47
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | jennifer-anderson |
| View: | 217 times |
| Download: | 1 times |


Introduction
• Diabetes causes a number of lethal complications affecting almost every system of the body and hence the overall quality of life.
• The Gastrointestinal Tract (GIT) is no exception to diabetic complications; it affects the digestive processes, motility as well as nervous control of the entire system.
• Since the absorption and metabolism of glucose is mediated by GIT and liver respectively, gastrointestinal (GI) complications commonly occur in diabetes.

GASTROINTESTINAL COMPLICATIONS OFDIABETES MELLITUS: AN OVERVIEW
• GI symptoms are more common in individuals with diabetes than nondiabetics.• It is seen that 76% of diabetics had at least one clinical manifestation of GI
complications. • Constipation was the most frequent amongst them (60% of cases). Also, upper GI
symptoms were more closely• associated with diabetes mellitus

Common GI symptoms among diabetics

PATHOPHYSIOLOGY

Early identification and appropriate management of GI complications is important for improving both diabetic care and quality of life of the patients.
The common GI complications of diabetes have been discussed in thesubsequent sections.
Gastrointestinal Complications of Diabetes

GIT COMPLICATION ALONG WITH
DIABETES INCLUDE
GERD
GASTROPARESIS
CONSTIPATION
DIARRHOEAFAECAL INCONTINENCE
IBS
LIVER DISEASES

1. GASTRO-OESOPHAGEAL REFLUX DISEASE (GERD)
Epidemiology: Up to 50% of patients with diabetes have oesophageal abnormalities that involve motility disturbance and/or acid reflux. A North Indian study revealed that the prevalence of GERD was 16.2%, with diabetes as one of the co-morbidities.
Pathophysiology: Autonomic neuropathy and structural remodelling of the oesophageal musculature in diabetes results in abnormal peristalsis, spontaneous contractions and reduced lower oesophageal sphincter (LES) tone.

Clinical features of GERD in diabetes
Heartburn and epigastric pain are known to be the most frequent GERD associated symptoms, occurring in up to 90% of patients with proven type 2 diabetes mellitus (T2DM).

Diagnosis
• High resolution manometer and impedance manometer are newer modalities to assess oesophageal motility
• Upper GI endoscopy to detect hiatal hernia, oesophagitis • Barium oesophagogram• Oesophageal histology to detect oesophagitis, dysplasia, etc.• 24-hour oesophageal pH monitoring
Endoscopy for the diagnosis of GERD

Prevention
• Glycemic control and weight management are the cornerstones for preventing GERD in diabetes mellitus
• Patient should be advised to:– Raise the head end of the bed by 6–8 inches to avoid nighttime symptoms– Refrain from lying down in recumbent position for 2–3 hours after the meals– Abstain from smoking, drinking alcohol, soda and caffeine containing
beverages– Avoid foods that reduce LES pressure like fatty foods, tea, coffee, etc.

