Integrating Telehealth for Medically Fragile Patients Presented by: Robert Abel, RN, Chief Nursing Officer and Palliative Care Director Mia Millefoglie, Vice President Development & Marketing Heather Lomax, RN, Telehealth Coordinator
Transcript
Integrating Telehealth for Medically Fragile Patients
Presented by:
Robert Abel, RN, Chief Nursing Officer and Palliative Care Director
Mia Millefoglie, Vice President Development & Marketing
Heather Lomax, RN, Telehealth Coordinator
In this session, participants will be able to:
1) Identify the tools of Telehealth Technology and its application to specific disease
groups
2) Discuss the effectiveness of Telehealth identifying financial, quality and patient
adherence measures
3) Articulate strategies for sustainability, collaboration with healthcare providers
and patient engagement
3
Learning Objectives
4
A Glimpse Into
the History of Visiting Nurses
In 2014, HHVN touched the lives of
more than 16,000 children, adults and
elders.
HomeHealth Visiting Nurses (HHVN) is a
fully licensed not-for-profit organization
caring for patients of all ages. As the leading
provider of home health care in southern
Maine, we provide nursing, physical therapy,
occupational therapy, speech therapy, home
health aide, and counseling services to
patients in the comfort of homes. Services
available 24/7 throughout York, Cumberland
and southern Oxford Counties.
5
HomeHealth Visiting Nurses - at a glance
6
Strategies for Sustainability
2001-2003
Demo RUS Telehealth (8 units) & Point of Service
2002 -Telehealth expansion – Polycom & POS
2004-2006
Telehealth Expansion, broader service area and expanded disease groups
POS upgrade to Lifebooks
RUS funds & Foundations
2007-2012
RMCL collaborative group/ Transition to monitoring units/ focus on CHF & COPD
RUS Funds &
Foundation support
2012 - 2014
Vendor buyout
Expansion
Integration with system IV Diuretic Protocol
1st insurance contract
Secured 2014 RUS
Secured shared savings grant
Equipment Failure
Expedited vendor search
New vendor Selection
2015-2014
Secured tablets with video capacity/
Deployed 100 units in 1st qtr.
Submitted 2015 RUS grant
