150 Administrative Waiver/Place of Service Review Number(MUST, IF APPLICABLE)
If the service was prior authorized or approved through an 1150 Administrative Waiver(MA97), enter the appropriate authorization number in Item 43. The prior authorizationnumber is a ten-digit number, and the 1150 Administrative Waiver approval number isan eight-digit number.
Refer to the appropriate appendix in your provider handbook for information regardingPrior Authorization and 1150 Administrative Waiver (Program Exception).
Prior Auth. Number
43 1__4_30_3_6_92_4_7_5_--, OR
Admin. Waiver Number
43IL--__43_2_1_84_9_7__
Certain services are provided through Place of Service Review. These services will begiven a Place of Service Review Number. Enter that number in Item 43.
Place of Service Review Number
2924050099 I
-25-
DPW Items (LEAVE BLANK)
These items are for Department use only. DO NOT COMPLETE.
Remarks and Signatures
The Remarks Section is for additional information relevant to the patient, provider or serviceprovided. Items 45 through 47 are for patient and provider signatures and for the invoice date. Theprovider providing the service is responsible for the correctness of the invoice even if a signaturestamp is used. Failure to complete Items 45 through 47 will result in immediate rejection of the invoice.
44A REMARKS: 448 Original Rejected CRN 44C RA Number I certify lhat the infcnnation shown on this invoice is true. correct and accurate. I under-
I I I Istand lhat payment and satisfaction of this claim will be from Federal and State funds.and lhat any false claims. statements. or documents. or concealment of material factsmay be prosecuted underapplicable Federal and Slate Laws. Invoice Date (mm dd yy)
45 461 IProvider's Sianature
47Recipient's Signature
Item 44A Remarks (MUST, IF APPLICABLE)
This section may be used if additional space is needed to explain unusual circumstances or conditions relative to services reported on the invoice or as required in anyother section of the handbook.
Item 45 Provider's Signature (MUST)
The provider rendering the service must sign the invoice. The signature certifies thatthe service has been provided in accordance with Medical Assistance regulations. Asignature stamp is acceptable if the provider authorizes its use and assumes responsibility for the information on the invoice.
NOTE: FOR MACHINE PRINTED CONTINUOUS FORM INVOICES OR MAGNETIC TAPEBILLING, A SIGNED MA 307, INVOICE TRANSMITTAL FORM, SHOULD BE SUBMITTED WITH EACH BATCH OF INVOICES OR TAPE.
Item 46 Invoice Date (MUST)
Enter the date the invoice is being submitted to the Department for processing. Use asix-digit format for all dates. For example, if the submission date is June 7, 1998,enter:
Invoice Date
46 I 060798
-26-
Item 47 Recipient Signature (MUST)
ALL INVOICES MUST HAVE EITHER THE RECIPIENTS SIGNATURE OR THEWORDS "SIGNATURE EXCEPTION" APPEARING IN THIS ITEM.
There are some situations in which the provider is not required to obtain the recipient'ssignature. Those situations are:
1. When billing for inpatient hospital, short procedure unit, nursing facilityand emergency room services provided by an independent physician.
2. When billing for services which are paid in part by another thirdparty, such as Medicare or Blue Cross.
3. WHen billing for services provided to a recipient who is unable to signbecause of a physical condition such as palsy.
4. When billing for services provided to a recipient who is physically absent,such as laboratory services, reading an X-ray or reading an EEG.
5. When resubmitting an invoice which was previously rejected.
6. When billing on computer generated (pinfed) invoices.
In all of the above situations, you must print the words "Signature Exception" on therecipient's signature line of the invoice.
An initial supply of invoices (MA 319) will be sent to each facility under separate cover. Additional invoices may be ordered from the Medical Assistance Provider Order Form (MA 300X).
If you would like to receive a copy of the Medical Assistance Fee Schedule, complete thename and address section of the attached Medical Assistance Literature Subscription Form (MA-109)and mail to the address listed on the bottom of the form. There is a $30.00 charge for the Fee Schedule.