ofatt, ~pa[ lig. .~rential thena ~tion sly atione( er thin ’ere ounger ~ei ,,:yn- d prob- ml liga- llowing ,~rature. iscrimi- :locities his pre- nptoms ; testing anation is more ity sys- 1. and re- t to pa- ,’ome in l, nerve .pparent ¯ ve. 1 .nel syn- e median :.ansplan ~ ~5-8. gJ. ~f autoso- tterature. dhood. J ood. Dev Intraneurai Topography of the Ulnar Nerve in the Cubital Tunnel Facilitates AnteriorTransposition Greg P. Watchmaker, MD, Gilbert Lee, MD, Susan F. Mackinnon, MD, St. Louis, MO The surgical management of cubital tunnel syndrome includes anterior transposition of the ulnar nerve. The success of all transposition procedures is dependent on placementof the nerve anterior to the medialepicondyle without tension. Fifteen cadaveric upper extremities underwent anterior transposition followed by anterior transposition with separation of the most proximal motorbranches from the mainulnar nerve for a distance of 1, 2, and 3 cm. Proximal dissection of these motorbranches achieved an average gain in distance from the epicondyleof 71%, with an average distance from the epicondyleof 3.6 cm. The intraneural topography of the ulnar nerve was studied in five additional cases. Cross-section analysis of the fascicular anatomy at 333 Ixmintervals along the length of the nerve with longitudinal reconstructions confirmed a safe dissection plane without interfascicular plexus formation. The most proximal motor branch in the forearm could be traced proximally an average of 6.7. cm within the nerve before interfascicular mingling occurred(range 6.0 to 7.5 cm). Thus, 6.0 cm represented the upper limit of safe proximal dissection in these nerves. Proximal separation may be performed without disruption of interfascicular plexus connections and will facilitate anterior transposition. (J Hand Surg1994; 19A:915-922.) Many surgical techniques have been described for the management of cubital tunnel syndrome. Suc- cessful treatment by transposition requires not only a complete release at all points of compression, but .,. also prevention of recurrent compression in its new position. Leaving the transposed nerve close pi-oximity to the medial epicondyle subjects the nerve to injury from direct trauma as well as injury if it becomes tethered to adjacent or fibrous tissue. Posterior motor branches tend to tether or pull the nerve posteriorly and limit : From Washington University Medical Center and Barnes Hos- pital, St. Louis, MO. - Received for publication Aug. 13, 1993; accepted in revised Oct. 29, 1993. No benefits in any form have been received or will be received from a commercialparty related directly or indirectly to the sub- ject of this article. Reprint requests: Susan Mackinnon, Division of Plastic Sur- gery, Washington University School of Medicine, One Barnes Hospital Suite 17424, St. Louis, MO 63110. This study was designed to answer whether sepa- ration of these motor branches is topographically feasible, and if so to what extent this maneu~-er would facilitate anterior transposition of the ulnar nerve. Materials and Methods Transposition Measurements Transposition distances were evaluated in 15 ulnar nerves. Fifteen nonfixed cadaveric upper ex- tremities disarticulated at the shoulder w-ere ob- tained for analysis. With the elbow in 30 ° flexion, standard skin incisions were used to expose the ulnar nerve for anterior transposition procedures. The nerve was exposed from 5 cmproximal to the level of the medial epicondyle to 5 cm distal to the medial epicondyle. A 5-0 silk suture placed on the nerve at the level of the medial epicondyle was des- ignated the 0 cm mark. Points distal to this suture were given positive values; points proximal were TheJournal of Hand Surgery915
Intraneurai Topography of the UlnarNerve in the Cubital Tunnel
Facilitates Anterior Transposition
Greg P. Watchmaker, MD, Gilbert Lee, MD, Susan F. Mackinnon, MD,
St. Louis, MO
The surgical management of cubital tunnel syndrome includes anterior transposition of theulnar nerve. The success of all transposition procedures is dependent on placement of thenerve anterior to the medial epicondyle without tension. Fifteen cadaveric upper extremitiesunderwent anterior transposition followed by anterior transposition with separation of themost proximal motor branches from the main ulnar nerve for a distance of 1, 2, and 3 cm.Proximal dissection of these motor branches achieved an average gain in distance from theepicondyle of 71%, with an average distance from the epicondyle of 3.6 cm. The intraneuraltopography of the ulnar nerve was studied in five additional cases. Cross-section analysis ofthe fascicular anatomy at 333 Ixm intervals along the length of the nerve with longitudinalreconstructions confirmed a safe dissection plane without interfascicular plexus formation.The most proximal motor branch in the forearm could be traced proximally an average of6.7. cm within the nerve before interfascicular mingling occurred (range 6.0 to 7.5 cm). Thus,6.0 cm represented the upper limit of safe proximal dissection in these nerves. Proximalseparation may be performed without disruption of interfascicular plexus connections andwill facilitate anterior transposition. (J Hand Surg 1994; 19A:915-922.)
