Inter-professional practice in health care David Patrick Ryan, Ph.D. Director of Education & Knowledge Processes, Director of Education & Knowledge Processes, Regional Geriatric Program of Toronto Regional Geriatric Program of Toronto Assistant Professor, Faculty of Medicine, University Assistant Professor, Faculty of Medicine, University of Toronto of Toronto
Transcript
Inter-professional practice in health care
David Patrick Ryan, Ph.D.
Director of Education & Knowledge Processes, Regional Geriatric Director of Education & Knowledge Processes, Regional Geriatric Program of TorontoProgram of Toronto
Assistant Professor, Faculty of Medicine, University of TorontoAssistant Professor, Faculty of Medicine, University of Toronto
What is an interprofessional team?
• People from several professions • Each trained to use different tools and concepts• Whose labor organized around a common problem• With continuous communication and frequent reflection
on both the groups work and its process• Usually with group responsibility for the final product
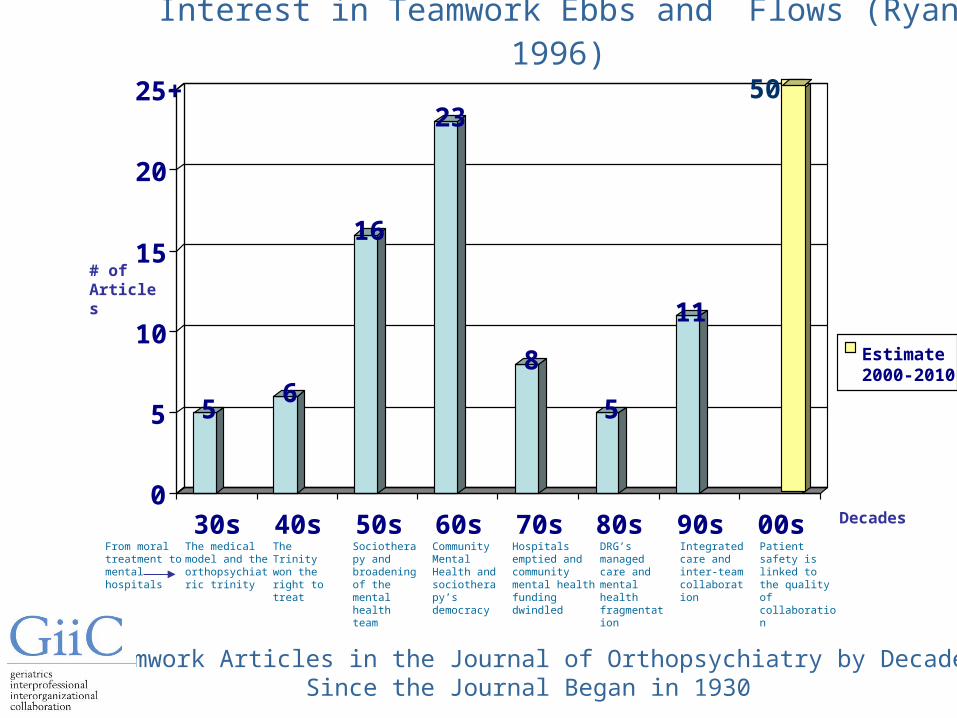
Interest in Teamwork Ebbs and Flows (Ryan 1996)
From moral treatment to mental hospitals
The medical model and the orthopsychiatric trinity
The Trinity won the right to treat
Sociotherapy and broadening of the mental health team
Community Mental Health and sociotherapy’s democracy
Hospitals emptied and community mental health funding dwindled
DRG’s managed care and mental health fragmentation
Integrated care and inter-team collaboration
# of Articles
Decades
Patient safety is linked to the quality of collaboration
56
16
23
8
5
11
50
0
5
10
15
20
25+
30s 40s 50s 60s 70s 80s 90s 00s
Estimate 2000-2010
Teamwork Articles in the Journal of Orthopsychiatry by Decade Since the Journal Began in 1930
Chronic Disease and FrailtyPatient SafetySuccess of Quality Improvement The Quality of Working LifeLocal Health Integration Networks HealthForce Ontario’s Inter-Professional Care Blueprint for Action Primary Care and Family Health Teams
Why Interprofessional Practice? Why Now?