Management
• H2 antagonists: Ranitidine, Famotidine, etc.
• Proton pump inhibitors: Pantoprazole, Rabeprazole, etc.
• Prokinetic drugs such as metoclopramide
• A 2-week course of erythromycin has been shown to reduce mean oesophageal transit time and gastric emptying time in type 2 diabetics
2. DIABETIC GASTROPARESIS
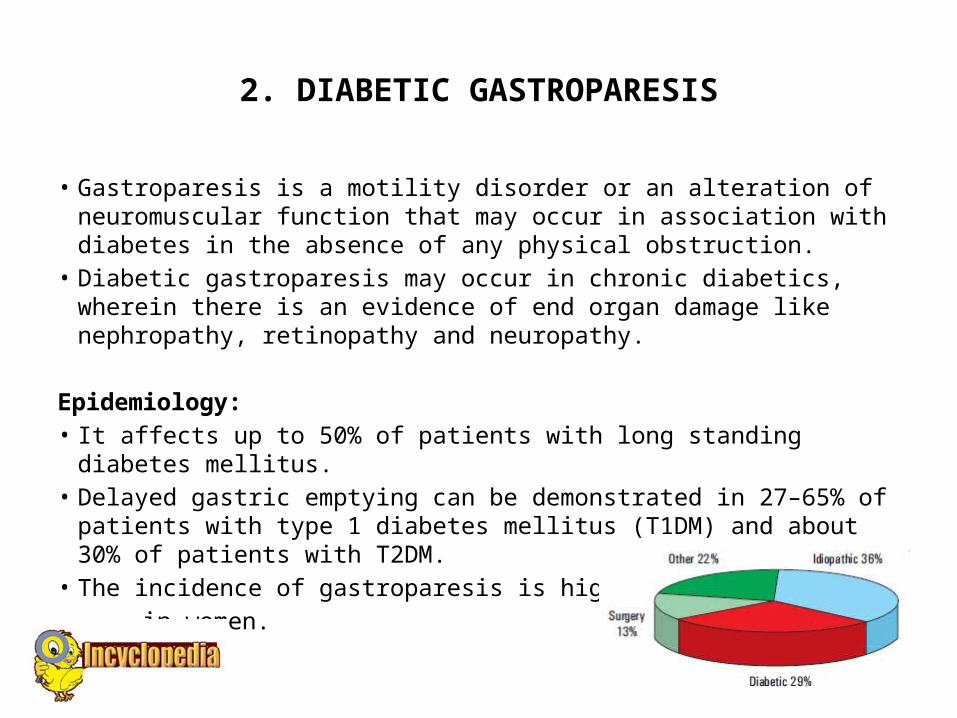
• Gastroparesis is a motility disorder or an alteration of neuromuscular function that may occur in association with diabetes in the absence of any physical obstruction.
• Diabetic gastroparesis may occur in chronic diabetics, wherein there is an evidence of end organ damage like nephropathy, retinopathy and neuropathy.
Epidemiology: • It affects up to 50% of patients with long standing diabetes mellitus.• Delayed gastric emptying can be demonstrated in 27–65% of patients
with type 1 diabetes mellitus (T1DM) and about 30% of patients with T2DM.
• The incidence of gastroparesis is higher in women.
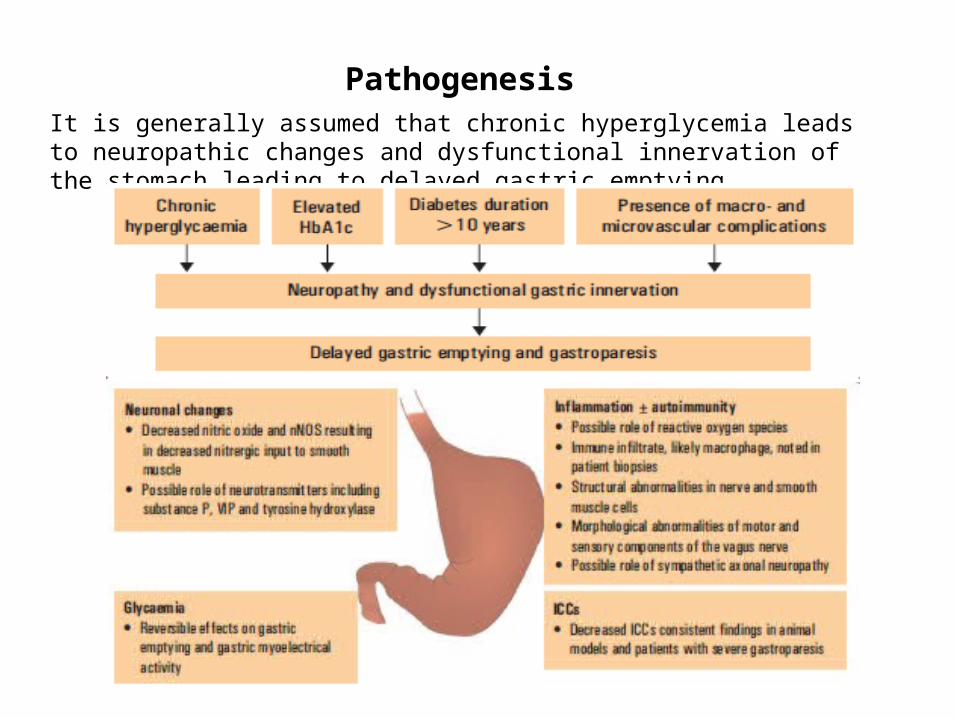
It is generally assumed that chronic hyperglycemia leads to neuropathic changes and dysfunctional innervation of the stomach leading to delayed gastric emptying.
Pathogenesis