Secured system match
Convened task force for private carriers
Expanding to pediatrics
EMC HL7 interface
Funded through RUS-USDA with CHF focus in rural areas
Challenges
Lack of clinician buy in
Lack of physician buy in
Small scale project
Not integrated into clinical practice
Successes
76.5% reduction in overall hospital admissions compared to CHF non-telehealth group
80% of patients noted high satisfaction
Actual savings per visit - $21.21 realized by time, travel and mileage efficiencies
7
Telehealth Demonstration Project 2001
Secured second RUS-USDA Funds & foundation support for expansion to include
CHF, COPD, Wound & Diabetes
Challenges:
Partnership failure
Continued difficulties with clinical buy in
Management leadership changes due to agency merger
Third party reimbursement still pending
Only 10% admission rate from screened referral
Successes:
Reduction in the cost per episode
High levels of patient satisfaction
Improved quality outcomes
Reduction in hospitalization rate
8
Telehealth Expansion 2003
Challenges
Meeting demand – constant wait list
Older equipment
Reimbursement barriers
Vendor sunset of equipment
Expedited vendor search
Successes
Successful transition to new vendor
Secured clinical and physician buy-in
Established data collection and reporting
Consistent and significant reduction in hospitalization rates
Consistent high levels of patient satisfaction
Improvement in key quality scores
9
Telehealth Monitoring Program 2011- 2014
10
2014 - 2017 Telehealth Aims:
1) To expand access to care and improve quality measures for elders with at-risk
chronic diseases by deploying enhanced telehealth technology
2) To expand access to care and improve quality measures for medically fragile
children copying with the challenges of chronic disease or serious illness by
introducing new pediatric telehealth modules and peripheral devices
3) To standardize protocols and integrate delivery of services on a system level
4) To improve coordination of care and communication with healthcare providers
by securing an HL7 interface between EPIC and telehealth provider
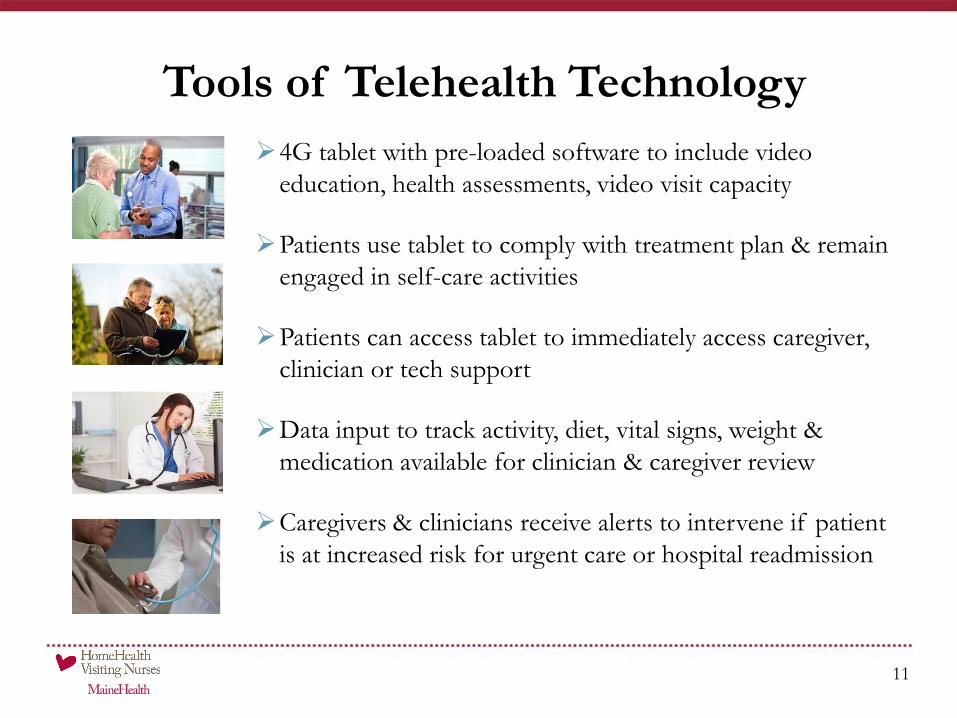