Many surgical techniques have been described forthe management of cubital tunnel syndrome. Suc-cessful treatment by transposition requires not onlya complete release at all points of compression, but
.,. also prevention of recurrent compression in its newposition. Leaving the transposed nerve
close pi-oximity to the medial epicondyle subjectsthe nerve to injury from direct trauma as well as
injury if it becomes tethered to adjacentor fibrous tissue. Posterior motor branches
tend to tether or pull the nerve posteriorly and limit
: From Washington University Medical Center and Barnes Hos-pital, St. Louis, MO.- Received for publication Aug. 13, 1993; accepted in revised
Oct. 29, 1993.No benefits in any form have been received or will be received
from a commercial party related directly or indirectly to the sub-ject of this article.
Reprint requests: Susan Mackinnon, Division of Plastic Sur-gery, Washington University School of Medicine, One BarnesHospital Suite 17424, St. Louis, MO 63110.
This study was designed to answer whether sepa-ration of these motor branches is topographicallyfeasible, and if so to what extent this maneu~-erwould facilitate anterior transposition of the ulnarnerve.
Materials and Methods
Transposition Measurements
Transposition distances were evaluated in 15ulnar nerves. Fifteen nonfixed cadaveric upper ex-tremities disarticulated at the shoulder w-ere ob-tained for analysis. With the elbow in 30° flexion,standard skin incisions were used to expose theulnar nerve for anterior transposition procedures.The nerve was exposed from 5 cmproximal to thelevel of the medial epicondyle to 5 cm distal to themedial epicondyle. A 5-0 silk suture placed on thenerve at the level of the medial epicondyle was des-ignated the 0 cm mark. Points distal to this suturewere given positive values; points proximal were
The Journal of Hand Surgery 915
916 Watchmaker et al. / Anterior Transposition of the Ulnar Nerve
BRANCHING PATTERN OF ULNARNERVE AT THE ELBOW
I cm...E~;.U ..........................................................................................................................................I .......................i .........................
FF FC F CO
FCU,,’FDP
ULNAR RADIAL
Figure 1. The branching pattern for each ulnar nerve is demonstrated. The medial epicondyle is designated 0 cm.ity in number and level of branching between specimens is present.
given negative values. Sutures were then placed atmeasured intervals proximally and distally.
A reference suture was also placed on the medialepicondyle. Branches to the flexor carpi ulnaris(FCU) and flexor digitorum profundus (FDP) identified as to their number and distance distal tothe epicondyle (Fig. 1). The nerve was then releasedfrom its bed and transposed anteriorly. A small ar-ticular branch was found in two specimens. Thisbranch was sacrificed. The distance was thenrecorded from the nerve’s original untransposed bedto its new position. This transposition distance wasrecorded at the level Of the medial epicondyle andals0 at 1, 2, 3, and 4 cm proximal and distal to theepicondyle. Distances were also measured from theepicondyle to the transposed nerve.