• Nausea• Vomiting• Early satiety• Postprandial fullness after few bites of food• Bloating• Upper abdominal pain• Palpitations and heartburn• About 53% of patients may experience weight loss, but 18–24% may experience
weight gain• Unexplained alternating hyper- and hypoglycemia due to a mismatch between
insulin action and carbohydrate absorption• Prolonged gastric distension increases propensity for transient relaxation of the
LES, thus exacerbating gastro-oesophageal reflux
Clinical features

Types of Gastroparesis

Diagnosis
• Detailed medical history
• Physical examination: Focus on abdominal and neurological examination
• Blood investigations
• Scintigraphy
• Plain X-ray abdomen
• Barium meal study
• GI endoscopy

• Tracer method of scintigraphy
• Ultrasonography
• Electrogastrography (EGG)
• Other modalities like magnetic resonance imaging (MRI)
• Computed tomography (CT)
• Impedance epigastrography
• Impedance tomography
• Real time ultrasonography
• Positron emission tomography (PET) can be used to document delayed gastric emptying

Management
The therapeutic pyramid

Management
Dietary management:• Patients should be advised to eat a diet low in fat content, and should be instructed to
consume frequent and small meals
• Preferentially consume a diet low in fiber
• Small particle size helps in accelerating gastric emptying. Hence, patients should be instructed to chew their food adequately
• Food should be consumed in liquefied form. Taking fluids throughout the meal and sitting upright or walking for 1–2 hours after meals may help the patient to accelerate gastric emptying
• Low and high fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAP) foods: A reduction of FODMAPs in a patient’s diet may improve functional Gl symptoms
• Low FODMAP foods: To be eaten, High FODMAP foods: To be avoided

Pharmacotherapy

Pharmacotherapy Continued
Prevention:• Keeping the blood glucose levels under control through compliance with diabetes
medications• Lifestyle modifications like physical activities and dietary changes prevent damage
to the vagus nerve• Maintenance of a normal body mass index (BMI)

3. CONSTIPATION
• Constipation is seen as a major GIT complaint in patients with diabetes than in non-diabetics.
• It affects up to 60% of patients with long-standing diabetes mellitus. • Hyperglycemia may directly inhibit intestinal transit in such patients.
Epidemiology:• The prevalence of constipation is higher in women, and amongst those diabetic
patients who consume medications like calcium channel blockers, which cause constipation.
Pathogenesis:• Neuronal dysfunctions in large bowel along with impaired gastro colic reflex are
associated with constipation.
• Difficult, infrequent or seemingly incomplete defecation
• Straining at stools and hard stools
• Two or fewer bowel movements in a week
• Occasional massive amount of fecal material found in the large atonic and dilated colon of diabetes patients
• It can infrequently lead to mega colon, pseudo-obstruction, perforation, etc.
Clinical features

• Detailed history about bowel movements, straining at stools, duration, stool consistency and associated bleeding, if any, should be obtained.
• Thorough physical examination with focus on abdominal examination and auscultation for bowel sounds.
• Rule out other causes of constipation like hypothyroidism or medications .
• Constipation that does not respond to lifestyle changes or first-line medications require further investigations.
• Anorectal inspection looks for skin excoriations, skin tags, anal fissures or haemorrhoids.
• Digital rectal examination, aabdominal X-ray and barium enema, colonoscopy, radio-opaque marker test
Diagnosis

Prevention and Management
Management
• Laxatives: Sorbitol or lactulose can be used to treat constipation• Osmotic laxatives and saline are reserved for severe cases
Prevention
• Patients should be enquired for medications like antidepressants and calcium channel blockers, which can cause constipation and advised to avoid the same
• Patients should be advised to:– Consume large quantity of water i.e., around 2–3 liters per day. Warm water
early in morning can improve colonic motility– Perform deep breath exercises and walking– Have a diet high in fiber content like beans, cereals, vegetables and fruits– Set a particular time of defecation each day

4. DIARRHEA
• Intestinal and colonic motility disorders in both types of diabetes (1 and 2) can lead to diarrhea.
• Diabetic diarrhea can be described as the presence of chronic diarrhea which is usually brown, watery, profuse and might be associated with tenesmus.
• The diarrhea is long-lasting, typically episodic and consistent with hyperglycemia and the presence of diabetic neuropathy.
Epidemiology• Around 4–22% of people with diabetes suffer from diarrhea.

