15
Internal Medicine 2015 Highlights Ryan D. Mire, MD, FACP
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | nicholas-leonard |
| View: | 217 times |
| Download: | 4 times |
Internal Medicine 2015 HighlightsRyan D. Mire, MD, FACP
2
Assessing and Managing Testosterone Abnormalities in All Your Patients (MTP 022) - Dr. Matsumoto
Most reliable testosterone level is early morning (~ 8 am) and fasting.• Should be repeated x 1 to confirm low level
Biologic variability ~30% fluctuation day to day
Requires BOTH symptoms and low level to meet diagnosisModerate obesity decreases SHBG• Check SHBG and free testosterone levels in obese • Other factors: steroids, hypothyroidism, and nephrotic syndromeFemales: with PCOS and hirsuitism, testosterone levels are not required.
3
Evaluation and Management of Kidney Stones (MTP 077) – Dr. Curhan
20% men / 9% women will have a kidney stone in lifetime.Accounts for $2 billion / year in US healthcare expenditures
Wait 6 weeks prior to 24 hour urine for metabolic work-upDietary calcium associated with decreased risk of stones, but calcium supplements can increase risk.
Calcium oxalate stones (70%) - do not advise a low calcium diet!
First time stone does not require metabolic workupRenal U/S is adequate for follow-up/surveillance of stones
4
Lung Cancer Screening (PN 035) – Drs. Kane, Nana-Sinkam, and Redberg
Using LDCT for screening, ~ 25% will have nodules and ~ 10% of nodules will be cancerousLDCT is ~ ¼ of the radiation exposure of standard CT
The most impactful intervention in the past 10 year to affect a disease of high mortality
Despite patient inclusion guidelines by USPSTF, risk stratification is essential for best screening outcome.• PLCOm2012 model (risk calculator) > USPSTF
factors: ethnicity, SES, BMI, Ca hx, COPD, FHx of cancer• http://www.brocku.ca/lung-cancer-risk-calculator
5
Lung Cancer Screening (PN 035) – Drs. Kane, Nana-Sinkam, and Redberg
Smoking cessation is much less expensive than LDCT annual screening!!!• Remains the #1 impact on lung cancer incidence
6
Clinical Triad: The Experts Weigh in on Obesity (CT 001) – Drs. Cody-Stanford, Schirmer, and Puri
Laparoscopic sleeve gastrectomy is now the most common U.S. surgery (~45% of all surgeries)Mortality is 30% greater for every 5 point in BMI above 25 (independent of age)Indications for bariatric surgery:
Failed lifestyle efforts (minimum of 6 months)BMI > 35 with co-morbidities or BMI > 40 Psychiatrically stable
Monitor for nutritional deficiencies:- iron, vitamin B12, folate, and vitamin D
7
Clinical Triad: Immunizations in Adults, Travelers, and Healthcare Workers (CT 003) – Drs. Schaffner, Freedman, and Talbot
Lifetime risk of shingles is ~ 33% and with age No need to have a hx of chicken pox or to do a
varicella titer – just give the vaccineShingles vaccine is license for 50 y.o. and older, but proven benefit only last ~ 10 years and only a 1 time vaccine, so optimal to wait until age 60New recommendation for pneumococcal conjugate vaccine (PCV13) in patients > 65 (as of August 2014)
8
Clinical Triad: Immunizations in Adults, Travelers, and Healthcare Workers (CT 003) – Drs. Schaffner, Freedman, and Talbot
• No pneumococcal vaccine:- PCV13 first, followed by PPSV23 one year
later*Can be practically be given 8 weeks