Province-Wide investment in Inter-Professional Education
Inter-professional Mentoring
Inter-professional Coaching
Inter-professional Preceptorships
Inter-professional prevention of delirium in the ED
Impact inter-professional practice within primary care groups
Inter-Professional Practice and Hospital/LTC accreditation
The Journal of Inter-Professional Care
GiiC – the geriatrics, inter-professional practice & inter-organizational collaboration initiative for family health teams and community health centers
Current Initiatives in Interprofessional Care
Barriers to interprofessional teamwork: practice based issues
• There is a lack of preparation for interdisciplinary hostility . . . If the practice of this specialized form of aggression is to be placed on a higher level, at least as high as professional wrestling…the subtle arts of patronage, insult and innuendo must be taught. Brody & Weithorn, 1965
• Unrealistic expectations, lack of knowledge and perceived threats to autonomy Fried & Leatt, 1986
• Professional jealousies and role boundary issues Strasser et al 1994
• We practice together but we train apart
Barriers to teamwork: professions think differently (from Qualls and Czirr, 1988)
Logic of assessment: from ruling out to ruling in
Focus of efforts: from acute episodes to quality of life
Locus of Responsibility: from executive to collaborative
Pace of Action
Focus of attention: from task to process
Interprofessional stereotypes
Decision making expectations: from executive to consensus
Beliefs about professional independence: from autonomy to interdependence
Barriers to teamwork: Though we practice together until recently we trained apart (from Cleary & Howell, 2003)
A framework for examining teamwork
DecisionsAuthorityAccount-
bility
Roles &Inter-
dependence
Communication&
ConflictManagement
Team Member Skills &
Strengths
Clarity/Coherence
of Goals
PerceivedSupport fromOrganization
THE DIMENSIONS OF TEAMWORK
OU
TC
OM
ES
OF
T
EA
MW
OR
K
CustomerNeeds &Interteam
Issues
CustomerFocused
Outcomes
InternalFocused
Outcomes
FinancialFocused
Outcomes
InnovationFocused Outcomes
Ad hoc Inter-agency Shared Care Teams
Acute Care Teams
Continuing care and Rehabilitation teams
Specialized Geriatric Services Teams
Management Teams
TYPES OF TEAMS
Primary Care Teams
History of Teamwork in Health Care The Original Team - Romantic Era (circa 1900)
General Practitioner
History of Teamwork in Health Care Classic Sequential Teamwork and the Specialist Era
(circa 1920)
Specialist Specialist
Nurse Nurse
History of Teamwork in Health Care Sequential Multi-Professional Practice Teams
(circa 1930)
Specialist
Nurse
PsychologySocialWork
Rehab
History of Teamwork in Health Care Dynamic Multi-Professional Team (circa 1960)
from a cadre of professionals
Physician
Nutrition
Psychology
Physio
Nurse Social Work
SLP
OT
Pharmacy