Diagnosis
• The diagnosis depends on a judicious clinical assessment accompanied by a stepwise laboratory evaluation, which allows the differentiation of idiopathic diabetic diarrhea from many other causes of diarrhea, that can occur in diabetes and non-diabetes patients.

Pathophysiology

• Diarrhea associated with diabetes characteristically occurs at night following meals and is watery
• Painless diarrhea is mainly associated with fecal incontinence
• Intermittent diarrhea can alternate with constipation
• Evidence of diabetic peripheral and autonomic neuropathy
Clinical features

• The management chiefly relies on use of alpha-2 adrenergic agonist to stimulate intestinal absorption of fluids and electrolytes
• Patients should be instructed to maintain strict glycaemic control and adequate hydration
• Avoid medications like biguanides and alpha-glucosidase inhibitors
• Symptomatic measures like atropine, codeine sulphate and loperamide as antimotility agents to relieve abdominal cramps
• Adrenergic agonists like clonidine that have antisecretory action Octreotide, somatostatin based on their antisecretory and antimotility actions
Management

• Rifaximin, a GI selective antibiotic along with other antibiotics like amoxicillin-clavulanic acid, doxycycline, ciprofloxacin, metronidazole, neomycin can be used to eradicate the small intestinal bacterial overgrowth
• Clonidine 0.1–0.6 mg BD can reverse peripheral adrenergic resorptive abnormalities, while octreotide 100–150 mcg is reserved for refractory cases
• If no specific cause of diarrhoea is identified, empiric therapy with simple antidiarrhoeal agents (e.g., loperamide) is a reasonable starting point
Management (continued)

Small intestinal bacterial overgrowth (SIBO)
• SIBO refers to bacterial overgrowth in the small intestine generally due to intestinal stasis. It is seen in about 15% of patients with T2DM. Also, 44% of patients with T1DM had autonomic neuropathy.
When to suspect SIBO?• Predominant symptom is diarrhoea• Marked milk intolerance• Older age/ long duration diabetes• Type 1 diabetics with autonomic neuropathy• Marked abdominal bloating• Marked flatulence• Proton pump inhibitor therapy• History of response to antibiotics/ probiotics

5. FAECAL INCONTINENCE
• Fecal incontinence is the inability to control bowel movements, causing stool to leak unexpectedly from the rectum.
Epidemiology• Reported in 20% of patients in a study on diabetic population
• Mainly affects the elderly patients
• The prevalence of fecal incontinence secondary to anorectal dysfunction has also been reported to be increased in patients with diabetes

Pathogenesis
• Many factors like aberrant autonomic and enteric regulation of the internal anal sphincter and rectal contraction are involved in the pathogenesis of faecal incontinence
• Acute hyperglycemia also inhibits external anal sphincter function and decreases rectal compliance

• It is characterised by normal or moderately increased stool volumes and anorectal sensory and motor dysfunction
• It occurs more commonly at night
• Rectal prolapse can be demonstrated by asking the patient to attempt defaecation
• Anorectal examination reveals a reduced anal muscle tone and loss of anal wink reflex (anus normally squeezes on stroking the skin around the anus)
Clinical features

• Anorectal manometry
• Endoscopic examination of recto sigmoid region
• Rectal sensory testing
• Anal endosonography, MRI, defaecography Detailed neurological examination of back and lower limbs
Diagnosis

• Strict glycaemic control
• Use of loperamide
• Laxatives for regular bowel movements
• Anal sphincter repair
Management
6. IRRITABLE BOWEL SYNDROME (IBS)
• IBS is a functional bowel disorder characterized by abdominal pain or discomfort and altered bowel habits in the absence of detectable structural abnormalities.
Epidemiology• IBS is the most common reason for referral to gastroenterologists
• In South Asia and India, men are most commonly affected by IBS
• Data suggests that diabetics experience IBS symptoms significantly more frequently than the general population
• Gut bacteria and metabolism are the common factors affected by IBS