After these measurements were recorded, a care-ful separation of the proximal motor branches fromthe main ulnar nerve was performed. The most prox-imal motor branch in the forearm was always thebranch that tethered the ulnar nerve to the epicon-dyle. Using microsurgical instruments, this branchwas separated under 2.5 x loupe magnification fromthe other ulnar nerve fascicles for a distance of 1cm. The plane of dissection was the epineurium be-tween the main ulnar nerve and the motor branches.If two branches exited the nerve at the same level,both branches were dissected free as a group. Fol-lowing this maneuver, the nerve was then trans-
posed again and measurements were taken.process was repeated again after 2 and 3 cmsection. After each centimeter of sel:gain in transposition was recorded. A totalmeasurements were thus taken on eachall measurements were completed, eachbranch was traced distally to confirm whichor muscles it innervated.
A frequent observation was a motoring from the medial aspect of the nervecrossed anteriorly and laterally to ~FCU (Fig. 2A). On occasion, thisarising with a branch traveling medially, als~nervating the FCU (Fig:" 2B). When thiswas present, adequate transposition couldobtained by separating these two breach other (Fig. 2C).
Topographic Analysis
Cross-sectional topographic study wason five ulnar nerves in the region of the elbow.nonfixed cadaveric upper extremities were
for dissection. The ulnar nerve and itswere dissected along a distance from 8 cmto the medial epicondyle to 8 cm distal with the)of loupe magnification. The level at which
branch left the ulnar nerve was measured inters. The medial epicondyle was designated 0
The Journal of Hand Surgery / Vol. 19A No. 6 November 1994 917
A
PROXIMAL
FCU
EP1CONDYLE.~,,,.~.~ DISTAL
B
FCU
FCU
PROXIMAL DISTAL
FCU
(A) The ulnar nerve often contained a motor branch that crossed from medial to lateral over the nerve. (B) vet: nerves, the proximal branch bifurcated to travel both medially and laterally to innervate separate fibers of the
FCU. tC) Separation of these branches from one another was necessary to achieve adequate transposition.
Ten-micron-thick sections were cut every 333 ~m. The dark fibers of the orienting suture are visible near the
composing the proximal motor branch to the FCU is on the far right. A well-defined layer of epineurial
exists between this fascicle and the main ulnar nerve fascicles at this level.
918
with proximal points given negative values and dis-tal points given positive values. 6-0 silk orientationsutures were passed along the length of nervethrough the epineurium. Nerves were labeled, pho-tographed, fixed in formalin, and processed en bloc.The nerves were then cut into 3 cm segments andembedded into paraffin cylinders for microtome sec-tioning.
Each block of nerve tissue was cut into sections10 ~xm thick. A section of tissue was saved every333 ~xm, and three such sections were mounted ona single glass slide. In this manner, a single sliderepresented 1 mm of nerve length. Each nerve wassectioned in this manner over its entire dissectedlength yielding approximately 480 sections per nerve(160 slides per nerve). The tissue was then stainedwith hematoxylin and eosin (Fig. 3).
The nerves thus processed were analyzed usingsoftware previously described.] Briefly, each sec-tion was entered into a computerized database usinga microprojector and digitizing tablet. The fascicularpatterns thus entered were followed proximally anddistally to identify changes in orientation and fascic-ular branching. Each fascicle was followed in a dis-tal to proximal direction, noting the levels at whicheach fascicle merged with neighboring fascicles.Using this technique, the level at which each fascicleto the FCU and FDP merged into adjacent fascicleswas determined. This level was then compared with
Watchmaker et al. / Anterior Transposition of the Ulnar Nerve
.the level at which each branch grossly separate~from the ulnar nerve distally as determined attime of the dissection. The distance between the:two levels represented the distance that the branchcould have been safely separated from the maulnar nerve without damaging plexus intercennec.itions.
Results
Transposition Measurements ....
The overall branching pattern to the FCU andFDP was variable (Fig. 1). The most proximal motorbranch arose an average of 1.6 cm distal to the epiocondyle (range, 0.5-3.2 cm). This branch mostquently provided innervation to the FCU alone (12specimens). The second branch arose an average of3.4 cm distal to the epicondyle (range, 1.6-5.2 cm).Branches arising more than 5 cm distally were notidentified, as the dissection was stopped at thi:point.