later, but CMS will only reimburse if given one year apart
• If PPSV23 has been given:- Wait at least one year before PCV13 is
given.
9
Clinical Triad: Hypertension – Devices, Drugs, and Diet (CT 004) – Drs. Cohen, Nesbitt, and Taler
White coat hypertension occurs in ~ 20% with untreated hypertensionAt night, BP should drop ~ 15%. However, higher rate of CV events when nighttime BP is elevated.
- compared to self monitoring, ambulatory BP monitoring provides data during sleep hours
For persistent proteinuria, add aldosterone antagonistEvidence does not support renin-angiotensin-aldosterone system (RAAS) blockade
10
Providing High Value in Cardiology Care (MTP 004) – Dr. Merz
In 2012, the NHLBI removed themselves from the guideline business. In August of 2013, the ACC/AHA took overNew and lower threshold for the ASCVD 10 year risk calculation cutoff from 10% down to 7.5%!No longer treat to targeted LDL levels
- use moderate (30-50%) / high (> 50%) intensity statins
African American ethnicity factors in risk calculationRoutine LFT checks no longer recommended
11
Lipid Management 2015: What Works, What Doesn’t (MTP 009) – Dr. Duffy
Algorithm for risk score calculator is very driven by age controversy for overestimation in healthy pts ASCVD patients (secondary prevention)
< 75 years old – use high intensity statin Atorvastatin 40-80mg dose / Rosuvastatin 20 - 40mg dose
> 75 years old – use moderate intensity statinRisk calculator is class IIb recommendation for other ethnic populations (e.g. Hispanics, American-Indians)Clinical judgment must always prevail the decision to initiate any treatment
12
Clinical Triad: Anticoagulants Update (CT 002) – Drs. Deo, Ma, and Zumberg
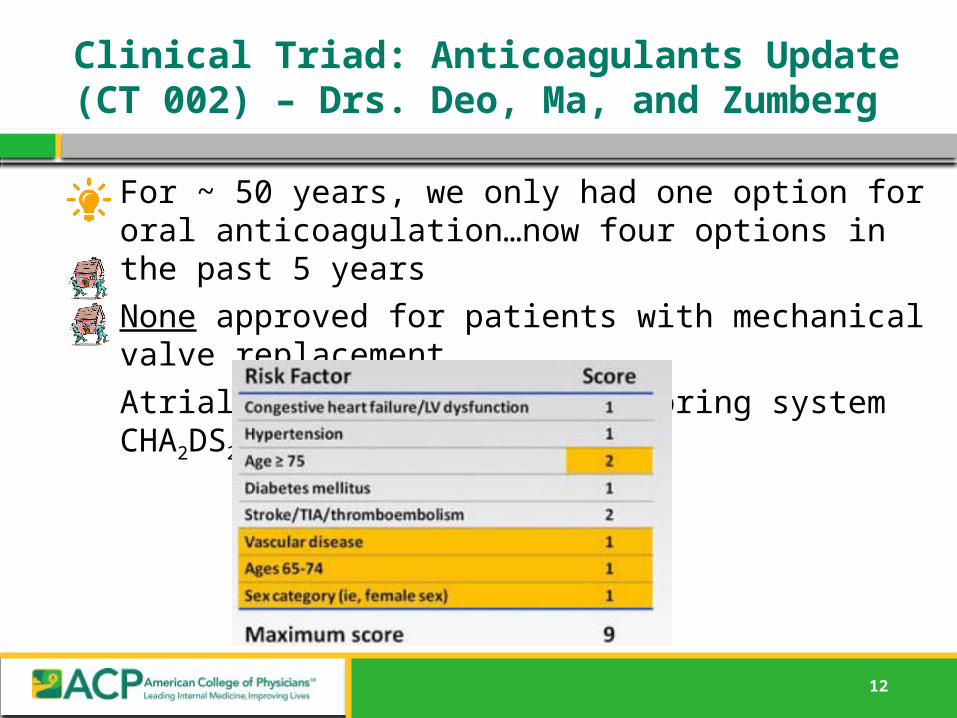
For ~ 50 years, we only had one option for oral anticoagulation…now four options in the past 5 yearsNone approved for patients with mechanical valve replacementAtrial fibrillation – new scoring system CHA2DS2VASc
13
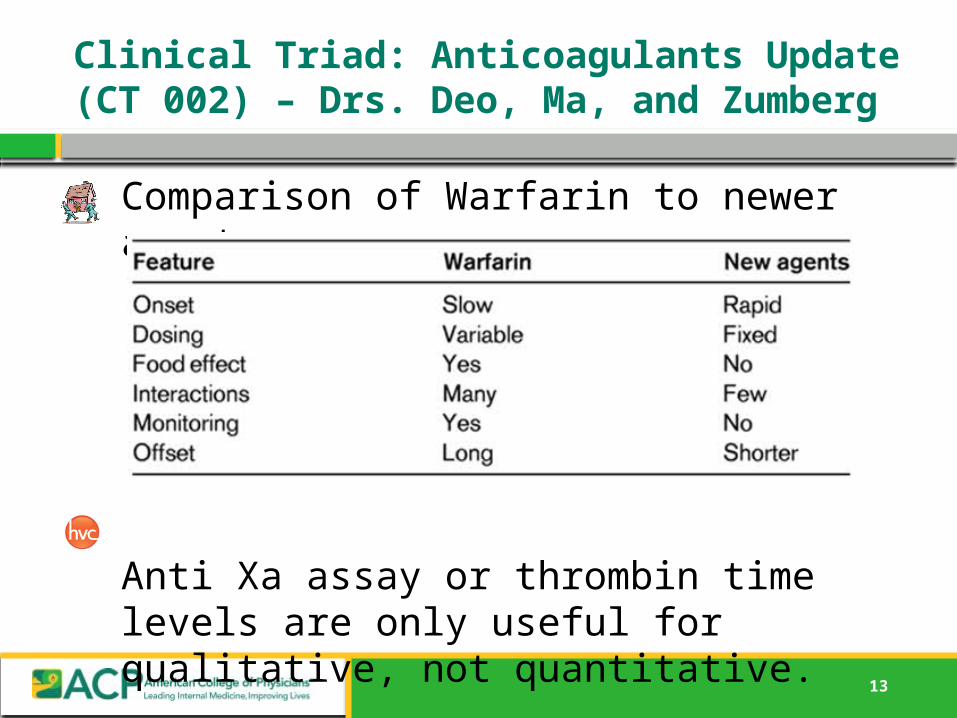
Clinical Triad: Anticoagulants Update (CT 002) – Drs. Deo, Ma, and Zumberg
Comparison of Warfarin to newer agents
Anti Xa assay or thrombin time levels are only useful for qualitative, not quantitative.
14
Headache Evaluation and Management (MTP 079) – Dr. Loder
Aura occurs in ~ 30% of migrainesFocal neurologic symptom: visual, sensory, or
motorAvoid recommendation for prolonged or frequent use of OTC analgesics even for mild headachesTriptan non-responders…suboptimal management???
dose too low?
did not treat early enough?suboptimal formulation?
Avoid neuroimaging in stable pattern headaches that meet criteria for migraines
- Head MRI is the imaging of choice (exceptions: ER, SAH)
15
Thyroid Management (PN 013) – Drs. Wartofsky, Cooper, and Gharib
95% of thyroid nodules are benignWhen should be biopsy?
Nodules 1 cm with high suspicion sonographic pattern
Nodules 1 cm with intermediate suspicion US pattern
Nodules 1.5 cm with low suspicion US pattern
Nodules 2 cm with very low suspicion US pattern
20% of thyroid FNA pathology are indeterminate•25% of those are malignant after surgical diagnostic thyroid lobectomy•Molecular genetics to decrease number of unnecessary surgeries
Cytologically benign nodules can be followed at 1 year and then at 5 years

