Diagnosis
• History and physical examination
• Proctoscopy examination to rule out local anal fissures
• Routine stool examination is done for Amoebae and Giardia
• Sigmoidoscopy or colonoscopy is done in suspected cases

• Abdominal pain or discomfort localized in the periumbilical region or left hypochondriac region
• Abdominal pain and other accompanying features like bloating are usually relieved temporarily by defaecation
• In India, there is either constipation or diarrhea predominant pattern, which varies regionally within the country
• Incomplete evacuation is a distressing symptom in constipation predominant form
• Stool consistency may vary from small-quantity semisolid or liquid with mucous in those with diarrhea, to hard pellet-like with mucous in constipated subjects
• Abnormal psychological features have been reported in over 70% of patients
Clinical features

• Reassurance and psychological support
• Restriction of milk and spicy food in those with diarrhea and restriction of milk, legumes and cabbage in those with bloating
• Commercially available isabgol husk preparations can be taken with meals to ensure an additional fiber intake of 15–20 g/day
• Tegaserod, a specific serotonin (5-HT4) agonist, can improve symptoms in patients with IBS and constipation
• Patients with diarrhea benefit from loperamide and antispasmodics
• Selective chloride-channel activators lubiprostone; rifaximin, a GI selective antibiotic and probiotics have proven to be beneficial in IBS
Management

7. LIVER DISEASES
• The liver is a key organ involved in glucose metabolism and energy homeostasis. A major amount of carbohydrates absorbed from the GIT undergo hepatic processing and subsequent storage as glycogen or are metabolized into amino acids or fatty acids.
• Hyperglycemia occurs owing to a combination of processes such as increased rate of hepatic glucose output secondary to insulin resistance and diminished peripheral uptake.
• There is a profound relationship between diabetes and liver disease.

Liver diseases occurring as a consequence of diabetes mellitus:• Glycogen deposition, Steatosis and non-alcoholic steatohepatitis (NASH), Fibrosis
and cirrhosis, Biliary disease, cholelithiasis, cholecystitis, Complications of therapy (cholestatic and necroinflammatory)
Diabetes mellitus and abnormalities of glucose homeostasis occurring as a complication of liver disease:• Hepatitis, Cirrhosis, Hepatocellular carcinoma
• Fulminant hepatic failure
• Post-orthotopic liver transplantation

• Glycogen deposition: Abdominal pain, nausea, vomiting and hepatomegaly, liver enzyme abnormalities
• Fatty liver: Hepatomegaly, normal or only mildly abnormal transaminases and normal bilirubin
• Cholelithiasis: Obesity and hyperlipidaemia are the confounding variables
• NAFLD: Most patients with non-cirrhotic NAFLD are initially asymptomatic, and are diagnosed due to an incidental detection of raised liver enzymes or fatty liver on ultrasonography.
• Presence of diabetes, elevated BMI and liver fibrosis were identified as risk factors for progression to hepatocellular carcinoma (HCC) among NAFLD casesHCC: Weight loss, jaundice, abdominal pain and deranged liver enzymes.
Clinical features

• All pharmacological therapies should be supplemented with lifestyle modification and weight reduction especially for NAFLD
• Insulin sensitising agents like metformin and pioglitazone; vitamin E; glucagon-like peptide-1 (GLP1) analogues like liraglutide; omega-3 fatty acids; antiobesity drugs like orlistat are the pharmacological options for management of NAFLD.
• Insulin management for diabetic control can benefit patients of glycogenic hepatopathy within 4 weeks
• Glycaemic control, weight reduction and ursodeoxycholic acid are the therapeutic options for fatty liver
Management

• Weight management is the single key aspect for preventing NAFLD
• Patients should be given a target for sustained weight loss of 7–10% of body weight with a combination of a balanced, calorie-restricted diet.
• Lifestyle modification inclusive of exercise and alcohol cessation
• Improvement in glycaemic control
• Proper patient evaluation, counselling to prevent the development of hypertension
Prevention

