Two specimens contained a small branch exitinthe ulnar nerve at the level of the epicondyle.branch could be traced directly into the joint con-nective tissue. This branch did not travel to ammuscle group and likely represented an articula:branch. When present, this branch was sacrificedprior to transposition.
NONEN ONE ca m wvo ca mTHREE ca]Figure 4. Fifteen ulnar nerves underwent anterior transposition followed by proximal dissection of the first motofrom the main ulnar nerve. Significant gain in transposition away from the epicondyle was achieved.
Ynined attweent them the rnai~
The Journal of Hand Surgery / Vol. 19A No. 6 November 1994 919
transposed before and after separation of the motornches from the main ulnar nerve. This distance
measured from the prominence of the medial)icondyle to the transposed nerve (Fig. 4). The
distance to the epicondyle was 2.3 cm (range,~,1.5-2.0 cm) prior to this maneuver. There was an
e gain in transposition of 25% with 1 cm dis-55% with 2 cm, and 71% with 3 cm dissec-
tion. Following proximal dissection, the average dis-:ance from the epicondyle was 3.6 cm (range,
2.8-4.5 cm). Measurements were taken with thenerve placed superficially on the flexor musclemass. Gain in transposition after placement in a sub-muscular plane may be greater.
The gain in transposition varied with the level andpattern of branching. It also varied with the pointalong the nerve that was investigated. Figure 5 illus-trates the increase in transposition along the lengthof two nerves. The greatest gains were achieved inthe segment of nerve nearest the epicondyle.
e FCU an,dmal mot
to the:h mbst fre:U aloneaverage of
.6-5.2 cm)Ly were notped at
nch exitingadyle. This: joint con’:~
nsacrifice~
e could
18
!-12
¯ -J 9
z-- 6z
3
GAIN IN TRANSPOSITION FROM EPICONDYLE
0+4cm +3cm +2cm +lcm 0cm -lcm -2cm -3cm -4cm
LEVEL WITH RESPECT TO EPICONDYLE
ONE CM DISSECTION ~ TWO CM DISSECTION ~ THREE CM DISSECTION
GAIN IN TRANSPOSITION FROM EPICONDYLE18
)tor branch
+4cm +3cm +2cm +lcm Ocm -lcrn -2cm -3cm -4cm
BLEVEL WITH RESPECT TO EPICONDYLE
c. t~,ss~cr,o. - m "Two c. m c. t~,ss~cr, o.]Figure 5. Proximal dissection achieved the greatest gain in transposition where the nerve was tethered near the epicondyle
motor branches in this specimen. (B) Similar pattern observed in an additional ulnar nerve.
920 Watchmaker et al. / Anterior Transposition of the Ulnar Nerve
ULNARNERVE
Figure 6. Motor branches are labeled distally at the level that they grossly left the main ulnar nerve. Solid circles indithe level at which plexus interconnections occurred for these motor branches. The proximal motor branches couldtraced a minimum of 6 cm prior to interfascicular connections.
Fascicular Topography
Cross-sectional fascicu]ar studies demonstratedthat the fascicles that formed the most proximalmotor branches of the ulnar nerve in the forearmascended for long distances before interminglingwith other fascicles. Fascicles from these motorbranches ascended an average of 6.7 cm (range,6.0-7.5 cm) before plexus formation and intermin-gling with other fascicles occurred (Fig. 6). Moredistal motor branches in the forearm had a more
Figure 7. Longitudinal three-dimensional reconstructionof the ulnar nerve from 6 cm proximal to the epicondyle(lower right) to 4 cm distal to the epicondyle-(upper left).A small motor branch can be seen entering the nerve onthe left and traveling 7 cm prior to intermingling with otherfascicles.
variable internal topographic pattern. Themotor branch could only be traced an averagecm (range, 1.7 cm-6.3 cm) prior to joiningfascicles.