Dentist Recreation
History of Teamwork in Health Care Dynamic Multi-Professional Team (circa 1960)
a team is convened around the needs of a particular patient
Physician
Social WorkNurse
Psychology
OT
SLP
History of Teamwork in Health Care Dynamic Inter-Professional Team (circa 1985)
from a cadre of professionals
Physician
Nutrition
Psychology
Physio
Nurse Social Work
SLP
OT
Pharmacy
Dentist Recreation
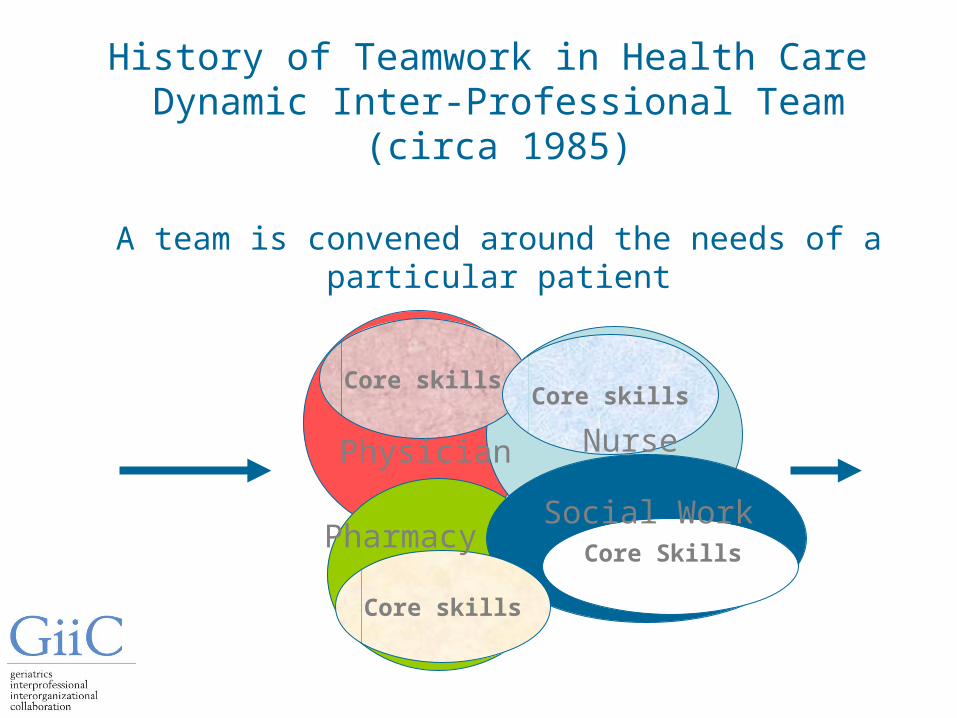
History of Teamwork in Health Care Dynamic Inter-Professional Team (circa 1985)
A team is convened around the needs of a particular patient
Core skillsCore skills
Core Skills
Core skills
Social Work
Physician
Pharmacy
Nurse
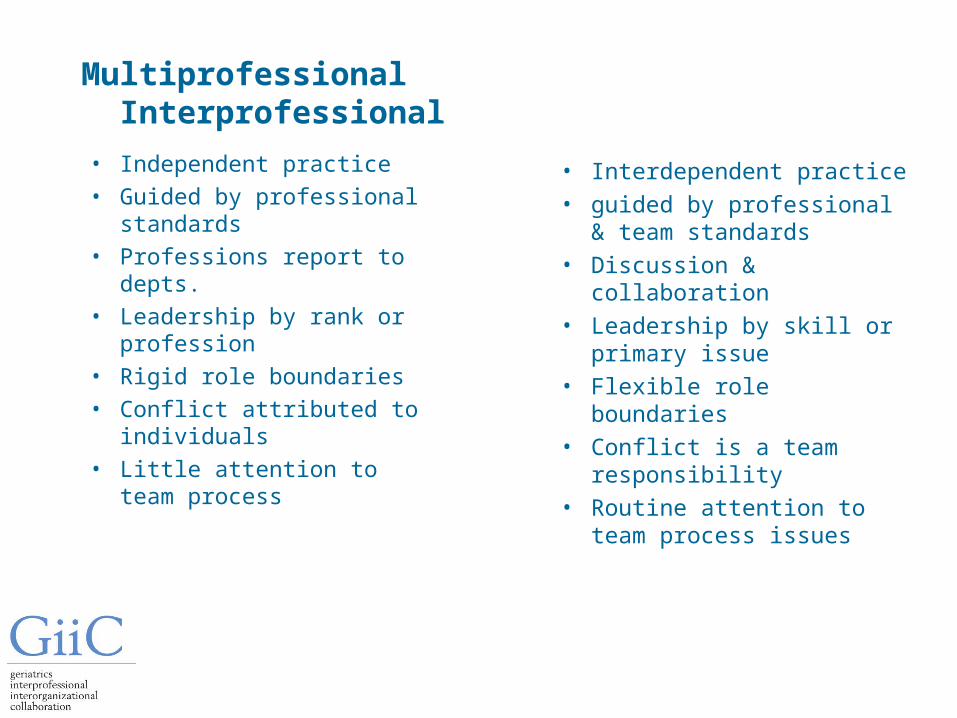
Multiprofessional Interprofessional
• Independent practice• Guided by professional
standards• Professions report to
depts.• Leadership by rank or
profession• Rigid role boundaries• Conflict attributed to
individuals• Little attention to team
process
• Interdependent practice• guided by professional &
team standards• Discussion &
collaboration• Leadership by skill or
primary issue• Flexible role boundaries• Conflict is a team
responsibility• Routine attention to team
process issues
Myths about Teamwork
• There are no leaders on teams; everyone is equal• If we just work together, we will eventually become a
high performance team• Everyone is accountable for everything on teams• Teams take a long time to get up and running• All team decisions must be made by consensus• Conflict must be worked out for a team to be productive• On the best teams, everyone likes everyone else• The most important work takes place in team meetings• Confrontation means conflict
Just putting people together to work in teams doesn’t
necessarily produce effective interprofessional teamwork
Some of the things a team can do to maximize performance
Develop expertise to facilitate interprofessional practice
Annually monitor and reflect on team culture
Balance attention to task and process functions
Develop clear goals and monitor outcomes
Understand the dynamic nature of team development
Recruit or develop the right mix of skills
Value professional and personal diversity
The Dimensions of Teamwork Annual Survey
• Customer and inter-team issues
• Team member strengths and skills
• Communication and conflict management
• Roles and interdependence
• Clarity of team goals
• Decision-making and leadership
• Perceived organizational support
Quarterly review of informal team role performance
Leaders joke to soften control Member joke about the team and about patients
Stage 2: Storming
The leader tries to convince the team.
Team members resist.
Scapegoating is evident Clowning reduces
tension
Conflict emerge often in response to minor issues which take on broader symbolic meanings.
Humour is often barbed and personal, interspersed with the clowns buffoonery.