4G tablet with pre-loaded software to include video
education, health assessments, video visit capacity
Patients use tablet to comply with treatment plan & remain
engaged in self-care activities
Patients can access tablet to immediately access caregiver,
clinician or tech support
Data input to track activity, diet, vital signs, weight &
medication available for clinician & caregiver review
Caregivers & clinicians receive alerts to intervene if patient
is at increased risk for urgent care or hospital readmission
11
Tools of Telehealth Technology
Provides real-time patient data post-
discharge
Algorithms highlight which patients are
at an increased risk of readmission
12
Platform leverages caregivers and family
members in the formal discharge process
Empowers patients to change the way
they behave and view their medical
condition
13
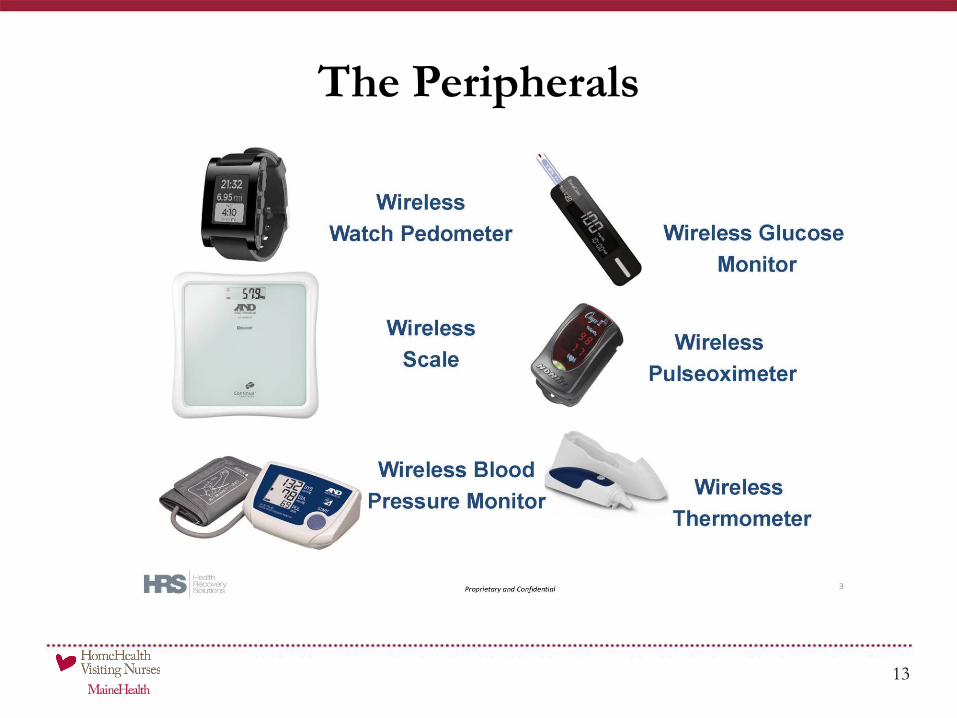
The Peripherals
Population and patient level data
Reports, alerts, team care collaboration
Customizable to fit client needs
14
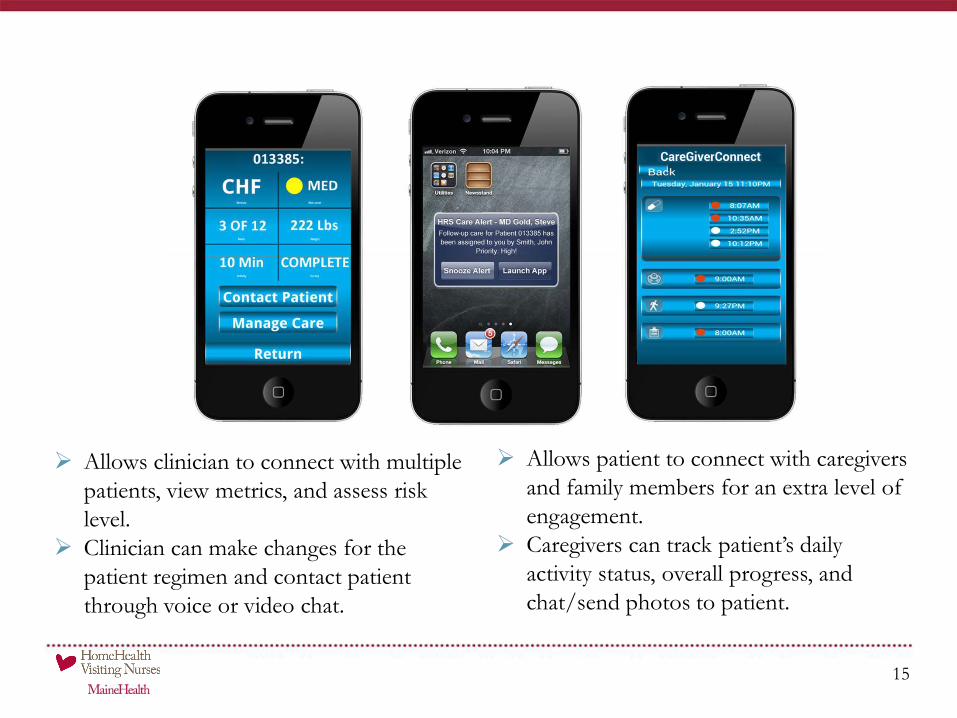
Allows clinician to connect with multiple
patients, view metrics, and assess risk
level.
Clinician can make changes for the
patient regimen and contact patient
through voice or video chat.
15
Allows patient to connect with caregivers
and family members for an extra level of
engagement.
Caregivers can track patient’s daily
activity status, overall progress, and
chat/send photos to patient.
Referrals received from system healthcare providers
Population Focus: Congestive Heart Failure, Chronic Obstructive Pulmonary
Disease, Cardiac Surgery, and Diabetes
HHVN Telehealth Team reviews medical record and assesses for Telehealth
admission
Home Diuretic Protocol assessment:
Frequent re-admissions for volume overload
Failed up-titrations of home diuretics
Stable renal function
Home weights correlate to volume overload
Patient demonstrates compliance
16
Telehealth Delivery of Care Model
Telehealth Assistant
Coordinates installation and teaching
Reviews equipment use, services, contact procedures, and monitoring
protocols
Re-visit patients for additional education and/or equipment retrieval