The number of fascicles in each nerve decreasedat the level of the epicondyle. At the elbow,ulnar nerve typically consisted of one or twofascicles along with a separate smaller fasciclefascicular group (Fig. 7). More distally, thisfascicular group gave rise to the first motor branche:to the FCU and FDP. i
Discussion
’The reasons for sub optimal results followirterior transposition for cubital tunnel syndrcmany and include tethering by posteriorbranches. Several techniques have beento deal with the branches to allow adequate transsition. In 1942, Learmonthz described and illu~trated a technique of transposition includingmal dissection of these motor~ branches in thearm as a mechanism of "freeing up" theireffects. 3"4 Intramuscular dissection of thebranches has also been advocated to facilitate
5position. Several authors, however, doany approach to the management of thesebranches. This leaves one to conclude thatbranches are either left in situ to tether the nerveare sacrificed to allow anterior transour dissections, we found articular branchesrarely present. Thus if "small branches" arequently sacrificed, they more likely retreal motor branches and not articular branches.viewpoint is supported by the microdissectionies of Jabaley, in which no articular branchesdocumented in the dissection of four
The Journal of Hand Surgery / Vol. 19A No. 6 November 1994 921
could be
second~e of
tg
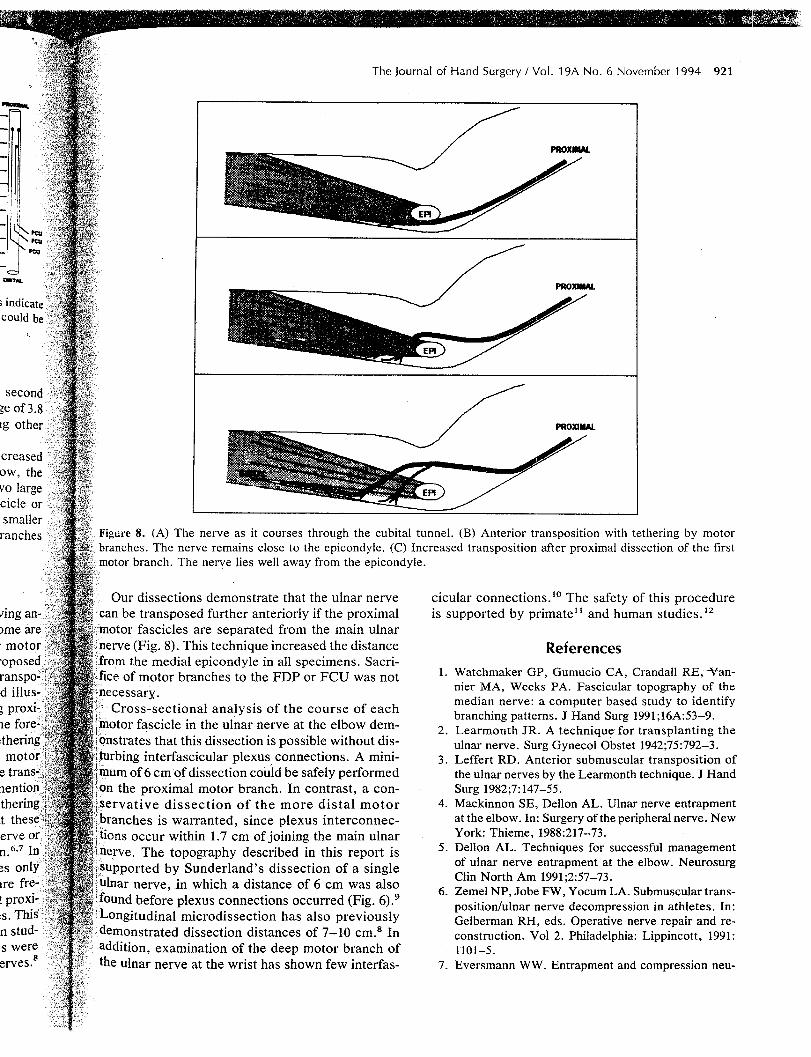
creasedow, thevo largeciclesmallerranches ~! Figure 8. (A) The nerve as it courses through the cubital tunnel. (B) Anterior transposition with tethering by motor
~ branches. The nerve remains close to the epicondyle. (C) Increased transposition after proximal dissection of the firsti:?~;~!i motor branch. The nerve lies well away from the epicondyle.