Stage 3: Norming
Leadership exercised by coalitions of members based on Perceptions of competence
Members are colleagues who are able to defer to a each other’s relevant experience.
Members provide mutual support . Parties express solidarity. Team symbols emerge
Sharing of team deprecating humor. Self-disparaging jokes. In-jokes emphasize membership
Stage 4: Performing
Authority exercised by a coalitions depending on skills and emergent needs
Members find opportunities for interdependence and resist earlier activities such as scapegoat and clowning
Members have pride in the teams accomplishments. Team meetings become constructive and enjoyable. Team legends emerge and team anniversaries celebrated.
The team laughs at itself but explains its in-jokes to new or non-members. It enjoys it's own funny stories and myths. Humour typically at the expense of the team but without loss of task orientation.
Routinely reflect on the stage of team development
Value one another's diverse personal styles
I stay cool, calm and collected and tend to keep my thoughts and feelings to myself
I get pretty excited and energetic and tend to let my thoughts and feelings show
C 4 3 2 1 0 1 2 3 4 E
I get into new things quickly, make up my mind fast and hate to wait.
When new things come I prefer to wait, watch, ask questions and hear all sides before reacting
J 4 3 2 1 0 1 2 3 4 S
Use the ratings to plot your place on the “So Simple” grid. The results can be amusing even insightful. Remember we are not rating whether someone is good or bad. We are trying to better understand difference.
C 4 3 2 1 0 1 2 3 4 E
J4
3
2
1
1
2
3
4
S
DRIVERS prefer to move ahead calmly, watching results, staying organized and asking “what’s next”
ENTHUSIASTS like to jump into new things, sets everyone on fire by “just doing it” and asking “Why not?”.
ANALYSTS like to hear the details, see facts and figures and asks “How is this going to work?”
HARMONISTS like to give everyone the opportunity to express themselves and their opinions often asking “how is everyone feeling?”
Stay cool calm and collected
Let feelings and emotions show
React quickly and hate to wait
Wait, watch, hear all sides
Value one another's diverse personal styles
To summarize
It has taken us more than 100 years to get to this point of recognizing interprofessional interdependence
The provincial interprofessional care blueprint is removing barriers
Frailty and chronic disease demand high quality interprofessional practice
Effective teamwork doesn’t just happen it needs ongoing care and tending
Teamwork can enhanced by a few strategic interventions
GiiC provide family health teams and community health centres with several useful tools
GiiC has embedded interprofessional thinking within each geriatric topic
GiiC provides a consultant to help you to facilitate your team