mg an, I,!Z~Our dissections demonstrate that the ulnar nerve
can be transposed further anteriorly if the proximalmotor fascicles are separated from the main ulnar
(Fig. 8). This technique increased the distancemedial epicondyle in all specimens. Sacri-
of motor branches to the FDP or FCU was not
S
~rveS.8
sectional analysis of the course of eachin the ulnar nerve at the elbow dem-
onstrates that this dissection is possible without dis-interfascicular plexus, connections. A mini-
of 6 cmof dissection could be safely performedthe proximal motor branch. In contrast, a con-
dissection of the more distal motorbranches is warranted, since plexus interconnec-
occur within 1.7 cm of joining the main ulnarThe topography described in this report is
mPported by Sunderland’s dissection of a single
nerve, .in which a distance of 6 cm was also!found before plexus connections occurred (Fig. 6).9Longitudinal microdissection has also previouslydemonstrated dissection distances of 7-1-0 cm.8 Inaddition, examination of the deep motor branch ofthe ulnar nerve at the wrist has shown few interfas-
cicular connections.I° The safety of this procedureis supported by primate~ and human studies.~2
References
1. Watchmaker GP, Gumucio CA, Crandall RE,-Van-nier MA, Weeks PA. Fascicular topography of themedian nerve: a computer based study to identifybranching patterns. J Hand Surg 1991;16A:53-9.
2. Learmonth JR. A techniqu,e for transplanting theulnar nerve. Surg Gynecol Obstet 1942;75:792-3.
3. Leffert RD. Anterior submuscular transposition ofthe ulnar nerves by the Learmonth technique. J HandSurg 1982;7:147-55.
4. Mackinnon SE, Dellon AL. Ulnar nerve entrapmentat the elbow. In: Surgery of the peripheral nerve. NewYork: Thieme, 1988:217-73.
5. Dellon AL. Techniques for successful managementof ulnar nerve entrapment at the elbow. NeurosurgClin North Am 1991;2:57-73.
6. Zemel NP, Jobe FW, Yocum LA. Submuscular trans-position/ulnar nerve decompression in athletes. In:Gelberman RH, eds. Operative nerve repair and re-construction. Voi 2. Philadelphia: Lippincott, 1991:1101-5.
7. Eversmann WW. Entrapment and compression neu-
922 Watchmaker et al. / Anterior Transposition of the Ulnar Nerve
ropathies. In: Green DP, ed. Operative hand surgery.3rd ed. New York: Churchill Livingstone, 1993:1356-64.
8. Jabaley ME, Wallace WH, Heckler FR. Internal to-pography of major nerves of the forearm and hand: acurrent view. J Hand Surg 1980;5:1-19.
9. Sunderland S. Nerves and nerve injuries. 2nd ed.New York: Churchill Livingstone, 1987;728-49.
10. Chow JA, Van Beek AL, Meyer DL, Johnson MC.Surgical significance of the motor fascicular group of
the ulnar nerve in the forearm. J Hand Surg10A:867-72.
11. Mackinnon SE, Dellon AL. Evaluation of microscal internal neurolysis in a primate medianmodel of chronic nerve compression. J Hand1988;13A:345-51.
12. Mackinnon SE, McCabe S, Murray JF et al. interneurolysis fails to improve the results of primarpal tunnel decompression. J Hand Surg 1991:211-9.





















![yeditepeanatomy1.files.wordpress.com · Web viewKey word for this class [Nerve] Entrapment [/Compression] ... Motor: Patients with cubital tunnel syndrome present with paresthesias](https://static.documents.pub/doc/80x56/5c9e1e9e88c993d0368c165b/-web-viewkey-word-for-this-class-nerve-entrapment-compression-motor-patients.jpg)


